
Abstract
Background:
Asians in the United States receive less palliative care and enter hospice less than Whites, disproportionately receive more invasive mechanical ventilation, and report less involvement in decision-making with physicians than they would like. Despite the growing literature addressing serious illness in diverse patient populations, communication with Asians is understudied. This study aimed to explore U.S. physician perceptions of clinical interactions with Asian patients with serious illness and barriers and facilitators to physician–patient communication.
Methods:
This is an exploratory qualitative descriptive study using semistructured interviews with U.S. physicians who cared for Asian patients with serious illness. We used an inductive content analysis approach to identify themes related to facilitators and barriers to communication between Asian patients, their families, and physicians.
Results:
We conducted 10 physician interviews between February and April 2024. Of participants, 50% were White and 50% were Asian, the majority were male, and 50% specialized in palliative care. Three major themes arose: (1) trust cannot be assumed; (2) understanding and honoring the role of family are key; and (3) honoring the patient’s preferences for communication can build trust.
Conclusion:
This study is a step in illustrating how a cross-cultural approach to communication needs to align physicians, patients, and families on the process of communication and shared decision-making and not only on the goals for care. Moving toward a cultural adaptive approach can empower clinicians to engage in a trust-building process of inquiry, observation, and understanding of how sociocultural factors impact patient preferences for health care.
Introduction
Culture shapes how people make meaning of illness and dying.1–3 The National Consensus Project 4 stresses the need to emphasize the cultural aspects of care in palliative care delivery. With increasing global migration, encounters between patients and physicians of different backgrounds are more common, thus increasing the risk of cross-cultural misunderstandings. 1 Even with the growing literature addressing serious illness in diverse patient populations, there are relatively few studies focused on Asians, especially in the United States, despite being the fastest growing racial or ethnic group in the United States.5,6
Marginalized groups of patients, including Asians, report low satisfaction with end-of-life care.7–9 Asians report less involvement in decision-making with physicians than they would like, 10 receive less palliative care and enter hospice less than Whites,11,12 and disproportionately receive more invasive mechanical ventilation. 13 One challenge to addressing disparities for this population is the diversity of traditional norms, values, and religious beliefs among this heterogeneous population who come from East Asia, South Asia, and Southeast Asia. In the United States, Chinese adults comprise the largest subpopulation (22%), followed by Indian (20%) and Filipino adults (17%). 14
To address care disparities, two bodies of literature have emerged that are relevant to health care delivery for Asian patients. One body of scholarship can be described as “culture specific” and focuses on subgroups of Asians15,16 who live in specific locales (e.g., patients in Hong Kong, Mainland China, and Taiwan; 17 Japanese Americans and Japanese living in the United States; 18 or South Asians in Canada). 19 The other body of literature can be described as “culture general” and more broadly addresses how clinicians can improve care for patients from diverse backgrounds.2,20–23 While both are critical, several important ideas can become lost when focusing on one or the other. First, palliative and end-of-life care in the United States are historically rooted in White middle-class cultural and religious values, 24 which creates a dominant culture and assumed approach to communication and care delivery. Second, the idea of culture is often constrained to the notions of race, ethnicity, and country of origin, without adequately acknowledging that other experiences, such as workplace culture or religious practice, can also create cultural subgroups.23,25
In 2001, Kagawa-Singer and Blackhall's JAMA article, “Negotiating Cross-Cultural Issues at the End of Life,” addressed the tension of being both “culture-specific” and “culture-general” in end-of-life care. 1 They accomplished this by inviting readers into the life stories of an African American couple in southern United States and a Chinese American woman from Hawaii, while asking readers to consider the ABCDE framework [attitudes (A), beliefs (B), contexts (C), decision-making styles (D), and environments (E)] for assessing patient and family perspectives on end-of-life conversations. 1 Since then, much has been written about addressing palliative care disparities for Blacks,26–28 but less so for Asians. 6 Particularly in the United States, the health narrative is shaped by the systematic exclusion and misrepresentation of Asian populations in health research.7,29–32 Racialized stereotypes reinforce inaccurate societal impressions that Asians seldom experience disproportionate health disparities,32,33 despite Asians’ experiences of racism in health care. 34
To address the literature gap, we conducted an exploratory qualitative descriptive study to provide a snapshot of physician perspectives on cross-cultural palliative and end-of-life care for Asian patients in the United States. We sought to characterize physicians’ perceptions on barriers/challenges (Theme 1) and facilitators/strategies (Themes 2 and 3) to build trust and effective communication with Asian patients with serious illness. This study contributes to the growing literature about communication with persons with serious illness.
Methods
Following the Consolidated Criteria for Reporting Qualitative Research guidelines, 35 we conducted semistructured interviews to characterize physician perspectives on communication with U.S. Asian patients with serious illness and their families. Exploratory-descriptive qualitative research is appropriate to explore a topic with limited coverage in the literature. 36
Study sample
Eligible participants resided in the United States, had experience as a practicing clinician with patients who self-identify as Asian and have a serious illness, and were able to provide consent. We used a purposeful sampling approach to recruit a nationwide sample from different states in order to describe the phenomena across diverse locales. We recruited participants by using cold emails and via various public health and physician networks.
Data collection
Interview guide.
The semistructured interview guide was developed based on a literature review23,37,38 by the interviewer (C.H.), who worked collaboratively with two palliative care physicians, including a physician-researcher (J.T.) and clinician-educator (I.M.Y.) (Supplementary Table S1). Open-ended and probing questions addressed participants’ personal and professional experiences with Asian patients with serious illnesses, cross-cultural communication, considerations of how “best care” might be defined, and approaches to culturally-adaptive care. The team used interviewer feedback to iteratively refine the guide after the first two interviews. Acknowledging that the term “Asian” encompasses a broad diaspora of people, we did not focus on a specific Asian population in the interview guide.
Interview procedure
The interviewer (C.H.) had no prior relationship with participants and conducted one-on-one, semistructured interviews after training and under the guidance of the physician-researcher (J.T.) and clinician-educator (I.M.Y.). C.H. completed interviews on a video-conferencing platform after obtaining verbal informed consent and collecting participant demographics (age, gender, race, and ethnicity) and their specialty. The interviewer kept reflexive notes after each interview. All interviews were recorded, transcribed, and de-identified. Participants provided verbal informed consent prior to participation, which includes the publication of anonymized quotes in this article.
Data analysis and trustworthiness
We used an inductive content analysis approach 39 to identify broad content categories and themes related to facilitators and barriers to communication between Asian patients, their families, and physicians. We used MAXQDA (VERBI Software, Berlin, Germany) to support the analysis. Preliminary data analysis occurred simultaneously with data collection, which involved reviewing interview recordings and transcripts to develop an understanding of key concepts. The interviewer (C.H.) used the first two transcripts to create a preliminary codebook. Additionally, the palliative care team members (I.M.Y., J.T.) independently reviewed the first two coded transcripts and, together with the interviewer, consolidated findings into a coding scheme used to categorize excerpts. After completing the majority of interviews, the interviewer (C.H.) and a research assistant (F.L.T.) (hereafter “coders”) used the coding scheme to independently code all interviews. The coders met regularly and consulted with the rest of the team to review, refine, and reconcile coding. Sampling continued until we identified a high degree of redundancy in new interviews, indicative of data saturation. 40 After all transcripts were coded, the entire research team met to identify key themes. To explore the credibility of the results, we returned the thematic findings to 3 of the 10 participants to check for accuracy and resonance with their experiences. 41 The Institutional Review Board of the University of North Carolina at Chapel Hill determined this study to be exempt.
Results
We conducted 10 physician interviews between February and April 2024. Interviews lasted 40–75 minutes. Of participants, 50% were White and 50% were Asian, the majority were male, and 50% specialized in palliative care (Table 1). Three major themes arose: (1) trust cannot be assumed; (2) understanding and honoring the role of family are key; and (3) honoring the patient’s preferences for communication can build trust (see Fig. 1). Table 2 provides additional quotes to supplement the results below.
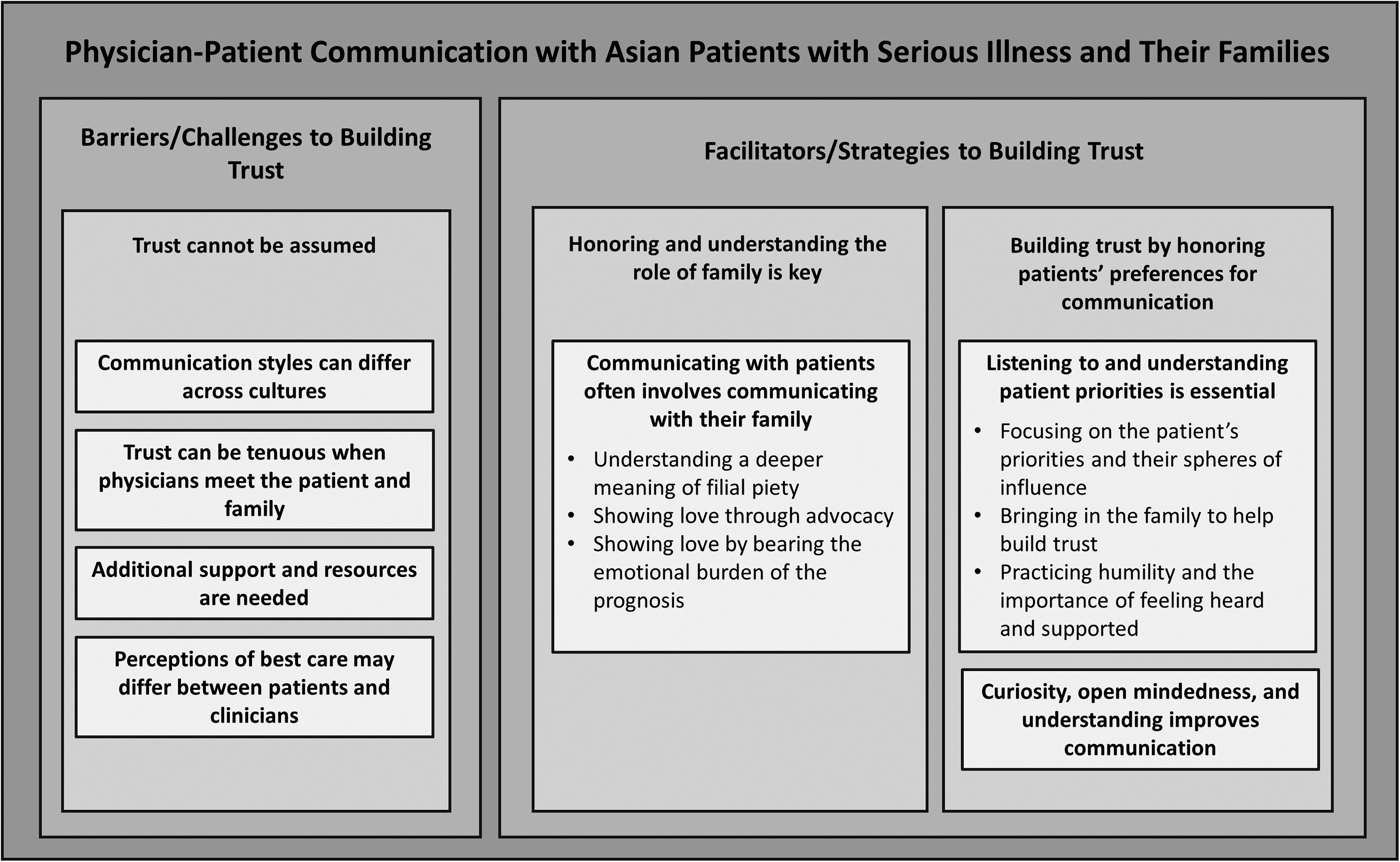
Barriers/challenges and facilitators/strategies for effective communication with Asian patients with serious illness and their families.
Participant Demographics
Themes, Subthemes, and Representative Quotes in the Context of Communication with Asian Patients with Serious Illness and Their Families in the United States
THEME 1: Trust cannot be assumed
Communication styles can differ across cultures
Participants noted that although trust is universally beneficial to care, trust-building strategies vary by culture and personal experience.
…if I had to sort of try to identify some of the differences, though not unique to Asian patients, is probably more use of metaphors and…indirect forms of communication, so oftentimes there is more relying on context. There is…I was going to say, need to build trust, but that is not right. The reason I pause is because I think that [trust] is important for all patients. But…the way that you build trust oftentimes for Asian patients may be different than other patients. (P9)
Silence and mismatch of communication styles complicated encounters.
[Y]ou can be in a meeting with an Asian family, and everyone is sitting there very quiet, and you think everyone is agreeing with you. Then, it turns out they are super mad, but no one is saying anything…it’s sort of like a respect thing. So, you have no idea. (P1)
Trust can be tenuous when physicians meet the patient and family
Participants recognized that patients’ previous experiences with health care impacts their receptiveness to health care interventions and communication.
If this is the fourth time that they are having this conversation, they have already been kind of traumatized. And they feel that we are not listening to them, and they have to advocate more and more. (P2)
Approaches to conversations are culturally bound. Some physicians described the U.S. health care systems’ approach to serious illness conversations as failing to capture the needs of marginalized populations.
[T]he way conversations about serious illness was…formed and built was by White people…it was informed by what works when you talk to White patients about their illness, their understanding of their illness...a lot of the questions we were taught to ask...are informed by the fact that it was predominantly White people who…taught us this. (P2)
Additional support and resources are needed
Several participants revealed low confidence in their ability to navigate cross-cultural serious illness conversations.
I have a hard time feeling confident that I understand someone else’s beliefs and values, though [we] always discuss what those are. (P6)
At times, unease was amplified in situations where the patient and family members had prior negative health care experiences.
I feel like sometimes I am just another link in the chain of: this has been difficult, we haven’t felt listened to, this is another person who doesn’t want what I want. (P2)
Participants felt that their unease was exacerbated by a lack of training on how to navigate cross-cultural serious illness conversations. Few participants received formal training for cross-cultural communication in the United States.
I have not received any training or skills workshops or really any tips, like what I should be looking out for… (P8)
Nor did they receive any information about communicating with Asian populations.
Not a lot about Asian populations…I think [we] probably could use more. (P5)
Most participants learned about cross-cultural communication techniques and approaches for Asian patients with serious illness through self-initiated opportunities (e.g., conversations with colleagues and friends) and resources (e.g., journal articles).
Just in my personal life, and in my professional life with my colleagues, the literature, in meetings, and also just talking through cases. (P1)
Overall, participants wanted more resources about cross-cultural communication with Asian patients with serious illness and their families.
In general, if there was more teaching about communication and…culturally sensitive communication beyond palliative care…I think that would be very helpful…there is still a big gap. (P2)
Perceptions of best care may differ between patients and clinicians
Physician expertise confers trust.
Some physicians noted that a lack of interpersonal trust can lead to patients’ reliance on hierarchy.
[A] lot of our patients don’t really have a personal trust [of clinicians]. They’re kind of trusting more in the fact that we’re on faculty at [redacted]. (P5)
Similarly, social hierarchies (e.g., medicine judged as a respectable profession) can influence communication with physicians viewed as “experts.” Participants noted that Asian patients may seek out and defer to professional expertise on what care plan options to pursue.
[D]epending on the culture, I think patients and families perceive physicians to be definitely more in higher power than they are. (P9)
Whatever you think doc…you know better than I do. (P8)
However, differences in the expectation and perception of “best care” between physicians, patients, and families can make it challenging to provide high-quality care that aligns with patient preferences and fulfills patient and family’s expectation of power distance.
[T]he challenge is how can you get their perspective and what is important to them while also sort of fulfilling the role that they expect. Which is that you guide them and tell them what to do. (P4)
Participants also warned that if patients are only following recommendations due to the cultural belief of physicians as authority figures, and if physicians reinforce this power dynamic, it may hinder care.
[I]f culturally they feel like they have to do what the doctor says but really, they are not into it…they are doing it because you are an authority figure. I think you are also doing the patient and the family a disservice. (P9)
THEME 2: Honoring and understanding the role of family are key
Communicating with patients often involves communicating with their family
It was difficult when patients involved or deferred clinical communication to family members.
[Y]ou have to do both dances, two different levels of communication…in the same encounter...I am having different conversations with the family and the patient. (P8)
I guess the way we are trained…[is] to be very patient-centric…But when the patient themselves opts out, that makes that really difficult. (P7)
Understanding a deeper meaning of filial piety
Filial piety is perceived as an Asian phenomenon, traditionally linked to duty and obligation. However, filial piety can also represent a practice of love through acts of service.
[F]ilial piety is a big value in Asian culture. (P4)
[F]or Asian families, it’s a way of wanting what is best for them. It’s a way of showing I care. (P9)
Showing love through advocacy
Some physicians inferred that Asian patients and families adapt their health care-related behavior and decision-making to demonstrate love and duty, and thus seek out the “best care” by seeking additional information, care, and/or services.
[T]he way of showing love and support is through seeking more care, more aggressive care….I think the disconnect is around giving up hope…the family feeling like if we pursue more palliative care, then we are giving up on our loved one or we are sort of not supporting them enough. (P2)
Showing love by bearing the emotional burden of the prognosis
Participants noted that Asian families may express a protective, advocating approach to patient care to preserve their loved one’s fortitude. Physicians observed this belief through nondisclosure, where patients were unaware of the full extent of their condition.
[A] family will say, “I don’t want my mom to know she has cancer or…is going to die. Because that will just kill her spirit.” (P1)
THEME 3: Building trust by honoring patients’ preferences for communication
Participants recognized that differences between physician, patients, and family cultures, beliefs, and values can create communication challenges.
[W]hen you are dealing with families and patients that are outside of your culture…it is a challenge. (P7)
Facilitators of trust were noted to include: 1) listening to and understanding patients’ priorities and 2) demonstrating curiosity, open-mindedness, and understanding.
Listening to and understanding patients’ priorities are essential
Focusing on the patient’s priorities and their spheres of influence
Participants shifted priorities toward supporting a patient’s well-being by meeting the patient where they are and forming care plans around the patient’s priorities.
It’s whatever you can do to achieve that alignment of their hopes and their wishes as it matches their values and in the context of reality. I think it incorporates the spheres that are most important to them. That sphere might be family, it might be their own personal sphere, it might be spirituality….(P8)
I don’t try to force them to decide. (P10)
Bringing in the family to help build trust
Participants noted that, among Asian patients, the inclusion of family members in serious illness discussions is vital.
I think if you don’t have the family involved, it often can fail…our best allies in working with patients is to work with their families. (P3)
Practicing humility and the importance of feeling heard and supported
Participants noted that identifying and integrating patient and family core values and beliefs into the care plan build trust.
I used to be quite…certain that I had all the answers and that…my recommendations were the most valid. But as I’ve gone on in my practice, I have decided that sometimes the patient just needs to be heard and realize that I am going to try to help them even if I don’t think that this is the right medicine for them...(P7)
Curiosity, open-mindedness, and understanding improves communication
To build trust and ensure that Asian patients and families feel heard and seen, physicians clarified that decision-making should ultimately center on patient and family preferences.
[E]ntering these conversations with true curiosity, true need to understand, and really trying to listen where they are coming from, and not so much imposing where I need to get in these conversations. (P2)
[T]he data is there. You just have to be willing to see it. (P9)
Discussion
Communication between clinicians and patients with serious illness often involves high-stakes encounters. This qualitative study explores the perspectives of a nationally drawn sample of clinicians about conversations with Asian patients with serious illness in the United States. Unseen in prior studies, participants noted that trust in clinician–patient encounters could not be assumed but earned through the development of a relationship, and that patient or family silence in conversations does not surmise agreement. Our findings shed light on the complexities of the family’s role in communication and advocacy and underscore the challenges that clinicians report in struggling to provide goal-concordant care across cultures.
What is seldom acknowledged in cross-cultural communication studies is that one culture is typically dominant and the other nondominant. Explicitly stating that a hierarchy of cultures exists can help us acknowledge that the person from the nondominant culture (e.g., patient/family) is often in the position of having to respond by choosing to “assimilate, accommodate, or separate” from the communicator from the dominant culture, according to the communication theorist Mark Orbe. 25 His Co-Cultural Communication Theory 25 can help us think about mismatches in expectations, where physicians may expect patients to have an “assertive” communication style when patients may have a “nonassertive” or even an “aggressive” communication style.
Misinterpretations of patient and family motives based on their actions are not surprising when one considers that the quote “Your silence gives consent” is attributed to Plato, a foundational giant of Western culture. The prior literature acknowledges that Asians often use indirect communication strategies,42–44 which rely on inferred meaning. Nodding and smiling to show respect for authority45,46 are gestures that may be misunderstood as signs of agreement if different meanings are inferred. Moreover, if the patient or family member does not agree with the treatment plan, disagreement may appear indirectly as resistance as it may feel inappropriate to openly disagree with “authority.” 47 Continued dissonance in patient–clinician communication styles and understanding of the patient’s health care wants and needs erodes trust.1,17,48
This finding highlights the importance of the process of involving families in a meaningful way when such involvement is preferred by the patient and feasible. Throughout our study, conversations on “filial piety” arose. However, we are concerned that the limited definition of filial piety as duty and obligation perpetuates the misrepresentation of Asian populations in health research and facilitates the oversimplification of individual health preferences.7,29–32 Our analyses go beyond the filial piety label to illustrate how families show love through advocacy, a finding consistent with a study among Korean patients where a key theme was that families bear the emotional burden of illness by “becoming a ballast in the journey toward death.” 17 Dishonoring this meaningful family act can be a threat to physician–patient trust.
Furthermore, the disclosure of a terminal prognosis is regarded as imperative in end-of-life care in Western medicine, but truth-telling is not a globally shared moral position.2,49 The U.S. health care system’s reliance on the shared decision-making model is grounded primarily on the ethical idea of individual autonomy. 49 In contrast, beneficence and nonmalfeasance are core concepts within the ethical model that is more dominant in Asian cultures, consistent with the collectivist values of relational autonomy.49,50 Family involvement would then be considered much more than “filial piety” if defined solely as duty and obligation. It should be also acknowledged that including family is broadly important to providing palliative care to patients across various cultural backgrounds, but effective approaches may vary depending on the cultural context.20,51–56
Taken together, we ask the reader to consider that the examples of cultural differences highlighted in our study (e.g., communication style, inclusion of family priorities) illustrate how communication, especially in the setting of serious illness, can collide across cultures. Consideration of culture would go beyond knowing about belief systems, values, and expectations 22 but how it impacts the six core functions of health communication, including fostering the patient–family–clinician relationship, exchanging information, responding to emotions, managing uncertainty, making decisions, and enabling patient/family management.25,57 A key theme of our study is the importance of the need for physicians to listen to and learn from patients and families about their process and communication preferences. 23 We argue that this is more than just “cultural humility,” defined as the process of self-reflection to understand and respect cultural differences. Instead, our findings support a need for the clinician communicator to actively flex one’s own cultural framework to become more effective communicators. Our findings suggest that the process starts with “true curiosity” and “really trying to listen to where they are coming from” in order to build trust and then requires clinicians to have practical communication skills that enable them to understand a patient’s desired process of how to communicate and make decisions. This culturally adaptive approach 37 bridges the tension of being both “culture-specific” and “culture-general” in serious illness communication. Cross-cultural education has historically focused on the cognitive activities of asking questions and learning cultural traits that could easily become stereotypes, with less emphasis on attitude and skills. Cultural adaptivity is a process of inquiry, observation, and understanding how sociocultural factors impact health-related behaviors and preferences, all in the service of becoming a more effective patient and family-centered communicator. 58 An adaptive approach is consistent with Bettencourt’s argument that we need “less knowledge” and “more skills.” 58 The participants in this study stressed how resources and additional training to equip clinicians with this method in the United States are sorely needed.
Limitations of this study include a smaller sample size that does not encompass the range of locations, socioeconomic statuses, and cultural differences across the country. This study also utilizes physician perspectives to characterize patient–provider communication in the United States. Further study is needed to understand patient and family experiences. Nevertheless, the study population included individuals from varying locations, health care facilities, cultures and ethnicities, clinical experience, and specialties. Finally, while we did not specify a particular Asian subgroup in the interview guide, we acknowledge that participants’ examples trended toward patients from East Asian populations.
In summary, culture affects both the content and process of communication and decision-making. Our findings from physician interviews about Asian patients in the United States highlight the need for clinicians to be able to communicate in a way that gains alignment on the content for care goals, process on how to discuss care goals, and includes both patient and family priorities on the journey. Our study provides valuable insights into physicians’ adaptive strategies from respondents’ narratives: listen carefully, remain open-minded, be supportive and offer options, leverage engaged family members, use simple and clear communication methods, and take time. Further work to understand and develop clinicians’ skills in these areas is needed to get us closer to reducing disparities in palliative and end-of-life care.
Footnotes
Acknowledgments
The authors would like to acknowledge the participants for their generous contribution of time, insight, and sharing of their experiences for this study. Additionally, the authors would like to acknowledge Dr. Karl Umble for his advice and guidance on this study.
Authors’ Contributions
C.H.: Conceptualization (equal); methodology (lead); data curation (lead); formal analysis (lead); funding acquisition; investigation (lead); project administration (lead); writing—original draft (lead); writing—review and editing (equal); visualization. I.M.Y.: Conceptualization (equal); formal analysis (supporting); writing—review and editing (equal); supervision (equal). F.L.T.: Data curation (supporting); formal analysis (supporting). J.T.: Conceptualization (equal); methodology (supporting); formal analysis (supporting); funding acquisition; writing—review and editing (equal); supervision (equal).
Author Disclosure Statement
J.T. serves as a consultant to CVS Health and CVS Omnicare for work unrelated to this article. C.H. conducted part of this research for her honors thesis as an undergraduate student at the University of North Carolina at Chapel Hill Gillings School of Global Public Health for the Department of Health Policy and Management. C.H. is a research assistant at L&M Policy Research for work unrelated to this article. All other authors have nothing to disclose. The content of this article does not reflect the views of any author’s employer.
Funding Information
This work was supported by the Alexandre Honors Carolina Fund administered by Honors Carolina, an internal grant from the University of North Carolina at Chapel Hill, to C.H. J.T. was supported by K24 AG068300. Funders had no role in study development or implementation.