
Abstract
Purpose:
This study describes human papillomavirus (HPV) vaccination, cervical cancer screening (CCS), and HPV-related knowledge, attitudes, and behaviors among gender diverse adults with a cervix.
Methods:
This was an anonymous online survey of 1096 adults aged 25+ years who were assigned female sex at birth, have a cervix, had not identified as a woman for at least a year, and lived in the United States (U.S.) or Germany. The survey (April–October 2023) collected demographic information, gender identity, and HPV-related knowledge, beliefs, and behaviors, including sexual behaviors, HPV vaccination, and CCS. Descriptive statistics were generated and country differences explored with chi-square and Mann–Whitney U tests.
Results:
HPV-related risk behaviors were common: 42.8% reported penile–vaginal intercourse and 38.1% performed oral–vaginal sex in the past year. Sixty-one percent had had a health care provider recommend the HPV vaccine; 54.7% had been vaccinated. Vaccination was 1.6 times more common in United States (p < 0.001). Unvaccinated U.S. respondents were more likely to believe that they were not at risk for cervical cancer (16.4% vs. 4.8%, p = 0.008). A total of 82.1% had a CCS in their lifetime, but only 64.5% had been screened since last identifying as a woman. CCS barriers centered on concerns about lack of gender-affirming care or discrimination related to gender identity, concerns which were more prevalent in Germany than the United States.
Conclusion:
Despite prevalent HPV risk behaviors, HPV vaccination and CCS rates were low in these gender diverse adults with a cervix, and there were notable country differences. Findings highlight the need for gender-neutral policies and gender-affirming health care practice.
Introduction
Human papillomavirus (HPV) causes both benign and malignant tumors. Cervical cancer is responsible for the greatest HPV-related burden of disease, accounting for more than 300,000 deaths globally in 2022. 1 Until the introduction of HPV vaccination in 2006, when primary prevention of cervical cancer became possible, secondary prevention through cervical cancer screening (CCS) was the only method to prevent invasive cervical cancer. Fourteen years later, in August 2020, the World Health Organization (WHO) launched their cervical cancer elimination initiative with the goal of reducing the cervical cancer incidence rate to less than 4 per 100,000 women worldwide. 2
The research on cervical cancer prevention and elimination is vast. However, the research has focused on cisgender women, leaving deep knowledge gaps on HPV vaccination and CCS among gender diverse people, including transgender men, nonbinary individuals, intersex populations, and other gender-diverse people with a cervix. 2 There are few studies of CCS among these populations3,4 and, as of 2022, none on HPV vaccination. 5 Previous sexual and gender minority research on HPV vaccination has focused on men who have sex with men (MSM) and transgender women, who are not at risk for cervical cancer.5,6 Several countries include MSM and transgender women in HPV vaccination recommendations and financial coverage7,8 but, despite demonstrated appropriateness, 4 no country to date recommends HPV vaccination for gender diverse adults with a cervix who identify differently than “woman.” In response to the dearth of information, in 2021, the WHO called for research on HPV prevention among gender diverse people who have a cervix. 9
The lack of information on HPV prevention among gender diverse people with a cervix remains to be addressed. The aims and purpose of this study were to respond to this call for research and address the recognized lack of information on HPV disease prevention in gender diverse adults with a cervix who do not identify as women. Specifically, this study explored HPV vaccination and CCS behaviors, as well as HPV-related knowledge, beliefs, and risk behaviors among gender diverse adults with a cervix who had not identified as a cisgender woman for at least one year and who lived in the United States (U.S.) or Germany. These countries were chosen as exemplar countries because they were quick to adopt HPV vaccination (2006 in the United States and 2007 in Germany), have expanded vaccination to males and, in the United States, to MSM and transgender women, and both have long-standing CCS programs. However, neither country specifically addresses gender diverse people with a cervix in their HPV vaccination or CCS guidelines.10,11
Methods
Participants and procedures
This was an anonymous online survey study of adults who (1) were at least 25 years of age, as individuals 25 and older with a cervix should have had at least one CCS per United States and Germany screening guidelines,10,11 (2) were assigned female sex at birth, (3) had a cervix at the time they completed the survey, (4) had not self-identified as a cisgender woman for at least 1 year, and (5) lived in the United States or Germany. Inclusion criteria were assessed through self-report at the initiation of the survey. Those who did not meet all inclusion criteria were exited from the survey before answering any research questions. Participants were recruited through targeted advertisement on social media and in partnership with organizations working with sexual and gender minority people using snowball sampling. Recruitment flyers, advertisements, and emails directed people to an anonymous, internet-based survey fielded from April to October 2023 in English in the United States and in German in Germany. Of the 2619 individuals who initiated the survey, 565 (21.6%) did not meet inclusion criteria and were screened out before completing the survey. Of the remaining 2054, 53.9% completed the survey, 98.9% of whom (n = 1096 individuals; n = 945 United States, n = 151 Germany) provided useable data and were included in the study sample.
Informed consent was obtained before survey initiation. This project was deemed exempt (Category 2, anonymous survey procedure) from institutional review board review by Advarra.
Survey measures
The survey, which was developed using previously tested items from large national or previously published surveys,12–16 collected demographic information, sex assigned at birth, presence of a cervix, gender identity, HPV vaccination, and CCS history as well as HPV-related knowledge, beliefs, and behaviors, including sexual behaviors and past diagnoses. The survey was designed so that the initial questions assured that participants met the five inclusion criteria. Current gender was assessed by a “mark all that apply” item that had nine options (Agender, Genderfluid, Gender non-conforming, Genderqueer, Intersex, Man, Nonbinary, Transgender, Woman) as well as the opportunity to specify another gender. Based on the responses, respondents were classified as transgender man, nonbinary, agender, or intersex. The English version of the survey is available in Supplementary Appendix.
Data analysis
Descriptive statistics (mean, standard deviation [SD], median, interquartile range [IQR]) were generated for the overall sample and separately by country. Given the skewed distribution of the data, we report median and IQR instead of mean and SD. Differences between the United States and Germany were assessed with chi-square tests of independence for categorical variables. Mann–Whitney U tests were used to assess differences between the United States and Germany for continuous variables due to skewness. Statistical significance was set at p < 0.05. Analyses were conducted with SAS Enterprise.
Results
The median age was 30 years (IQR: 27–35). Age was higher among U.S. respondents (U.S. median age 30, IQR: 27–36 vs. Germany median age 28 years old, IQR: 26–32, p < 0.001). U.S. respondents were 79.5% Non-Hispanic White, 7.0% non-Hispanic Black, 7.7% Hispanic, 4.2% Asian, 3.3% American Indian or Alaskan Native, and 0.4% Native Hawaiian or Other Pacific Islander. The highest level of education among U.S. respondents was 21.4% high school degree or less, 10.9% two-year college degree, 42.7% four-year college degree, and 18.3% graduate or professional degree. Race/ethnicity and education were not assessed for German respondents.
Gender identity
Table 1 describes respondent gender identity. More than 1 in 10 (10.6%) had never identified as a cisgender woman and another 59.2% had not identified as a cisgender woman for 5 or more years. Nearly three-quarters (72.9%) currently identified as a transgender man, and 5.8% identified as agender. There were significant country differences in gender identification. Regarding current gender identity, German respondents were 1.9 times more likely to currently identify as nonbinary, whereas U.S. respondents were 1.3 times more likely to currently identify as a transgender man (p < 0.001). Although U.S. respondents were more likely to have held their current identity for five or more years (61.2% U.S. vs. 51.0% German, p = 0.01), never having identified as a cisgender woman was 2.8 times more likely among German than U.S. respondents (23.8% German vs. 8.5% U.S., p < 0.001).
Gender Identity Among Adults with a Cervix Who Have Not Identified as a Cisgender Woman for at Least One Year
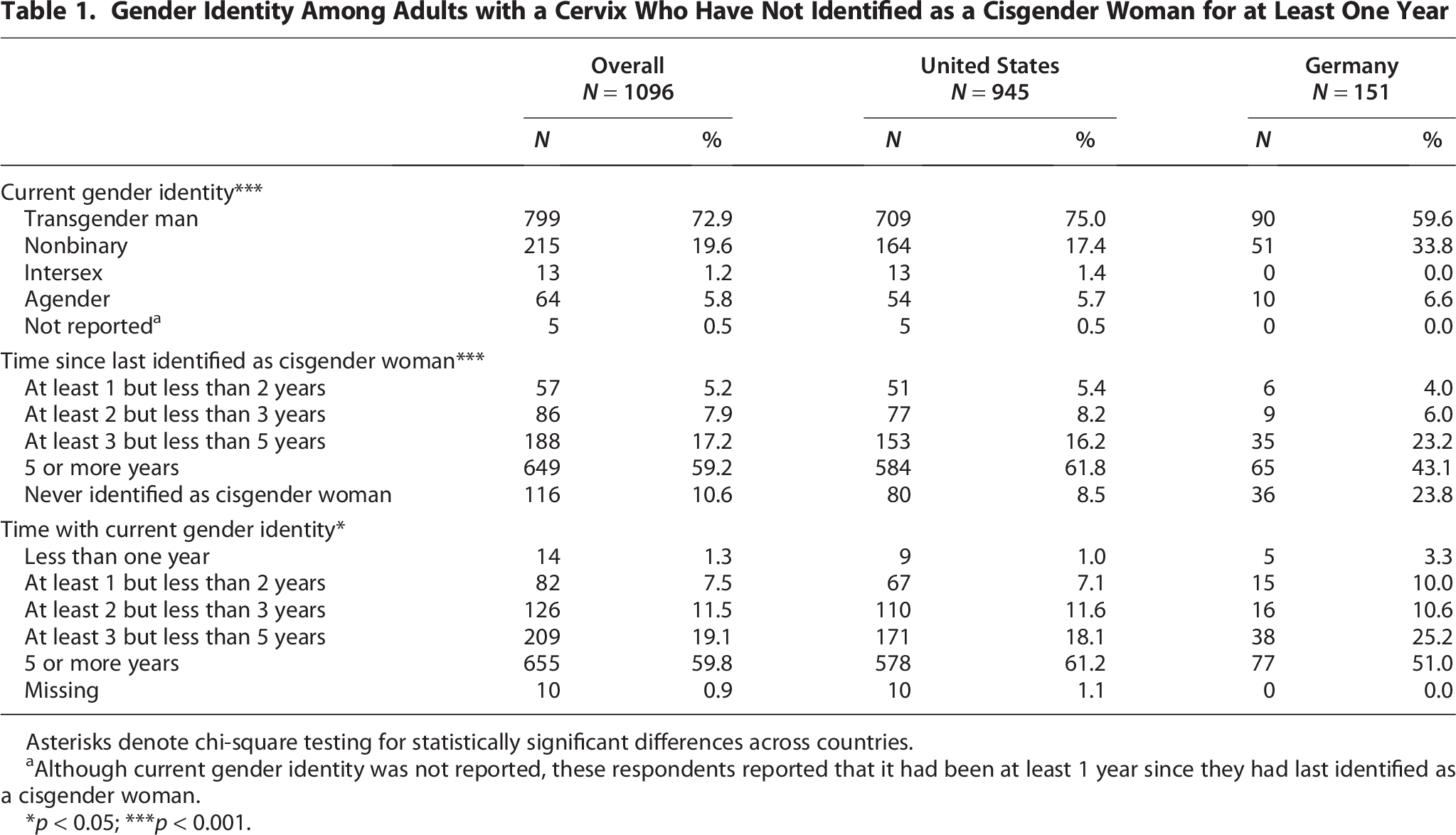
Asterisks denote chi-square testing for statistically significant differences across countries.
Although current gender identity was not reported, these respondents reported that it had been at least 1 year since they had last identified as a cisgender woman.
*p < 0.05; ***p < 0.001.
HPV-related sexual risk behaviors and related diagnoses
HPV-related sexual risk behaviors and related diagnoses are described in Table 2. HPV-related sexual risk behaviors in the past year were prevalent, with 42.8% engaging in receptive penile–vaginal intercourse, 38.3% performing oral–vaginal intercourse, and 18.3% engaging in receptive penile–anal intercourse. U.S. respondents were more likely to engage in receptive penile–vaginal intercourse (44.2% vs. 33.8%, p = 0.01) and receptive penile–anal intercourse (19.3% vs. 12.6%, p = 0.046) than German respondents. There were no significant differences in performing oral sex between U.S. and German respondents. U.S. respondents were thrice more likely to have been diagnosed with HPV than German respondents (13.7% U.S. vs. 4.6% German, p = 0.006).
Human Papillomavirus-Related Sexual Risk Behaviors and Prior Diagnoses
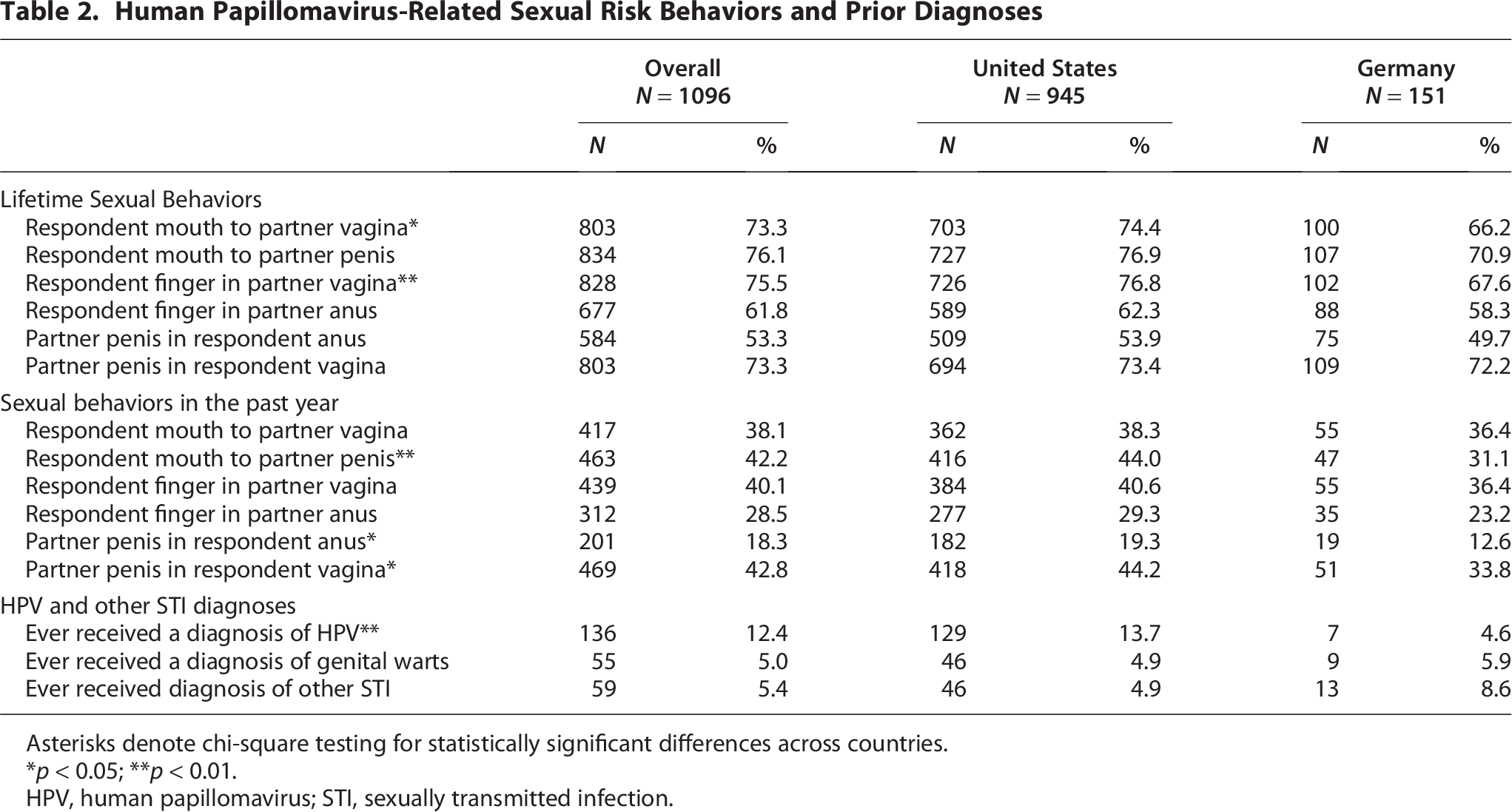
Asterisks denote chi-square testing for statistically significant differences across countries.
p < 0.05; **p < 0.01.
HPV, human papillomavirus; STI, sexually transmitted infection.
HPV awareness, knowledge, and attitudes
Almost all (94.2%) had heard of HPV. HPV awareness was higher in the United States than Germany (95.6% vs. 86.8%, p < 0.001). Among those who had heard of HPV, HPV knowledge was variable (Fig. 1). There was no significant country difference in general HPV knowledge scores (median score = 5). However, U.S. respondents were more likely to correctly answer that people are at risk for new HPV infections even if they had HPV before (68.3% U.S. vs. 49.6% German, p < 0.001). Vaccine-specific knowledge scores were higher among German (median 1, IQR: 1–3) than U.S. respondents (median 1, IQR: 0–2, p = 0.0043). German respondents were more likely to correctly answer that the HPV vaccine might not work as well for people with a previous HPV infection (38.4% vs. 27.2%, p = 0.01) or for people with a history of multiple sexual partners (28.6% vs. 16.0%, p = 0.001) and that the vaccine works better if given before sexual debut (50.9% vs. 25.0%, p < 0.001), whereas U.S. respondents were more likely to correctly answer that HPV vaccination is not useful in treating infections (48.1% vs. 34.8%, p = 0.008).
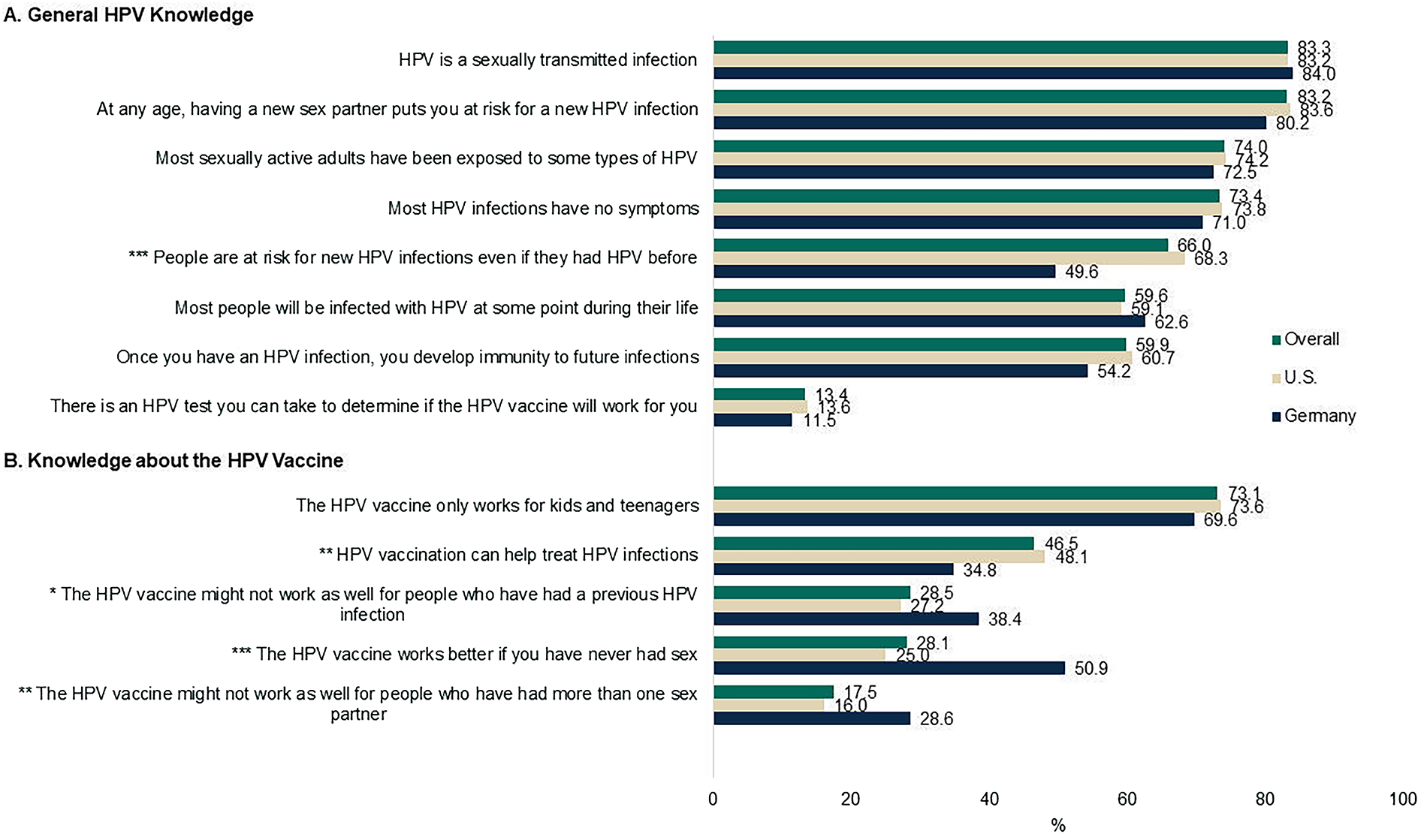
Human papillomavirus-related knowledge. Panel
HPV vaccination and CCS experiences
HPV vaccination experiences are shown in Table 3. Sixty-one percent had received an HPV vaccine recommendation from a health care provider, and 54.7% had been vaccinated (Table 3). U.S. respondents were 1.3 times more likely to report that a health care provider had recommended they receive the HPV vaccine (63.2% U.S. vs. 47.0% German, p < 0.001) and were 1.6 times more likely to have received at least one dose of the HPV vaccine (57.7% U.S. vs. 36.4% German, p < 0.001). Among those vaccinated, the median age of first HPV dose was higher among U.S. than German respondents (18 years [United States] vs. 15 years [Germany], p = 0.001).
Human Papillomavirus Vaccination and Cervical Cancer Screening
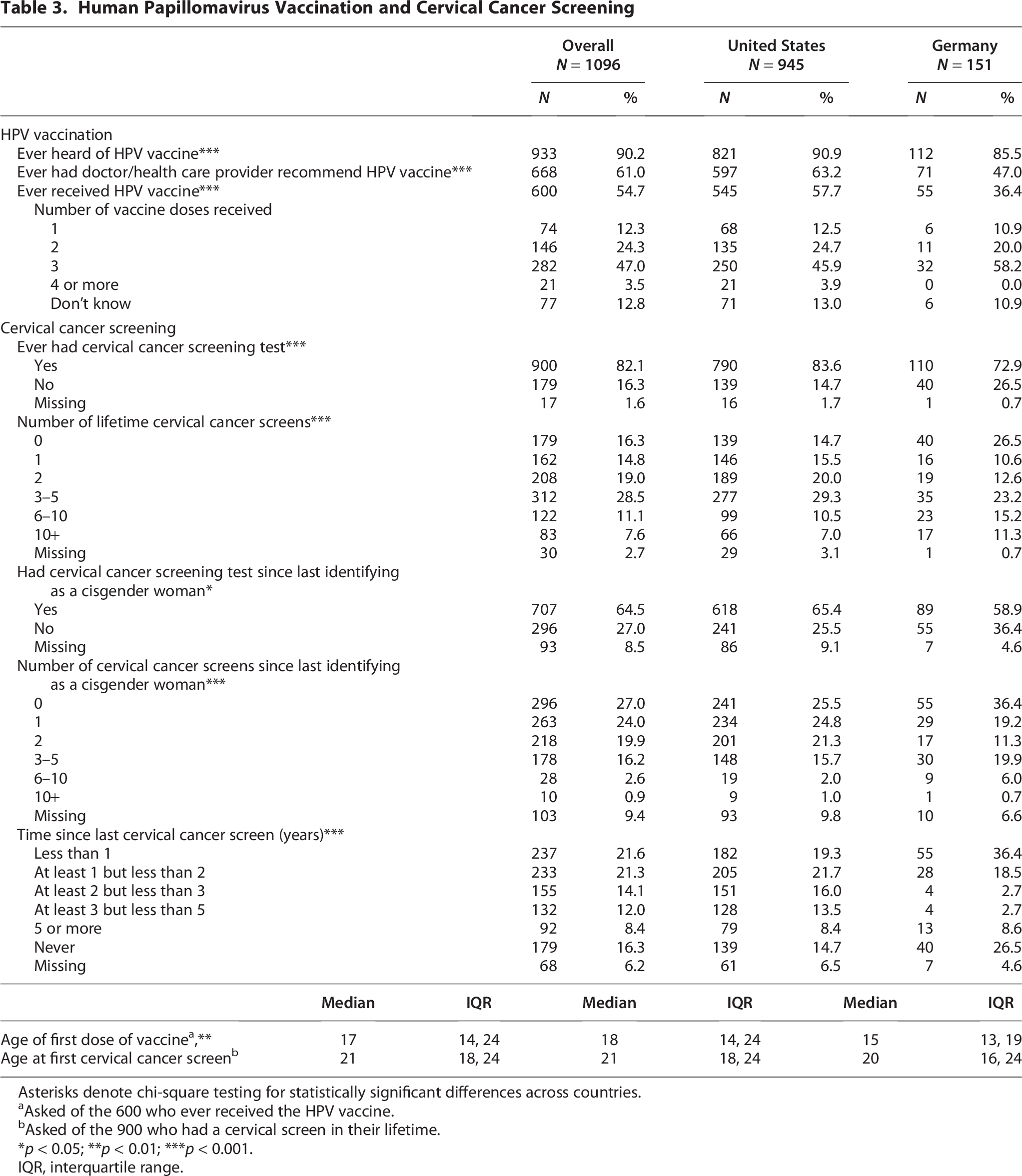
Asterisks denote chi-square testing for statistically significant differences across countries.
Asked of the 600 who ever received the HPV vaccine.
Asked of the 900 who had a cervical screen in their lifetime.
p < 0.05; **p < 0.01; ***p < 0.001.
IQR, interquartile range.
Reasons for not being vaccinated are shown in Figure 2. Not having had a discussion with a health care provider about HPV vaccination was the most frequently cited reason for not being vaccinated, with more than half endorsing this factor. The second most frequently cited reason was not having enough information about the vaccine. There were no country differences in endorsement of these reasons for lack of vaccination. Overall, 13.7% of those who had not been vaccinated did not believe they were at risk for cervical cancer despite still having a cervix; this belief was 3.4 times more prevalent among the U.S. than German respondents (16.4% U.S. vs. 4.8% German, p = 0.008). Unvaccinated U.S. respondents were also more concerned about side effects.
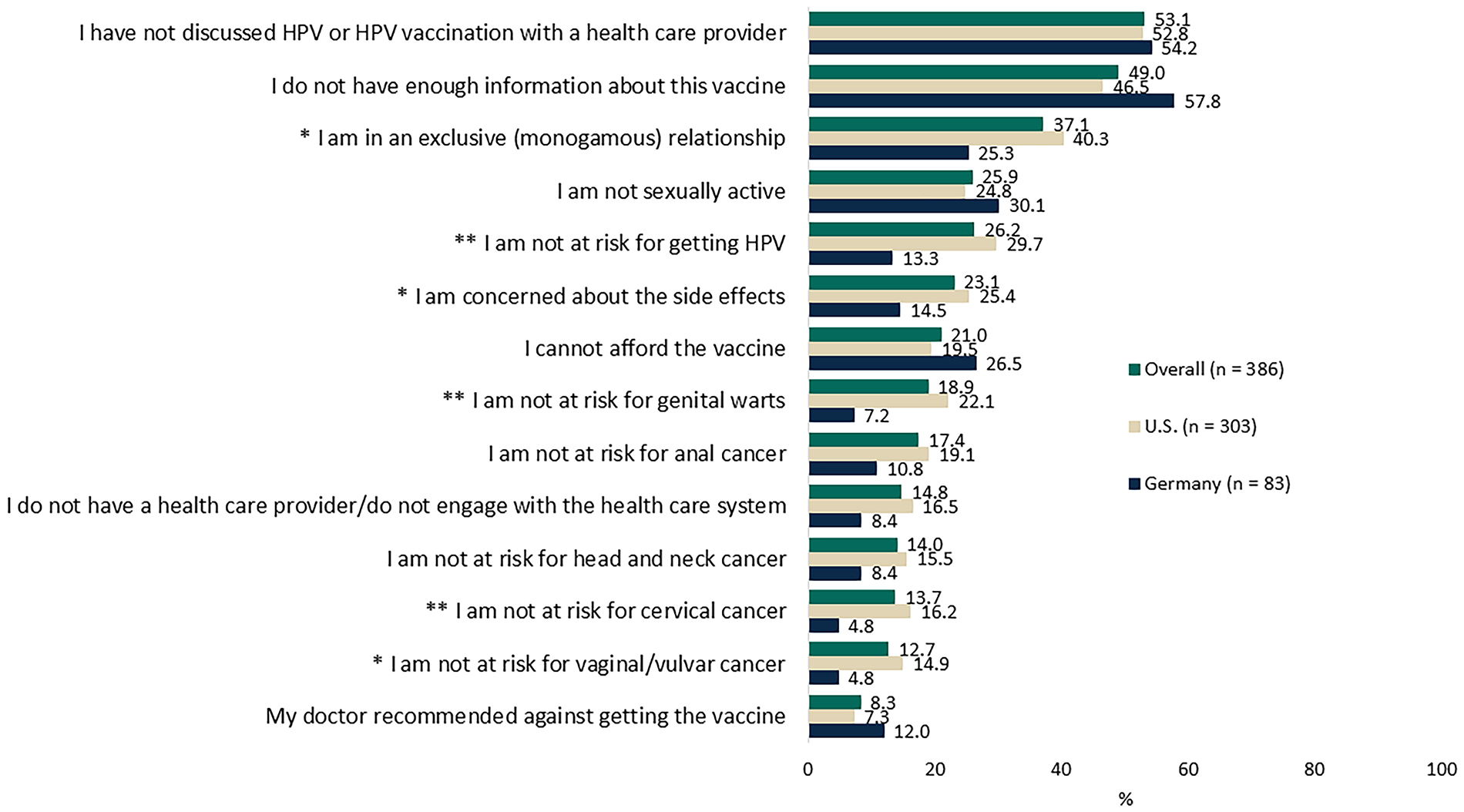
Reasons for not receiving the human papillomavirus vaccine among respondents who reported they were not vaccinated. For each reason, a chi-square test of independence was conducted to assess whether endorsement of that reason differed between the United States and Germany. *p < 0.05; **p < 0.01.
CCS experiences are also shown in Table 3. A total of 82.1% had received at least one cervical cancer screen in their lifetime. Among those who had been screened, average age at first screening was 21.4 years old. Although most had had a lifetime screen, more than one-third had not been screened since last identifying as a cisgender woman. Lifetime CCS was lower among German than U.S. respondents (72.9% German vs. 83.6% United States, p = 0.001), and German respondents were also less likely to have been screened since last identifying as a cisgender woman (58.9% German vs. 65.4% United States, p = 0.01). German respondents were also 1.8 times more likely to never have been screened for cervical cancer (26.5% German vs. 14.7% United States, p < 0.001).
Barriers to CCS were assessed among those who reported no CCS in the past 5 years, including those who had never been screened (Fig. 3). Gender identity-related barriers (Fig. 3B) were more prevalent than barriers unrelated to gender identity (Fig. 3A). The three most common reasons were feeling uncomfortable going to a clinic that primarily serves cisgender women (77.0%), feeling uncomfortable getting screened as their current gender identity (72.3%), and feeling they would be disrespected or mistreated because of their gender identity (65.4%). Feeling shame or embarrassment, which may or may not be related to gender identity, was the fourth most common barrier identified (62.6%). Lack of access to a screening facility (17.9%), transportation (14.9%), insurance coverage (13.6%), or childcare (8.1%) were the least frequently cited barriers.
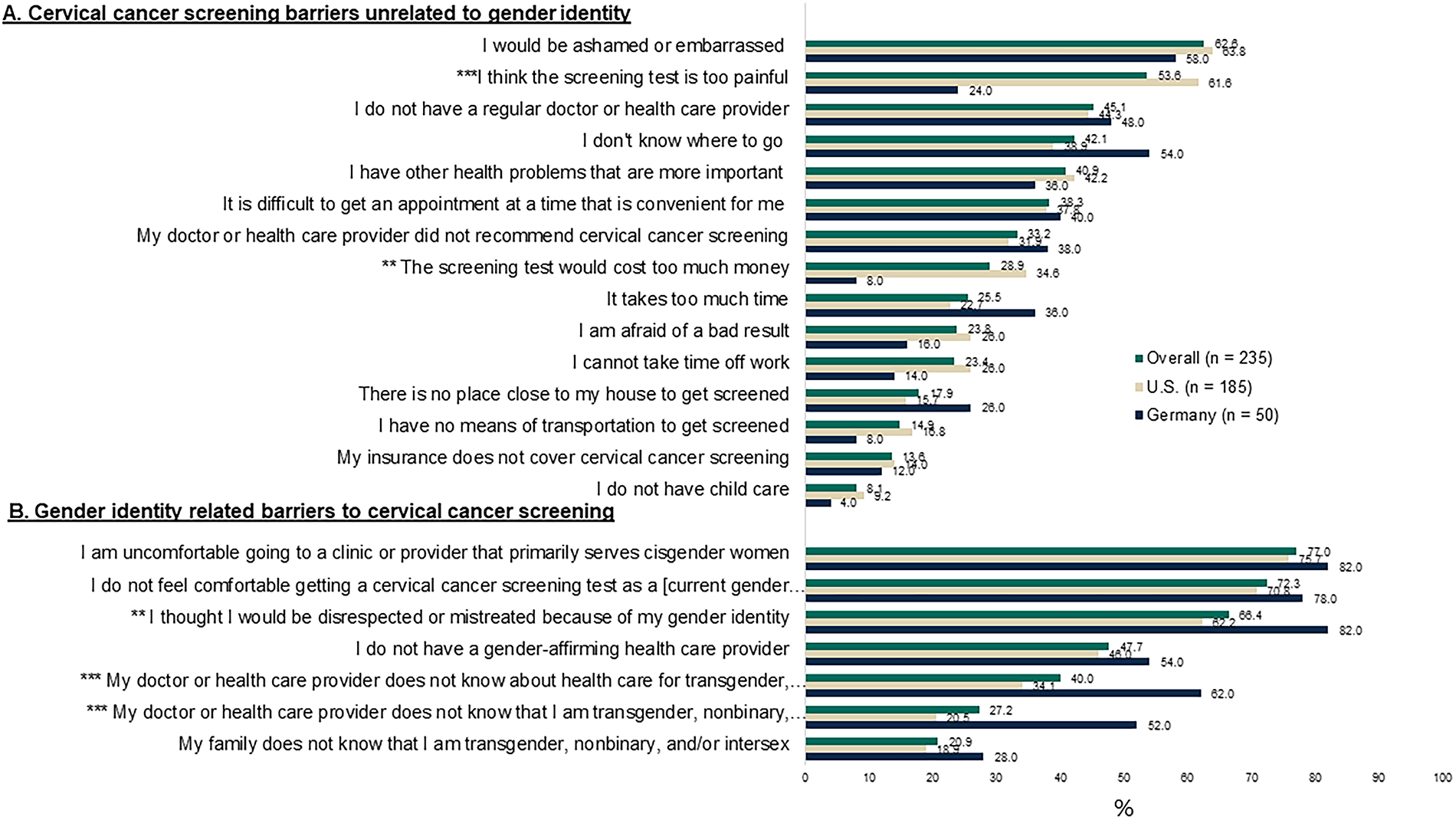
Barriers to obtaining cervical cancer screenings among respondents who have never been screened or had not been screened in the past 5 years. Panel
Country differences in barriers to CCS related largely to the provision of health care (Fig. 3). U.S. respondents were 2.6 times more likely to be concerned about pain and 4.3 times more likely to cite cost as a barrier, whereas German respondents were 1.3 times more likely to cite concern about being disrespected, 1.8 times more likely to cite lack of gender affirming care, and 2.5 times more likely to cite lack of provider awareness of their gender identity as barriers. Although German respondents were more likely to cite nondisclosure of their gender identity to their health care provider as a barrier, there were no country differences in family awareness of current gender identity, which was the least cited gender-specific barrier.
A subgroup of 117 individuals (10.7%) at risk for undetected cervical cancer due to never having received an HPV vaccine and not having had a cervical cancer screen for 5 or more years was identified. Among this subgroup, current identity was 74.1% transgender man, 22.4% nonbinary, 2.6% agender, and 0.9% intersex. For most (62.4%), 5 or more years had elapsed since they had identified as a cisgender woman. A total of 79.5% had never had a CCS test, and only 19.8% had had a doctor recommend they receive an HPV vaccine. HPV risk behaviors were prevalent: 35.9% had engaged in penile–vaginal intercourse in the past year, 17.1% in penile–anal intercourse, and 35.9% had performed oral–vaginal intercourse.
Discussion
This study of a large convenience sample of gender diverse adults with a cervix found that HPV-related risk behaviors were common and spanned gender-stereotypical assumptions of risk. Nearly half of these individuals had engaged in penile–vaginal intercourse in the past year, a behavior which is typically considered a cisgender, “female” risk for cervical cancer, and more than one-third had performed oral–vaginal sex, a behavior which increases risk for oropharyngeal cancer and is stereotypically associated with cisgender males. Although risk behaviors were common, HPV vaccination and CCS rates were low in this population. More than 1 in 10 were neither vaccinated nor screened in the past 5 years, underscoring the need for improved access to HPV prevention for these gender diverse adults who are at risk for cervical and other HPV-related cancers.
Gender diverse people represent a growing population,17,18 but they experience substantial disparities in health and access to care, including barriers to preventive health services such as vaccination and screening.3,19 Most respondents in this study were age eligible, as “females” for HPV vaccination as per their country’s national immunization programs and, if not vaccinated as part of the national immunization program, could access HPV vaccination. HPV vaccination was introduced in 2006 in the United States and 2007 in Germany with female only vaccination. Currently, HPV vaccination is recommended for females and males through age 26 and is available through shared clinical decision making up to age 45 in the United States. In Germany, there is no upper age limit for HPV vaccination for men or women. Despite availability of HPV vaccines, more than one-third of these gender diverse adults with a cervix had never had a health care provider recommend an HPV vaccine and almost half had not been vaccinated, a rate similar to that seen in transgender populations.20,21
Like HPV vaccination, CCS rates were low in these individuals who all had a cervix and were age eligible for CCS as per their countries’ guidelines. Only 57% had had a cervical cancer screen in the past 3 years, a rate lower than that seen for women in these countries. In the United States, 77.1% of women aged 21–44 years had a CCS in the past 3 years, 10 and in Germany, 80% of women are up to date with CCS. 22 Barriers to CCS centered on concerns about lack of gender-affirming care or discrimination related to gender identity, particularly for German respondents. Possible reasons for these disparities, supported by this and other studies, include lack of health care provider training in health issues of gender-diverse people, 23 distrust of the health care system among gender minority individuals, 24 and concerns about safety and confidentiality. 25
These findings highlight the need for gender neutral HPV vaccination and gender inclusive language in policy and practice guidelines for CCS. In its cervical cancer elimination initiative, the WHO calls for 90% HPV vaccination among “girls” and 70% CCS of “women.” 2 Most countries do not provide guidance for CCS in gender diverse populations. In the United Kingdom, individuals with a cervix who are registered with a general practitioner as male are required to request CCS, unlike individuals registered as female, who are routinely invited for CCS. 26 Such cisgender-specific policies raise needless barriers that limit access to HPV vaccination and CCS for gender diverse people at risk for cervical cancer. In contrast, policies which incorporate the needs and preferences of gender diverse people, like enabling self-sampling, could reduce barriers to screening and facilitate access. 27
In addition to highlighting the need for increased inclusivity of HPV policy and practice guidelines, these findings underscore the need for health care providers’ education and training on HPV-related risks and how to provide gender-affirming HPV-related care for this vulnerable population.4,28 Future research could explore the effectiveness of clinical and community-based interventions that address barriers for gender diverse adults with a cervix, with the goal of improving their access to HPV vaccination and regular CCS.
Limitations
There are some important limitations to this study. First, these results reflect the experiences and views of a convenience sample and may not be representative. Second, responses could be subject to recall, desirability, or other reporting biases on the part of participants. Balancing these limitations are several notable strengths. Although this is not a random, representative sample, the survey includes a relatively large number of gender diverse individuals. Several steps were taken to minimize bias due to self-report. Recruitment strategies were implemented in all regions throughout the United States and Germany, and experts were consulted in the selected countries to tailor the survey recruitment strategies. The website and survey were built to ensure anonymity to decrease potential concerns of identity disclosure. Previously tested survey items of knowledge, attitudes, and behavior were used to increase the likelihood that the survey collected valid and reliable data.
Conclusion
This study found that, despite prevalent HPV-related sexual risk behaviors, HPV vaccination and CCS rates were low among these gender diverse people with a cervix. Lack of vaccination and screening places this population at increased risk for cervical cancer, a preventable disease, as well as other HPV-related diseases, especially given documented barriers to accessing health care. These findings highlight the need for gender-affirming care, increased HPV-related education for health care providers caring for such individuals, and gender-inclusive language in policy and practice guidelines. The findings support recommendation and funding for HPV vaccination for gender diverse people with a cervix. Taking these steps may advance health equity and decrease HPV-related disease burden in this vulnerable population.
Authors’ Contributions
E.G.: Conceptualization, funding acquisition, project administration, methodology, supervision, writing—original draft, writing—review and editing, and visualization. A.R.: Methodology, investigation, software, formal analysis, and writing—review and editing. M.A.F.: Conceptualization, methodology, and writing—review and editing. M.E.P.: Methodology and writing—review and editing. G.G.: Methodology and writing—review and editing. D.F.: Methodology, investigation, project administration, funding acquisition, formal analysis, writing—original draft, writing—review and editing, and visualization. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Footnotes
Author Disclosure Statement
E.G., M.A.F., and M.E.P. are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and may hold stock in Merck & Co., Inc., Rahway, NJ, USA.
Funding Information
This work was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.