
Abstract
Background:
Tubal infertility is a major cause of female infertility, necessitating accurate evaluation of fallopian tube patency and fimbrial function. While a laparoscopic dye test (LDT) remains the gold standard, its invasiveness limits clinical use. This study proposes a multimodal hysterosalpingography approach combining four-dimensional (4D) contrast-enhanced ultrasound (4D HyCoSy), two-dimensional color Doppler imaging (2D-CIS), and 2D baseline scanning with saline-infused uterine cavity contrast (2D-FS + SIPS) for noninvasive, comprehensive tubal assessment.
Methods:
A prospective study included 136 infertile patients (242 fallopian tubes) from March 2022 to August 2025. All patients underwent multimodal hysterosalpingography. Diagnostic performance was compared against LDT, and correlations between fimbrial morphology and tubal function were analyzed.
Results:
Multimodal integration significantly improved diagnostic accuracy: sensitivity for patency, partial obstruction, and total obstruction was 93.94%, 85.29%, and 90.7%, respectively, with a specificity of 97.49%, outperforming single-modality examinations (p < 0.05). The addition of 2D-FS + SIPS enhanced visualization of fimbrial structures, increasing detection rates from 34.7% to 62.1% (p < 0.001). Abnormal fimbrial morphology strongly correlated with tubal dysfunction, with abnormality rates rising from 16.9% (patent) to 61.1% (partially obstructed) and 95.1% (obstructed) (p < 0.001). Multimodal evaluation showed 88.6% concordance with LDT (kappa = 0.765), sensitivity of 92.9%, and specificity of 94.4%.
Conclusion:
Multimodal hysterosalpingography provides a noninvasive, one-stop solution for precise evaluation of tubal patency and fimbrial function. It identifies fimbrial pathology as a key factor in distal tubal obstruction, offering valuable insights for etiology diagnosis and personalized treatment of tubal infertility.
Keywords
Introduction
Tubal infertility affects approximately 15% of reproductive-aged couples globally and accounts for 25%–50% of female infertility cases. 1 The fallopian tubes play a critical role in fertilization and embryo transport, making their patency and functional integrity essential for female fertility. Thus, accurate evaluation of both tubal structure and function is crucial in the diagnosis and management of infertility. Although laparoscopy is considered the gold standard for assessing tubal patency, its invasive nature, high cost, and associated anesthetic risks limit its use as a first-line screening tool. 2
Hysterosalpingography (contrast-enhanced ultrasound [HyCoSy]) has emerged as a valuable noninvasive, radiation-free, and real-time alternative for evaluating tubal patency. Transvaginal three-dimensional (3D)/four-dimensional (4D) HyCoSy further improves the visualization of uterine morphology, tubal course, and patency. Studies have demonstrated that 4D-HyCoSy offers superior diagnostic accuracy (95.92%) compared with 3D-HyCoSy (81.63%), along with shorter procedure times and fewer adverse reactions. 3
Despite these advantages, single-modality HyCoSy has limitations. Diagnostic accuracy can be compromised by factors such as bowel gas interference, variations in tubal anatomy, and contrast reflux—particularly in the assessment of distal tubal lesions and fimbrial function. Recent advances in multimodal hysterosalpingography, which integrates imaging from multiple angles and parameters, have been shown to enhance diagnostic precision and reliability. 4
In this prospective study, we analyzed clinical data from 128 infertile patients to compare the diagnostic outcomes of multimodal imaging—combining 4D-HyCoSy, dual-amplitude imaging (2D-CIS), and two-dimensional baseline scanning with saline-infused pseudocontrast (2D-FS + IPS)—against laparoscopic results. We aimed to test the hypothesis that the combination of 4D-HyCoSy and 2D-HS significantly improves diagnostic accuracy for tubal patency and fimbrial pathology, thereby contributing to a noninvasive and precise functional assessment of the fallopian tubes.
Materials and Methods
Study population
This prospective study enrolled 136 infertile patients (mean age: 28.5 ± 4.2 years; mean infertility duration: 3.1 ± 1.8 years) at the Reproductive Center of the First Affiliated Hospital of Fujian Medical University between March 2022 and August 2025. All examinations were performed 3–7 days after menstruation, with patients abstaining from sexual intercourse prior to the procedure. Data on infertility history, medical history, and prior pelvic surgeries were collected.
Inclusion criteria
Primary or secondary infertility lasting ≥1 year. Requirement for tubal patency assessment or postoperative evaluation.
Exclusion criteria
Acute or subacute reproductive tract inflammation or tuberculosis. Malignant tumors of the reproductive tract. Systemic or infectious diseases. Infertility due to male or endocrine factors. Ongoing menstruation or vaginal bleeding. Pregnancy or known allergy to ultrasound contrast agents.
Equipment
A GE Voluson E10 ultrasound system equipped with a RIC5-9 4D transvaginal probe (frequency range: 2.5–5.0 MHz) and contrast-specific imaging software was used. The mechanical index was set between 0.04 and 0.07, with a volume angle of 120° and a fan angle of 179°.
Contrast agent
SonoVue® (sulfur hexafluoride, Bracco International B.V.; 59 mg per vial) was used as the ultrasound contrast agent. Each vial was reconstituted with 5 mL of normal saline and agitated to form a microbubble suspension. A 2 mL aliquot was then diluted with 18 mL of saline prior to use.
Examination procedure
Patients were placed in the lithotomy position. After routine disinfection, a uterine catheter was inserted, and the balloon was inflated with 1.5–2 mL of saline to secure it above the internal cervical os. 2D and 3D baseline scans were performed to visualize the uterine cavity and adnexa.
Real-time 4D hysterosalpingography (4D-HyCoSy) was initiated while slowly injecting the contrast agent. The infusion process—including uterine cavity filling, tubal transit, and pelvic spill—was dynamically observed. Using the contrast-specific imaging mode (2D-CIS), the distribution of contrast in the fallopian tubes and around the ovaries was tracked. Imaging time, flow direction, tubal diameter, and fimbrial spill were recorded.
Subsequently, the 2D-FS + IPS technique was applied to assess fimbrial morphology, mobility, and relationship with adjacent tissues. Injection resistance and patient discomfort were monitored throughout the procedure. Contrast reflux prompted immediate cessation. Postexamination records included contrast volume, reflux occurrence, and adverse reactions. Patients were observed at rest for approximately 30 minutes after the procedure.
Diagnostic criteria for multimodal hysterosalpingography
4D-HyCoSy
Tubal patency and fimbrial morphology were assessed based on injection resistance, contrast reflux, tubal filling pattern, fimbrial spill, and the degree of pelvic dispersion.
2D-CIS mode
Dual-amplitude contrast imaging (2D-CIS) was used to quantify the time from contrast injection to fimbrial spill: <30 seconds indicated patency, 30–60 seconds indicated partial patency, and >60 seconds indicated obstruction.
4D-FS + SIPS mode
After saline infusion into the pelvic cavity, morphological features of fimbrial spill were observed to assess tubal function.
Integrated multimodal assessment
In all modes (4D-HyCoSy, 2D-CIS, and 2D-FS + SIPS), the following criteria were applied:
Patency: Minimal injection resistance and negligible reflux. Partial obstruction: Mild resistance and slight reflux, with contrast still advancing. Complete obstruction: Significant resistance and marked reflux.
Contrast spill time was quantified consistently across modalities (<30 seconds: patent, 30–60 seconds: partial obstruction, and >60 seconds: obstruction). Diagnostic criteria are summarized in Table 1 and Figure 1. 5
Classification of Tubal Patency Based on Multimodal Hysterosalpingography (4-Dimensional Contrast-Enhanced Ultrasound, 2-Dimensional Color Doppler Imaging, and 2-Dimensional Baseline Scanning with Saline-Infused Uterine Cavity Contrast) Findings

2D-CIS, two-dimensional color Doppler imaging; 2D-FS + SIPS, two-dimensional baseline scanning with saline-infused uterine cavity contrast; 4D-HyCoSy, 4-dimensional contrast-enhanced ultrasound.

Multimodal hysterosalpingography (4D-HyCoSy and 2D-FS + SIPS) evaluation of tubal patency and fimbrial morphology.
Gold standard: Laparoscopic dye test
Laparoscopic methylene blue tubal perfusion (laparoscopic dye test [LDT]) served as the reference standard. 6 Two senior gynecologists, blinded to ultrasound results, jointly evaluated:
Tubal patency
Patent: No resistance to 10–20 mL methylene blue infusion, with free spill from fimbriae. Partial obstruction: Increased resistance and mild reflux but minimal spill after clamping the contralateral tube and increasing pressure. Complete obstruction: Significant resistance, marked reflux, and no spill or only localized tubal staining.
Fimbrial morphology
Normal: Open, mobile, with complete mucosa and active fimbriae. Abnormal: Mucosal defects, fibrosis, adhesion, or scarring.
Statistical analysis
Data were analyzed using SPSS 26.0. Diagnostic performance was evaluated using McNemar’s test, kappa consistency analysis, and ROC curves. A two-tailed p < 0.05 was considered statistically significant.
Ethical approval and quality control
The study was approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University (approval no.: [2021] 429). All participants provided written informed consent. The authors guarantee that all methods are performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki). To ensure reliability, ultrasound examinations were performed independently by two physicians with ≥5 years of experience in reproductive ultrasound. Imaging results were evaluated in a double-blind manner, with disagreements resolved by a third senior specialist. Laparoscopic videos were jointly reviewed by two gynecologists to ensure diagnostic consistency.
Results
Imaging characteristics of multimodal hysterosalpingography
Multimodal hysterosalpingography, incorporating 4D-HyCoSy, 2D-CIS, and 2D-FS + SIPS, was employed to evaluate tubal patency, course, and fimbrial morphology.
Patent group
In 4D-HyCoSy, the fallopian tubes exhibited natural motility with continuous contrast filling. Contrast agent spilled from the fimbriae within 10–30 seconds, presenting a petal-like opening pattern (Fig. 2A). 2D-CIS imaging demonstrated rapid and uniform periovarian diffusion of the contrast (Fig. 2B). 2D-FS + SIPS further revealed soft, well-defined fimbriae without periadnexal adhesions. The contrast flowed freely between the fimbrial folds in multiple streaming patterns (Fig. 2C,D).

Imaging features of fallopian tubes assessed by multimodal hysterosalpingography (4D-HyCoSy, 2D-CIS, and 2D-FS + SIPS).
Partially obstructed group
4D-HyCoSy showed tubular dilation, tortuosity, or kinking in the mid-to-distal segments, with delayed contrast spillage (Fig. 2E). 2D-CIS imaging revealed contrast retention within the tube and only faint arc-like diffusion around the ovary (Fig. 2F). 2D-FS + SIPS indicated that although some fimbriae remained pliable, adhesions restricted contrast outflow to a single narrow stream resembling a “fine line” (Fig. 2G), suggesting localized fimbrial adhesion.
Obstructed group
4D-HyCoSy demonstrated a “truncation sign” at the distal tube with no contrast spill (Fig. 2H). 2D-CIS revealed significant intraluminal contrast retention; the tubal course was often displaced from the ipsilateral ovary due to pelvic adhesions, with no periovarian diffusion (Fig. 2I,J). 2D-FS + SIPS clearly depicted fimbrial structures encased and fixed by fibrous adhesions, with marked morphological distortion, confirming adhesion as the etiology of tubal obstruction (Fig. 2K).
HyCoSy unimodal and multimodal joint diagnostic results
In this study, 136 infertile patients were initially enrolled, which included 5 patients with a unicornuate uterus and 9 patients with a history of unilateral salpingectomy due to ectopic pregnancy. This provided a total of 258 fallopian tubes for assessment. Based on the LDT as the gold standard, 165 tubes were classified as patent, 34 as partially obstructed, and 59 as obstructed. The obstructed group included 16 tubes from 8 patients with bilateral obstruction. Because the subsequent 2DHS-SIPS examination could not be performed for patients with bilateral tubal obstruction, these 8 patients (16 tubes) were excluded from the final comparative analysis. Consequently, data from a total of 242 fallopian tubes were analyzed. The diagnostic concordance rates for tubal patency assessment using 4D-HyCoSy alone were 83.64% (138/165) for patent, 61.76% (21/34) for partially obstructed, and 74.42% (32/43) for obstructed tubes. The combination of 4D-HyCoSy and 2D-CIS improved concordance to 89.09% (147/165), 67.65% (23/34), and 81.40% (35/43), respectively. The multimodal approach (4D-HyCoSy + 2D-CIS + 2D-FS + SIPS) demonstrated the highest concordance: 93.94% (155/165) for patent, 85.29% (29/34) for partially obstructed, and 90.70% (39/43) for obstructed tubes (Table 2).
Contrast-Enhanced Ultrasound Single-Modal and Multimodal Joint Diagnosis Results. Unit: Bar

HyCoSy single-modal and multimodal joint diagnostic performance
Using LDT as the reference standard, the multimodal combination (4D-HyCoSy + 2D-CIS + 2D-FS + SIPS) achieved a sensitivity of 90.70% and a specificity of 97.49% for evaluating overall tubal patency. The specificity, accuracy, and positive predictive value of the multimodal approach were significantly higher than those of 4D-HyCoSy alone or the combination of 4D-HyCoSy and 2D-CIS (all p < 0.05). In contrast, no statistically significant differences were observed in sensitivity or negative predictive value among the different diagnostic modalities (p > 0.05), as detailed in Table 3.
Diagnostic Efficiency of Contrast-Enhanced Ultrasound Single-Modal and Multimodal (%, [n/m])

Compared with 4D HyCoSy + 2D + 2DHS-IPS.
*p < 0.05.
Fimbrial visualization: 4D-HyCoSy alone versus combined with 2D-FS + SIPS
After excluding tubes with severe fimbrial displacement or distortion due to pelvic adhesions from the initial 242 tubes, 219 tubes were eligible for fimbrial evaluation. The addition of 2D-FS + SIPS to 4D-HyCoSy significantly enhanced the fimbrial display rate across all patency categories compared with 4D-HyCoSy alone (p < 0.001). In the patent group, the rate increased from 52.5% to 73.2%; in the partially obstructed group, from 23.8% to 66.7%; and in the obstructed group, from 4.4% to 19.5%. The overall fimbrial visualization rate improved markedly from 34.7% to 62.1%, demonstrating the substantial value of the combined technique in assessing fimbrial morphology and mobility, crucial for evaluating pelvic adhesive disease (Table 4).
Display Rates of 4-Dimensional Contrast-Enhanced Ultrasound and 2-Dimensional Baseline Scanning with Saline-Infused Uterine Cavity Contrast on the Fimbrial End of Fallopian Tubes. Unit: Bar

Indicates the number of difficult finger-like protrusions on the fimbriae of some fallopian tubes, excluding those with obstruction in the proximal and middle segments and severe pelvic adhesions.
Correlation between fimbrial lesions and tubal dysfunction
A strong correlation was observed between the status of the fimbrial structure and the degree of tubal dysfunction. The abnormality rate of the fimbriae was lowest in the patent group at only 16.9%. This rate increased significantly to 61.1% in the partially obstructed group and further to 95.1% in the obstructed group. The differences in fimbrial abnormality rates between the patent group and the two dysfunctional groups were statistically significant (p < 0.001), indicating that fimbrial pathology is a critical factor in tubal functional impairment, particularly in cases of distal obstruction (Table 5).
Finger-Like Protrusions at the Umbrella Ends of Each Group in 2-Dimensional Baseline Scanning with Saline-Infused Uterine Cavity Contrast Mode
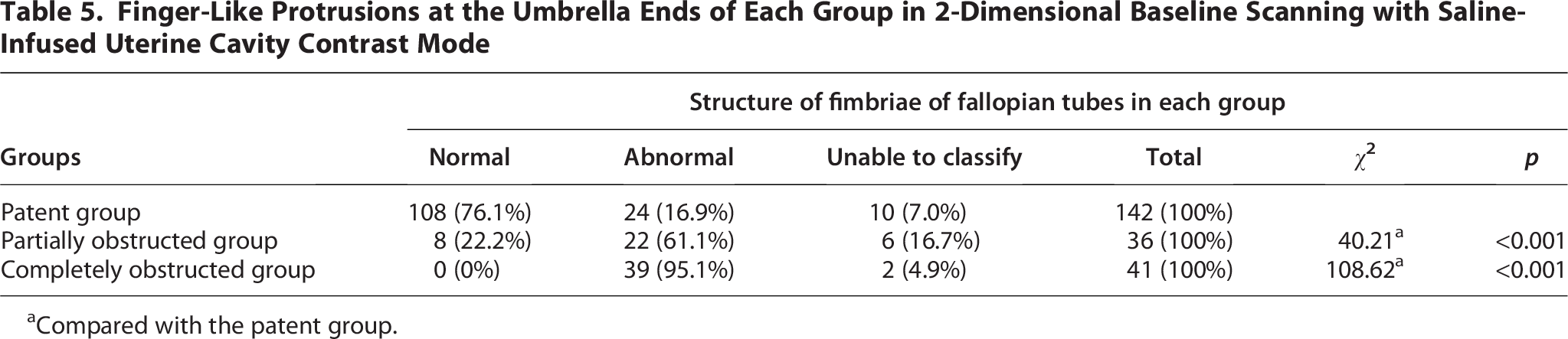
Compared with the patent group.
Diagnostic efficacy for fimbrial structure using 4D-HyCoSy + 2D-CIS + 2D-FS + SIPS
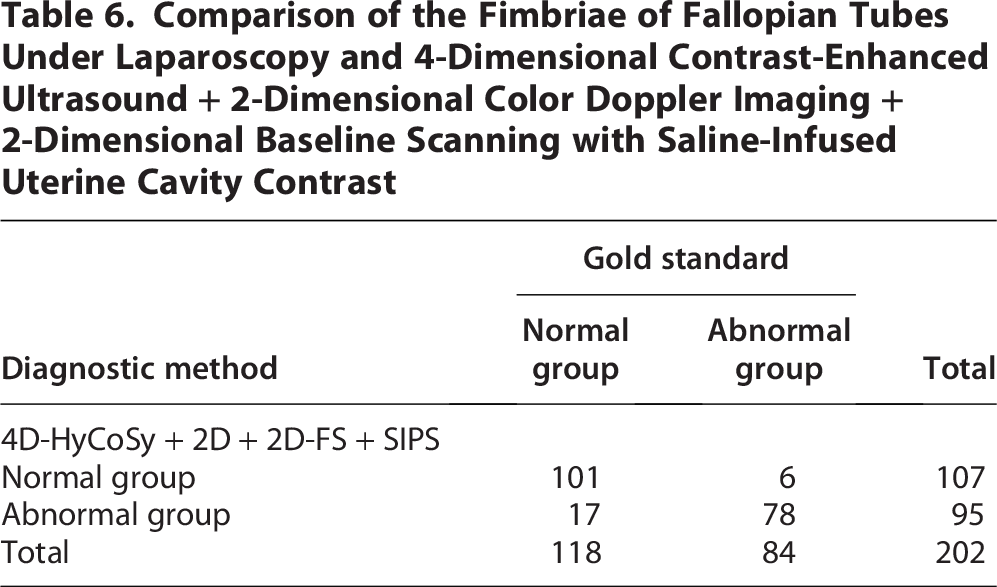
For the 202 fallopian tubes where the fimbrial structure was clearly visualized by the multimodal approach, LDT results identified 118 as normal and 84 as abnormal. The multimodal evaluation showed an overall concordance of 88.6% with LDT, with a sensitivity of 92.9%, a specificity of 94.4%, a positive predictive value of 92.9%, and a negative predictive value of 85.6%. The agreement with the invasive gold standard was substantial (kappa = 0.765), confirming that this noninvasive multimodal method is a reliable and accurate alternative for the clinical evaluation of fimbrial morphology (Table 6).
Comparison of the Fimbriae of Fallopian Tubes Under Laparoscopy and 4-Dimensional Contrast-Enhanced Ultrasound + 2-Dimensional Color Doppler Imaging + 2-Dimensional Baseline Scanning with Saline-Infused Uterine Cavity Contrast
Discussion
This study systematically evaluated fallopian tube patency, course, and fimbrial morphology using multiple imaging modalities, including 4D-HyCoSy, 2D-CIS, and 2D-FS + SIPS. The results demonstrate that a multimodal HyCoSy approach offers significantly superior diagnostic performance compared with any single modality alone, particularly in assessing tubal patency and fimbrial anatomy. A detailed analysis of imaging characteristics under different tubal conditions—patent, partially obstructed, and obstructed—provides more precise imaging evidence for diagnosing tubal infertility.
The multimodal strategy (4D-HyCoSy + 2D-CIS + 2D-FS + SIPS) achieved high diagnostic accuracy (93.94% in the patent group, 85.29% in the partially obstructed group, and 90.7% in the obstructed group) and specificity (97.49%), underscoring the synergistic effect of combining complementary imaging techniques. 7
While 4D-HyCoSy provides valuable 3D dynamic imaging of tubal motility—revealing features such as tubal thickening, tortuosity, or rigidity that may suggest reduced tubal function—it cannot definitively distinguish whether such morphological changes reflect true pathology or normal anatomical variation in the presence of brisk contrast spill. This limitation highlights the importance of integrating additional modalities. For instance, combining 2D-FS with SIPS (or similar techniques such as S3D-HS or D3D-HS) enables detailed evaluation of fimbrial morphology, relative position to the ovary, and mobility, as well as the pattern of contrast spillage (e.g., multistream vs. thread-like), offering a more functional assessment of the fimbriae. 8
The structural and functional integrity of the fimbriae is critical for ovum pickup, and accurate grading of distal tubal damage is essential for diagnosis and treatment planning. 9 In clinical practice, mild fimbrial adhesions or peritubal adhesions may be managed with fimbrioplasty or adhesiolysis, with postoperative natural pregnancy rates reaching up to 50%. In cases of severe fimbrial obstruction, salpingectomy or proximal tubal occlusion followed by in vitro fertilization is often recommended. 10 Our prospective study confirms that the 2D-FS + SIPS technique significantly improves the visualization of fine fimbrial structures, increasing the overall detection rate from 34.7% to 62.1%. Moreover, the rate of fimbrial abnormalities rose sharply with worsening tubal patency—from 16.9% in the patent group to 61.1% in the partially obstructed group and 95.1% in the obstructed group—supporting the strong association between fimbrial pathology and distal tubal dysfunction.
Multimodal hysterosalpingography represents a shift from assessing mere tubal “patency” toward evaluating “functional status.” While 4D-HyCoSy allows indirect assessment of tubal course and fimbrial morphology, 2D-FS + SIPS directly visualizes fimbrial architecture and contrast spill patterns, reflecting the functional adequacy of the fimbrial opening. This integrated approach effectively overcomes the limitations of single-modality imaging, consistent with current trends in diagnostic imaging development. 11
Our findings establish a clear quantitative relationship between fimbrial pathology and tubal dysfunction. The steep gradient in fimbrial abnormality rates across patency categories provides compelling evidence that fimbrial adhesions, fibrosis, or fixation are central to the pathophysiology of tubal obstruction, particularly at the distal segment. This underscores a conceptual evolution in tubal assessment from luminal patency to overall functional integrity. 12 The multimodal protocol used in this study—especially 2D-FS + SIPS—offers a noninvasive means to evaluate fimbrial morphology and mobility, aiding in individualized treatment planning. High sensitivity (92.9%) and specificity (94.4%) with substantial agreement with LDT (kappa = 0.765) support its reliability as an alternative to invasive laparoscopy.
Notably, diagnostic performance varied by obstruction site: sensitivity and specificity for proximal obstruction were 91.0% and 93.0%, respectively, with a positive predictive value of 68.5% and negative predictive value of 98.4%. For distal obstruction, sensitivity was lower (69.9%), though specificity remained high (96.8%), likely due to greater anatomical complexity and variability in distal tubal course. These findings align with previous work by Lanzani et al., 9 reinforcing the clinical utility of multimodal ultrasound in locating tubal pathology.
This study offers a standardized, one-stop noninvasive protocol for the etiological assessment of infertility. Limitations include its single-center design and the need for a larger sample size. Although multimodal imaging improved fimbrial visualization, severe pelvic adhesions causing significant tubal displacement or distortion still pose diagnostic challenges. 13 Technical factors such as injection pressure or patient discomfort may also induce tubal spasm, a known cause of false-positive obstruction. 14 Preprocedural counseling, use of antispasmodics, gentle technique, and shorter examination times may help mitigate these issues.
Future integration of artificial intelligence for automated fimbrial recognition and contrast flow quantification could further objectify diagnosis and enhance reproducibility, 15 paving the way for more precise, operator-independent tubal evaluation.
The high concordance with LDT and the noninvasive nature of the multimodal exam support its utility as a first-line screening and triage tool. Based on our findings, we propose the following practical management algorithm: (1) Bilateral Patency on Multimodal Testing: Patients can proceed with timed conception attempts for 6 months without immediate recourse to LDT. (2) Unilateral Patency: Management can focus on ovulation monitoring on the patent side for 6 months. If conception does not occur, LDT is then recommended for definitive diagnosis and potential therapeutic intervention (e.g., chromopertubation and adhesiolysis). (3) Bilateral or Unilateral Obstruction: LDT should be directly recommended. In these cases, LDT serves the dual purpose of confirming the diagnosis and allowing for simultaneous therapeutic intervention if needed. So multimodal hysterosalpingography can effectively stratify patients. It provides a reliable, noninvasive method to identify those with a high likelihood of patency who can defer surgery, while rigorously selecting those for whom diagnostic/therapeutic LDT is clearly indicated, thereby optimizing resource use and patient care pathways.
Conclusion
In conclusion, multimodal hysterosalpingography combines the strengths of various imaging modalities to provide a comprehensive and precise assessment of the fallopian tubes—from macroscopic patency to microscopic fimbrial function. This integrated approach not only improves diagnostic accuracy but also enables noninvasive and detailed evaluation of fimbrial morphology and activity, elucidating the critical role of fimbrial pathology in tubal dysfunction. As such, it offers valuable imaging insights for the etiological diagnosis, personalized treatment planning, and prognostic evaluation of female infertility, underscoring its significant potential for broad clinical adoption.
Authors’ Contributions
L.X. contributed to the conception of the study, data acquisition, wrote the article, and approved the final version. X.L., H.L., L.H., T.Z., and W.W. provided assistance for data acquisition analyses. L.G. and L.X. contributed to analysis and article preparation.
Footnotes
Acknowledgments
The authors would like to appreciate the researchers who participated in their study and also the nurses who helped in the process.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The present study was funded by the Fujian Provincial Science and Technology Plan Guiding Project Fund, No. 2022Y0013.