
Abstract
Background:
Rurality is a risk factor for metastatic breast cancer (MBC), mediated by factors such as distance to treatment centers and screening access. Coordinating optimal timing of genetic, genomic, and other advanced testing to identify next-line therapies and expand access to clinical trials is crucial. This qualitative study explored factors that patients with MBC consider when choosing a treatment location, and barriers and facilitators to referral between facilities.
Materials and Methods:
Thirteen patients and four clinicians from rural settings completed semistructured interviews. Transcripts were analyzed using NVivo software and deductive coding guided by the Health Equity Implementation Framework. Codes from transcripts were analyzed for themes or barriers and facilitators to referral.
Results:
We identified five themes describing factors involved in treatment location decision-making: distinctive features shaping rural care experiences, care preferences formed across multiple levels of influence, decisions based on position within cancer survivorship, splitting care between facilities based on care type, and differing priorities for those receiving local care vs. traveling to a comprehensive cancer center. We identified seven barriers to referral: incomplete communication, outdated/incompatible medical record systems, lack of awareness of options, military insurance requirements, procedural requirements of referral institutions, timeliness, and travel. Facilitators included formal/informal collaboration between institutions, support from clinicians, common electronic medical record systems, and patient self-advocacy.
Conclusions:
This study sets the foundation for characterizing factors that influence where rural patients receive care and works toward providing patient-centered care, focusing on decreasing travel burden and optimizing referral between local and distant options.
Keywords
Introduction
A growing number of women are living with Stage IV, or metastatic breast cancer (MBC), in the United States, and by 2025, nearly 170,000 women will have MBC in the country. 1 The complex management of MBC often includes coordinating care to provide optimal timing of genomic, genetic, and other testing to identify next-line therapies and expand access to clinical trials to potentially improve outcomes. 2 However, despite numerous and evolving treatment options, no “gold standard” exists, and outcomes remain poor, with a 5-year survival rate of 30%. 3
Impact of rurality on MBC patient care
Rurality is a risk factor for MBC, mediated by factors such as distance to treatment centers and screening access.4,5 Rural status exacerbates the already present demands of MBC management, including more time traveling, inpatient care, and higher financial toxicity than patients with earlier-staged breast cancer.6,7 As survival often depends on ongoing access to high-level care, there is a need (1) for clinicians to provide individualized plans that consider unique disease presentation, account for rural status, and address psychosocial needs and (2) to explore how women from rural settings navigate these barriers when making treatment and facility decisions.
Rural patients also experience the burden of navigating the referral process.7,8 Receiving treatment at National Cancer Institute (NCI) designated and/or academic facilities can provide specialized treatments (e.g., anti-HER2, immunotherapy, hormonal therapy), access to clinical trials, and improved outcomes for women with breast cancer.9–11 Deciding where to receive treatments and potentially seeking a second opinion on the diagnosis, prognosis, and proposed regimen that are initially given to patients may impact health outcomes. However, potential benefits must be weighed against the logistical and financial burdens faced by rural patients in accessing these facilities. While existing studies have explored referral patterns for palliative care for patients with MBC, a significant knowledge gap exists regarding the experiences of those who are responding positively to treatments and may need referrals for reasons other than end-of-life care.12,13 Elucidating these experiences is crucial for developing patient-centered care models that address the unique needs of rural patients with MBC throughout survivorship.
Study aims and significance
This study examines the multilevel factors that influence health care decisions and referral experiences of rural patients with MBC. We sought to identify:
Factors that impact treatment facility choice. Barriers and facilitators to referral between institutions for patients and their clinicians.
By identifying these factors, we aimed to inform the development of more effective care coordination models that can improve outcomes and quality of life.
Materials and Methods
Preliminary work
We previously adapted a multilevel collaborative care model between an National Cancer Institute (NCI) designated comprehensive cancer center (CCC) and referring community hospitals with the goal of improving MBC care coordination (Project ADAPT). 14 We used the Exploration, Preparation, Implementation, and Sustainment framework to assess acceptability and satisfaction with the existing referral process.15,16 We shared findings with key individuals involved in referral, outlined processes and clinical flow, and incorporated adaptations in real time. The preliminary findings provided rationale to further investigate the additional structural, individual, and contextual influences on facility choice, care coordination, and referral reported by participants—specifically for patients in rural settings. Therefore, in this study, we applied a determinant framework to clarify the multilevel influence on implementation missing from the Project ADAPT approach.
Multilevel model needed to evaluate this complex system
We applied the Health Equity Implementation Framework (HEIF) 17 to guide our evaluation. HEIF incorporates the Integrated-Promoting Action of Research Implementation in Health Services 18 and the Health Care Disparities Framework 19 and effectively explains factors related to disparities and the uptake of a health care innovation. HEIF centers on the Clinical Encounter while integrating Innovation Characteristics (coordinated care models), Recipient Factors (patient and clinician motivators for facility selection), Medical Context, and Social Influence (sociopolitical forces, health care infrastructure). This multilevel approach is ideal for identifying barriers and facilitators to rural MBC care and referral.
Study design
We used a qualitative descriptive approach to explore the experiences of rural patients with MBC and their clinicians. We employed the standards for reporting qualitative research checklist to ensure methodological rigor and transparent reporting. 20 Washington University School of Medicine Institutional Review Board approved the study procedures (IRB#202309027).
Recruitment
We recruited English-speaking adults (≥18 years) with MBC who self-identified as rural, representing diverse races, ethnicities, and treatment pathways (CCC only, community hospital only, or both). Patients were recruited via tumor registry, social media, and snowball sampling. Community hospital clinicians with MBC treatment and referral experience were recruited via email and snowball sampling. All participants completed eligibility screening via cold call, email, or REDCap. 21
Data collection
We developed semistructured interview guides for patients and clinicians, informed by HEIF domains (see Supplementary Data), to gather data on decision-making, facility preferences, and referral experiences. A qualitative researcher with >10 years of experience (A.J.H.) oversaw the guide development and trained the team to conduct interviews. Clinician interviews addressed treatment discussions, referral circumstances, and their role in referrals. Patient interviews explored treatment decision-making, facility preferences, and referral experiences (if applicable). All interviews were conducted individually over Zoom (video conferencing platform), starting with informed consent review and verbal consent documentation. Interviews concluded with a sociodemographic survey and lasted up to 60 minutes. Participants were compensated with a $50 gift card for their time.
Analysis
Audio recordings from interviews were transcribed verbatim through a professional transcription service. The interviewer reviewed each transcript and manually de-identified it before analysis to ensure accuracy. Transcripts were coded using QSR NVivo 12.
Two coders (R.R., A.J.H.) tested the first codebook iteration using a clinician transcript. After revising the master codebook (see Supplementary Data), the remaining transcripts were divided between two coders (R.R. + M.E. or R.R. + S.L.). Coders met regularly to review independent coding and reach consensus. Once all transcripts were coded, R.R. and S.L. categorized relevant data as either facilitators or barriers to referral using HEIF domains and reviewed them together to reach consensus.
In the next level of analysis, the team identified the embedded and interconnected relationships within and across codes. They met regularly throughout data collection and analysis phases to provide feedback and data interpretation.
Results
Fifty-nine potential participants were identified via various recruitment methods: social media (n = 33), tumor registry (n = 25), and snowball sampling (n = 1). A research coordinator completed a screening assessment with 24 of these individuals. Fifteen met eligibility criteria, but one declined. Thirteen of the 14 scheduled interviews were completed; 1 interview (PID#14) was incomplete due to technical difficulties and excluded. Participants experienced multiple care pathways as described in Table 1, and indicated in parentheses next to patient ID numbers throughout the main text. The mean age was 50.5 years (range: 33–80). Eleven self-identified as non-Hispanic White, one as non-Hispanic Pacific Islander, and one as non-Hispanic Black.
REACH Patient Pathways
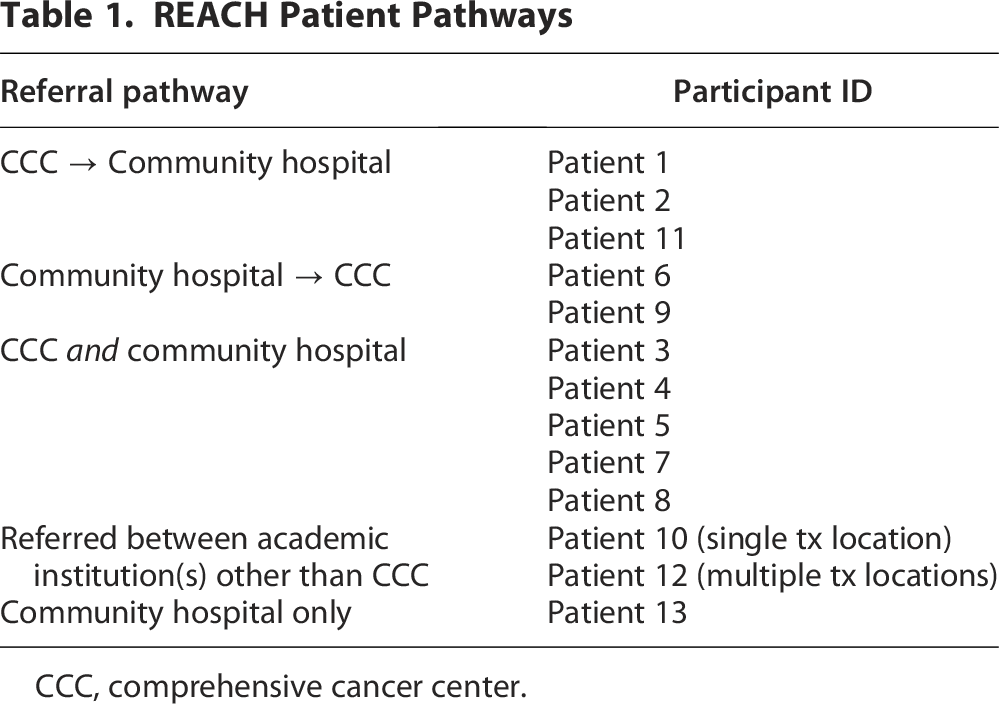
CCC, comprehensive cancer center.
Four eligible clinicians completed an online screening assessment via REDCap and were interviewed. All were non-Hispanic White women. Clinicians’ roles were breast surgeon, registered nurse, nurse practitioner, and nurse coordinator, who all worked in the context of breast cancer. Their mean employment duration at their institutions was 10.5 years (range: 2–21).
From the 17 transcripts (13 patients and 4 clinicians), we identified five themes relating to rural women diagnosed with MBC, treatment facility selection, and referral process between the CCC and community hospitals.
Theme 1. Individual, clinical, and community features shape rural care experiences
Clinicians cited a higher prevalence of older patients seeking care in their rural communities, while younger patients opted for urban locations:
“… I think younger patients are definitely more willing to travel… older patients are gonna be more content to stay locally. Younger patients, especially in the metastatic setting are gonna be more willing to travel. They probably have a little bit easier time traveling. Maybe not financially, but it’s easier to get in and out of the car. It’s easier to park. It’s easier to get from the parking garage into the building.”—Clinician#2
Geographical dispersion of services was a central aspect of rural life described by participants. Younger patients anticipated additional transportation requirements and appeared to nonchalantly describe distance and time spent traveling to everyday necessities, including their treatment visits, as was the case with this 33-year-old participant:
“… so I don’t feel like it’s that big of a deal to drive 45 minutes away, but that’s because that’s a normal thing for me. If we need to go downtown for anything, it’s going to be a 45-minute drive.”—Patient#12 (referred and received care simultaneously between multiple academic institutions other than CCC)
While rural patients suggested they commonly accept these travel demands, clinicians noted some patients appeared hesitant to travel or did not realize the burden associated with traveling to receive care at the CCC:
“They don’t understand what that means. They don’t realize it’s a two-hour drive. I have people who won’t even drive on [rural highway] because it’s a highway that’s 4 lanes, let alone get on [urban highway] … they just assume there’s like a bus or something that goes there.”—Clinician#1
Another defining feature was limited health care infrastructure in rural communities. Some patients described resource gaps in rural health care, identifying supports necessary for ongoing treatment as more often available in urban centers:
“We actually do not have a hospital. The closest is [city], so it’s 45 minutes to an hour. There are no oncologists in the town or anything associated with oncology that I could go to, for appointments or anything like that”—Patient#13 (received care from community hospital only)
“My neurology care is in [major city] now because we don’t have a local neurologist, which is one downside to a smaller town. I had to go to [CCC]”—Patient#3 (received care simultaneously from CCC and community hospital)
Theme 2. Care preferences are formed across multiple levels of influence
Patients desired patient-centered care reflecting their priorities, beliefs, and circumstances influenced by individual values, clinical encounter dynamics, health care structures, and rural social determinants of health (SDOH).
At the individual level, patients varied between accepting the chronic nature of their diagnosis and seeking out options to improve their outlook. While some patients remained with ongoing maintenance care, others actively sought out clinical trials or complex treatments to potentially improve their health outcomes and preferred clinicians who prioritized and respected their wishes:
“I just wanted the best treatment I could possibly get, and I wanted a team that all believed in the same way as I did… just because I have metastatic breast cancer doesn’t mean it’s an automatic ‘We don’t treat this.’ I wanted a team behind me that was 100 percent on board of treating and curing it, not just maintaining it.”—Patient#12 (referred and received care simultaneously between multiple academic institutions other than CCC)
At the Clinical Encounter level, patients emphasized the importance of clinician knowledge, compassion, and honest communication. While some valued a clinician’s bedside manner, others prioritized clinical expertise: “I don’t need you to have good bedside manner; just do your job well. It doesn’t bother me if you’re not friendly. But if you’re a great brain surgeon, fine.”—Patient#3 (received care simultaneously from CCC and community hospital).
At the systems level, factors within treatment facilities shaped patient preferences. Patients appreciated in-network care options, use of common electronic medical record systems, a welcoming atmosphere, and consistent collaboration between clinicians. One patient stated, “I liked that they were all willing to come together and coordinate between each other to make sure it all happened correctly for what I needed.”—Patient#12 (referred and received care simultaneously between multiple academic institutions other than CCC).
Facility characteristics elicited contrasting preferences. Some patients were drawn to the prestige and reputation of urban medical centers, while others valued personalized culture and convenience of local facilities. Several patients equated large hospital size with superior care, while others prioritized the intimate atmosphere and accessibility of smaller community centers:
“It’s not a big-built place … I can be walking from the lab over to the doctor’s office and I’ll see one of the nurses. And they usually stop and speak. And even when I go from the doctor’s office to the treatment center, it’s all in one building. It’s all on one floor, I can drive myself, and the people are really nice.”—Patient#5 (received care simultaneously from CCC and community hospital)
At the societal level, SDOH like health insurance policies/requirements and social networks operated beyond patients’ control yet significantly impacted decision-making and quality of care received. One patient employed by the military described her experience:
“What I would expect from [military hospital] is—and Tricare, more specifically—to not continuously try to have all of my healthcare done there and flat-out refusing with the right of first refusal. I think that’s what Tricare called it, um, to have me solely seen there at that hospital. And it takes, like, an act of Congress to be able to be seen at a specialty hospital such as even [community hospital] in [city] or out there with you guys in [major city].” —Patient#2 (was referred from CCC to community hospital)
Another explained the impact of a state-level decision to remove coverage from her insurance:
“I felt like Medicaid had put a nail on my coffin ‘cause I was wondering, how am I gonna afford treatments, any medication? ‘Cause they took part D away. It was gone … it has been a challenge ‘cause … bills and prescriptions and all that kinda things.”—Patient#7 (received care simultaneously from CCC and community hospital)
This participant also highlighted how support groups influenced decision-making but were only accessible online due to their rural location:
“Well, I have Facebook groups, and I’m on this group that wants to meet, I guess, in [state] somewhere… they’re gonna keep me in the loop, but I think it’s gonna be north of here, like, by [major city], which is, like, four hours from here.”—Patient#7 (received care simultaneously from CCC and community hospital)
Theme 3. Rural patients with MBC treatment decisions differ based on where they are in their survivorship
We identified three distinct phases in the MBC care trajectory, each characterized by different decision-making priorities and needs: (1) diagnosis, including screening, diagnostics, and treatment plan conversations following diagnosis; (2) treatment, which can include the first year or several years aimed at controlling cancer spread and size; and (3) maintenance, when established treatment regimens are integrated into the patient’s ongoing care plan, focusing on long-term disease management and quality of life.
Patients often described the Diagnosis Phase as overwhelming due to the flood of important and sometimes unfamiliar information and perceived urgency to begin treatment quickly:
“So the day I found a lump verse the day I found out I had metastatic breast cancer was over a 10-day period. So they pretty much got in there as fast as I possibly could and got it all figured out, and I really didn’t have much time of thinking. It was more just we’re going to figure out what’s going on.”—Patient#12 (referred and received care simultaneously between multiple academic institutions other than CCC)
The Treatment Phase was marked by adapting and evaluating care options for effectiveness. It involved patients trying different recommended treatments to establish a long-term plan:
“I’m just moving forward on that level of care about that situation… So it’s just decisions about continuing to be a patient and getting more and more [laughter] healthcare ‘cause you really just wanna stop. You just wanna, like, get your [treatment] and go on with your life.”—Patient#3 (received care simultaneously from CCC and community hospital)
In this phase, patients were most likely to seek second opinions, especially when treatments became ineffective, or they felt uncertain about their provider(s):
“When we really originally looking for the [CCC] trials, that was when we got told we were out of options. So we started searching heavily. Then I’m seeing this doctor and she’s like, ‘Oh, well, we do have other options still.’ I still have two other treatments that I can try. And so I think we plan on trying those as long as it goes with the trials well enough.”—Patient#10 (received care from academic cancer center other than the CCC)
The Maintenance Phase represented a transition to long-term disease management, marked by biological remission and/or psychological acceptance of ongoing treatment:
“Everything has been good… in a year I didn’t have anything that showed up on the scans… And so, she said if it hadn’t reared its ugly head in two years, it’s probably not coming back to my breast. ”—Patient#1 (referred from CCC to community hospital)
Maintenance often triggered reevaluation of care locations. Upon entering this phase, several patients opted to seek local care due to the convenience and ongoing nature of treatment.
Theme 4. Rural patients with MBC sought to split their care between facilities based on type of care
Some patients maintained specialized treatment at academic hospitals while obtaining imaging and routine care at local community hospitals. Patient 3 described her preference to receive specialized treatment at the CCC:
“I wanna keep my foot in the door at [CCC] so I can be a continuing patient. So, if something comes back in my brain, I can get a gamma knife. I have been there twice before. I am keeping that relationship going.”—Patient#3 (received care simultaneously from CCC and community hospital)
Another patient described her approach: “The radiologist up there, I just told him I would do all my appointments here, just because it is close. But other than that, I’ll still do all my treatments at [CCC].”—Patient#4 (received care simultaneously from CCC and community hospital).
Theme 5. Priorities differ for those receiving care locally vs. traveling to the CCC
We identified two distinct patient participant groups with contrasting priorities: (1) patients who chose exclusively local care and (2) patients who committed to traveling to a CCC. For local-care patients, geographical, logistical, and social considerations preceded perceived benefits of receiving care at the CCC:
“The reason I have stayed there is because it’s the closest facility for me. And I have children. … And I’m active in work. And, it’s easier than driving the two hours to [major city]”.—Patient#13 (received care from community hospital only)
“It seemed like [at the CCC] you were a number. You come in, you da-da-da, you’re done. Here, they seem like they actually care whether you come or not.”—Patient#11 (referred from CCC to community hospital)
This group of patients indicated that only the prospect of a cure would motivate them to travel significant distances for care:
“Interviewer: Under what circumstances would you ever consider getting treatment far away from home again? Patient 11: I guess the promise of a cure.”—Patient#11 (referred from CCC to community hospital)
Conversely, CCC-exclusive patient participants prioritized perceived quality and institutional reputation above all other factors:
“Interviewer: Can you tell me more about [why you prefer to drive the extra distance]?
Patient 8: Well, I think just like reputation and just feel more comfortable being at [city]. You know, you kind of hear things about some of the other hospitals, not even necessarily with oncology, but just stories that I’ve heard from people and I’m like, “I’ll just go to [city]. It’s worth the extra-the extra drive.”—Patient#8 (received care simultaneously from CCC and community hospital)
Barriers and facilitators of the referral process
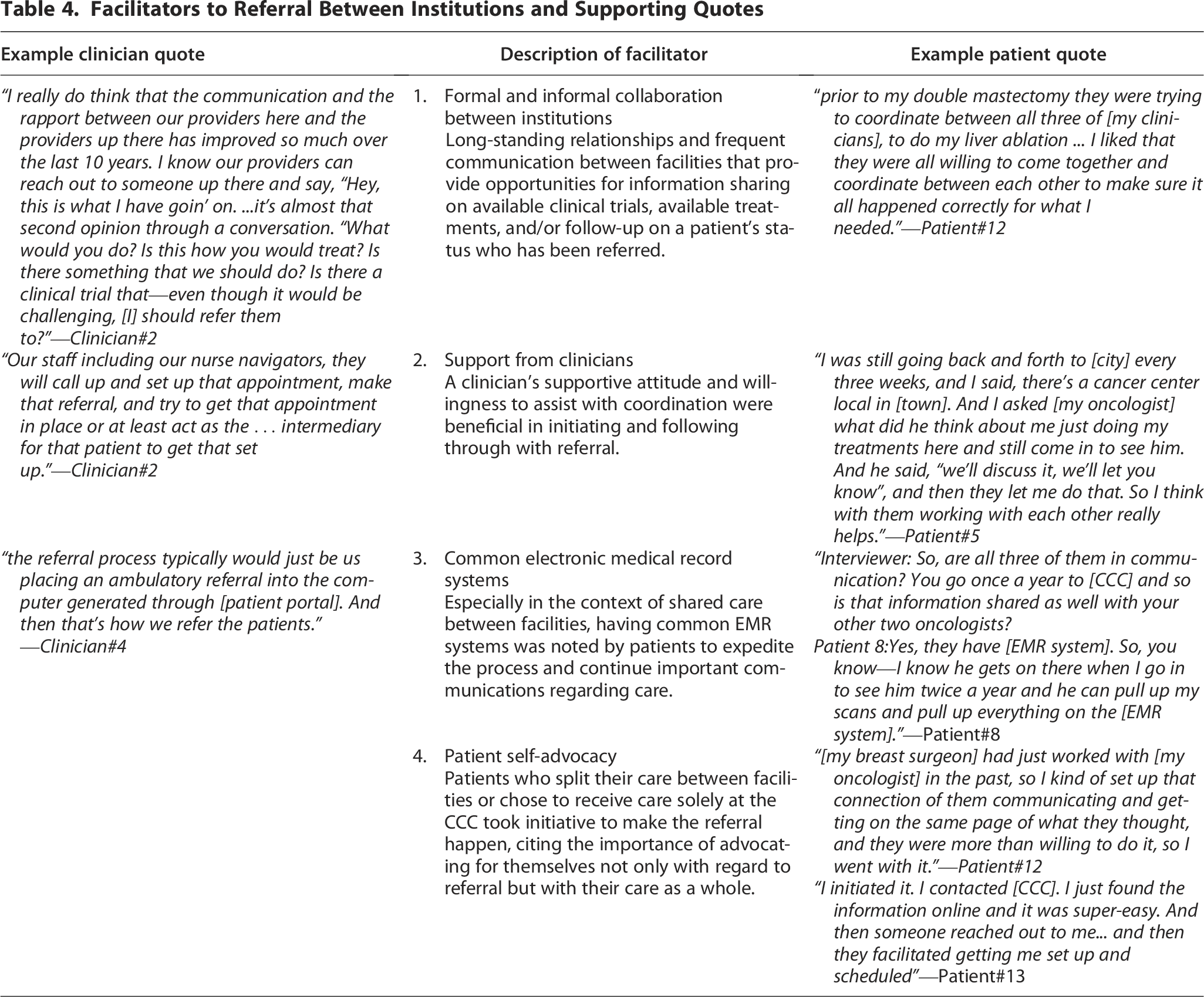
Multiple scenarios caused referrals between facilities (Table 2). We observed seven barriers (Table 3) and four facilitators (Table 4) to referral. A key methodological finding was that several barriers (3, 4, and 5) and facilitators (4) were supported exclusively by either patient or clinician quotes.
Scenarios That May Initiate Referral Between Facilities

Barriers to Referral Between Institutions and Supporting Quotes

Facilitators to Referral Between Institutions and Supporting Quotes
We mapped the barriers onto relevant HEIF domains to identify intervention points (Fig. 1). We found that most barriers (1, 2, 5, and 6) fall within the Societal Context domain, which encompasses the outer and inner settings of institutions (i.e., referral and referring facilities) and organizational structures and systems. Of the remaining barriers, barrier 3 falls within the Clinical Encounter, barrier 4 falls within Societal Influence, barrier 7 falls within Recipient Factors.

Barriers to referral adapted from the HEIF domains. Barriers to the referral process have been color-coded and mapped onto relevant HEIF domains to identify intervention points. Most barriers (1, 2, 5, and 6) are within the Societal Context domain, which encompasses the outer and inner settings of institutions and organizational structures and systems. The remaining barriers are within the Clinical Encounter (3), Societal Influence (4), and Recipient Factors (7). The figure demonstrates how these 7 barriers get in the way of the referral process. HEIF, Health Equity Implementation Framework.
Discussion
Our findings reveal a complex decision-making process that rural patients with MBC navigate when selecting care facilities and to balance competing priorities, including quality of care, travel burden, and personal values. These decisions evolve throughout the patient’s cancer journey, reflecting changing needs and responses to treatments.
The most common reasons for receiving local care included geographic proximity (saving time and resources) and relationships with clinicians and staff. This aligns with existing studies that highlight the financial toxicity of MBC treatment,22–24 travel burden on rural patients with breast cancer, 25 and unique care experience that a community hospital can provide.26,27
Our results highlight the distinct phases in the MBC survivorship (diagnosis, treatment, and maintenance), each associated with different decision-making priorities. Many patients who positively responded to treatments over an extended period transferred select (Patients 3, 4, 5, 7, 8) or all (Patients 1, 2, 11) treatments to a local community hospital. For these patients, the phase of their current disease greatly impacted their decision about where to receive care. While the concept of cancer survivorship phases is documented elsewhere with varied definitions for each phase,28–30 formal recognition could enable delivery of more relevant care option discussions, particularly regarding referral. Future research should investigate the impact of survivorship phases on other care-based decisions, such as intervening at opportune moments during the Maintenance Phase.
Patients receiving care at the CCC were willing to travel regardless of their phase of cancer survivorship or, at the very least, maintained specialized treatments there due to the location’s perceived reputation. Sholevar et al. studied “Institutional Transference,” where patients idealize academic cancer centers, traveling far distances in search of state-of-the-art treatments. 31 We noted that reputation was assumed due to the facility’s size and volume or inferred through others (e.g., previous clinicians, family, friends, or other patients with breast cancer). Few studies have assessed the impact of perceived reputation on care preferences and quality of life. The significance of a CCC’s reputation—especially for rural patients—should be further explored, as it seems to influence satisfaction.
The strategic approach that many rural patients with MBC adopted by splitting their care between facilities was a novel finding of this study. This balancing act—weighing high-quality care with logistical ease—highlights the sophisticated decision-making that rural patients employ to meet their complex needs. Collaboration between clinicians across facilities was noted by patients to be a facilitator to splitting aspects of their care between sites. This finding challenges the traditional binary view of care location decisions and suggests that health care systems develop more flexible, coordinated care models that formally support this hybrid approach.
The barriers we identified—including incomplete communication, outdated medical record systems, lack of awareness of options, insurance requirements, procedural requirements, timeliness, and travel burden—represent actionable targets for system-level interventions. The quality of communication between the CCC and community hospitals was a barrier to some participants but a facilitator to others, which warrants further investigation. This finding lends to the ad hoc nature of relationships between clinicians at community hospitals and those from the CCC. From our interviews, these relationships appear to be individually generated rather than standard practice. A coordinated care model may help to address this, moving the responsibility for establishing efficient and ongoing relationships from individual clinicians to the system level. We also found that several barriers and facilitators were reported exclusively by either patients or clinicians, underscoring the importance of incorporating both perspectives when designing referral processes. Alongside the preliminary work completed through Project ADAPT, we will seek to implement improved referral processes for patients with MBC, aiming for timely access to clinical trials and reduced burden. Our findings show that most barriers to effective referral exist at the Societal Context level, suggesting interventions focused on organizational structures and systems may yield the greatest improvements in care coordination.
The number of participants recruited despite the rarity of MBC and smaller populations of rural communities was a strength of this study. The semistructured interview style promoted the patient voice in our design, conduct, and analysis. Participants offered a diverse set of care pathways and perspectives, adding to the breadth of our findings.
This study is not without limitations. We recruited a small sample of clinicians with experience providing MBC care and referral. A larger sample size may have resulted in a richer dataset. However, the data from these four clinicians help demonstrate the clinical structures and systems involved in referral, provide perspective on the rural patient experience, and provide key multilevel insights into the barriers and facilitators to referral relevant to HEIF.
Conclusion
For rural patients with MBC, deciding where to receive treatment carries more weight given the chronic nature of their disease, access to treatment facilities, and frequency of visits throughout survivorship. Guided by HEIF, this inquiry examined the multilevel factors that rural patients with MBC consider when choosing a facility and the barriers and facilitators to referral between a CCC and external hospitals. These findings provide a basis for defining what patient-centered care means for rural patients with MBC that face unique challenges and how to deliver it through streamlined referral processes.
Footnotes
Acknowledgments
The authors would like to express our sincere gratitude to all the participants who shared their time and experiences to contribute to this study.
Authors’ Contributions
R.R.: Writing—original draft, writing—review and editing, project administration, investigation, formal analysis, data curation, and visualization. S.L.: Writing—original draft, data curation, and formal analysis. M.E.: Writing—review and editing, investigation, project administration, data curation, and formal analysis. A.G.: Writing—review and editing. S.H.: Data curation and writing—review and editing. A.B.A.: Supervision and writing—review and editing. L.L.P.: Supervision, funding acquisition, and writing—review and editing. A.J.H.: Supervision, conceptualization, methodology, funding acquisition, validation, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This resarch was funded, in part, by the Siteman Cancer Center Siteman Investment Program Bernard Research Fund, “Characterizing Rural Metastatic Breast Cancer Care: A Qualitative Analysis” to A.J.H., PI. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health or other funding agencies.
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.