
Abstract
Background:
Multiligamentous knee injuries are complex, with highly individualized treatment plans based on patient and injury-specific factors. Stress radiographs are an important tool for objectively quantifying knee laxity; however, they are often not formally taught during clinical training.
Purpose:
To provide a reproducible method for obtaining stress radiographs.
Indications:
Stress knee radiographs are used in the setting of acute and chronic knee ligamentous and soft tissue injury.
Technique Description:
Coronal laxity: Knees are flexed at 20°, the x-ray beam is tilted 20° cephalad, and aligned with the inferior pole of the patella. Apply a valgus force with slight external rotation to the knee to test the medial collateral ligament (MCL). Perform on the contralateral knee. Use a varus force to test the lateral collateral ligament (LCL) and the posterolateral corner. Measure the joint space width with the LaPrade method. Sagittal laxity: Position the patient supine and flex the knee to 80°. The patient holds the cassette parallel to the x-ray beam, which is at the foot of the bed. Allow the tibia to sag without support, and compare the side-to-side difference on the bilateral radiograph.
Results:
The case in this video shows a side-to-side difference, suggesting a grade 3 MCL, LCL, and partial posterior cruciate ligament injury.
Discussion/Conclusion:
Stress radiographs support accurate diagnosis of complex knee injuries and provide an objective measure of knee stability. These techniques can be performed in an ambulatory clinic setting and are cost-effective, efficient, and support clinical decision-making in the treatment of complex knee injuries.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.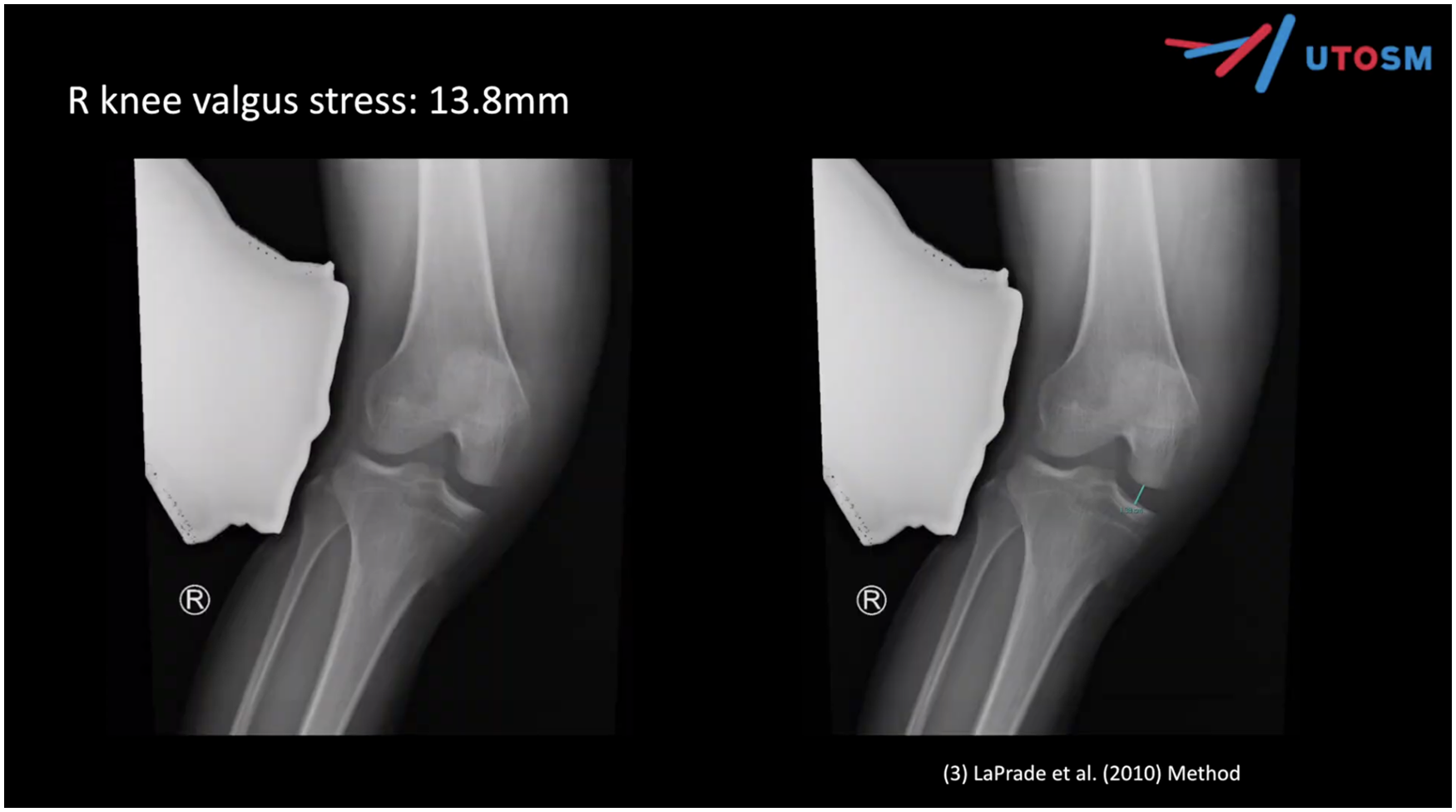
Video Transcript
Background
Today, we will discuss our technique for assessing laxity in multiligamentous knee injuries using stress radiographs—a simple technique for a busy clinic.
First, we will review the background and indications of stress radiography, followed by a technique description demonstrated through a case, followed by the case results, discussion, and conclusion.
Multiligamentous knee injuries are complex and nuanced. There can be challenges with the clinical examinations that include concomitant injuries, obesity, guarded patients, fractures, and interrater variability with clinical examination maneuvers.
Stress radiographs can be an important, if not essential, adjunct to basic imaging and clinical examination to objectively quantify knee laxity. 1 We utilize them routinely in the assessment of these complex patients. Stress radiography can also be used in cases of isolated collateral or posterior cruciate ligament (PCL) injuries, in cases when the clinical examination or magnetic resonance imaging (MRI) is not entirely indicative of the injury.
Multiple different publications and infographics have helped demonstrate the radiographic parameters associated with the extent of injury of multiple ligaments within the knee. 2 The purpose of this video, in particular, is to provide a reproducible method to help achieve these stress radiographs that then can be compared with prior established values.
Indications
Today, we will be discussing the case of a 25-year-old man who had a large cabinet fall onto his right knee. He had a lateral impact on the knee. This was 6 weeks prior, and he was treated by an outside physician and started on a gentle knee range of motion with physical therapy and immobilization. He is an otherwise healthy individual. He is active but does not participate in any particular sports.
On examination, he had neutral alignment with a mild effusion. The range of motion lacked 5° of terminal extension to 120° of flexion. His anterior cruciate ligament (ACL) was a grade 2 tear, as determined by Lachman anterior drawer testing. The PCL was a grade 2 with a posterior drawer testing. The MCL had a grade 3 injury with valgus laxity, and the lateral collateral ligament (LCL) was a grade 2 injury with varus laxity. The next step would be to obtain baseline radiographs and MRIs.
Upon reviewing his radiographs, no concerning features or fractures were found. We also obtained 3-foot standing alignments that showed neutral alignment.
On the MRI, we see a complete ACL tear and a significant partial or complete PCL tear, as well as medial-sided and lateral-sided collateral injuries.
Again, on the radiographs, we see no acute fractures or neutral alignment. On the MRI, there is a complete ACL tear, significant PCL tear, proximal tear of the medial collateral ligament (MCL), and significant lateral-sided injury, as well as a posterior horn longitudinal lateral meniscal tear. At this point, we want to quantify their laxity with coronal stress views.
Technique Description
Coronal Testing
We have a 25-year-old man who had a workplace injury to his right knee.
We are going to do some stress radiographs. The knees are bent in a 15° to 20° flex position. You will note that the radiograph is angulated in a 15° cephalad direction for an anteroposterior (AP) tunnel view. The x-ray beam is aligned with the cross here between the knees and the horizontal level at the inferior pole of the patella. To the best of our ability, we have the patient align his knees so that the kneecap is facing toward the ceiling, allowing us to obtain a true AP view.
Valgus Stress
To start, we will apply a valgus force to the right knee. This is done with the radiographic glove at the level of the knee or just above, and a valgus force and external rotation force are applied to the tibia at the level of the medial malleolus and lateral malleolus to keep this hand out of the field of the x-ray beam.
For this view, we are taking a valgus stress force on the right knee. The x-ray beam is aligned at the inferior pole of the patella on the affected knee, and the beam is appropriately combed in to reduce exposure. The same procedure is done for the left knee, with the beam again aligned at the inferior pole of the patella, and a valgus force applied.
Varus Stress
In the same way, a varus force is applied to each knee, again with the beam centered at the inferior pole of the patella, and a varus force on the affected (right) knee. Again, trying to keep the kneecap toward the ceiling to allow for a true AP, and a maximal manual force with the knee in varus.
Results
These are the radiographs obtained after the stress views were taken. We used the Laprade method to determine the distance. 3 On the medial side, there was 13.8 mm with the right knee valgus stress. On the left, there was 7.9 mm.
With varus stress on the right, there was a 13.6-mm difference, and on the left, a 10.1-mm difference. 4
Combined, there was a 5.9-mm difference when comparing the right to the left with the valgus stress of the MCL. Similarly, there was a side-to-side difference of 3.5 mm with the varus stress of the LCL.
The next step is to quantify posterior laxity. To assess PCL laxity and quantify a sag, we will use a bilateral skyline radiograph. This is done with the patient supine, with the knee flexed approximately 70° to 80°. The patient holds the cassette, preferably parallel to the level of the collimator beam. The collimator is placed at the foot of the bed. The patient brought down the bed. We do not want anything supporting the back of the tibia, so it hangs free, as you will see.
The foam is positioned to allow for a 70° bend.
These radiographs are obtained after the posterior sag stress radiograph. As you can see, there is a side-to-side difference of 6.9 mm.
Overall, in stress testing of the MCL with valgus stress, a side-to-side difference of 5.9 mm is observed. Stress testing of the LCL had a side-to-side difference of 3.5 mm. Stress testing of the PCL had a side-to-side difference of 6.9 mm.
When comparing with established values, there is a complete grade 3 MCL injury, a complete grade 3 LCL/fibular collateral ligament and popliteus tear, and a partial PCL tear.
Conclusion
The next step is to have a nuanced discussion with the patient regarding reconstructive and repair options. In conclusion, knee stress radiographs are a dynamic examination that can aid in evaluating functional laxity secondary to ligament injury. These can be used for both isolated ligamentous injuries and combined multiligamentous injuries. It may be easier than other described techniques, particularly for the PCL, such as kneeling stress views and the Telos device, as the patient remains supine throughout the assessment and radiographs, with minimal additional equipment required, and the knees are only bent to 70°, which may be easier early on in rehabilitation.
Having thorough discussions with your radiography team is key to building an efficient process, and this method can be reproducible without direct surgeon involvement. Furthermore, research is currently ongoing to describe specific cutoff values for the technique used to assess PCL sagittal laxity.
These techniques for knee stress radiographs can be performed effectively within a busy clinic, and having a thorough discussion with your radiography team is key to building an efficient process.
Footnotes
Submitted July 22, 2025; accepted August 28, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.