
Abstract
Background:
One of the most consistent pathoanatomic findings in lateral patellofemoral instability is trochlear dysplasia. Trochleoplasty is a procedure designed to deepen the trochlear groove, thus correcting trochlear pathoanatomy and improving patellofemoral tracking.
Indications:
Patients with high-grade trochlear dysplasia that includes anteriorization of the floor of the trochlear groove (trochlear bump >5 mm), with lateral patellofemoral instability.
Technique Description:
The technique described is a thin flap trochleoplasty. By an open lateral parapatellar approach, trochlear cartilage is elevated. A new groove is created by removing subchondral bone with a burr. The cartilage flap is then reduced on the subchondral bone, and gentle pressure is applied to the cartilage. Plastic deformity occurs, and the cartilage is fixed with bioabsorbable nails. This technique should be accompanied by a stabilizing procedure, such as a medial patellofemoral ligament reconstruction.
Results:
Thin-flap trochleoplasty has low redislocation rates (3%-4%) in appropriately selected patients. Multiple clinical studies and meta-analyses have shown good postoperative patient-reported outcome scores and improved postoperative knee scores. There is a high rate of patient satisfaction, return to work, and return to sports following surgery (>85%). Notable complications include patellofemoral osteoarthritis (7%-18%), knee ankylosis (4.4%), and the need for additional surgery (8%-11%). However, the risk of complications seems to be similar to other patellar-stabilizing procedure.
Discussion/Conclusion:
Trochleoplasty is a technically demanding surgical procedure but is safe, reliable, and effective in appropriately selected patients.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.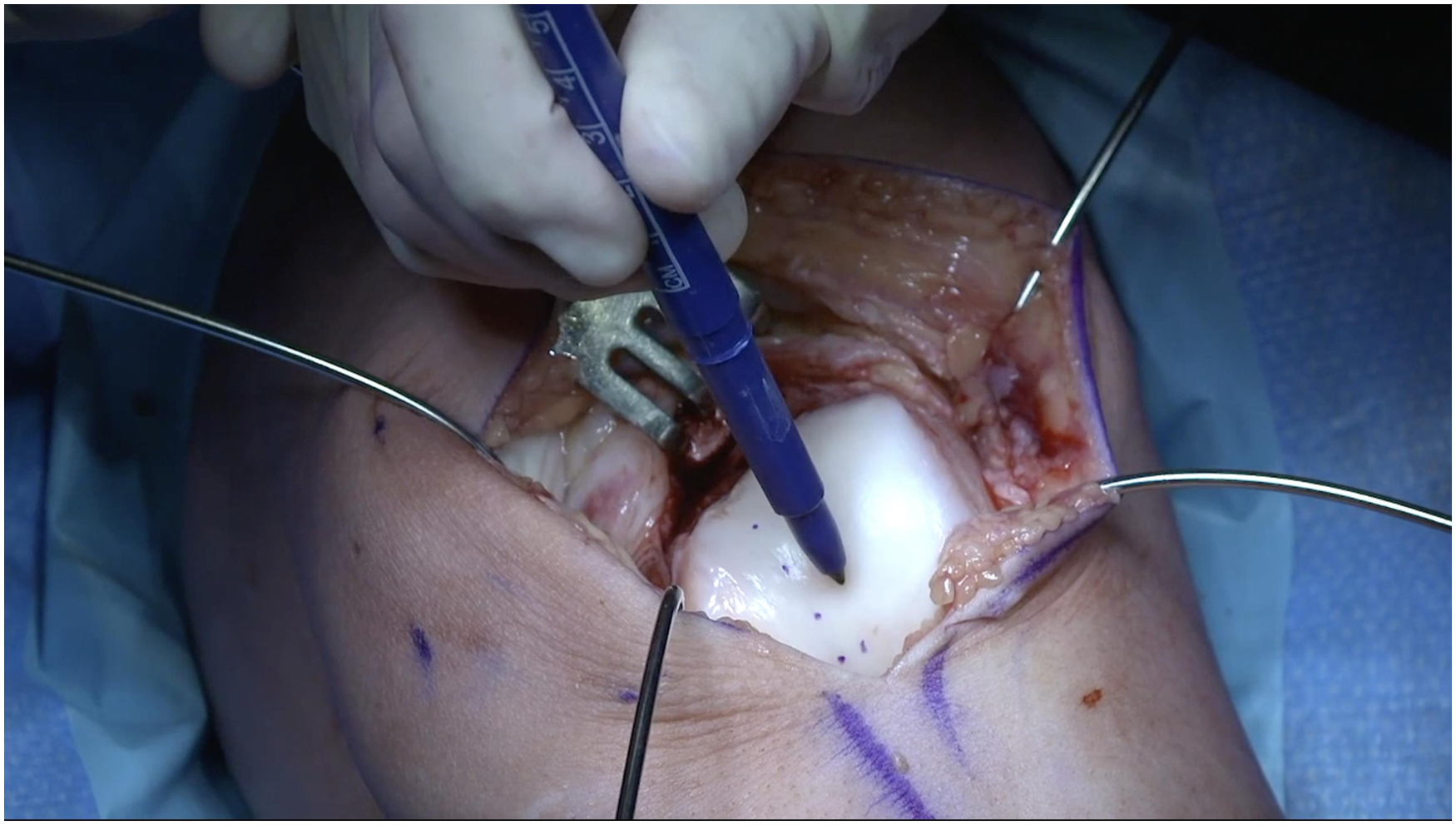
Keywords
Video Transcript
Hello, my name is Laurie Hiemstra. I am a sports medicine knee orthopaedic surgeon with a large patellofemoral instability practice. Today, we are going to discuss the role of trochleoplasty in patients with lateral patellofemoral instability in the presence of high-grade trochlear dysplasia and present a thin flap trochleoplasty surgical technique. The procedure was performed at the Banff Mineral Springs Hospital in Banff, Canada.
These are my disclosures.
Background
For patients with patellofemoral instability and high-grade trochlear dysplasia, trochleoplasty is a procedure designed to deepen the trochlear groove, correcting trochlear pathoanatomy and improving patellofemoral tracking.1,2,6 The indications for considering adding a trochleoplasty to a patellar stabilization procedure are the presence of high-grade trochlear dysplasia with a trochlear bump >5 mm, along with a significant J sign, such as a jumping J or grade 3 to 4 J sign.7,10 The technique described in this video is a thin flap trochleoplasty. Studies assessing trochleoplasty have demonstrated statistically significant improvements in clinical outcomes with complication rates equal to those of an isolated medial patellofemoral ligament (MPFL) reconstruction.3,4,7,8,11 Trochleoplasty is safe, reliable, and effective in appropriately selected patients.5,10
Indications
Relative contraindications to performing a trochleoplasty include advanced patellofemoral osteoarthritis.5,10 Skeletal immaturity is controversial, but authors have reported no growth disturbance after trochleoplasty in a skeletally immature patient with <2 years of growth remaining. 9
The patient is a 24-year-old woman with recurrent lateral patellofemoral instability. She has high-grade trochlear dysplasia, a normal tibial tubercle-posterior cruciate ligament (TT-PCL) distance, normal patellar height, and no significant rotational abnormalities. Her Beighton score is 4 of 9. She has a significant J sign, in which the patella jumps laterally at about 30° of flexion. The plan is for a trochleoplasty and MPFL reconstruction. This video reviews the trochleoplasty part of the procedure, using a thin flap technique.
A diagnostic arthroscopy is routinely performed to assess the chondral surfaces of the knee and exclude concomitant pathology. The trochlea and the patella are examined and the surgical plan confirmed.
Technique Description
The patient is placed in the supine position, with the affected leg bent to approximately 30°.
The trochleoplasty is performed through a lateral parapatellar approach, including a lateral retinacular lengthening of approximately 1 cm. This allows for closure of the lateral side of the joint at the end of the procedure in a lengthened position. The lateral arthrotomy extends above the proximal pole of the patella to ensure adequate exposure of the proximal trochlea. Detachment of the periosteum and associated fat pad at the proximal trochlear edge allows for visualization of the bone-cartilage interface. Steinman pins are placed to retract the tissue and then bent out of the surgical field.
The existing trochlear sulcus is marked, and the new location of the sulcus is planned in its anatomic position, in line with the femoral notch and the femoral shaft. This is usually about 1 cm lateral to the existing trochlear groove, which is most often medialized.
Curved osteotomes are then used to create an osteochondral flap approximately 5 mm in thickness. Most of the trochlear bump in this particular patient was proximal, so the osteochondral flap did not extend all the way to the notch distally. A burr is then used to create the groove in the femur at its planned new location and then to thin the osteochondral flap.
I currently use a combination of a Lindeman-type side-cutting burr and a 6-mm oval burr. The groove in the femur is developed first to give the surgeon more room to negotiate under the osteochondral flap. The flap is then sequentially thinned and tested for malleability at regular intervals. Senn retractors can be used to gently raise the osteochondral flap so that the surgeon can work on the undersurface. Saline is slowly dripped on the cartilage to keep it moist. A curette or similar instrument can be used to palpate the contour under the flap and ensure this area is smooth and that enough bone has been removed.
The surgeon moves back and forth between the 2 burr types until they are satisfied with the shape and location of the groove, as well as the thickness and malleability of the flap. A malleable osteochondral flap will be approximately 1 to 2 mm in thickness and has considerable flexibility, particularly in the younger population.
Once enough subchondral bone has been removed from the osteochondral flap, firm thumb pressure is all that is required to deform the chondral surface of the flap into the new groove on the femur. There is no need to crack the articular surface. The flap is held in place using 2 to 3 transchondral compression devices, 25 mm in length and 1.5 mm in diameter. These provide compression to the malleable flap and hold it in place until healing.
The contour of the trochlea surface can be seen to have changed dramatically with removal of the lateral bump, and a groove has been created for the patella to track smoothly according to its natural force vector.
This procedure will always be accompanied by an MPFL reconstruction.
Results
The rehabilitation plan after trochleoplasty and MPFL reconstruction is the same as for an isolated MPFL reconstruction and can be found on our website at www.banffsportmed.ca.
Studies on patient outcomes after trochleoplasty demonstrate low redislocation rates, especially when combined with an MPFL reconstruction.7,8,11 Statistically significant improvements in knee stability, patient-reported outcome measures, high rates of return to work, and high patient satisfaction have been reported in various series totaling over 1000 patients.1,3,4,7
The return to sport and activity rate for these patients is high. 3 However, time to return to sport is patient specific. These patients are often deconditioned prior to surgery, and before returning to activity, the patient must regain good neuromuscular control. Patients generally return to their activities between 6 and 12 months, although this time frame may be extended up to 2 years. 3
Complications reported for the thin flap trochleoplasty technique are similar to those of an isolated MPFL reconstruction. These include redislocation of the patella (3%-4%), residual feelings of instability and apprehension (6%-9%), and knee stiffness (4.4%).8,11 Although greatly feared, nonunion of the osteochondral flap has been rarely reported.
Discussion/Conclusion
In conclusion, trochleoplasty is safe, reliable, and effective in appropriately selected patients.5,10 Higher-quality evidence is still needed to better define which patients would benefit from trochleoplasty in addition to an MPFL reconstruction.
We thank Conmed Canada for their financial support for the video recording and editing.
Here are our references for your review.
Thank you for watching!
Footnotes
Submitted December 17, 2024; accepted July 28, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received by ConMed for the videographer. L.A.H. is on the board of directors for the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and the Patellofemoral Foundation; is a paid consultant and on the speaker’s bureau for Smith & Nephew, ConMed, Pendopharm, Sanofi, and Precision OS; and has received research support from ConMed, Smith & Nephew, and Pendopharm. S.M. is a paid speaker for Stryker and Smith & Nephew, received research grants from ISAKOS, and is on the speaker’s bureau for Stryker and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.