
Abstract
Background:
Posterior sternoclavicular joint (SCJ) dislocations are uncommon because of the strength of the posterior joint capsule but pose a significant risk of neurovascular and mediastinal compression. Various surgical techniques have been described, with the sternal docking reconstruction using tendon allografts demonstrating improved biomechanical stability, elimination of anterior bulk, and ease of graft passage. This study outlines the intramedullary posterior SCJ reconstruction with a semitendinosus allograft for recurrent symptomatic posterior SCJ dislocations.
Indications:
Surgical reconstruction is indicated in patients with symptomatic recurrent posterior SCJ dislocations that fail conservative management. A semitendinosus allograft with suture augmentation may be utilized because of its strength, availability, and ability to provide long-term stability while minimizing donor site morbidity.
Technique Description:
The procedure involves an open reconstruction using a semitendinosus allograft, which is passed through bone tunnels in the clavicle and sternum to recreate the function of the sternoclavicular ligament. The graft is tensioned manually and secured using a nonabsorbable, high-tensile suture to restore joint stability while allowing for controlled mobility. The construct aims to replicate native joint biomechanics and reduce the risk of recurrent dislocations.
Results:
At 2 weeks postoperatively, the patient reports satisfactory recovery with improved shoulder stability and pain managed with over-the-counter analgesics. He has not experienced complications, such as infection, neurovascular impairment, or graft failure. Continued rehabilitation is expected to facilitate return to full function.
Discussion/Conclusion:
This study presents the surgical management of a recurrent posterior SCJ dislocation in an 18-year-old male patient with a semitendinosus allograft reconstruction. Given the rarity of symptomatic posterior SCJ instability, the optimal surgical approach remains debated. Further research is warranted to establish best practices and long-term outcomes in SCJ reconstruction; however, numerous beneficial outcomes are reported for this reconstruction technique.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication
This is a visual representation of the abstract.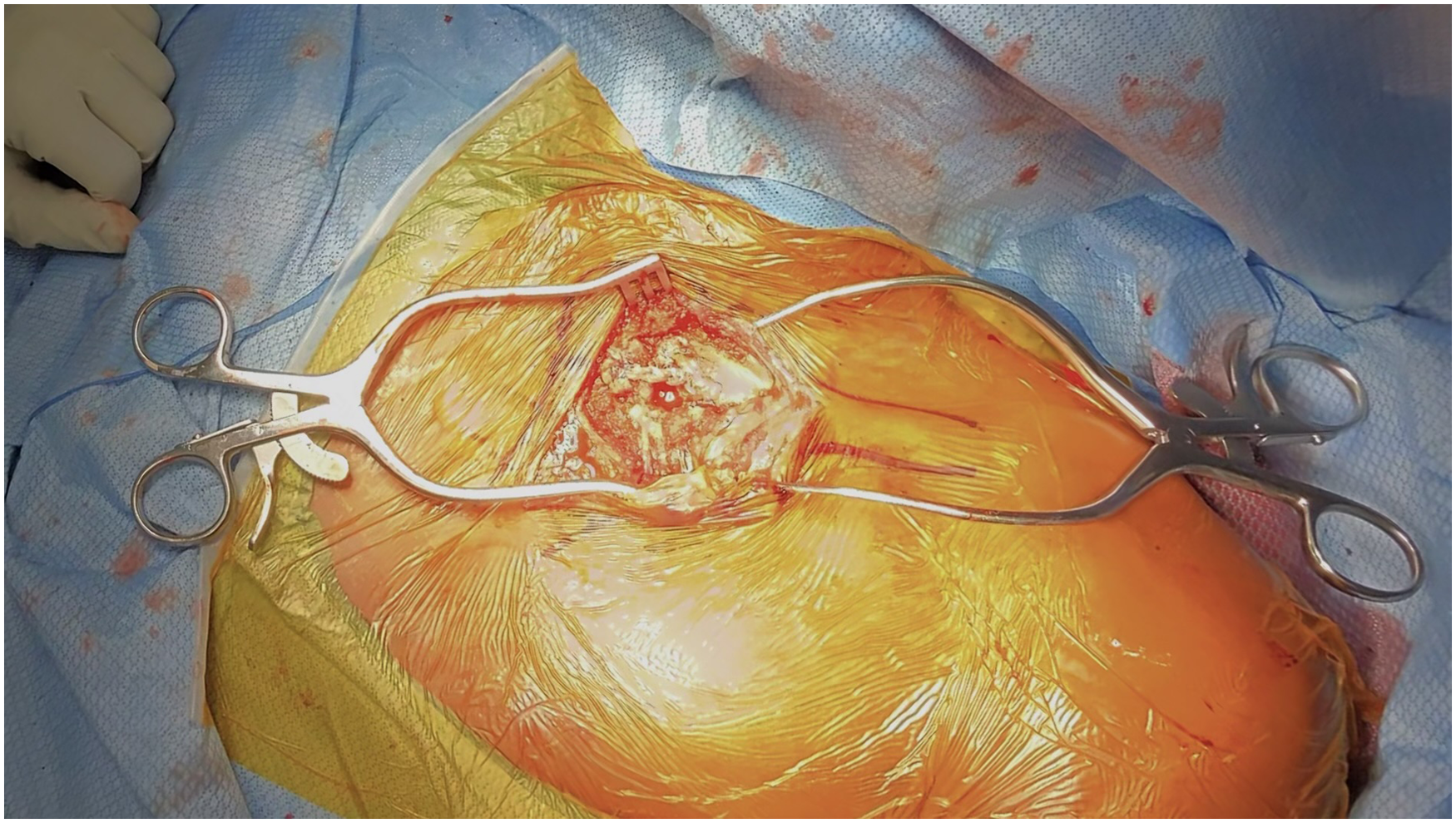
Keywords
Video Transcript
This video demonstrates our technique for posterior sternoclavicular joint (SCJ) reconstruction using a semitendinosus allograft in patients with symptomatic posterior SCJ dislocations.
Background
Reconstruction of an unstable sternoclavicular joint (SCJ) was first described by Bankart, using an autograft passed through bone tunnels, dating back to 9 1938. Posterior SCJ dislocations are uncommon because of the strength of the posterior joint capsule, but carry a higher risk of neurovascular and mediastinal organ compression. 10 While symptomatic recurrent posterior SCJ dislocations requiring surgery are rare, various surgical techniques exist, with the figure-of-8 reconstruction being the most common.2,4 The sternal docking approach has also demonstrated improved patient satisfaction and increased biomechanical stability while eliminating anterior bulk and clavicle displacement. 7 This technique also allows for easier passage through the bone tunnels, prompting increased graft viability. 7
Indications
The procedure involves an intramedullary reconstruction using a semitendinosus allograft, which is passed through bone tunnels in the clavicle and sternum to recreate the function of the sternoclavicular ligament. We prefer this graft stabilization technique for all anterior and posterior sternoclavicular dislocations, as well as some medial clavicle resections secondary to arthritis. This technique allows tensioning and maintenance of the reduction with a low-profile result.
The patient is an 18-year-old man presenting to our clinic with persistent pain and instability of the left shoulder, following a posterior sternoclavicular joint (SCJ) dislocation from being pushed and landing on a protracted shoulder during a football game. It was managed nonoperatively 1 year ago, with physical therapy and sling immobilization. However, he continues to experience pain and discomfort with mobility during sprinting and has elected for surgical intervention.
Technique Description
Preoperative Planning and Examination
The shoulder has a full passive range of motion with mild hypermobility and asymmetry at the left SCJ on preoperative physical examination. Deltoid strength is normal in all planes, and tenderness is present at the SCJ but not at the acromioclavicular joint. The vascular examination is normal, with symmetric pulses. Preoperative imaging on computed tomography shows a posterior SCJ fracture and dislocation. For the procedure, the patient is positioned supine in a modified beach-chair position, approximately 30° from the horizontal position. The shoulder and arm are prepped in the field with full access to bilateral SCJ. The vascular team is aware and on standby.
Exposure of the SCJ
The intraoperative examination confirms hypermobility and the ability to posteriorly subluxate the SCJ upon manipulation of the clavicle. The open procedure begins with an initial hockey-stick incision made over the inferior one-third of the affected SCJ for subperiosteal dissection. Flap formation is created through a mix of electrocautery and sharp dissection, with frequent palpation of the SCJ to guide further dissection. An oscillating microsagittal saw blade is used to carefully excise 5 to 10 mm of clavicle and intra-articular disc, which is anteriorized with Homan retractors. Careful blunt instrumentation protection is used to avoid traction injury to posterior structures.
Clavicular Tunneling
Then, 2 unicortical guide holes are made 1 cm apart on the medial clavicle using a 4.5-mm drill. A curette is used to remove any remaining cancellous bone and help connect the tunnels. An oblong medullary canal is drilled on the medial side of the clavicular head to allow for superior and inferior tunnel convergence.
Sternal Tunneling
Similarly, 2 unicortical holes are created 1 cm apart on the anterior surface of the lateral sternum. To achieve confluence, an oblong medullary canal is made on the sternal articular facet, using a 4.5-mm drill bit. Again, a curette removes cancellous bone and helps connect the tunnels.
Traction Suture Placement
To allow future graft passage, sutures are passed with a Hewson suture passer, traveling through each superior and inferior clavicular tunnel and exiting through the medullary canal. The exact process is repeated on the sternum. The Hewson suture passer is first threaded through the inferior drill hole, exiting via the medullary canal of the lateral sternum. This allows for easy passage and management of sutures. Here, you see the completed tunnels with traction suture placement. The semitendinosus allograft is prepared with a whipstitch on each end at the back table in a sterile fashion.
Construct Diagram
This diagram illustrates the osseous tunnels drilled in the clavicle and sternum, as well as the trajectory of the graft in a sternal docking configuration, with the graft wrapped through the clavicular tunnels and fixed to the sternum, as described by Sanchez-Sotelo et al. 7
Graft Passage
We now transition to the graft, beginning with entrance through the clavicular medullary canal and exiting via the inferior clavicular tunnel, leaving adequate graft available for ultimate passage through the inferior sternum in a later sequence. Next, the lead end of the allograft is passed through the superior clavicular tunnel, exiting medially through the sternal medullary canal. Then, the graft is passed across the joint, through the lateral sternum, via the superior tunnel. You can see the joint begin to reduce as the tail end of the graft is assessed for length. The graft is then marked to the appropriate length and whipstitched before the excess is removed. Finally, the sternal docking is completed with the passage of the tail end of the graft through the sternal medullary canal and out of the inferior sternal tunnel. Slack is removed, and tension is applied before suture fixation.
Securing the Semitendinosus Allograft and Final Inspection
Final tension is held with manual reduction as the intersection of the graft is tied with high-tensile nonabsorbable suture, fixed in an onlay fashion. The tails are trimmed, and the remaining limbs are incorporated into the anterior capsule. Then, a range of motion assessment is performed, revealing full physiologic mobility of the extremities. Additional 2-0 FiberWire sutures are placed in the periosteum and the peripheral disk to reapproximate the SCJ. Then, the periosteum and myofascial layers are closed with a pants-over-vest reconstruction. Subcutaneous tissues are closed with 3-0 Vicryl and 3-0 Monocryl. Postoperative radiographs demonstrated an excellent reduction and a symmetric position compared with the contralateral side.
Results
Rehabilitation instructions include 6 weeks of immobilization in a shoulder sling. The patient may resume range of motion in the elbow, wrist, and hand as soon as comfort allows. Additionally, the patient will undergo cryotherapy but continue wearing the abduction sling. Passive to active assist range of motion will start after 1 week, in line with our SCJ reconstruction protocol. Ultimately, local wound care can be rendered in the immediate 2 weeks. At his 2-week postoperative follow-up, the patient reports a satisfactory recovery, with regained range of motion and uneventful soft tissue healing. He has initiated strength training and plans to return to sport after 4 to 6 months, pending clearance of a sports-specific transition program.
Discussion
Overall, sternoclavicular reconstruction has a complication rate of 16%, including issues such as recurrent instability, infection, inadequate reduction, bone fractures, and neurovascular damage.1,3,4,7 However, the specific technique using ligament reconstruction with tendon grafts showed an even lower rate of instability and complications. Patient outcomes are positive, with a significant improvement in visual analog scale pain scores and Single Assessment Numeric Evaluation scores rising6,9 from 40% to 90%. Functional outcomes also improved, with a 90% survivorship at a 5-year follow-up, and most patients returned to their preinjury level of sports or activity.5,8 Ultimately, with insufficient evidence to definitively guide a decision, management of these injuries should be made on an individualized basis.
Tips and Tricks for the Procedure
When performing SCJ reduction, it is important to ensure a wide surgical field for optimal exposure. Before reducing the SCJ, clear any scar tissue, osteoarthritis, and the intra-articular disc. To protect neurovascular structures, use a periosteal elevator under the manubrium and clavicle. Before graft passage, clear the bone tunnels with a small curette to prevent graft obstruction. Finally, utilize a layered closure of the incision to increase stability and always have the vascular team on standby for potential complications.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.W. serves on committees for the American Academy of Orthopaedic Surgeons, the American Orthopaedic Society for Sports Medicine (AOSSM), and the Arthroscopy Association of North America; receives research support from Arthrex, Inc; serves on editorial or governing boards for Arthroscopy; receives publishing royalties and financial or material support from Arthroscopy and Elsevier; is a paid consultant for FH Ortho; is an unpaid consultant for Kaliber AI and Sparta Science; holds stock or stock options in Kaliber AI and Vivorte; and is a paid presenter or speaker for Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.