
Abstract
Background:
Osteochondral fractures of the patella resulting from an acute patellar instability event may undergo fixation in the acute setting. Transosseous suture fixation may be advantageous in certain instances in comparison to other modalities by minimizing further violation of the articular cartilage and by helping to achieve adequate compression of thin and broad fragments.
Indications:
A 35-year-old man with a large osteochondral patella fracture in the setting of an acute, traumatic lateral patellar dislocation event.
Technique Description:
Diagnostic arthroscopy is performed. The donor site is identified and prepared, and the osteochondral fragment is removed. A medial parapatellar approach is utilized to expose the patella for medial patellofemoral ligament (MPFL) graft fixation and to allow for eversion and access to the articular surface of the patella. The osteochondral fragment is sized relative to the donor site. Metal, headless, cannulated screws are employed for the fixation of suitable areas of the osteochondral fragment. Vicryl sutures are shuttled through transosseous tunnels and tied over the anterior patella to achieve appropriate compression of the thin, broad peripheral area of the osteochondral fragment and augment the stability of the fixation construct. MPFL reconstruction is completed.
Results:
There were no immediate complications following surgery. Surgical management led to improvement of the patient's clinical function and patellar stability. The patient returned for second-look arthroscopy and removal of hardware at 3 months postoperatively, at which time the fragment demonstrated early healing and the Vicryl sutures had resorbed.
Discussion/Conclusion:
The senior author's preferred technique for transosseous suture fixation of an osteochondral patella fracture is presented. Transosseous suture fixation may be used in isolation or to augment fixation where sufficient implant purchase or fragment compression may not be obtained with other fixation modalities. Further clinical study is needed to investigate long-term clinical outcomes with this technique.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.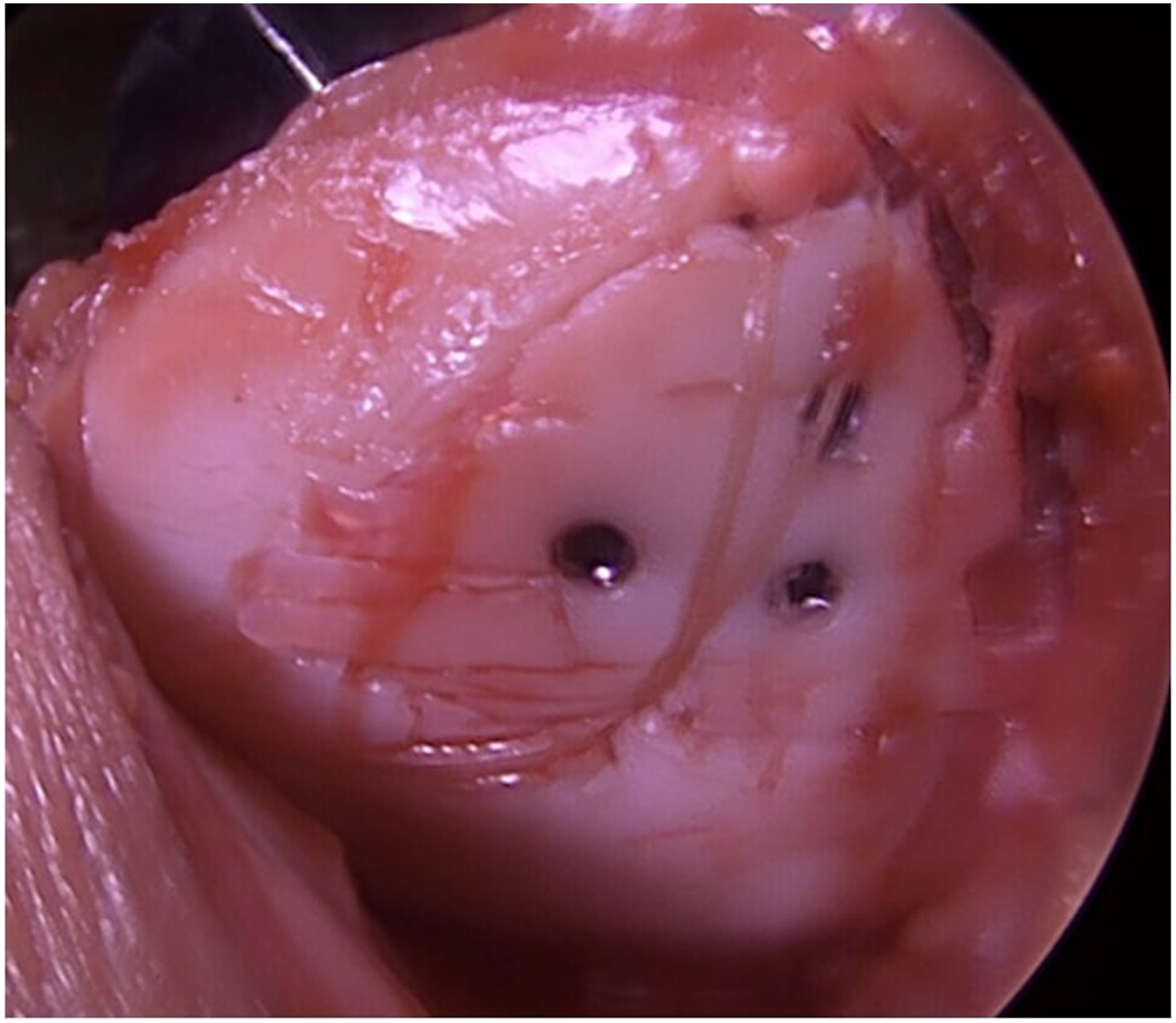
Keywords
Video Transcript
In this video, we discuss the indications, surgical technique, and outcomes for transosseous suture repair of a patellar osteochondral fragment following an acute patellar instability event.
Here are our disclosures.
Background
We utilize a case presentation to demonstrate the indications for transosseous suture repair of a patellar osteochondral fragment. Our patient is a 35-year-old man who sustained a contact injury while playing hockey the day before presentation, where a valgus force was imparted upon his left knee. He noted immediate pain and swelling. Notably, the patient had no prior injuries or surgical history with regard to his left knee. His physical examination was notable for a grade 1 effusion, limited range of motion, medial patellar tenderness, and asymmetric lateral patellar translation on the left knee compared to the contralateral side, with associated apprehension.
Left knee radiographs were acquired, which demonstrated no obvious acute pathology.
Left knee magnetic resonance imaging (MRI) subsequently demonstrated a large joint effusion, an osseous contusion pattern consistent with a lateral patellar dislocation event, a patellar-sided medial patellofemoral ligament (MPFL) injury, and a large osteochondral fragment displaced from the medial patellar facet into the suprapatellar pouch.
Given the presentation consistent with a lateral patellar instability event, the Caton-Deschamps Index was further characterized to be 0.97 and within normal parameters. The patient did not have significant trochlear dysplasia. The tibial tubercle–trochlear groove distance was 4.7 mm.
Indications
Based on the patient's clinical presentation, examination, and radiographic findings of a large, displaced osteochondral fragment from the patella in the setting of an acute, traumatic lateral patellar instability event, he was determined to be a candidate for surgical intervention, consisting of left knee arthroscopy with patellar osteochondral fragment fixation versus excision and possible MPFL reconstruction (MPFL-R). Notably, this patient had no history of patellar instability and no underlying anatomic risk factors.
Technique Description
Requisite materials for the transosseous suture repair of the patella osteochondral fracture are listed here. Tranexamic acid is utilized to aid in the performance of this procedure on an outpatient basis. The patient is positioned supine with the operative extremity contained in a surgeon-controlled extremity holder and the contralateral leg in a lithotomy position. We use a thigh tourniquet to reduce bleeding intraoperatively.
After an examination under anesthesia, a diagnostic knee arthroscopy is performed, utilizing standard anterolateral and anteromedial portals. The examination under anesthesia is of high clinical relevance in this setting when deciding whether to perform MPFL-R if the fragment is unsalvageable. In the absence of significant or asymmetric lateral patellar translation on examination, shared decision-making can occur based upon an informed discussion with the patient about their risk for subsequent patellar dislocation, the relative surgical risk of an MPFL-R, and the prolonged rehabilitation required from this procedure.
A complete diagnostic arthroscopy is performed to rule out other concomitant pathology and to completely evaluate the displaced fragment and its donor site. If the fragment is determined to be unsalvageable based on its appearance, it is excised arthroscopically, and an abrasion chondroplasty is performed at the donor site.
If the fragment is determined to be salvageable, the arthroscopic portion of the case is concluded and a standard anterior approach to the knee is performed, followed by a limited medial parapatellar arthrotomy to allow for eversion of the patella and to expose its medial aspect for patellar-sided graft fixation during MPFL-R. It is recommended that the surgeon attempt to use the shortest length of arthrotomy required to evert the patella and provide adequate visualization of the articular surface of the patella. If the osteochondral fragment is to be fixed, the senior author (A.B.Y.) recommends the concomitant performance of MPFL-R to reduce the risk of loss of fixation from a potential subsequent instability event. The senior author prefers to place suture anchors before osteochondral fragment fixation to avoid disruption of fragment fixation during this process. The osteochondral fragment is identified in the suprapatellar pouch, excised from the knee, and taken to the back table for further preparation. The purple coloration on the fragment represents the aspect of the fragment that has sufficient subchondral bone attached to accommodate metal, headless compression screws. The part without purple coloration is representative of a purely chondral segment of the fragment, similar to what was present in the case presentation. The purple coloration present in the donor site is used to further differentiate the defect from the normal cartilage to the viewer. The surgeon should expect the osteochondral fragment to be larger than the donor site, even in the acute and subacute setting. It is unlikely that the fragment removed will appropriately fit within the donor site as it is found. A burr or curette is often necessary to exaggerate the depth of the donor site to allow the fragment to sit flush with the surrounding cartilage. Additional microfracture is not performed as the subchondral bone is already exposed. The surgeon may also use a No. 11 blade scalpel to carefully contour the fragment to a smaller size to appropriately fit the donor site.
Next, a towel clip may be placed at both the superior and inferior aspects of the patella, respectively, to aid in the eversion and stabilization of the patella. The fragment and donor site are then inspected. If sufficient subchondral bone is present on the fragment to achieve adequate purchase, a 2.0-mm metal, headless, compression screw (2.0 mm Acutrack 2 Micro screw; Acumed) is favored by the senior author to achieve fragment fixation. In this case, part of the large fragment would support the use of metal, headless compression screws. However, it was determined that another broad segment of the fragment was inadequate to sufficiently accommodate the use of a headless compression screw to achieve the appropriate compression necessary for healing. The use of hybrid fixation was planned.
At the lateral extent of the donor site, a 0.67-mm K-wire is then used to create a transosseous tunnel exiting the anterior patella. A suture passer (Nitinol Suture Passing Wire, 8 in.; Arthrex) is then passed retrograde and utilized to shuttle pairs of 0-Vicryl (Ethicon/Johnson & Johnson) through the tunnel created. Two sutures are used in this cadaveric demonstration, but the senior surgeon may use 4 or more, as the sutures are absorbable and atraumatic. Two additional transosseous tunnels are then created in a similar fashion, centered at the superior one-third and inferior one-third extent of the medial aspect of the donor site. Note that differing configurations may be employed at the surgeon's discretion to appropriately center the suture to achieve balanced compression of the unsupported aspect of the fragment. The suture passer is, again, passed retrograde and utilized to shuttle 1 limb of the 0-Vicryl suture through each respective transosseous tunnel. The sutures are kept loose at this time. The osteochondral fragment is then reduced into the donor site. In this case, part of the large fragment supports the use of 3 headless compression screws. After placement of the headless compression screws, the unsupported segment of the osteochondral fragment is held reduced while an assistant ties each suture individually to achieve fixation. MPFL-R may then be completed, and a final arthroscopic evaluation of the fragment can be performed. Final fixation is seen here.
Some of the more notable potential complications of performing transosseous suture repair are listed here and include symptomatic instrumentation, arthrofibrosis, failure to heal or loss of fixation of the fragment, iatrogenic chondral damage, and patella fracture.
Results
Patients are initially kept in full extension in a brace. At 2 weeks postoperatively, formal physical therapy is initiated, and a hinged knee brace is used to prevent flexion beyond 90°. An additional 15° of flexion is then further allowed at 2-week intervals. Patients are instructed to remain partially weightbearing until 4 weeks postoperatively. At 3 months postoperatively, physical therapy progresses to include more advanced plyometric and dynamic exercises. Patients are allowed to return to sports at 6 months postoperatively, after they complete a sport-specific return-to-play protocol.
There is a relative paucity of clinical studies or series reporting outcomes following transosseous suture repair of osteochondral fragments from the patella. Reports are largely limited to case reports or small series,1,3,5-7 such as the one by Dhawan and Hospodar. 3 The authors presented a case report of a 19-year-old man who underwent transosseous suture repair of a patellar osteochondral fragment. 3 At 9 weeks postoperatively, the lesion appeared to have healed on MRI. 3 The patient returned to athletics without issue at 18 weeks postoperatively. 3 Return to preinjury activity level was maintained through a final follow-up of 2 years postoperatively. 3
In the largest series by Malecki et al., 4 the authors reported a series of 17 patients who underwent transosseous suture repair of displaced osteochondral fragments from the patella following patellar instability events. Mean Lysholm and Kujala scores at the final follow-up, a mean of 7.5 years postoperatively, were 89.2 and 89.6, respectively. 4 All patients achieved healing of the fragments on MRI at follow-up. 4
The patient in the current case subsequently underwent second-look arthroscopy at 12 weeks postoperatively during a planned removal of the metal, headless compression screws utilized in his hybrid fixation construct. At the time of surgery, the fragment demonstrated excellent signs of early healing, and the Vicryl sutures had resorbed.
Discussion/Conclusion
Further study is needed to evaluate the clinical outcomes of transosseous suture repair of osteochondral patella fractures in isolation and to augment other fixation modalities. The most challenging aspect of transosseous suture repair is establishing the appropriate indication for its use versus excising fragments unsuitable for fixation. The use of transosseous suture repair may, however, allow the surgeon to expand the indication for fixation of certain fragments, as it can achieve compression of areas of fragments that are poorly supported for fixation with a screw or other modality. It also may be useful in achieving compression of large, purely chondral fragments, which have shown the ability to heal in the appropriate setting. 2 Transosseous suture repair also avoids violation of the articular surface and therefore reduces the risk of iatrogenic fracture of the osteochondral fragment if tenuous. Additionally, the Vicryl suture does not require later implant removal, as the Vicryl suture is absorbable. (See Table 1 for pearls and pitfalls of performing transosseous suture repair of an osteochondral patella fracture.)
Pearls and Pitfalls of Performing Transosseous Suture Repair of an Osteochondral Patella Fracture a
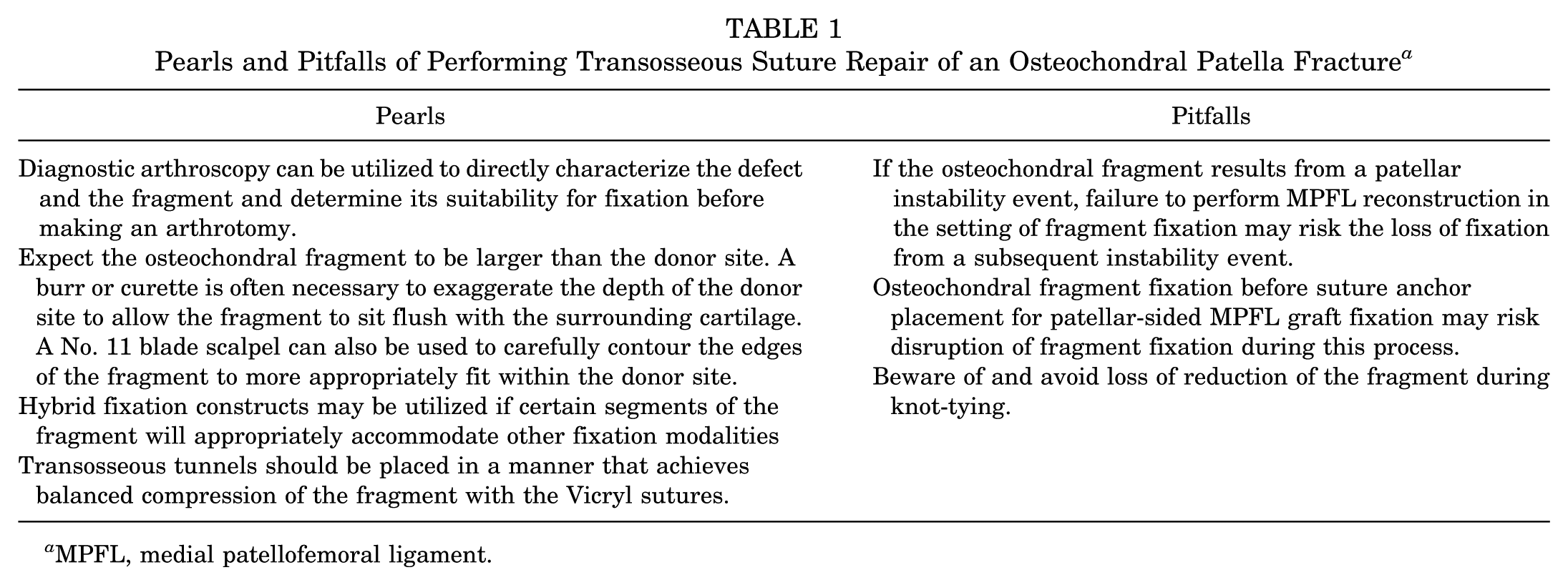
MPFL, medial patellofemoral ligament.
From Midwest Orthopaedics at Rush, we thank you for watching.
Footnotes
Submitted November 17, 2024; accepted May 27, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.Y. received research support from Arthrex and Organogenesis; is a paid consultant for AlloSource, JRF Ortho, and Stryker; is a paid presenter or speaker for Stryker; is an unpaid consultant for Patient IQ and Sparta Biomedical; and has stock or stock options in Sparta Biomedical, Icarus Medical, and Patient IQ. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.