
Abstract
Background:
A patient-specific, 3-dimensional-printed, custom glenoid baseplate can be utilized to address severe glenoid deficiency in reverse total shoulder arthroplasty (rTSA).
Indications:
A 73-year-old woman with right shoulder pain, weakness, and decreased range of motion in the setting of glenohumeral arthritis with severe glenoid bone loss. Additionally, this implant system was used in a 77-year-old man undergoing conversion to rTSA in the setting of glenoid erosion following prior failed total shoulder arthroplasty.
Technique Description:
A standard deltopectoral approach is utilized. In the revision setting, prior components are removed. Adequate glenoid exposure is obtained to allow for positioning and implantation of the custom glenoid baseplate. The glenoid is prepared utilizing patient-specific guides and trials before the custom glenoid component is seated within the glenoid vault and fixated with locking screws. Compatible glenosphere and humeral components are utilized for the remainder of the surgical procedure, as performed standardly.
Results:
There were no immediate complications following surgery. Surgical management led to improvement in the patient's pain and shoulder function.
Discussion/Conclusion:
Patient-specific, 3-dimensional-printed, custom glenoid baseplates may be used to manage severe glenoid deformity and bone loss in patients indicated for primary or revision rTSA.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.
Keywords
Video Transcript
In this video, we will discuss the indications, surgical technique, and outcomes with the use of patient-specific, 3-dimensional (3D)–printed, custom glenoid baseplates in primary and revision reverse total shoulder arthroplasty (rTSA).
Here are our disclosures.
The following topics will be covered in this video.
We will utilize a case presentation to demonstrate the indications for a patient-specific, 3D-printed, custom glenoid baseplate.
Background
Our patient is a 73-year-old woman with inflammatory arthropathy who had unsuccessful conservative management of chronic right shoulder pain and dysfunction. On physical examination, the patient is fully neurovascularly intact. There is crepitation and limited active shoulder range of motion (40° of forward flexion, 40° of abduction, 0° of external rotation, and internal rotation allowing her hand to reach the back pocket of her pants).
Radiographs revealed significant glenohumeral arthritis and decreased glenoid bone stock.
Computed tomography (CT) images were also obtained for the purposes of preoperative planning, further characterizing the significant glenoid bone loss. Imaging revealed a Walch type B3 glenoid/Sirveaux-Favard type E3 glenoid with 22° of retroversion and 10° of inclination.
The 3D reconstructions of the patient's CT scan are further demonstrated here.
Indications
Because the patient did not achieve durable relief of their chronic right shoulder dysfunction despite conservative treatment, they were determined to be a candidate for surgical intervention consisting of a right rTSA. The senior author's (S.F.B.) indication for using a patient-specific, 3D-printed, custom glenoid baseplate during primary and revision rTSA is the presence of combined and uncontained glenoid bone loss or glenoid dysplasia that would compromise the ability to obtain adequate fixation with a standard baseplate component. The preoperative radiograph and CT scans are used to evaluate the degree and pattern of glenoid bone loss, as well as for implant design.2-4 Relevant contraindications to the proposed surgical plan would have included active joint infection or infection elsewhere in the body, brachial plexopathy or axillary nerve dysfunction, and deltoid deficiency.
Technique Description
Requisite materials for the procedure are listed here. The procedure was performed on an outpatient basis with regional anesthesia. Consideration of the operative setting should be undertaken on a case-by-case basis to determine the likelihood of requiring an inpatient admission postoperatively. The patient is placed in a beach-chair position with the operative extremity secured on a surgeon-controlled arm positioner.
An example design conference between implant engineers (Restor3D) and the surgeon in this case will be presented as well. The custom glenoid component can be designed to be compatible with all humeral stems and is taken into account preoperatively by the design engineers. The custom glenoid baseplate was designed to allow for stable baseplate fixation in the setting of severe bony deformity. A small area of bony resection anteriorly and inferiorly was suggested to allow for the custom implant to seat fully onto the glenoid.
Additionally, these images show the addition of the glenosphere and locking screw length and trajectory facilitated by the custom glenoid baseplate once implanted.
First, the surgeon and engineer decide upon the appropriate glenosphere size. The amount of lateralization is then templated, aiming for neutral glenoid tilt and version, as well as seeking to restore adequate glenoid baseplate lateralization. The location of the glenosphere is then identified by utilizing the Friedman line and the floor of the supraspinatus. Positioning of the 7.3-mm glenoid baseplate post is performed via a wall thickness analysis, selecting the optimal area to allow for bony ingrowth. The 5.0-mm peripheral, titanium, locking screw length and trajectories are then determined after the custom glenoid baseplate template is added to the design rendering. Compression screw options and screw systems from other companies are compatible with the Restor3D custom glenoid baseplate and can be incorporated during templating. Screw length and trajectory can be adjusted on a case-by-case basis to allow for the capture of adequate residual cortical bone. At the conclusion of the design process, the registration tabs of the patient-specific targeting guide can then be reviewed to ensure they do not interfere with intended retractor placement. Surgeons then receive a detailed report and plan from the design conference.
After a standard deltopectoral approach and initial humeral preparation are performed, attention is turned to the glenoid exposure. Requisite mobilization of the subscapularis and anterior soft tissue release is performed to appropriately expose the glenoid to allow for its preparation and eventual custom glenoid baseplate (Restor3D) placement. Complete en face exposure of the glenoid should be obtained with appropriate retractors placed before proceeding with baseplate placement. Any minimal bone resection planned should be performed at this juncture.
Intraoperatively on the back table, a patient-specific glenoid model and targeting guides are available for intraoperative evaluation and comparison. The patient-specific targeting guide is then applied to the in vivo glenoid, and a central guide pin (2.8-mm Steinmann pin) is advanced through the targeting guide and confirmed to be appropriately positioned relative to the preoperative templating by placement of the patient-specific glenoid baseplate trial. The baseplate trial also serves as a targeting guide for the antirotation pin. The central post is then drilled for over the initial guide pin. The glenoid baseplate trial is used to once again confirm appropriate positioning and seating of the implant. Several drillholes are then created within the surrounding glenoid bone to encourage bony ingrowth. Additional reaming is not performed to preserve the remaining glenoid bone stock. The custom glenoid baseplate is then placed over the remaining pin and central post hole and impacted until fully seated. The glenoid baseplate is then secured with the placement of 4 self-tapping, 5.0-mm locking screws (Depuy Synthes) according to the preoperative templating. The glenosphere (Exactech) is then placed and impacted until fully seated and secure on the baseplate. Humeral preparation is then completed, and implants are trialed in a standard fashion to confirm satisfactory deltoid and soft tissue tension, as well as shoulder stability and range of motion. The humeral stem, tray, and polyethylene liner are then placed. The shoulder is then reduced and evaluated one last time before repair of the subscapularis and closure. Postoperative imaging is seen here.
This custom glenoid baseplate may also be used in the revision setting. A case example of a 77-year-old man undergoing conversion to rTSA following a prior unsuccessful total shoulder arthroplasty is shown here. The existing humeral implant is removed by using flexible osteotomes and back-slap, with care taken to preserve the tuberosities. The glenoid is then similarly exposed, removing prior components, cement, and soft tissue. It is critical to avoid removal of bone from the glenoid during the removal of the prior components and cement to preserve the fit of the custom glenoid guide and baseplate component. An initial guide pin and antirotation pin are then placed through the patient-specific guide before checking pin position with the trial glenoid component. The initial guide pin is drilled and the remainder of the glenoid baseplate placement proceeds in a similar fashion to the initial case presentation before the glenosphere is implanted. Postoperative imaging is seen here.
Results and Discussion
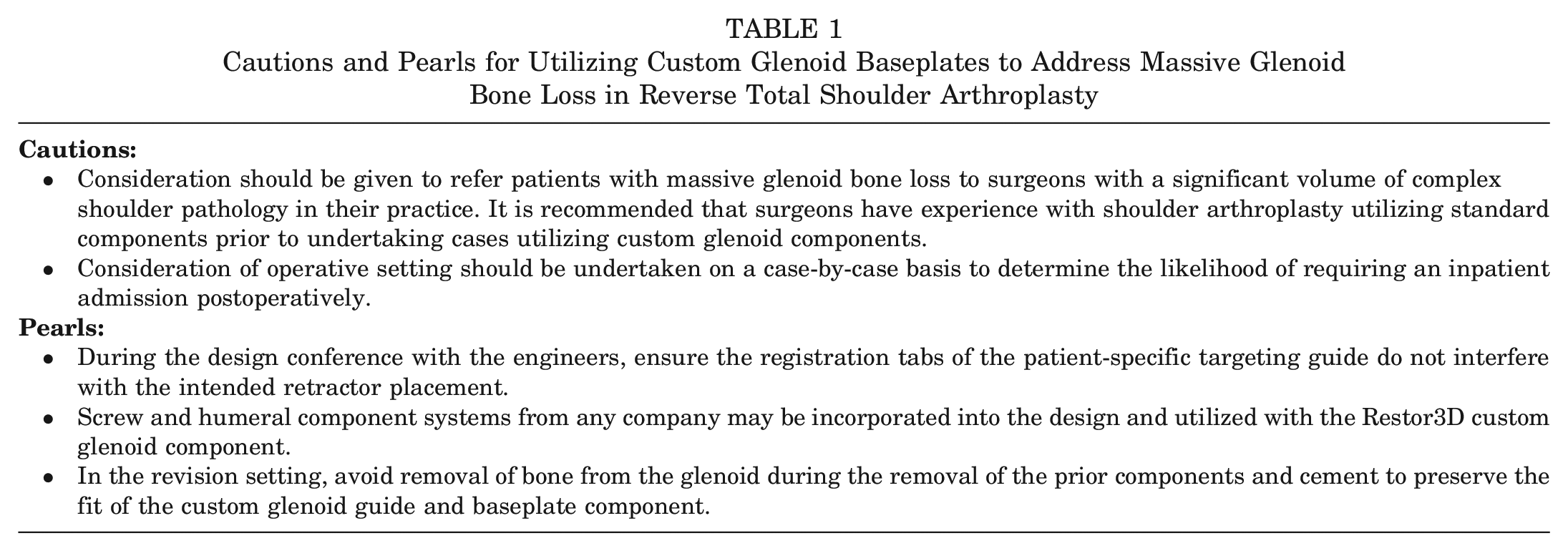
Some additional “cautions” and “pearls” are provided here (Table 1).
Cautions and Pearls for Utilizing Custom Glenoid Baseplates to Address Massive Glenoid Bone Loss in Reverse Total Shoulder Arthroplasty
Some of the more notable complications are listed here and include glenoid baseplate loosening and glenoid osteolysis, acromial stress fracture, periprosthetic fracture, neurovascular injury, instability, stiffness, and prosthetic joint infection.
We restrict and gradually advance the patient's activity for the first 8 weeks after surgery. Patients are kept nonweightbearing, and a shoulder immobilizer sling is used at all times except when performing home exercises and physical therapy. While protecting the subscapularis repair, physical therapy is initiated immediately postoperatively to include passive range of motion, pendulum exercises, and assisted elbow flexion and extension exercises. Passive range of motion is limited to 130° of forward flexion and 25° of external rotation initially. Patients gradually add active exercises at the discretion of the surgeon and therapist. Patients are allowed to progress to full activity at 12 to 16 weeks postoperatively. Venous thromboembolic disease chemoprophylaxis is utilized based on preoperative, patient-specific risk stratification.
While existing series in the literature are relatively small and limited to short-term follow-up, they have generally demonstrated encouraging early outcomes.1,2,4-6 Rangarajan et al 5 reported outcomes in 19 shoulders undergoing primary (n = 9) and revision (n = 10) rTSA with the vault reconstruction system (VRS) (Zimmer-Biomet) at a minimum 1-year follow-up (mean, 18.2 months). In this series, there were 4 complications reported, with 18 of 19 glenoid baseplates remaining clinically and radiographically stable at final follow-up. 5 Bodendorfer et al 2 also reported clinical and radiographic outcomes at a minimum 2-year follow-up (mean, 30 months) of 12 shoulders in 11 patients with severe glenoid deficiency who underwent primary (n = 7) and revision (n = 5) rTSA with the VRS. At the final follow-up, the authors reported that no patients experienced any postoperative complications or required revision surgery and that all implants appeared clinically and radiographically stable. 2 Finally, Moran et al 4 retrospectively reviewed outcomes of 14 shoulders with a mean 26.6-month follow-up in which the VRS was used in a total of 14 primary (n = 5) and revision (n = 9) rTSA procedures for severe glenoid bone loss. At the mean 26.6-month final follow-up, the authors reported all glenoid baseplates to be clinically and radiographically stable. 4 Despite the favorable early outcomes reported in the literature with the use of patient-specific, 3D-printed custom glenoid baseplates, given the relative scarcity of reports, further prospective study with longer-term follow-up is recommended to evaluate the outcomes when these implants are used for this indication.
From the Department of Orthopaedic Surgery at the University of Virginia, we thank you for watching.
Our references are listed here.
Footnotes
Submitted January 25, 2024; accepted May 17, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.W. is a board or committee member of AAOS, the American Orthopaedic Society for Sports Medicine, and the American Shoulder and Elbow Surgeons; is a paid consultant, paid presenter or speaker, and research supporter for Arthrex; and is a research supporter for Biomet, Exactech, and Flexion Therapeutics. S.F.B. is a board or committee member of the American Orthopaedic Society for Sports Medicine and the American Shoulder and Elbow Surgeons; is on the editorial or governing board of AOSSM Medical Publishing Board of Trustees and Video Journal of Sports Medicine and receives publishing royalties, financial support, or material support; is a paid consultant, presenter, or speaker for Arthrex; is a board or committee member of the Association of Clinical Elbow and Shoulder Surgeons; receives IP royalties from Biomet; receives IP royalties and is a paid consultant, presenter, or speaker at Exactech; has stock or stock options at Exactech and Johnson & Johnson; is a board or committee member of the MidAtlantic Shoulder and Elbow Society; is on the editorial or governing board of the Orthopaedic Journal of Sports Medicine; receives publishing royalties, financial support, or material support from Springer; is on the editorial or governing board of Techniques in Shoulder and Elbow Surgery; and is a paid consultant at WRS and receives IP royalties from Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.