
Abstract
Background:
Medial compartment osteoarthritis in young active patients presents a unique challenge with regard to joint preservation. Interventions, including cartilage restoration procedures, in the setting of high tibial osteotomy (HTO) have the potential to obviate or delay joint replacement if performed with a high degree of accuracy and avoidance of complications.
Indications:
The procedure is indicated in patients less than 65 years with isolated medial knee arthrosis, good range of motion, and no ligamentous instability.
Technique Description:
We present our technique for valgus producing opening wedge HTO with patient-specific instrumentation and implant with concomitant osteochondral allograft of the medial femoral condyle and tibial microfracture.
Results:
The goal of this intervention is to provide a minimally painful knee with durable (>10 year) outcome while minimizing the risk of perioperative complications including iatrogenic fracture and nonunion.
Discussion/Conclusion:
High tibial osteotomy with concomitant cartilage repair techniques can lead to high satisfaction and return to sport rates in appropriately selected patients.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.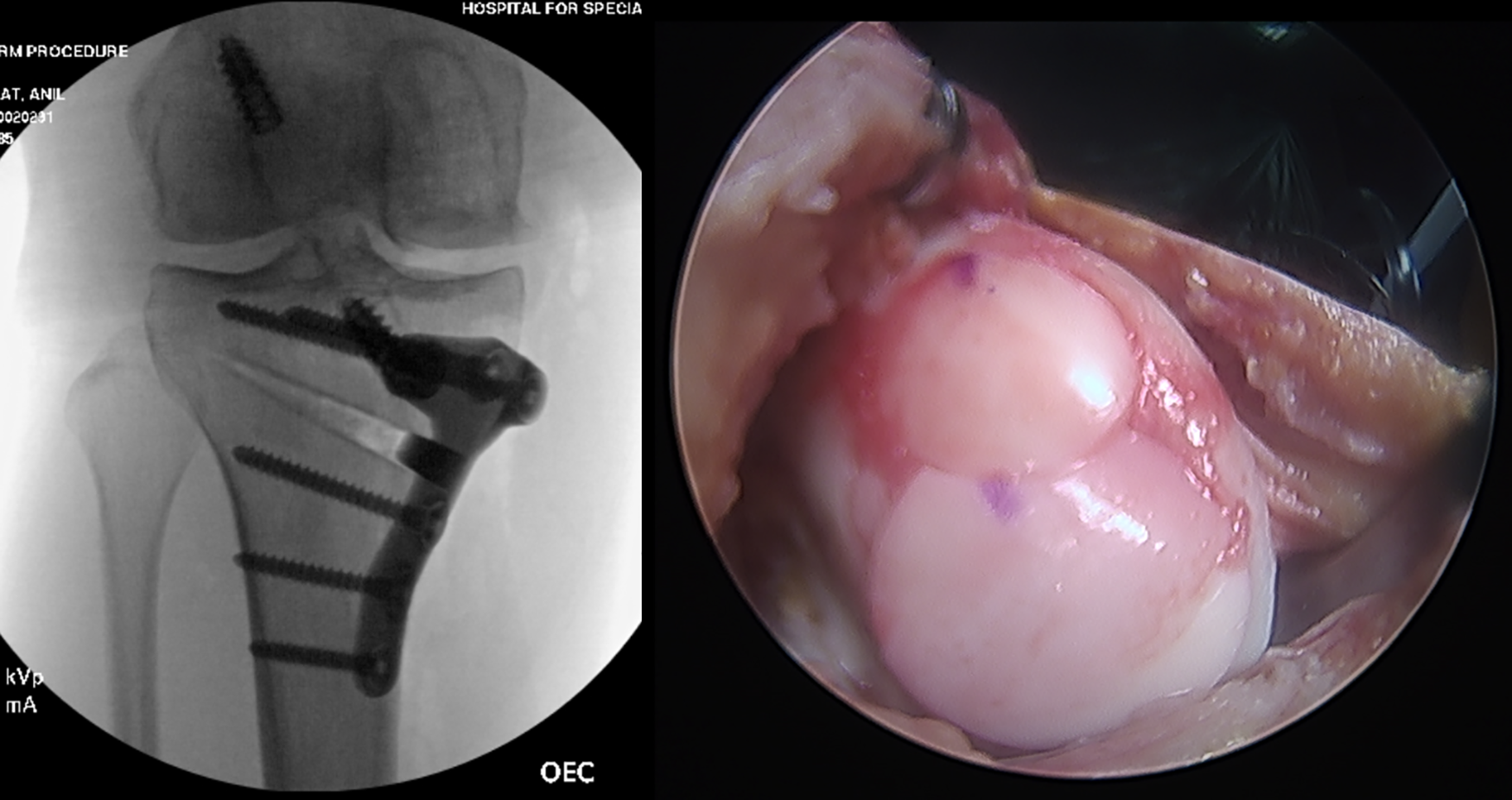
Keywords
Video Transcript
My name is Samarth Menta. I will be presenting our technique for osteochondral allograft (OCA) and high tibial osteotomy (HTO) with patient-specific instrumentation (PSI) from Hospital for Special Surgery.
These are our disclosures.
This is a brief overview of our presentation. Indications include a 35-year-old female with medial knee arthrosis, status post prior surgery.
We will present our technique for PSI and implant for HTO as well as OCA of the medial femoral condyle with a goal result of a minimally painful knee with durable outcomes greater than 10 years. We opted for PSI over standard implants because it offers precise correction, particularly in cases requiring multiplanar correction, and the ability to prevent implant jamming in patients with prior surgical implants.
This patient is a 35-year-old female with long-term right knee pain. She had a history of right knee anterior cruciate ligament (ACL) reconstruction with bone-patellar tendon-bone (BTB) autograft in 2013, and medial meniscectomy. She failed conservative measures including physical therapy and gel and cortisone injections and primarily localized her pain as medial on the knee.
On the examination, she had full range of motion, medial joint line tenderness to palpation, no flexion McMurray, and no varus instability. She had slight valgus instability at 0° and 30° of 3 to 4 mm, and her Lachman and anterior drawer are 2A.
These are the patients’ preoperative radiographs, which demonstrate medial compartment osteoarthritis with routine screws from a prior ACL reconstruction, where alignment demonstrated 8° of posterior tibial slope. She had a medial proximal tibial angle of 81°, lateral distal femoral angle of 84°, and 6° of varus mechanical alignment.
Here, we demonstrate representative magnetic resonance imaging (MRI); coronal and sagittal slices of the patient's knee demonstrate medial compartment arthritis with cartilage loss status post prior meniscectomy, and ACL reconstruction and an intact ACL graft.
In terms of planning, so for PSI, all patients get long leg alignment films as well as a computed tomography (CT) scan, and these are superimposed on one another, which allows us to obtain specific measurements with regard to the alignment of the lower extremity, the proximal tibia, as well as the distal femur. On the left, you can see the initial alignment and then where our goal correction would be. The extent of correction in HTO depends on the underlying pathology and degree of osteoarthritis. When performing HTO with concurrent cartilage procedures, it is recommended to correct the postoperative mechanical axis to neutral or slight valgus.
Here, we are correcting her medial proximal tibial angle from 81.8° to 87.3°, and then you can see we are introducing nearly no sagittal correction. Furthermore, we can template where specifically our jig will sit on the medial proximal tibia exactly where our osteotomy will be, as well as our hinge point. You notice the hinge point is distal and lateral to the proximal tibial cortical margins. This is to avoid intraoperative hinge fracture either through the joint or out laterally. In the middle portion of the slide, you can see where our jig will sit. Now the nice thing about the jig for this system is it uses drilling to perform the osteotomy with theoretically reduced risk of thermal osteonecrosis that might be related to a saw. Following this, we can see what our proposed postoperative correction will look like. You can see that we corrected to approximately an 87° medial proximal tibial angle and introduced no changes to the posterior tibial slope, and then on the right, you can see where our plate will sit, and you can see that we will avoid the tibial screw from her prior ACL surgery.
In terms of positioning, the patient is positioned supine on a flat Jackson table, with a thigh tourniquet, an ipsilateral foot roll, and a lateral articulating post.
The procedure is a right knee arthroscopy, a right knee medial tibial plateau microfracture, right knee medial femoral condyle multiple plug OCA in a snowman configuration, and then right knee medial opening wedge HTO with PSI jigs and implants for HTO.
Here you can see intraoperative arthroscopic photos of the medial compartment. This is the medial proximal tibia prior to microfracture, and this is the status after microfracture. Next, you can see the intraoperative photos of the medial femoral condyle with complete cartilage loss, and then on the right, you can see after our arthrotomy where OCA plugs were inserted.
Here we demonstrate a brief video of the HTO with the PSI. The implant we used is manufactured by Bodycad.
Here is the medial knee arthrotomy for the allografts that had previously been performed and the medial side of proximal tibia is exposed up to the level of fascia. Here, we incise the medial tibia pes (pes anserinus) insertion and just above the pes (pes anserinus) insertion such that the pes (pes anserinus) tendons can be reflected posteriorly. Once this is complete, then we begin our medial collateral ligament (MCL) peel in an anterior to posterior direction. This is performed until we are around the backside of the tibia, and a retractor can be placed posteriorly to protect the posterior neurovascular structures during the osteotomy.
Here, we are elevating slightly under the patellar tendon for the osteotomy. Next, we insert our PSI jig on the medial side of the tibia. Here, the jig is placed and then holes for the jig are drilled as well as screws inserted. Now, once this is complete, we will obtain an intraoperative fluoroscopic radiograph to confirm the height of our osteotomy, which you can see here on the right. Once this is completed, the jig for the drill bits is placed and then the drilling of the osteotomy is begun. The flute lengths are predetermined so that there is a positive stop with all drilling, and the length of the drill is predetermined so that you do not exit out the posterior aspect of the tibia. Once this is completed, the anterior portion of the osteotomy is completed with the osteotome, removing all bridging bone between the drill sites. Once we are satisfied with this, the anterior portion of the jig is removed and, again, we will check the osteotomy and complete any remaining bridging bone that is present at that point. This is confirmed with a ruler to see if there is any residual bridging bone. Once we are satisfied that we are complete anteriorly, the posterior aspect of the jig central portion is removed, and then we check for any bridge and bone. Here, there is posterior cortex remaining, and so we are slowly working this with the osteotome, taking care to protect the posterior nerve structures with a retractor.
We continue working in the posterior aspect of the osteotomy here, until we feel that we are satisfactorily lateral enough. Next, we use the stack osteotomes to get a controlled expansion of our osteotomy site. Once we feel that we have adequately done this, then an expander guide is inserted into the jig, and here we begin expanding the osteotomy. We felt that we were not quite complete posteriorly, and here we are checking this with a ruler. So again, the osteotome is inserted posteriorly to complete the osteotomy. Once this is done, a wedge is inserted to the predetermined correction millimeter and then a guide specific to the patient is inserted and the proximal drill holes are performed.
Once this is done, we then insert our patient-specific implant, and this is held in place with pegs. At this point, we can confirm that we like our correction and that the plate is in the appropriate position under fluoroscopy. Then once we are satisfied with this, we begin inserting our screws in the proximal portion of the plate. Following completion of that, the diaphyseal screw holes are drilled and these screws are inserted as well. Finally, the osteotomy is irrigated and demineralized bone matrix with the bone marrow aspirate concentrate is inserted into the lateral portion of the osteotomy through the medial side and then a medial cortical cancellous wedge is placed.
These are our final intraoperative fluoroscopy views confirming adequate coronal plane correction and that we did not introduce any iatrogenic slope increase or decrease in the sagittal plane. These are our postoperative radiographs that are from a 2-week follow-up visit in the clinic, and these are postoperative alignment films that are obtained once the patient is weight bearing. Here we can confirm that we corrected to approximately 88° as we had planned in our preoperative template.
So, potential complications with the surgery include bleeding, neurovascular injury, and infection, and complications specific to HTO include intra-articular fracture, iatrogenic slope increase, and delayed union or nonunion, the latter 3 of which are hopefully obviated with the use of this PSI.
This is our postoperative rehabilitation protocol: touch down weight bearing with crutches is allowed immediately after surgery, with the knee kept locked in extension for the first 2 weeks. Return to sports is permitted approximately 9 to 12 months after surgery.
These are our criteria for returning to sports.
Next, we will review pertinent literature. In terms of return to sport after HTO, Bonnin et al 2 reported the case series of 139 patients who underwent HTO for varus deformity. They noted that 77% of patients were satisfied or very satisfied with their knee, and 66% of motivated patients returned to strenuous sports and 88% returned to intermediate levels of sports.
With regard to medial cartilage defects in the setting of HTO, Hsu and Bugbee et al 4 had looked at a case series of 17 patients who underwent this, and they noted an 88% survival rate on average of 8 years with 92% satisfaction. Two patients had failed at a mean of 9.3 years, and they had a 29% removal of hardware rate.
Looking at longer-term outcomes of HTO with associated cartilage surgeries, there is a systematic review of more than 4000 patients, they noted that patients who had isolated HTO have survivorship approximately 92% at 5 years. Those who underwent HTO plus articular cartilage surgery had 97% survival at 5 years, and those with HTO with meniscal transplant had 90.9% survival at 5 years. 3
So, in terms of how much to correct in the setting of cartilage surgery, Ackermann, Gomoll, and colleagues 1 looked specifically at this. They reported 168 patients who underwent ACI or OCA plus or minus HTO, and they compared patients one to one with OCA or ACI, and then they stratified by postoperative alignment. They found no difference in survival between patients with postoperative varus, neutral, or valgus angulated knees who underwent cartilage repair with OCA, regardless of concomitant HTO, suggesting that survivorship of OCA does not relate to a degree of correction.
In terms of the accuracy of PSI compared to other methods, Tardy et al 6 conducted a nonrandomized multicenter study comparing conventional, navigation, and PSI methods for HTO. They also evaluated the accuracy of PSI and found no statistically significant difference when comparing all 3 groups together. However, on pairwise intergroup comparison, a significant difference was observed only between the navigation and PSI groups, with PSI being favored.
So, in summary, approximately 75% to 90% of patients return to sport after HTO. Data are limited, however, regarding elite or professional athletes. Satisfaction rates after HTO are high, with improved pain and 77% being satisfied or very satisfied. Degree of HTO correction does not appear to affect survivorship of OCA.
High tibial osteotomy is not for everyone. Indications include those less than 65 years, isolated medial knee arthrosis, good range of motion, and no ligamentous instability. 5
These are our references.
Footnotes
Submitted March 2, 2023; accepted June 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.S. received support for education from Medwest Associates, Arthrex, and Smith & Nephew; hospitality payments from Stryker Corporation; and a grant from Arthrex. A.S.R. has stocks, stock options, or other ownership interest in Enhatch, Conformis (A.S.R.; sibling of A.S.R.), and Strathspey (sibling of A.S.R.); is a consultant for Stryker, Enhatch, Smith & Nephew, Anika, Bodycad, Xiros, NewClip, Ranfac, Marrow Cellution, Arthrex (sibling of A.S.R.), CeramTec (sibling of A.S.R.), and Cervos; received consulting fees from Heron Therapeutics; received education support from Gotham Surgical Solutions; serves on the speakers’ bureau for Pfizer; and receives royalties from intellectual property from Stryker (sibling of A.S.R.) and DePuy (parents or other ancestors of A.S.R.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.