
Abstract
Background:
Meniscal allograft transplantation improves functional and patient-reported outcomes in patients with meniscal deficiency without significant osteoarthritis. In addition, it is known that valgus malalignment of the knee can lead to meniscal and chondral damage, and surgery is often indicated to restore the mechanical axis and slow progression of osteoarthritis.
Indications:
Indications for this procedure include patients with symptomatic lateral meniscal deficiency with associated valgus deformity of the knee. Patient’s age must be less than 50 years, body mass index less than 35 kg/m2, meniscal deficiency, and ipsilateral pain with or without swelling. Ligament tears, focal cartilage loss, and malalignment are not contraindications if also corrected.
Technique Description:
We begin by removing the remaining lateral meniscus, taking care to leave a small peripheral rim of meniscus. A transpatellar tendon arthrotomy is performed, and the meniscal allograft is passed through the arthrotomy and into the knee. An inside-out repair is performed using vertical mattress sutures. The sutures are tightened and tied with the knee at 30° to 40° of flexion. The distal femoral osteotomy is then performed. An approach is made to the lateral femur, where initial guidewires are placed using fluoroscopic guidance. The initial saw cut is made about 75% of the way across the femur, and an osteotome is used to complete the osteotomy. Care is taken to preserve the far medial cortex. An adjustable wedge osteotome is placed to open the lateral cortex in accordance with the preoperative template. The cortical wedge is fashioned using the tibial allograft from the meniscal transplant and is placed into the osteotomy. The osteotomy is secured using a locking plate with locking screws, and this is confirmed in safe position using fluoroscopy prior to the conclusion of the case.
Results:
Patients will have effective deformity correction and alleviation of pain. Many patients can return to sport without restrictions following appropriate rehabhilitation.
Conclusion:
Lateral meniscal allograft transplantation with distal femoral opening wedge osteotomy is an effective treatment for symptomatic lateral meniscal insufficiency with associated valgus deformity of the knee in patients without osteoarthritis.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.
Video Transcript
This presentation is on the lateral meniscal allograft transplantation with distal femoral osteotomy, by Brett Meeks, Marisa Ulrich, Robert Duerr, and David Flanigan at The Ohio State University.
Our disclosures are listed below and available via the academy website.
Meniscal allograft transplantation improves functional and patient-reported outcomes in patients with meniscal deficiency without significant osteoarthritis.2,6 It is known that valgus malalignment of the knee can lead to significant meniscal and chondral damage, and surgery is often indicated to restore the mechanical axis and slow progression of osteoarthritis.4,5 This video will review the current literature, present our approach for meniscal allograft transplantation with distal femoral osteotomy via case example, and discuss published outcomes.
For background, the axis deformity of the knee is measured via the difference between the mechanical axis of the femur and the tibial shaft axis.1,3 Normal knee alignment is considered 1.1° of varus to 1.1° of valgus, and malalignment affects axial loading. Further studies have shown that malalignment negatively affects the menisci in the dependent compartments and that correction of meniscus pathology without correction of malalignment is associated with poor outcomes.9,10
Case presentation: This is a 20-year-old woman with a history of right knee pain for several years. She has had 5 prior right knee surgeries, with the most recent occurring 6 months ago. She notices daily swelling and mechanical symptoms, as well as pain.
There is no significant past medical history or medications. Relevant surgical history: in 2017, she had a tibial tubercle osteotomy for patellar maltracking. In 2019, she had a previous subtotal meniscectomy with 60% of the meniscus removed and saucerization for lateral meniscus tear and discoid meniscus, as well as removal of tibial tubercle osteotomy (TTO) hardware. She had 3 more arthroscopic knee surgeries with meniscus repair and/or partial meniscectomy.
Physical examination is significant for full, symmetric range of motion and a 1+ effusion. There is valgus deformity of about 3° correctable to neutral as well as positive hyperextension pain. There is lateral joint line tenderness and pain with meniscus provocative maneuvers. Ligamentous examination is stable, and strength is full and symmetric.
Weight-bearing anteroposterior (AP), Rosenberg, lateral, and sunrise radiographs of the right knee reveal that the joint space remains well-preserved with minimal degenerative changes noted.
The mechanical axis is measured on full length weight-bearing x-rays, drawing a line from the center of the femoral head to the center of the distal femur vs a line from the center of the proximal tibia to the center of the tibial plafond. In this case, the mechanical axis of the knee measured 3° of valgus on the right and 2° on the left.
Advanced imaging was obtained with a magnetic resonance imaging (MRI) of the right lower extremity. Sagittal, coronal, and axial images show evidence of previous lateral meniscectomy with subtotal meniscectomy. Overall, the cartilage surfaces are intact, and the medial meniscus is also intact.
The diagnosis is a previous right knee lateral discoid meniscus tear with subsequent subtotal meniscectomy and postmeniscectomy syndrome, as well as right lower extremity valgus malalignment.
Surgical indications for meniscal allograft transplantation includes age <50 years, body mass index <35, patients with meniscal deficiency, and ipsilateral pain with or without swelling. Ligament tears, focal cartilage loss, and malalignment are not contraindications if these are also corrected. Contraindications include patients who are asymptomatic, obese, those with concomitant inflammatory arthropathy, irreparable chondral lesions, uncorrected instability or malalignment, and Kellgren-Lawrence grade 3-4 arthritis.
Preoperative templating: We templated for a 3° correction to correct the mechanical axis to neutral which equaled a 5-mm opening wedge gap.
For this procedure, the patient is positioned supine with a lateral thigh post and a foot post is used to maintain 90° of knee flexion when needed. The thigh post is removed during the osteotomy, and a bump is placed under the knee. The patient is placed under general anesthesia, and intraoperative intraarticular injection is given with 20 ccs of 1% lidocaine with epinephrine. The tourniquet is inflated only if needed during the procedure.
The plan is for a first-stage diagnostic arthroscopy to confirm lateral meniscus deficiency with intact cartilage. Once this was confirmed, we proceed with a right knee arthroscopy with lateral meniscus allograft transplantation with concomitant lateral opening wedge distal femoral osteotomy. We will plan for 3° of correction with an opening wedge of 5 mm.
Following diagnostic arthroscopy confirming no significant chondral damage, we begin removing the remaining lateral meniscus with a biter and arthroscopic shaver. We left a small peripheral rim of meniscus and were careful to avoid the popliteus and capsule. Bleeding was verified.
Next, an arthroscopic shaver was used to perform a notchplasty for easier access to the posterior horn insertion site.
Next, we used a spinal needle to plan our trajectory between the anterior and posterior horns and then made a transpatellar tendon arthrotomy.
A radiofrequency device was then used to demarcate the area between the anterior and posterior horns.
The shaver was used to make a 4-mm trough in preparation for a lateral meniscal transplant guide. The guide pin was placed between the anterior and posterior horns within the trough, and the guide was secured down to the anterior cortex. A guide pin was then placed and exchanged with a smooth guide pin and then reamed with a 10-mm reamer to the hard stop leaving a 5-mm posterior wall.
Next, we used a box chisel to make a teardrop shape followed by a rasp to smooth the trough. On the back table, the meniscal allograft transplant was prepared. The graft was then shaped to fit into the teardrop sizer. We demarcated the posterior portion as well as the popliteal hiatus.
We placed a traction suture just posterior to the popliteal hiatus region and then made a lateral approach to the knee for an inside-out meniscus repair. The interval between the lateral head of the gastrocnemius and the lateral capsule was used and a speculum was placed here.
Two free needles on the traction sutures were placed just behind the popliteal tendon and then the traction sutures were retrieved through our lateral exposure. These were then tensioned while the allograft was brought through the arthrotomy and into the trough.
The meniscus is then flipped into its appropriate location with the aid of a blunt trocar, and the knee was cycled multiple times.
Next, we began repair of the meniscal allograft transplant. We started by performing an inside-out repair at the posterior meniscus where we placed 4 sutures in a vertical mattress configuration. We continued this pattern by placing 5 more anteriorly.
At the most anterior portion of the lateral meniscus, we placed 2 more outside-in sutures. All sutures were provisionally tightened and then tied with the knee bent at about 30° to 40° of flexion on the lateral aspect of the capsule. No fixation of the bone block is required due to the press-fit nature of the tear drop design. At this point, we were satisfied with the repair and the stability of the meniscal transplant. The wound was then copiously irrigated, instruments were removed, portals were closed, and the arthrotomy was closed in a layered fashion.
Next, we began our distal femoral osteotomy. A lateral incision was made from the lateral epicondyle in line with the femur shaft proximally. The iliotibial band was split in line with this incision, and the vastus lateralis muscle was elevated subperiosteally anteriorly and posteriorly. A split was made in the lateral intermuscular septum to allow placement of a lap pad and posterior retractor along the posterior cortex to protect the neurovascular structures.
The initial guidewire was then placed under fluoroscopic guidance across the medial femur just distal to the medial flare toward the adductor tubercle. A parallel pin guide was used to place a second pin. Again, using fluoroscopy, our initial saw cut was made about 75% of the way across the femur with the retractor protecting us posteriorly. A perpendicular biplanar cut was then completed with a smaller sawblade along the anterior cortex. A biplanar technique was used to decrease risk of cortical fracture.
Next, we used an osteotome to complete the osteotomy on the posterior cortex with care to preserve the far medial cortex. Once we were able to gap open our femur cut, we placed our adjustable wedge osteotome and opened the lateral cortex until the gap measured 5 mm which corresponded with our preoperative template. We then assessed our alignment using the alignment rod and fluoroscopic x-rays to confirm center position of the hip and ankle, and our alignment of the knee corresponded with our preoperative plan at neutral. A 5-mm cortical wedge was then fashioned from part of the tibial allograft from meniscal transplant and was then placed into the osteotomy using a bone tamp. We then placed a left medial locking plate for the right lateral femur as this fits appropriately against her bone and had a lower profile for this smaller degree of correction. Locking screws were placed into the distal portion of the plate to fill the 4 distal holes. We then placed a cortical screw in the hole just proximal to the osteotomy site to compress through the plate and then filled the remaining proximal holes with locking screws. The plate and screws were confirmed in safe position on orthogonal fluoroscopic views. The fixation was stable at the conclusion of the case. The wound was irrigated and closed in a layered fashion.
Postoperative AP and lateral radiographs of the right knee show the distal femoral lateral opening wedge biplanar osteotomy with hardware in appropriate position.
For the postoperative protocol, weeks 0 to 6 consist of the protection phase with toe-touch weight-bearing, immediate passive range of motion to 90°, and deep venous thrombosis prophylaxis with apixaban. Weeks 6 to 8 are early loading with discontinuation of the brace and advancement of weight-bearing 25% per week. Weeks 8 to 12 consist of return to function with endurance and balance, while weeks 12 to 24 are strengthening with avoidance of running and pivoting, and the full protocol is available online.
Return to sport is considered beginning at the 6-month mark. Criteria include full pain-free knee range of motion, normalized gait and jogging mechanics, isokinetic strength testing 80% or greater for the hamstring and quadriceps at 60° per second and 300° per second, no reactive effusion with sport-specific activity, and for neuromuscular control, we want appropriate mechanics and force attenuation strategies with high-level agility, plyometrics, and high-impact movements. Functional hop testing showing limb symmetry index greater than 90%.
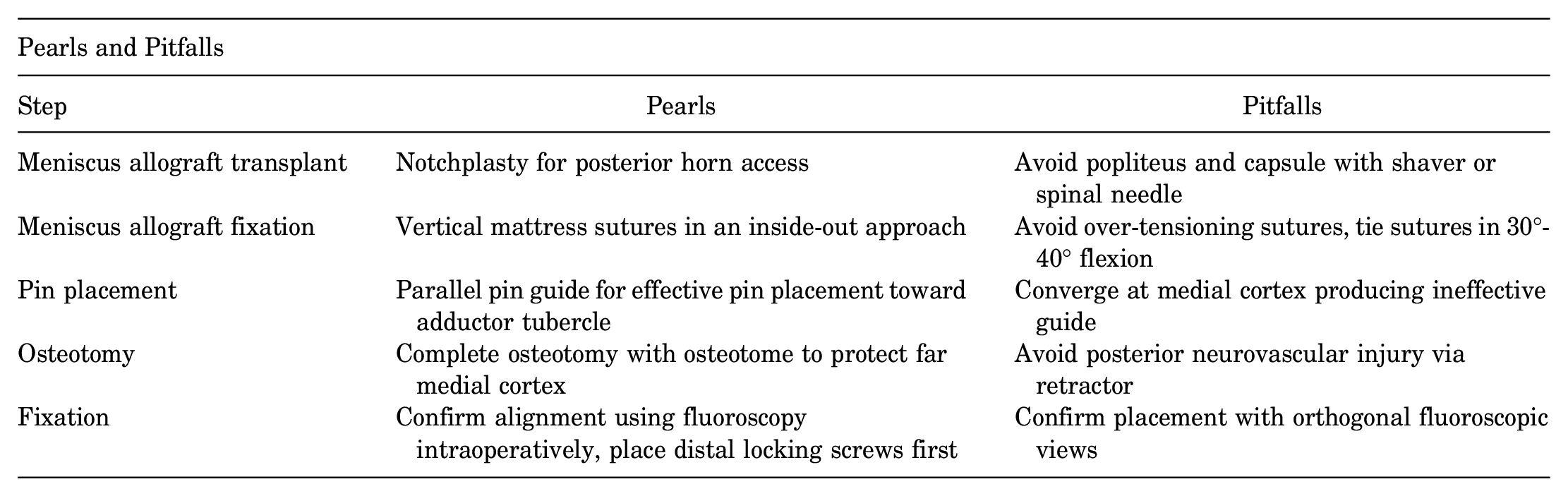
The following table lists technique pearls and pitfalls for each of the key steps. We would specifically like to highlight the pearls of using vertical mattress sutures in an inside-out approach and tying them in 30° to 40° of flexion to avoid over-tensioning, as well as using a parallel pin guide for effective pin placement toward the adductor tubercle.
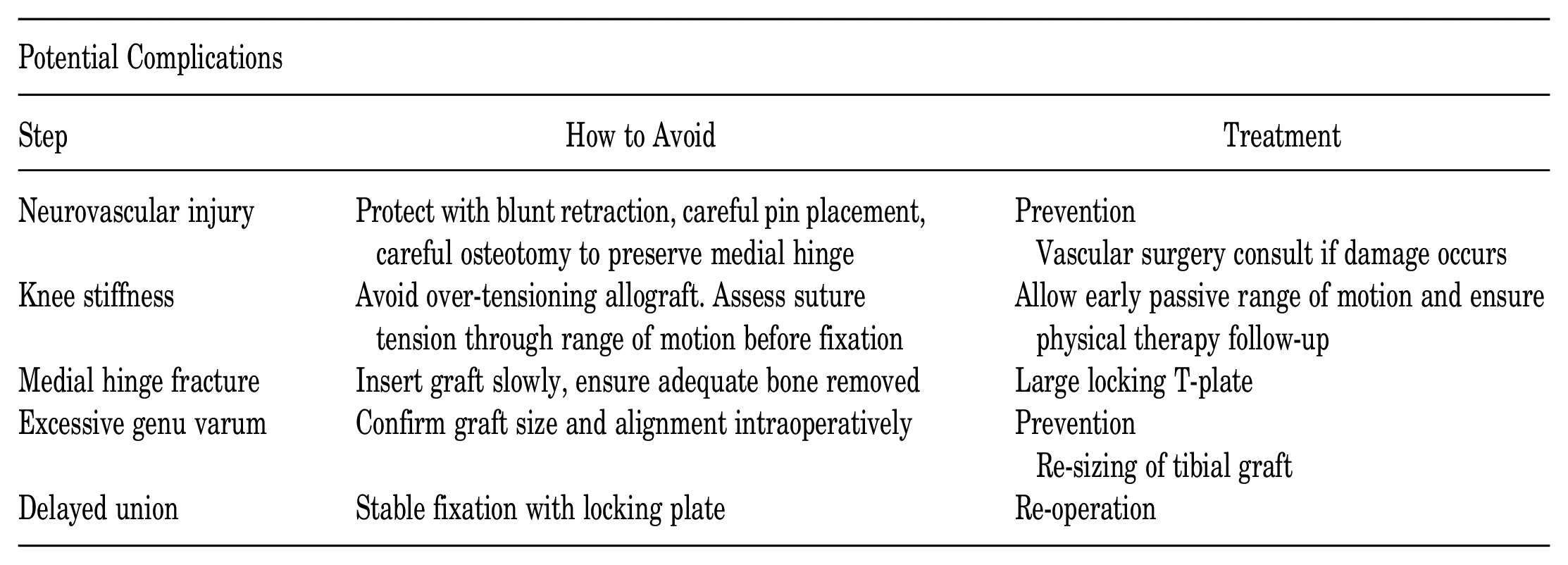
This table lists potential complications during the procedure, including neurovascular injury, knee stiffness, medial hinge fracture, excessive genu varum, and delayed union, as well as steps on how to avoid these complications and treatment should they be encountered. We would like to emphasize the importance of inserting the wedge allograft slowly and ensuring enough bone was removed so as to avoid a medial hinge fracture.
At 5 months post-operative, her osteotomy was well healed, and she was resuming activities per protocol.
Few studies evaluate outcomes following lateral meniscal allograft transplantation with distal femoral osteotomy. The study listed below by Puzzitiello et al 8 in Arthroscopy 2020 evaluated 21 patients who underwent lateral meniscal allograft transplantation with distal femoral osteotomy using similar techniques to those described here. Follow-up was 81% at a minimum of 2 years. All patients showed improvements in Visual Analog Scale scores, but 70% had persistent stiffness. Other complications described were persistent swelling, long-term pain, instability, and gait disturbances. Despite this, 82% of patients surveyed were able to return to some level of sport at an average of 17 months postoperatively.
The following study by Leong et al 7 in The Clinical Journal of Sports Medicine in 2019 assessed much of the recent literature on lateral meniscal allograft transplantation with distal femoral osteotomy using the lateral rather than the transpatellar approach. Although most patients demonstrated improved outcomes and return to sport, there were wide variations in allograft survival at long-term follow-up. The lack of consistent results and low sample sizes prevent reliable quantitative follow-up.
These are our references.
Footnotes
Submitted October 3, 2022; accepted December 22, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.