
Abstract
Background:
In cases of irreparable subscapularis (SSC) tendon tear in young and active patients, tendon transfers stand as the only surgical option. With a posterior-inferior-medial line of action and a synergistic action with the SSC muscle, the latissimus dorsi (LD) muscle appears to be the most adequate option.
Indications:
Indications include symptomatic and irreparable Lafosse type-IV or type-V SSC lesions in young and active patients with preserved glenohumeral joint.
Technique Description:
With the patient in the supine position under general anesthesia, a deltopectoral approach is used and extended distally so that the pectoralis major (PM) and long head of the biceps (LHB) tendons can be fully exposed and mobilized. The LD tendon is then exposed, freed from its humeral insertion to be prepared in a Krackow fashion, and extensively released from surrounding fasciomuscular adhesions to be freely mobilized proximally. The lesser tuberosity is prepared with a rongeur so that the LD tendon can be secured to cancellous bone on the former SSC insertion site with two rows of anchors. The rotator interval is then closed to prevent any extension of the existing tear to the superior aspect of the rotator cuff. Finally, the LHB is fixed to conjoint tendon in physiologic tension, and the surgical wound is closed.
Results:
With failure and revision rates ranging from 0% to 20%, this transfer seems as safe and reliable as other transfers. Unspecific complications were observed by different teams, but no cases of nerve compressions were reported. Conversely, significantly better functional outcomes are reported when using the LD muscle then when using the PM muscle as donor.
Discussion/Conclusion:
With a rather straightforward surgical technique, the open LD transfer seems to provide satisfactory short- to mid-term outcomes in cases of irreparable and symptomatic SSC tendon tear. Long-term results have yet to be determined, particularly regarding the prevention of glenohumeral osteoarthritis.
This is a visual representation of the abstract.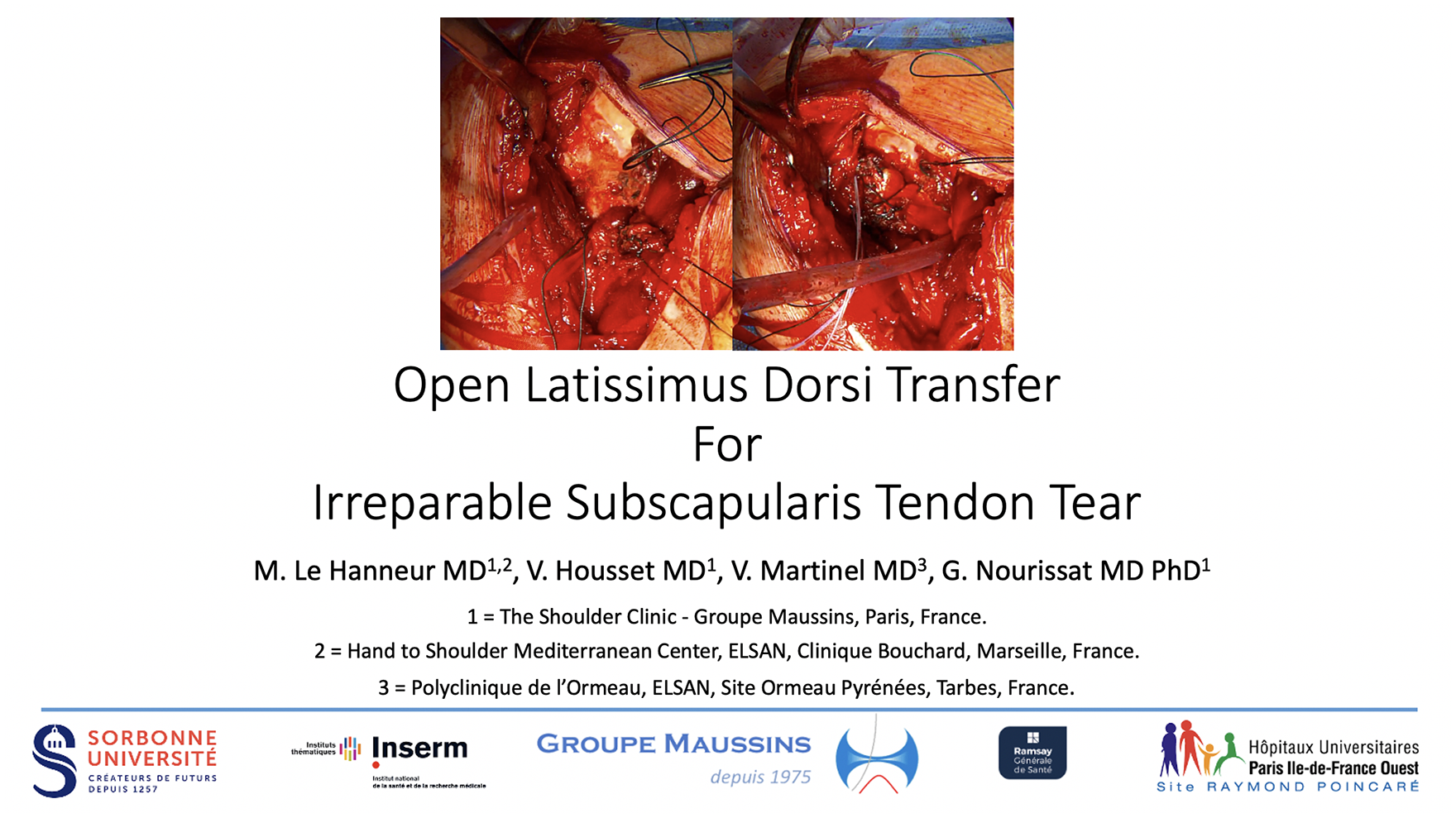
Video Transcript
In this video, we will present the surgical technique of the open latissimus dorsi transfer for irreparable subscapularis tendon tear.
Here is the overview of the video.
Subscapularis tendon tears have been classified by Lafosse and colleagues in 5 types of increasing severities, with types IV and V corresponding to complete lesions of the tendon. In cases of complete and irreparable tears, horizontal imbalance of the shoulder can be observed, leading to shoulder-anterior pain, shoulder-anterior instability, and active internal rotation weakness and/or loss, which can be detected clinically with the bear-hug test, the belly-press test, and the lift-off test. When combined with supraspinatus deficiency, vertical imbalance of the shoulder may occur, leading to a pseudo-paralytic shoulder.
When facing such dramatic presentations, two surgical options may be proposed to patients, including tendon transfers and reverse total shoulder arthroplasty (TSA). Since shoulder replacement should be avoided in young and active patients without glenohumeral osteoarthritis, tendon transfers stand as the only surgical option. Different muscles have been used as donors over the years, including pectoralis major, pectoralis minor, and latissimus dorsi (LD). While all these muscles have a synergistic action with the subscapularis muscle, namely shoulder internal rotation, the LD is the only one that has a posterior line of action, similarly to the subscapularis, thus producing compressive forces upon the glenohumeral joint and acting as a stabilizer. On the contrary, pectoralis muscles have an anterior line of action, subsequently producing shearing forces upon the glenohumeral joint and acting as destabilizers. Therefore, the LD appears to be the most adequate option as a donor.
In addition, the LD neurovascular bundle, namely the thoracodorsal nerve and artery, originates cranially from its entry points into the muscle belly; since the transfer proximalizes the LD muscle, the risk of stretching its pedicle is minimal. However, the two terminal branches of the posterior cord, namely the axillary and radial nerves, are passing superior and anterior to the LD insertion site, respectively, and great care must be taken to avoid any nerve impairment.
Commonly recommended indications of such procedure are young and active patients presenting with a symptomatic subscapularis deficiency due to irreparable Lafosse type-IV or type-V subscapularis lesions. Contraindications to this procedure are a non-transferable LD muscle, a massive and irreparable tear that involves the posterior aspect of the rotator cuff, and/or significant degenerative changes of the glenohumeral joint at the time of surgery.
Our illustrative case is a 51-year-old left-handed professional jockey, who suffered from a fall on his right shoulder while horseback riding. Based on an ultrasound examination in favor of a Lafosse type-IV subscapularis tendon tear, an attempt of repair was conducted in another center 2 months after the fall. Unfortunately, the surgeon found the tear to be irreparable intraoperatively. Since then, the patient felt some pain on the anterior aspect of the shoulder when using his arm but reported no instability, no motion limitation, and no weakness. On preoperative examination, ranges of motion were symmetric to the unaffected side, but belly-press and lift-off tests were positive.
Preoperative x-rays showed the previous attempt of repair, with two metallic anchors implanted in the lesser tuberosity, and excluded preexisting glenohumeral osteoarthritis.
Preoperative computed tomographic (CT) scan showed stage 3 fatty infiltration of the subscapularis muscle and excluded any supraspinatus impairment. CT arthrogram confirmed a type-IV subscapularis lesion, with a complete tendon tear retracted medial to the glenoid process and a centered humeral head, without concomitant supraspinatus tear and/or degenerative changes.
To perform this procedure in an open fashion, an extended deltopectoral approach is needed, so that the former subscapularis insertion site, as well as the pectoralis major (PM) entire insertion can be exposed. Tenotomies of both the long head of the biceps (LHB) and the remnant of the subscapularis tendon will then be performed, and extensive releases of the LHB and PM tendons will be conducted so that they can be freely mobilized. The LD tendon will then be exposed and progressively released from the humerus to be prepared in a Krackow fashion. Once prepared and freed from any surrounding musculofascial adhesion, the LD tendon will be mobilized proximally to the lesser tuberosity. The former subscapularis insertion site will be prepared with a rongeur, and the LD tendon will be secured to the lesser tuberosity with two rows of anchors, the first being medial and inferior and the second lateral and superior. Using a last anchor, the rotator interval will be closed. Finally, the LHB tendon will be sutured to the conjoint tendon in physiologic tension, according to Verbock technique.
Regarding our case, the patient was placed in the supine position under general anesthesia, with the affected arm resting on a table. The entire limb was drape-free, including the shoulder and the axilla.
A deltopectoral approach is made, starting at the coracoid process and extended 5 to 10 centimeters distal to the axilla. The deep surface of the deltoid is released from any adhesions, allowing exposing the former insertion site of the subscapularis tendon on the lesser tuberosity, with the conjoint tendon medially and the pectoralis major tendon distally. The bicipital groove is then widely opened, from the upper limit of the pectoralis major tendon to the rotator interval, so that the LHB tendon can be cut proximally and tagged with a strong suture; its remnant intraarticular part is excised. To expose the lesser tuberosity, the remnant part of the subscapularis tendon, if any, along with the medial glenohumeral ligament, are detached from the humerus, and tagged with a strong suture. The deep surface of the pectoralis major tendon is released from any adhesions to the conjoint tendon, so that the bicipital groove can be further exposed and opened distally. The pectoralis major is retracted anteriorly so that the LD tendon can be accessed and separated from the teres major. The latissimus dorsi tendon is then progressively detached from the humerus in a retrograde fashion and tagged with a strong nonabsorbable suture in a Krackow fashion. Once the latissimus dorsi is fully detached, the LHB tendon and the LD tendon are mobilized distally to ascertain that they are free from any adhesions that could restrain later mobilization.
Both tendons are then retrieved proximally, posterior to the pectoralis major tendon. Attention is directed to the lesser tuberosity, and the former insertion area of the subscapularis tendon is prepared with a rongeur to expose cancellous bone on its entire surface. A first row of anchors is inserted on the medial part of the insertion area; two self-tapping 4-strands loaded anchors are used, so that the latissimus dorsi tendon is first stabilized with two lasso-loop sutures on its superior and inferior edges, approximately 2 to 3 centimeters from its distal end, and then applied against the cancellous bone with two U-shaped sutures.
A second row of anchors is then inserted on the lateral part of the insertion area. Two self-tapping screwed anchors with eyelet are used, so that the sutures from the medial row and from the Krackow suture can be fixed laterally, in order to ensure optimal tendon-bone contact. A third self-tapping 4-strands loaded anchor is implanted at the superior end of the bicipital groove. The superior capsule is reinserted with two U-shaped sutures to close the rotator interval. Concomitant supraspinatus tears could be sutured at this time, whereas infraspinatus tears would require an initial arthroscopy to be fixed. Finally, the long head of the biceps is secured to the conjoint tendon, using strong nonabsorbable sutures, providing a tendon-to-tendon fixation. The excess is removed to avoid any impingement.
Intraoperatively, unsatisfactory exposure can be prevented by wide releases of both the deltoid, the PM and the LHB, which should be completely freed from its groove. To ease the preparation of the LD tendon, its physiologic tension can be preserved by progressive release of its humeral insertion. Once detached, the LD tendon must be extensively released, superiorly and inferiorly from fascial extensions to the medial intermuscular septum of the arm, posteriorly from the teres major, and medially from any fasciomuscular adhesions. Failure to perform such release will limit transfer mobilization and may lead to postoperative pain, motion limitations, and axillary and/or radial nerve compressions. In addition, the teres major should not be transferred concomitantly, since the bulk of its muscle belly and its more horizontal line of action may cause axillary nerve compression. Tensioning of the transfer should be such that the end of the LD tendon is flush with the proximal lateral aspect of the lesser tuberosity, as recommended by Elhassan and colleagues. Over-tensioning may lead to axillary nerve compression and/or shoulder internal rotation contracture while insufficient tensioning will result in shoulder internal rotation weakness. Similarly, tensioning of the LHB should be made accordingly to its physiologic tension to avoid postoperative muscular pain and/or cramps. Rotator interval closure limits the risk of further extension of the tear to the rotator cuff superior aspect and the subsequent shoulder vertical imbalance. A double-row fixation of the non-tubularized LD tendon onto the lesser tuberosity will ensure a satisfactory tendon-bone contact area and potentiate transfer healing. In case of transfer failure, depending on the patient’s symptomatology and functional requirements, several options may be contemplated, including another transfer (eg, bipolar teres major transfer), reverse TSA, or glenohumeral fusion.
After surgery, the patient was placed in a shoulder sling in the operating room, positioning his shoulder in adduction/internal rotation, and he had to keep it in place for 6 weeks. Physiotherapy was started on the third day after surgery, with pendular mobilization as well as passive abduction and flexion of the shoulder. Six weeks after surgery, active elevations and rotations were authorized, without resistance and/or stretching. Three months after surgery, active motion against resistance and stretching exercises were started. Sports training was allowed from the fourth postoperative month, but competitions were only allowed from the seventh month.
Since the anatomic study of Elhassan and colleagues in 2014 that demonstrated the feasibility and safety of this transfer with respect to the surrounding nerves, several teams reported on the satisfactory clinical and functional outcomes that such procedure may provide. Unspecific complications were observed, but no cases of axillary and/or radial nerve compression. With failure and revision rates ranging from 0% to 20%, Luo and colleagues noted no significant difference with those experienced when using the PM as donor. Conversely, the authors observed significantly better functional outcomes when using the LD as donor than when using the PM. If those short- to mid-terms outcomes are rather attractive, further studies are mandatory to assess the long-term outcomes that such procedure can provide, especially regarding the prevention of glenohumeral joint degenerative changes.
Thank you for watching.
Footnotes
Submitted July 14, 2021; accepted October 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This article’s publication fees were funded by COS Ramsay Santé. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.