
Abstract
Purpose
The purpose of the study was to evaluate factors associated with pneumococcal vaccination among non-Hispanic Black adults with type 2 diabetes mellitus (T2DM).
Methods
A cross-sectional, online survey was conducted in December 2023 using a Qualtrics research panel. Eligible participants were adults 19 years and older and non-Hispanic Blacks who self-reported a T2DM diagnosis. The survey comprised 55 items across 5 sections based on the health belief model. Descriptive and bivariate analyses and hierarchical binary logistic regression were used for data analysis.
Results
There were 330 eligible participants. Two-thirds received at least 1 dose of the pneumococcal vaccine. Participants had a mean age of 51.4 ± 16.8 years; 63.9% were women. Higher perceived susceptibility and higher cues to action were significantly associated with pneumococcal vaccination. However, higher perceived susceptibility, higher severity, geographical location, and history of influenza vaccination emerged as significant predictors, and improved model predictive ability for pneumococcal vaccination was observed (Akaike information criterion = 384.1 vs 423.5) after controlling for sociodemographic and other factors (education level, income, geographical location, diabetes-related complications, treatment types, frequency of health visits, influenza vaccination history, pneumococcal disease history, general vaccine beliefs, perceived mistrust).
Conclusion
Clinical, public health, and health policy programs should address these factors in planning educational campaigns and strategies to increase pneumococcal vaccination among non-Hispanic Black individuals with T2DM.
Diabetes mellitus is the 8th leading cause of death globally, affecting 589 million adults, with 38 million adults in the United States living with diabetes.1 -3 Type 2 diabetes mellitus (T2DM), the most prevalent form of diabetes (90%-95% of cases), is a chronic metabolic disorder characterized by insulin resistance and impaired glucose metabolism, leading to persistent hyperglycemia.4,5 The burden of T2DM is disproportionately borne by racial and ethnic minority groups, including non-Hispanic Black adults.6 -8 The prevalence of T2DM is higher compared to non-Hispanic White adults, with estimates indicating that 12.1% of non-Hispanic Black adults are diagnosed with diabetes compared to 6.9% of their White counterparts. 9
Non-Hispanic Black adults with T2DM are at heightened risk for severe microvascular and macrovascular complications compared to other racial and ethnic groups.10,11 Compared to other racial groups, poor glycemic control among non-Hispanic Black individuals with T2DM contributes to susceptibility to infectious diseases, such as pneumococcal disease.12 -14 Pneumococcal disease poses a significant public health challenge among non-Hispanic Black individuals with T2DM.15 -17 Pneumococcal disease is caused by Streptococcus pneumoniae and has been attributed to severe outcomes, including community-acquired pneumonia, invasive pneumococcal disease, meningitis, and bacteremia, contributing to substantial morbidity, mortality, and health care expenditures.18 -23 Pneumococcal coinfections have been observed in hospitalized COVID-19 cases.24,25
Pneumococcal vaccination is recommended for individuals with T2DM, and 1 to 3 doses are recommended in a lifetime based on age, type of vaccine, risk factors, immunity status, and shared clinical decision-making.26,27 Despite the effectiveness of pneumococcal vaccines,28 -30 pneumococcal vaccination rates in non-Hispanic Black individuals remain the lowest (40.8%) compared to other racial groups (44.3%-60.1%). 31 Prior studies in the general population among individuals with T2DM have identified several factors that influence vaccination behaviors, including limited access to health care, lack of knowledge regarding vaccine recommendations, and mistrust of the health care system.32 -34 Social determinants of health, such as socioeconomic status, education level, and geographic location, have been found to influence pneumococcal vaccination uptake.35,36 However, gaps remain with no studies conducted on factors related to pneumococcal vaccination among non-Hispanic Black adults with T2DM in the United States. Furthermore, the use of evidence-based theoretical models to explore factors influencing pneumococcal vaccination is sparse.
The health belief model (HBM) is a theoretical framework used to understand and predict health-related behaviors by examining individuals’ beliefs about health conditions and preventive actions.37 -40 It encompasses 7 key constructs: perceived susceptibility (belief about the likelihood of developing a condition), perceived severity (belief about the seriousness of the condition and its consequences), perceived benefits (belief in the efficacy of the preventive action), perceived barriers (perceived obstacles to taking action), self-efficacy (confidence in one’s ability to take action), cues to action (triggers prompting the behavior), and modifying factors.37 -40 Modifying factors are individual characteristics and contextual elements that influence health behaviors indirectly by shaping beliefs about susceptibility, severity, benefits, and barriers.39,40 HBM is widely applied in health promotion to design interventions that address these constructs and encourage behavior change.37 -40
Due to non-Hispanic Black adults’ increased susceptibility to severe pneumococcal disease, poor glycemic control, and worse health outcomes and persistently low pneumococcal vaccination rates,10 -17 investigating factors impacting pneumococcal vaccination among non-Hispanic Black adults with T2DM is important. Understanding these factors can inform targeted interventions to address pneumococcal vaccination disparities and prevent long-term pneumococcal-related complications in this high-risk population.
This study used the HBM to explore factors related to pneumococcal vaccination among non-Hispanic Black adults with T2DM. The study objectives were to describe pneumococcal vaccination status and the HBM constructs, evaluate bivariate associations between HBM constructs and pneumococcal vaccination, and examine the predictive effect of the HBM constructs on pneumococcal vaccination.
Study Design, Questionnaire, and Methods
Study Design and Sampling
A cross-sectional, web-based study was conducted in the United States in December 2023. Study participants were recruited using Qualtrics research panel, which offers access to a diverse, nationwide pool of respondents located in the United States. Qualtrics employs a double opt-in process to ensure participant engagement and data integrity, with individuals first volunteering to join the panel and then being invited to participate in surveys based on eligibility criteria. The study eligibility criteria were adults 19 years or older, identification as non-Hispanic Black, self-report of diagnosis of T2DM, and pneumococcal vaccination status of yes or no. Eligible individuals received email invitations containing a secure link to the online survey, which included a description of the study purpose, an emphasis on voluntary participation, and informed consent information. Screening questions were used to confirm study eligibility prior to the start of the survey. Participants who consented were directed to complete the survey. Participants received an incentive determined as a percentage of the total survey cost; however, the exact amount was not disclosed by Qualtrics. A dedicated project manager from Qualtrics was responsible for overseeing the soft launch of the survey, managing its distribution, and coordinating data collection efforts. Ongoing communication and regular meetings were held with the project manager to ensure the data collection process was executed smoothly and per the study protocol.
With an alpha level of .05 and a power of .80, the minimum required sample size for detecting medium effect sizes was 242.
Study Questionnaire
The development of the study questionnaire was informed by literature and by adapting previous questions on HBM constructs and perceived mistrust items to align with the study population.41 -43 The survey questionnaire (Supplement 1) comprised 57 items across 6 sections: (1) knowledge of pneumococcal disease and vaccines, history of pneumococcal disease, and general vaccine beliefs (8 items); (2) HBM beliefs constructs (21 items); (3) perceived mistrust in health care settings (12 items); (4) diabetes-related characteristics (7 items); (5) sociodemographic characteristics (7 items); and (6) negative and positive factors affecting pneumococcal vaccination (2 items).
Study Variables
The dependent or outcome variable was pneumococcal vaccination status, defined as receipt of at least 1 dose of pneumococcal vaccine (yes/no). Independent or predictor variables consisted of HBM beliefs constructs (perceived susceptibility, perceived severity, perceived benefits, perceived barriers, self-efficacy, and cues to action) and modifying factors consisting of self-reported sociodemographic characteristics, including age, gender, relationship status, educational level, household income, health insurance status, and geographical location; diabetes-related characteristics, including diabetes duration, complications, treatment types, diabetes control status, perceived health status, frequency of annual health visits, and influenza (flu) vaccination history; and psychosocial and structural variables, including knowledge of pneumococcal disease and vaccines, history of pneumococcal disease, general vaccine beliefs, and perceived mistrust in health care settings.
The perceived mistrust in health care settings was measured by adopting the Group-Based Medical Mistrust Scale (GBMMS), a well-validated and reliable 12-item tool consisting of suspicion (6 items), discrimination (3 items), and lack of support (3 items) domains.43,44 The GBMMS has been extensively utilized in vaccination studies and among the Black population.43,44 However, some modifications were made to reflect the current scope of the study: “People of my ethnic group” was replaced by “Black people,” “ethnic groups” or “ethnicity” was changed to “race” and “doctors and healthcare workers” was changed to “healthcare workers.”
Overall, the question responses were in either categorical or continuous formats. However, 2 open-ended items were incorporated to evaluate the negative and positive factors influencing pneumococcal vaccination for pneumococcal unvaccinated study participants: “What makes it hard for you to get the pneumococcal vaccine?” and “What would make you want to get the pneumococcal vaccine?”
Before administering the survey, the questionnaire was content validated by 5 experts and piloted among 6 non-Hispanic Black adults with T2DM. Participants did not suggest any changes to the survey questionnaire.
Data Analysis
Data analysis was conducted using SAS version 9.4. A priori statistical significance was set at P < .05. For Objective 1, descriptive statistics were calculated to describe the dependent and independent variables, and data were presented using mean, ranges, percentages, and frequencies. The reliability of multiitems was evaluated with Cronbach’s alpha, and the acceptable level was set at values of α ≥ .60.
Chi-square and independent samples t tests were used to evaluate bivariate associations between the predictor variables and pneumococcal vaccination for Objective 2. Statistically significant modifying factors were selected for inclusion in the multivariate model. However, perceived mistrust in health care settings was included irrespective of its significance status due to its relevance in influencing vaccination in the Black community. The variance inflation factor (VIF) was used to assess multicollinearity, with <10.0 as an acceptable level.
Given the binary nature of the dependent variable, a hierarchical binary logistic regression model was utilized to address Objective 3. In this analysis, the HBM beliefs constructs were introduced in an initial model (Model 1). Subsequently, modifying factors were included in the model (Model 2) to assess whether these additional variables improved the model’s predictive capability for pneumococcal vaccination. Adjusted odds ratios (aORs) measured the association between predictor variables and pneumococcal vaccination. The Hosmer and Lemeshow goodness-of-fit test was conducted to determine if the multivariate model better captured the factors related to pneumococcal vaccination compared to the intercept-only model, with statistically nonsignificant levels indicating a good model fit. The model evaluation relied on criteria such as the Akaike information criterion (AIC) and −2 log-likelihood, with lower values indicating a better fitting model. The Wald chi-square test assessed the significance of aORs for variables in individual models.
Qualitative content analysis was conducted on free-text responses (negative and positive factors affecting pneumococcal vaccine receipt). Two members of the research team independently reviewed and categorized the responses. Consensus meetings were held to discuss codes and reach a final consensus on code names.
Results
Pneumococcal Vaccination and HBM Constructs
Table 1 displays the characteristics of study participants. Three hundred thirty eligible participants completed the study questionnaire. Of the 330 eligible participants, 66.4% (n = 219) reported receiving at least 1 dose of pneumococcal vaccine. Regarding sociodemographic characteristics, study participants had a mean age of 51.4 ± 16.8 years (range: 19-81 years), were predominantly women (63.9%) and nonpartnered (67.3%), had an above high school education (64.6%) and an annual income level of $50 000 or less (62.4%), were health insured (94.9%), and were from the US South region (61.2%). For diabetes-related characteristics, participants most frequently reported having a diabetes diagnosis of more than 5 years (46.4%), 1 to 2 diabetes-related complications (54.6%), treatment with oral medications (eg, metformin; 40.9%), moderate diabetes control (A1C 7%-8.9%; 49.7%), at least 1 annual health visit (97.0%), perceived health status as “good” (45.5%), and received influenza (flu) vaccination in the past year (65.5%). For psychosocial/structural variables, knowledge of pneumococcal disease and vaccines (3.9 ± 0.7) was above the medium knowledge rating. General vaccine beliefs (4.1 ± 0.7) reflected a slightly favorable score for vaccines. Perceived mistrust scores (2.8 ± 0.7) were slightly below medium perceived mistrust. Most participants reported no history of pneumococcal disease (65.5%). In terms of HBM beliefs constructs, perceived susceptibility (3.7 ± 0.7), severity (3.3 ± 0.8), and cues to action (3.4 ± 0.9) had above medium rating scores. However, perceived barriers (3.0 ± 0.9) had medium rating scores. Slightly high scores were reported for perceived benefits (4.1 ± 0.8) and self-efficacy (4.1 ± 1.0).
Characteristics of Study Participants
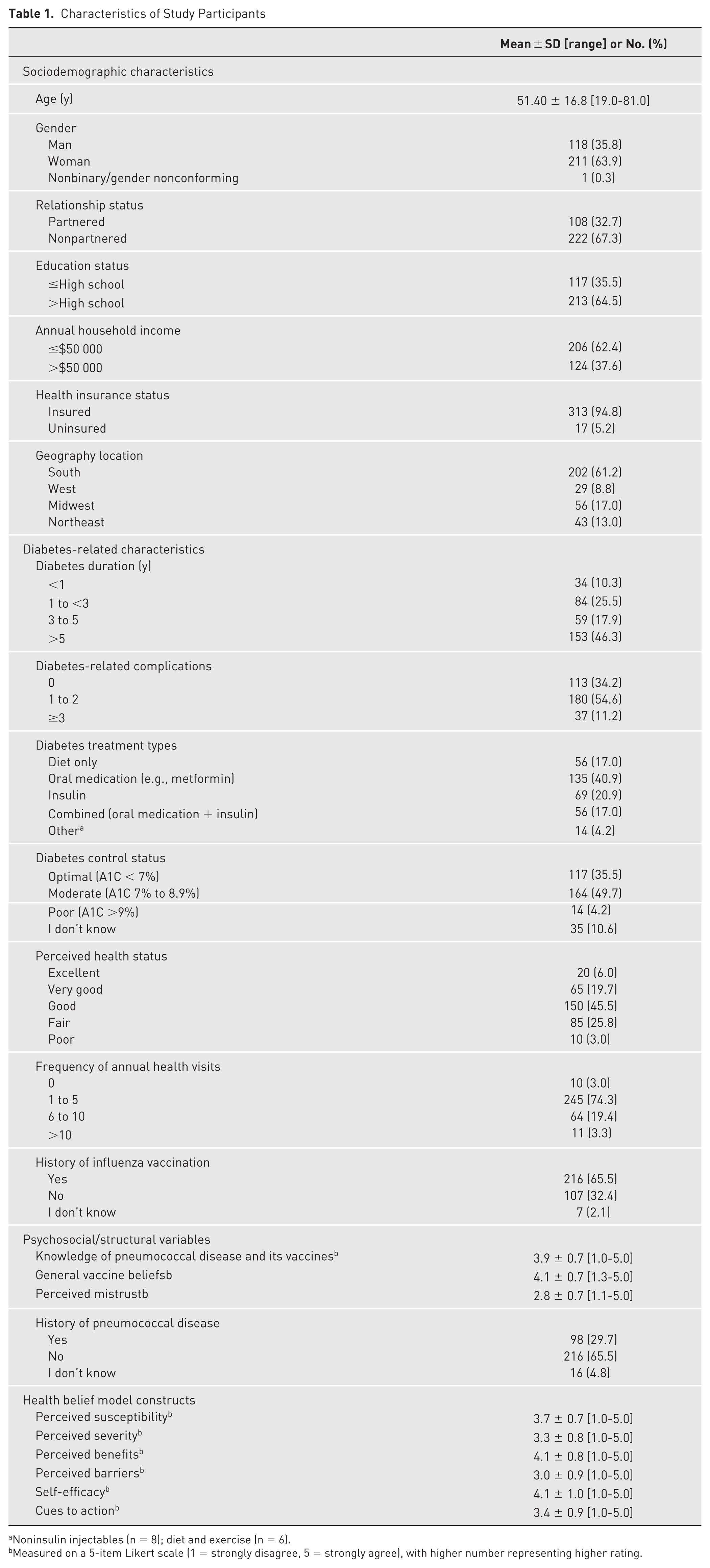
Noninsulin injectables (n = 8); diet and exercise (n = 6).
Measured on a 5-item Likert scale (1 = strongly disagree, 5 = strongly agree), with higher number representing higher rating.
Cronbach’s alpha scores were within the acceptable range (αs = .63-.88), except for knowledge items (α = .52). Therefore, the knowledge items were not included in the analysis. VIF values <10.0 were obtained, which implies the absence of multicollinearity. Response categories rated as “nonbinary/gender nonconforming,” “I don’t know,” and “other” were excluded from the data analyses.
Bivariate associations between HBM constructs and pneumococcal vaccination
Table 2 displays bivariate associations with pneumococcal vaccination. For sociodemographic characteristics, a significantly higher proportion of participants who reported pneumococcal vaccination had above high school education (χ2 = 6.7, 46.1% vs 18.5%; P = .01) and annual household income of $50 000 or less (χ2 = 6.6, 38.2% vs 24.2%, P = .00) and were from the U.S. South geographical location (χ2 = 18.3, 35.5% vs 25.8%, P = 0.00). Regarding diabetes-related characteristics, participants who reported 1 to 2 diabetes-related complications (χ2 = 13.6, 37.0% vs 17.6%, P = .00), oral medication as diabetes treatment type (χ2 = 12.0, 26.4% vs 14.6%, P = .01), annual health visits (χ2 = 11.3, 49.4% vs 24.9%, P = .01), and a history of influenza vaccination (χ2 = 85.1, 54.6% vs 10.9%, P < .00) showed higher proportion of significant associations with pneumococcal vaccination. General vaccine beliefs (t = 4.9, P < .00) and history of pneumococcal disease (χ2 = 21.0, P < .00) were the psychosocial/structural variables significantly associated with pneumococcal vaccination. For the HBM constructs, perceived susceptibility (t = 7.1, P < .00), benefits (t = 5.6, P < .00), self-efficacy (t = 4.2, P < .00), and cues to action (t = 6.0, P < .00) showed a significant positive association with pneumococcal vaccination. Perceived barriers (t = −2.1, P = .04) showed a significant negative association with pneumococcal vaccination.
Bivariate Analysis of Factors Associated With Pneumococcal Vaccination Among Non-Hispanic Black Adults With Type 2 Diabetes Mellitus
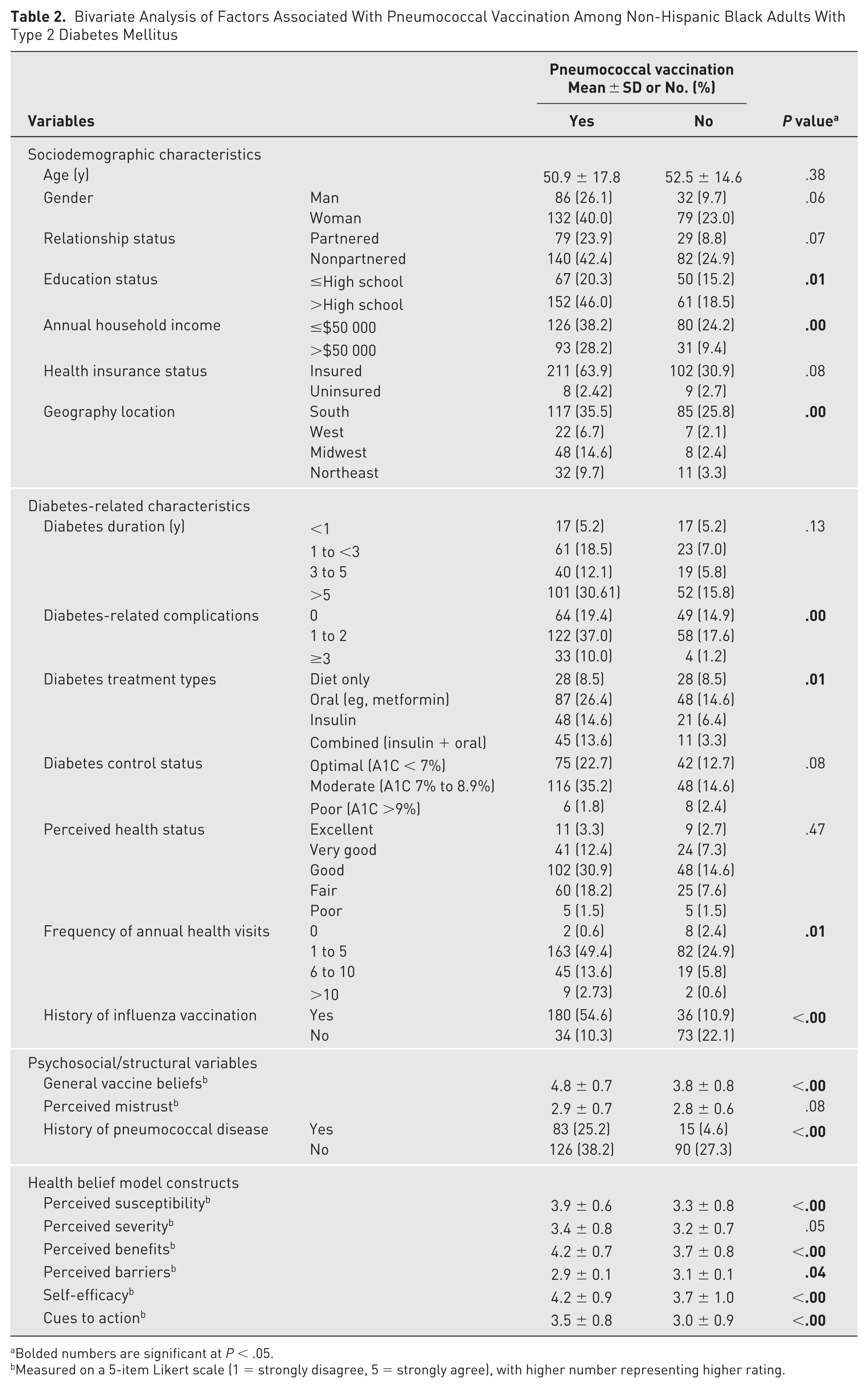
Bolded numbers are significant at P < .05.
Measured on a 5-item Likert scale (1 = strongly disagree, 5 = strongly agree), with higher number representing higher rating.
Predictive effect of HBM constructs on pneumococcal vaccination
Table 3 displays the results of the multivariate analysis of HBM constructs and pneumococcal vaccination (Model 1). The overall model was a good fit, χ2(8) = 6.8, P = .56, and significantly predicted pneumococcal vaccination, Wald χ2(6) = 52.1, AIC = 423.5, P < .00. Perceived susceptibility (aOR 2.8, 95% CI, 1.7-4.5, P < .00) and cues to action (aOR 2.8, 95% CI, 1.1-2.6, P = .01) showed higher odds of pneumococcal vaccination. Although perceived barriers showed lower odds of pneumococcal vaccination (aOR 0.7, 95% CI, 0.5-1.0, P = .05), this association was not statistically significant.
Multivariate Analysis of Health Beliefs Model Constructs Associated With Pneumococcal Vaccination Among Non-Hispanic Black Adults With Type 2 Diabetes Mellitus (Model 1)
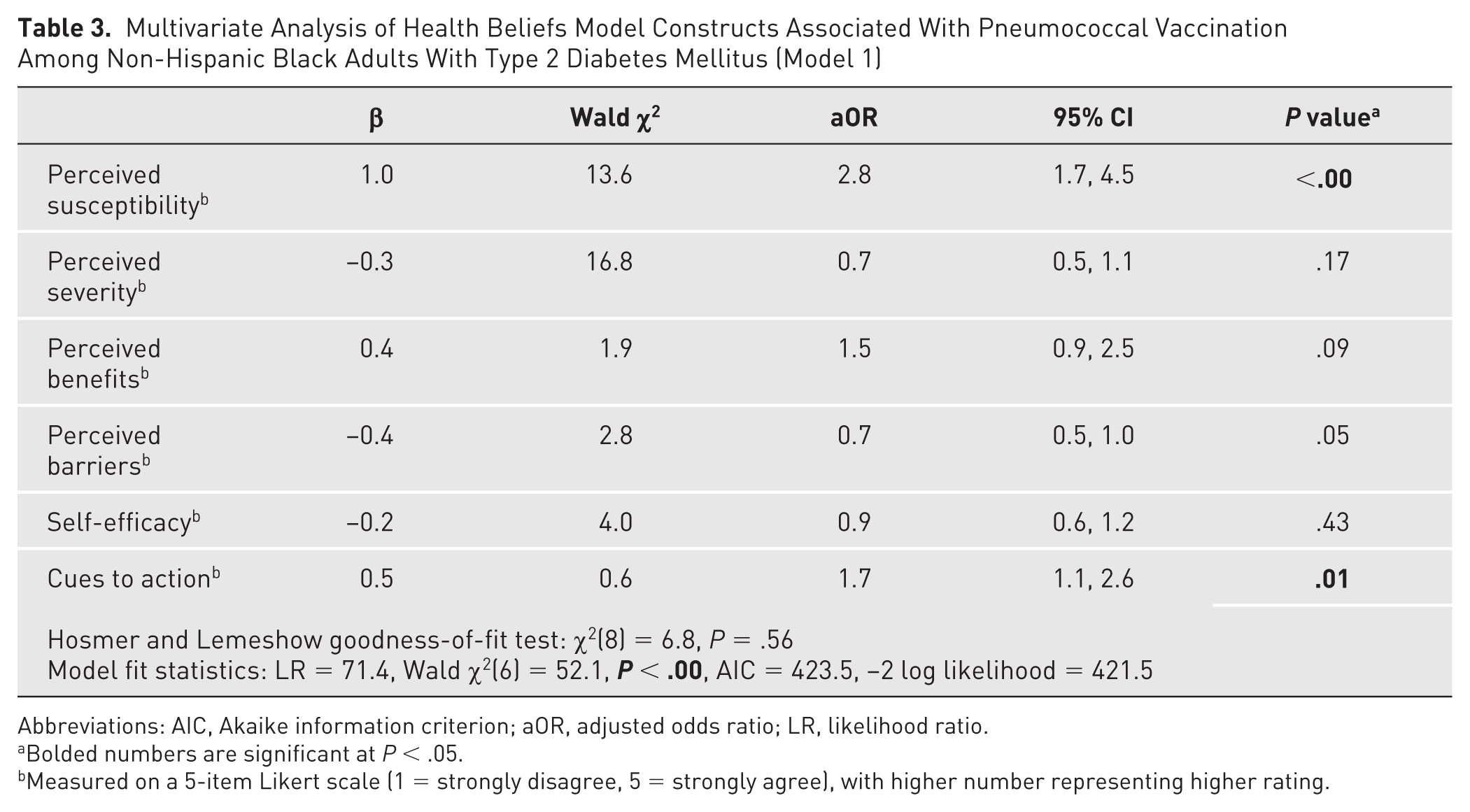
Abbreviations: AIC, Akaike information criterion; aOR, adjusted odds ratio; LR, likelihood ratio.
Bolded numbers are significant at P < .05.
Measured on a 5-item Likert scale (1 = strongly disagree, 5 = strongly agree), with higher number representing higher rating.
Table 4 presents the results of the multivariate analysis of HBM constructs and pneumococcal vaccination (Model 2). On inclusion of the significant modifying factors and perceived mistrust, Model 2 was a better fit, χ2(8) = 11.4, P = .18, and significantly improved the predictive effect on pneumococcal vaccination, Wald χ2(23) = 78.7, AIC = 384.1, P < .00, compared to Model 1. Perceived susceptibility was associated with higher odds of pneumococcal vaccination (aOR 2.6, 95% CI, 1.4-4.9, P = .00), and severity was associated with lower odds (aOR 0.5, 95% CI, 0.3-0.9, P = .03). A history of influenza vaccination (aOR 6.4, 95% CI, 3.0-13.4, P < .00) was associated with higher odds of pneumococcal vaccination. Compared to the US South, participants from the US Midwest showed higher odds of pneumococcal vaccination (aOR 6.5, 95% CI, 2.1-19.5, P = .00).
Multivariate Analysis of Health Beliefs Model Constructs and Modifying Factors Associated With Pneumococcal Vaccination Among Non-Hispanic Black Adults With Type 2 Diabetes Mellitus (Model 2)
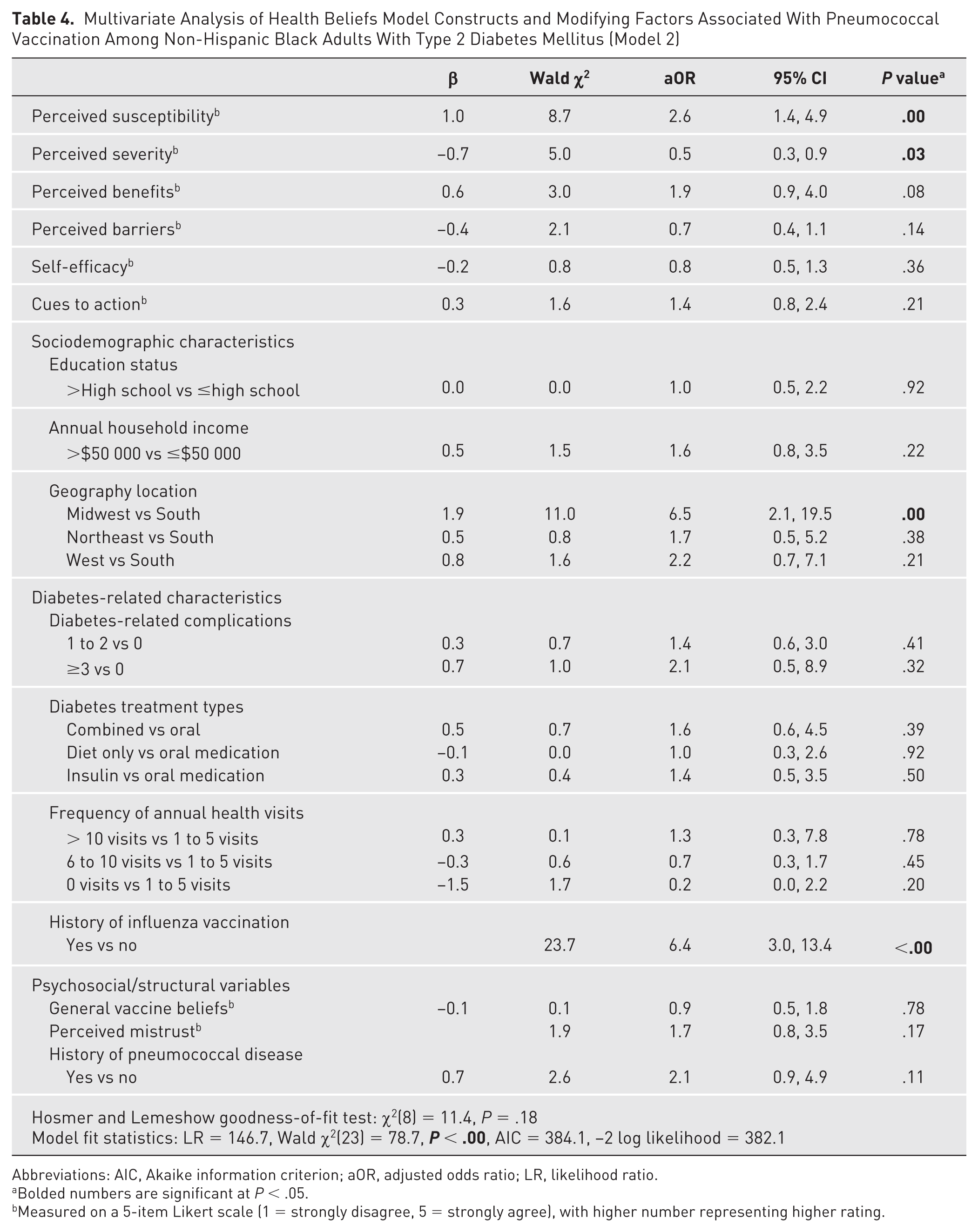
Abbreviations: AIC, Akaike information criterion; aOR, adjusted odds ratio; LR, likelihood ratio.
Bolded numbers are significant at P < .05.
Measured on a 5-item Likert scale (1 = strongly disagree, 5 = strongly agree), with higher number representing higher rating.
Content Analysis of Negative and Positive Factors Influencing Pneumococcal Vaccination
The qualitative content analysis conducted among pneumococcal unvaccinated participants is discussed in the following.
Negative factors influencing pneumococcal vaccination
Participants identified several factors that hindered pneumococcal vaccination. Vaccine-related barriers included mistrust, concerns about safety and side effects, and fear of needles. Accessibility challenges were also reported, such as inconvenient vaccination sites, unreliable transportation, busy schedules, and lack of health insurance. Many participants cited limited knowledge about pneumococcal vaccines, some unaware of their existence or benefits, whereas others noted the absence of health care provider recommendations. Despite these barriers, a few participants expressed willingness to discuss vaccination with their providers. Additionally, some participants mentioned personal health concerns about undesirable health outcomes based on age, T2DM, and overall health status as reasons for not vaccinating.
Positive factors influencing pneumococcal vaccination
Participants highlighted various factors that could influence their willingness to receive pneumococcal vaccines. Some expressed the need for more evidence of vaccine benefits, such as research demonstrating effectiveness and preventive effects against pneumococcal disease. Others noted that they might vaccinate if it protected against severe infections, was lifesaving, or had minimal side effects. Accessibility improvements, such as free and convenient vaccination at local pharmacies, were also seen as motivators. Increased information about vaccines, including their benefits and side effects, and recommendations from health care providers were critical for some participants. Additionally, participants indicated they would be more likely to vaccinate if facing significant health risks, such as chronic illnesses, life-threatening conditions, or susceptibility to pneumococcal-related complications.
Discussion
The sociodemographic profile of participants revealed predominantly middle-aged participants, aligning with the higher prevalence of T2DM in adults ages 40 to 59 years.1,2,45 Women comprised 63.9% of the sample, slightly exceeding national data showing comparable T2DM prevalence between genders in the Black population.45,46 Most participants (64.6%) had education levels above high school, indicating a moderately educated cohort, and 62.4% reported annual household incomes of $50 000 or less, consistent with national trends.47,48 A majority (94.8%) had health insurance, with a higher reliance on public insurance (52.4%) compared to national figures, potentially indicating fewer insurance-related barriers to vaccination. 48 Also, 42.4% of participants were single, and 61.2% resided in the southern United States, consistent with regional diabetes prevalence and population distribution.45,47,48
Nearly half of the participants had a T2DM diagnosis for over 5 years (46.4%), and more than two-thirds reported diabetes-related complications (65.8%), reflecting the disproportionate burden of diabetes among non-Hispanic Black adults.6 -14 Although 45.5% rated their health as good, nearly half (49.7%) had moderate diabetes control (A1C 7%-8.9%), consistent with literature indicating suboptimal management in this population.14,49 Most participants (74.2%) reported 1 to 5 annual health visits, aligning with the American Diabetes Association’s recommendations of at least 3 to 4 annual visits for T2DM management.50,51
Significant bivariate associations with pneumococcal vaccination were observed for higher education, higher annual household income, geographical location, higher diabetes-related complications, treatment types, frequent annual health visits, history of flu vaccination, history of pneumococcal disease, and positive general vaccine beliefs. Higher levels of perceived susceptibility, benefits, self-efficacy, and cues to action were significantly associated with pneumococcal vaccination. These findings align with findings from the literature highlighting the relevance of these factors on vaccination.41,42,52 -59
Model 1 showed that higher perceived susceptibility and higher cues to action were significantly associated with pneumococcal vaccination. These results align with existing literature highlighting the role of health beliefs in shaping vaccination behaviors.41,42,60 -62 However, after controlling for variables with significant bivariate association with pneumococcal vaccination obtained from Table 2 (education, annual household income, geography location, diabetes-related complications, diabetes treatment types, frequency of annual health visits, general vaccine belief, history of influenza vaccination, history of pneumococcal disease), including perceived mistrust (Model 2), perceived susceptibility and severity, history of flu vaccination, and geographical location (Midwest vs South) were significantly associated with pneumococcal vaccination, which aligns with previous studies.41,42,60 -62 Consistent with the HBM, individuals who acknowledged perceived susceptibility and severity to pneumococcal disease are more likely to be vaccinated.37 -42,60 -62 A history of influenza vaccination is a robust predictor of pneumococcal vaccination, aligning with findings from the literature that prior history of influenza vaccination has been associated with frequent health care interactions and willingness to receive recommended vaccinations.60,63 -66 Geographical location also played a significant role in pneumococcal vaccination, with respondents in the Midwest having higher odds of vaccination compared to respondents in the South. Regional disparities in health care access, health care provider engagement in preventive care, and local public health initiatives, including state-funded immunization and health literacy, could contribute to this variation.67,68 Compared to the South, the Midwest has a higher proportion of older adults. More integrated health care systems with emphasis on public health care and funding initiatives coupled with proactive community health initiatives could collectively contribute to a higher likelihood of pneumococcal vaccination. 69
Although perceived barriers and cues to action showed no significance in Model 2, results of the qualitative findings of unvaccinated study participants highlight their relevance to pneumococcal vaccination.60 -62 From the qualitative findings, respondents expressed concerns about safety, cost, accessibility, lack of health provider recommendation, mistrust, and vaccine hesitancy as barriers to pneumococcal vaccination, and this aligns with the literature32,36,70 -72 Despite this, respondents expressed interest in vaccinating based on health providers’ recommendations. Health provider recommendation is a key predictor of vaccination, and this aligns with the study findings that health care recommendation was the most frequently rated cue to action.54 -57 Health care providers’ recommendations are critical to pneumococcal vaccination, and proactive patient engagement can significantly influence vaccination.73 -75 Health care providers can utilize existing beliefs (perceived susceptibility and severity) and prior influenza vaccination history to encourage pneumococcal vaccination during routine diabetes care visits and annual influenza vaccination visits.43,44,60 -62,76 Although perceived mistrust was not significantly associated with pneumococcal vaccination in this study, as supported by the qualitative findings, mistrust of the health care system plays a relevant role in Black communities and their care-seeking behaviors.43,44,76 Culturally tailored interventions have been shown to enhance vaccination within Black communities.72 -74 Tailored educational initiatives emphasizing the heightened risks and severity of pneumococcal infections while highlighting its role in preventing pneumococcal-related complications and enhancing diabetes care management should be incorporated.43,44,71,73,76 Health care providers may consider engaging patients in codesigning and developing tailored messaging and recommendations to increase pneumococcal vaccination in non-Hispanic Black adults with T2DM.75,77
Health policy efforts should prioritize engaging Black communities through educational programs and transparent communication about the risks and severity of pneumococcal disease. To address access barriers, strategies such as home or telemedicine visits could be implemented to assess vaccination status, deliver targeted education, and administer pneumococcal vaccines, ultimately improving convenience and uptake across diverse geographical locations.75,77 -80 For geographical distribution, addressing disparities in access, education, infrastructure, and public health funding could help improve pneumococcal vaccination in the South. Collaborating with trusted sources, such as health care providers in public health campaigns, and aligning with cultural values to address specific concerns within the Black community can promote positive vaccine perceptions and disseminate accurate information. 80
Future research should include longitudinal studies to assess changes in beliefs over time, providing critical insights for public health strategies. Investigating the impact of beliefs on pneumococcal vaccination by geographical location and socioeconomic status could support the development of culturally sensitive interventions. Health care providers play a critical role in pneumococcal vaccination. Therefore, more research on health care provider education and its impact on vaccine recommendations among non-Hispanic Black adults with T2DM is essential. The influence of knowledge on pneumococcal vaccination warrants further investigation. In-depth qualitative interviews could offer a deeper understanding of vaccination beliefs and educational needs among non-Hispanic Black adults with T2DM, guiding the design of targeted educational materials and vaccination strategies.
Study Limitations
This study has several limitations. Its cross-sectional design captures perceptions at a single point, limiting the ability to observe changes over time. A longitudinal design could better assess temporal shifts in factors influencing pneumococcal vaccination. Additionally, the survey distribution may have introduced selection bias. The voluntary nature of participation could skew results because only motivated individuals may have enrolled. The utilization of a Qualtrics research panel as an online survey recruitment platform may introduce sampling bias, low-quality responses, limited control over participant identity, data security concerns, and platform-specific restrictions, which can compromise data reliability and generalizability.81,82 Recall bias is another concern because participants may have inaccurately reported past events, including their pneumococcal vaccination status, potentially leading to misclassification and confounding biases. Although the survey was distributed nationwide to enhance geographic diversity, the sample primarily comprised women, the southern United States, and those with health insurance. Thus, findings may not generalize to other genders, regions, or socioeconomic groups. However, given the high prevalence of diabetes among non-Hispanic Black individuals in the southern United States, these results may reflect broader trends within this demographic. Self-efficacy was assessed for general vaccine confidence rather than pneumococcal vaccination specifically, which may not fully capture participants’ confidence in receiving pneumococcal vaccine. This study did not inferentially analyze the role of knowledge on pneumococcal vaccination, and qualitative data collected via web-based open-ended questions may not fully represent participants’ perceptions. Nonetheless, this study offered valuable insights into barriers and motivators among non-Hispanic Black adults with T2DM across diverse geographic settings.
Conclusions
In conclusion, non-Hispanic Black adults with T2DM face heightened risks of pneumococcal infections and related complications yet demonstrate lower pneumococcal vaccine uptake compared to other racial groups. Hence, pneumococcal vaccination rates remain suboptimal. Factors such as perceived susceptibility, perceived severity, influenza vaccination history, and geographical location significantly influenced pneumococcal vaccine uptake, controlling for relevant covariates. The study underscores the importance of these salient factors in influencing pneumococcal vaccination among non-Hispanic Black adults. Targeted strategies that emphasize pneumococcal disease risk and severity awareness, leverage influenza vaccination as a gateway to pneumococcal immunization, and address regional vaccination disparities could enhance pneumococcal vaccination and reduce pneumococcal-related complications in this high-risk population.
Supplemental Material
sj-docx-1-tde-10.1177_26350106251371085 – Supplemental material for Factors Impacting Pneumococcal Vaccination Among Non-Hispanic Black Adults With Type 2 Diabetes: A Nationwide Cross-Sectional Study
Supplemental material, sj-docx-1-tde-10.1177_26350106251371085 for Factors Impacting Pneumococcal Vaccination Among Non-Hispanic Black Adults With Type 2 Diabetes: A Nationwide Cross-Sectional Study by Chinyere M. Okoh, Leticia R. Moczygemba, Carolyn Brown, Whitney Thurman, Anton L.V. Avanceña and Sharon Rush in The Science of Diabetes Self-Management and Care
Footnotes
Author Contributions
Study conceptualization: CMO, LRM; methodology: CMO, LRM, CB, ALVA, SR; study investigation: CMO; data analysis: CMO; data validation: CMO, LRM, CB, WT, ALVA, SR; data collection, cleaning, visualization, and analysis: CMO; original draft preparation: CMO; draft review and editing: CMO, LRM, CB, WT, ALVA, SR; study supervision: LRM; project management: CMO. All authors have read and consented to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and publication of this article.
Ethical Considerations
The University of Texas at Austin Ethics Review Committee approved the study (protocol code STUDY00005285) on November 22, 2023.
Consent to Participate
Informed consent was obtained from all subjects involved in the study. Consent was indicated before the start of the survey by clicking on the survey link. The consent statement was clearly outlined in the survey invitation letter and the web-based survey.
Data Availability
The data sets generated during and/or analyzed during the current study are not publicly available because the Ethics Review protocol did not indicate broad sharing of the data. Data will be available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.