
Abstract
Purpose
The purpose of this study was to explore age-specific differences in exercise barriers among females with type 2 diabetes (T2D).
Methods
An online survey explored psychosocial and logistical barriers to exercise among Australian females with T2D (≥18 years). Participants were categorized into younger (18-54 years) and older (≥ 55 years) age groups to explore age-related differences. The survey also collected sociodemographic, general health and T2D management data, and current physical activity (PA) levels and behaviors.
Results
A total of 119 females participated (younger: n = 36, age: 42.7 ± 9.6 years; older: n = 83, age: 66.8 ± 6.1 years). Although 57.1% reported being physically active, 77.1% of these individuals were not meeting the PA guidelines. Younger females more frequently cited barriers related to time constraints and lack of transport, and older females more frequently reported insufficient social support and not knowing how to initiate an exercise routine. Exercise knowledge and self-efficacy were low across all participants. Only 42.9% believed they could realistically meet the PA guidelines.
Conclusions
Australian females with T2D face distinct age-related barriers to exercise, highlighting the need for tailored strategies. Interventions should focus on improving exercise knowledge and self-efficacy while mitigating key barriers to enhance exercise self-management in females with T2D.
Regular exercise is a cornerstone of type 2 diabetes (T2D) self-management due to its multifaceted benefits on cardiovascular disease (CVD) risk factors, such as glycemic control, insulin sensitivity, blood pressure, lipid profile, and weight management. 1 This is reflected in the ADCES7 Self-Care BehaviorsTM framework, which highlights physical activity (PA) as 1 of the 7 essential behaviors for effective diabetes care. 2 The PA guidelines recommend that individuals living with T2D engage in at least 150 minutes of moderate- to vigorous-intensity aerobic activity per week and 2 or more sessions of resistance exercise to achieve optimal health benefits. 1 This recommendation is particularly pertinent for females, who face approximately 50% higher risk of developing and dying from CVD compared to males. 3 However, a recent meta-analysis found that among adults living with T2D, males are up to 65% more likely than females to meet the PA guidelines (odds ratio 1.65; 95% CI, 1.36-2.01). 4 This significant health disparity underscores a critical need for tailored interventions to overcome barriers to exercise self-management and improve cardiovascular outcomes for females with T2D.
Females with T2D experience numerous barriers to exercise, including low motivation, a lack of social support, embarrassment, and insufficient health care provider support.4,5 However, much of the existing literature on adults with T2D has focused on older females (> 50 years), with limited insights into factors influencing exercise self-management among younger females. In Australian primary care, females under the age of 55 experience significant disparities in CVD management compared to their male counterparts.6,7 Studies demonstrate that this group is often inadequately assessed for key CVD risk factors and is less likely to receive appropriate pharmacological intervention.6,7 These gaps in cardiovascular care combined with the rising T2D incidence in younger Australians 8 present a pressing need for effective exercise interventions. To better support females living with T2D in becoming physically active and meeting PA guidelines, a deeper understanding of age-related differences in exercise barriers is needed to guide the development of more personalized and impactful interventions. Therefore, this study aimed to explore potential age group differences in exercise barriers among Australian females with T2D.
Methods
Research Design
This study employed a quantitative cross-sectional survey design, which was chosen for its ability to assess associations between exercise barriers, self-reported behaviors, and demographic factors among Australian females with T2D at a single point in time. This approach is appropriate for identifying prevalent patterns and relationships in a population, making it ideal for understanding the challenges faced by this group. 9 The design also enabled efficient collection of data across a range of variables, facilitating the identification of key associations to inform targeted interventions.
Participants and Recruitment
Females with T2D were recruited through social media (Facebook, Instagram), the Diabetes Victoria website, and flyers posted around Deakin University (Victoria, Australia). Inclusion criteria required a self-reported diagnosis of T2D, self-identification as female, age 18 years or older, and currently residing in Australia. Due to the anonymous nature of the survey, clinical verification of T2D was not possible. Participants who did not report the duration since diagnosis were excluded. All participants provided informed consent. This research was approved by the Deakin University Human Ethics Advisory Group (reference: HEAG-H 116_2020).
Survey
An online survey examined exercise self-management among females with T2D. The survey consisted of up to 56 questions depending on participant responses and included tick responses, 5-point Likert scales (1 = not at all, 5 = extremely), and free-text responses. The questions collected sociodemographic information; PA levels; exercise knowledge, perceptions, and self-efficacy; and exercise barriers. The survey was developed by study investigators based on consensus statements on exercise for T2D1,10 and published surveys on female cardiovascular health 11 and PA behaviors in CVD populations. 12 The survey was hosted online through Qualtrics (Qualtrics, Provo, Utah, USA) between November 2023 and May 2024.
Sociodemographic information
Sociodemographic information included (1) personal information: age, sex, ethnicity, education, employment status, annual income, residential area, and living arrangement; (2) physical health measures of height and weight, with body mass index (BMI) calculated as kg/m2; (3) general health information: comorbidities, menopausal status, smoking status, alcohol consumption, perceived fitness levels, and perceived health and well-being; and (4) T2D management: T2D duration, A1C levels, medications, lifestyle modifications, and health care professionals consulted.
Physical activity and exercise
Participants were asked if they regularly engaged in ≥150 min/wk of PA for T2D management. Those responding “yes” were further queried about the duration of habitual PA (months or years), frequency of weekly exercise, and the estimated minutes per week spent in low-, moderate-, and vigorous-intensity exercise. The total weekly duration of moderate to vigorous PA (MVPA) was calculated by summing the time spent in moderate- and vigorous-intensity exercise, and this was compared to the PA guidelines. 1
Exercise barriers, knowledge, perceptions, and self-efficacy
Participants were asked to identify exercise barriers using predefined lists drawn from the literature,4,13,14 with the option to specify additional factors. Four questions assessed participants’ knowledge of exercise self-management, including exercise benefits, their familiarity with PA guidelines, considerations for safe and effective exercise (eg, timing workouts around meals and medications, subjective monitoring of exercise intensity), and sources of exercise information. Likert scales assessed satisfaction with primary health care provider guidance, perceived importance of exercise for T2D management, and confidence in performing regular PA. Participants estimated the minutes per week of low-, moderate-, and vigorous-intensity exercise they felt they could realistically achieve based on current exercise capacity and daily routine. Perceived MVPA capacity was calculated to determine the proportion of participants who believed they could meet the PA guidelines.
Statistical Analysis
Analyses were performed using Stata 18 (StataCorp, TX, USA). Missing data were not imputed. Normality was assessed using Shapiro-Wilk tests and visual assessment. Because all continuous variables were not normally distributed, data are presented as both mean (standard deviation) and median (95% confidence intervals). Categorical data are reported as frequency (%). Age was collected as continuous data and then categorized into younger (18-54 years) and older (≥ 55 years) groups for analysis. Comparisons between age groups were performed using Mann-Whitney U tests and χ2 analyses for continuous and categorical data, respectively. Fisher’s exact test was used in instances where >20% of cells had an expected count < 5. Where a significant difference was detected following χ2 analyses, 2-sample tests of proportions were performed. A P value <.05 was considered statistically significant.
Results
Participant Characteristics
A total of 150 respondents completed the survey. Duplicate responses (n = 15), respondents with an IP address outside of Australia (n = 10), and those unable to confirm their T2D status by providing a diagnosis duration (n = 6) were excluded. Descriptive data for the remaining 119 responses are shown in Table 1. Participants were between 22 and 87 years old. Most participants (69.7%) were older, with a mean age of 66.8 ± 6.1 years. Younger participants had a mean age of 42.7 ± 9.6 years. Ethnic minorities were underrepresented, with the majority identifying as Oceanian and/or British (84.0%). Only 4 respondents identified as Indigenous Australian.
Participant Characteristics a
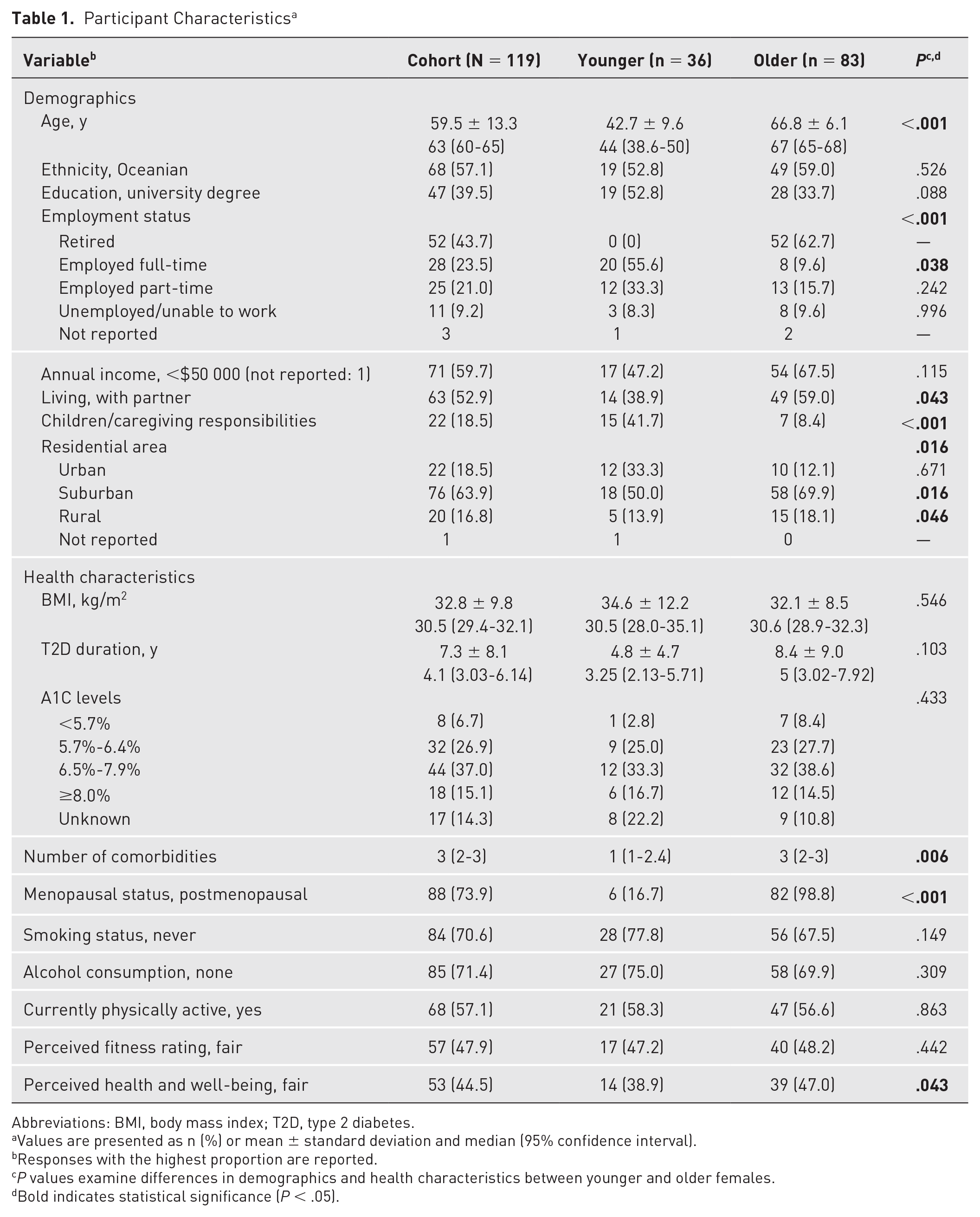
Abbreviations: BMI, body mass index; T2D, type 2 diabetes.
Values are presented as n (%) or mean ± standard deviation and median (95% confidence interval).
Responses with the highest proportion are reported.
P values examine differences in demographics and health characteristics between younger and older females.
Bold indicates statistical significance (P < .05).
The cohort had a median T2D duration of 4.1 years (95% CI, 3-6), and most (70.6%) had self-reported A1C levels <8.0%. The median BMI was 30.5kg/m2 (95% CI, 29.4-32.1), classifying most participants with obesity. Most typically did not consume alcohol (71.4%) and had either never smoked/vaped (70.6%) or had previously quit (24.4%; median quit duration: 16 years; 95% CI, 6-36). The majority self-reported as currently physically active (57.1%), but most rated their fitness level as fair or lower (83.2%). All but 1 older participant reported being postmenopausal, and one-third of the younger group reported they were perimenopausal (16.7%) or postmenopausal (16.7%). A higher proportion of older females rated their overall health and well-being as fair or good compared to younger participants (P = .043). No other significant differences were observed among health characteristics between age groups.
Participants were recruited from across Australia but were predominantly from Victoria (40.3%), New South Wales (28.6%), and Queensland (13.5%). Most younger females were working full-time or part-time (88.9%), and most older females were retired (67.5%). The majority of participants had completed vocational training or higher (77.3%) and had an annual income <$50,000 (59.7%). Although most participants resided in suburban areas (63.9%), a higher proportion of older females lived in suburban (69.9% vs 50.0%, P = .016) and rural areas (18.1% vs 13.9%, P = .046) compared to younger counterparts. Younger females less frequently lived with a partner (38.9% vs 59.0%, P = .043), and more had caregiving responsibilities compared to older females (41.7% vs 8.4%, P < .001). There were no other significant demographic differences between age groups.
Comorbidities
The most frequently reported comorbidities were obesity (60.0%), dyslipidaemia (47.8%), and hypertension (46.1%). Hypertension affected more older females compared to younger (53.2% vs 30.6%, P = .043). Only 12.6% of respondents reported no comorbidities, 37.0% reported having 1 or 2 comorbidities, and the majority (50.4%) reported having 3 or more of the listed comorbidities. Older females more frequently reported 3 or more comorbidities (57.8% vs 33.3%, P < .001). Three respondents did not report on their comorbidities.
T2D management
An overview of T2D management, including medications, lifestyle changes, and health care professionals consulted by participants, is provided in Table 2. Most participants were managing their T2D through 1 medication (most commonly Metformin, 68.1%) and lifestyle changes. Only 9 respondents (7.6%) had not made any lifestyle changes. Most had consulted with a general practitioner (GP; 92.4%) or diabetes educator (51.3%) regarding their T2D management. A higher proportion of older females had consulted a GP (96.4% vs 83.3%, P = .013) and podiatrist (51.8% vs 30.6%, P = .032) compared to younger participants. Only 3 respondents had never sought advice from a health care professional regarding their T2D management.
Type 2 Diabetes Management a
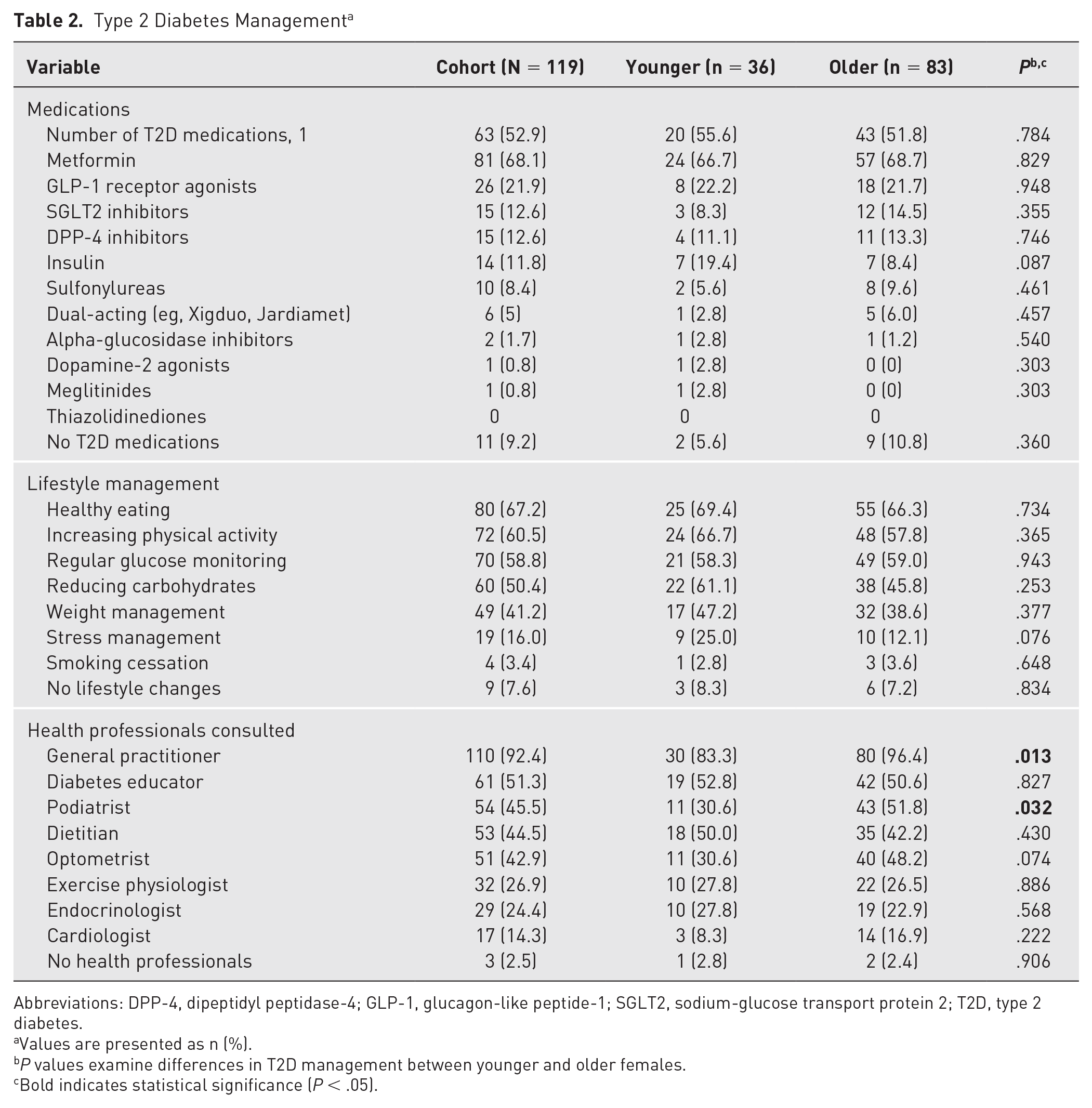
Abbreviations: DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SGLT2, sodium-glucose transport protein 2; T2D, type 2 diabetes.
Values are presented as n (%).
P values examine differences in T2D management between younger and older females.
Bold indicates statistical significance (P < .05).
Physical activity levels
A total of 68 (57.1%) respondents reported they currently exercised ≥150 min/wk. Most reported they were active on ≥3 d/wk (94.1%) and had maintained this routine for at least 1 year (69.1%). Of the current exercisers, 48 individuals (70.6%) provided estimates of their PA levels (Table 3). Participants reported a median of 120 minutes (95% CI, 60-150), 60 minutes (95% CI, 40-90), and 0 minutes (95% CI, 0-0) of low-, moderate-, and vigorous-intensity PA per week, respectively. The median total MVPA was 70 minutes (95% CI, 45-106). Over three-quarters (77.1%, n = 37 of 48) were not meeting the PA guidelines. No significant differences were observed in PA levels between younger and older participants (Table 3).
Self-Reported Physical Activity Levels a
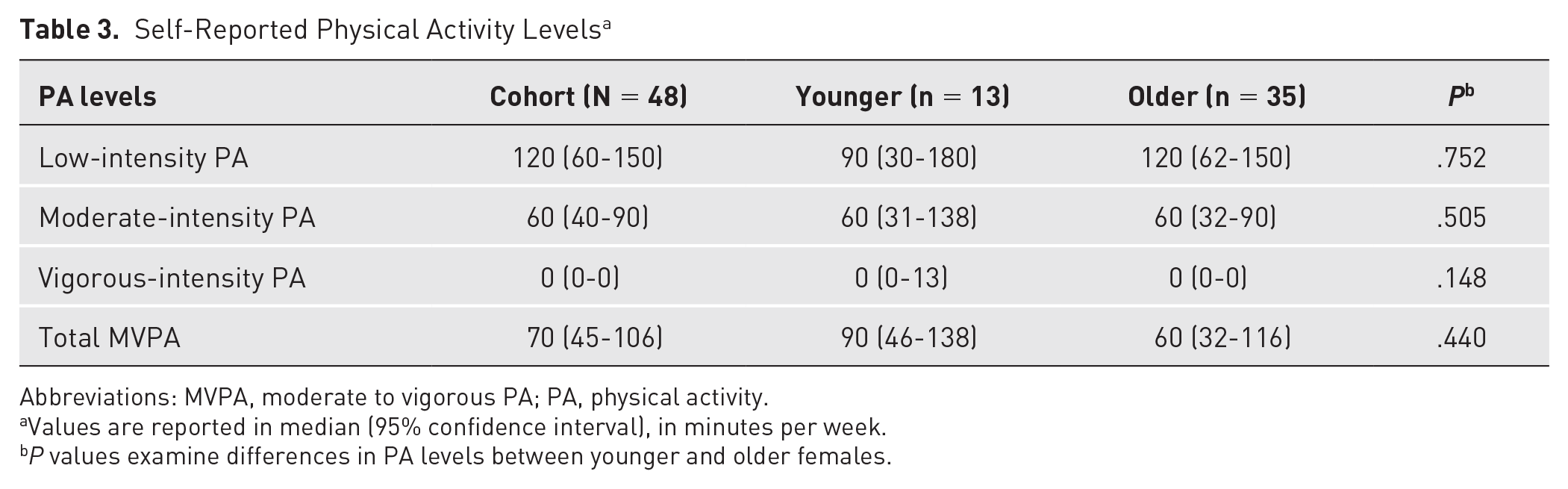
Abbreviations: MVPA, moderate to vigorous PA; PA, physical activity.
Values are reported in median (95% confidence interval), in minutes per week.
P values examine differences in PA levels between younger and older females.
Knowledge and perceptions of exercise for T2D management
Nearly all respondents (91.6%) believed that regular exercise was ‘very’ or ‘extremely’ important for managing T2D, and more than half (52.1%) associated it with improved quality of life. When asked about specific benefits, participants frequently highlighted improved weight management (89.1%) and glycemic control (83.2%). However, awareness of benefits for other CVD risk factors, such as hypertension (60.5%), dyslipidemia (45.4%), and insulin resistance (32.8%), was lower. Fewer than two-thirds identified that regular exercise was important for reducing the risk of cardiovascular events (62.2%) and other diabetes-related complications (56.3%).
Most participants reported low (49.6%) to moderate (31.1%) familiarity with the PA guidelines and demonstrated limited knowledge regarding key aspects of exercise self-management. This included gaps in their understanding of the appropriate timing of exercise around meals and medications (25.9%), recognizing symptoms of hypoglycemia (40.5%) and hyperglycemia (27.6%), and blood glucose management strategies, such as using fast-acting carbohydrates (22.9%) or monitoring ketones (13.6%). Additionally, there were deficits in knowledge regarding the appropriate frequency of exercise (38.1%) and types and intensities (24.6%) for optimal T2D management. Only 4 participants (3.4%) knew how to estimate exercise intensities using subjective measures such as the Borg rating of perceived exertion or talk test. Notably, 15 participants (12.7%) reported no knowledge of exercise self-management skills. The most frequently selected considerations were hydration (61.0%), proper foot care (57.6%), and appropriate exercise attire (49.2%). Older females were more likely to prioritize appropriate attire than younger counterparts (56.1% vs 33.3%, P = .027). No other significant differences were observed between age groups in responses to exercise knowledge and perceptions questions.
Sources of exercise information
The most frequent sources of information regarding exercise self-management were GPs (43.7%), followed by online sources (28.6%) and diabetes educators (26.9%). Only 21.8% reported obtaining information regarding exercise for T2D management from an exercise physiologist, and 10.9% had spoken to other exercise providers (eg, physiotherapist, personal trainer/gym staff). Very few cited diabetes educational programs (13.5%) or support groups (10.9%) as their primary sources of exercise information. Notably, one-quarter (26.9%) had never received or obtained exercise information regarding T2D self-management. Only one-quarter (26.9%) were satisfied with health care provider guidance, although a large proportion were neutral (42.9%). There were no significant differences in how exercise information was obtained or satisfaction with professional guidance between age groups.
Exercise self-efficacy
Most participants (73.1%) expressed ‘moderate’ or ‘low’ confidence in their ability to engage in regular exercise. The median MVPA was 120 minutes (95% CI, 83-161; Table 4), with fewer than half (42.9%) believing they could meet the PA guidelines. Participants, especially older females (P = .048), generally felt they could not perform vigorous-intensity exercise. One older participant did not report on exercise self-efficacy or perceived MVPA capacity.
Perceived Capacity for Physical Activity a
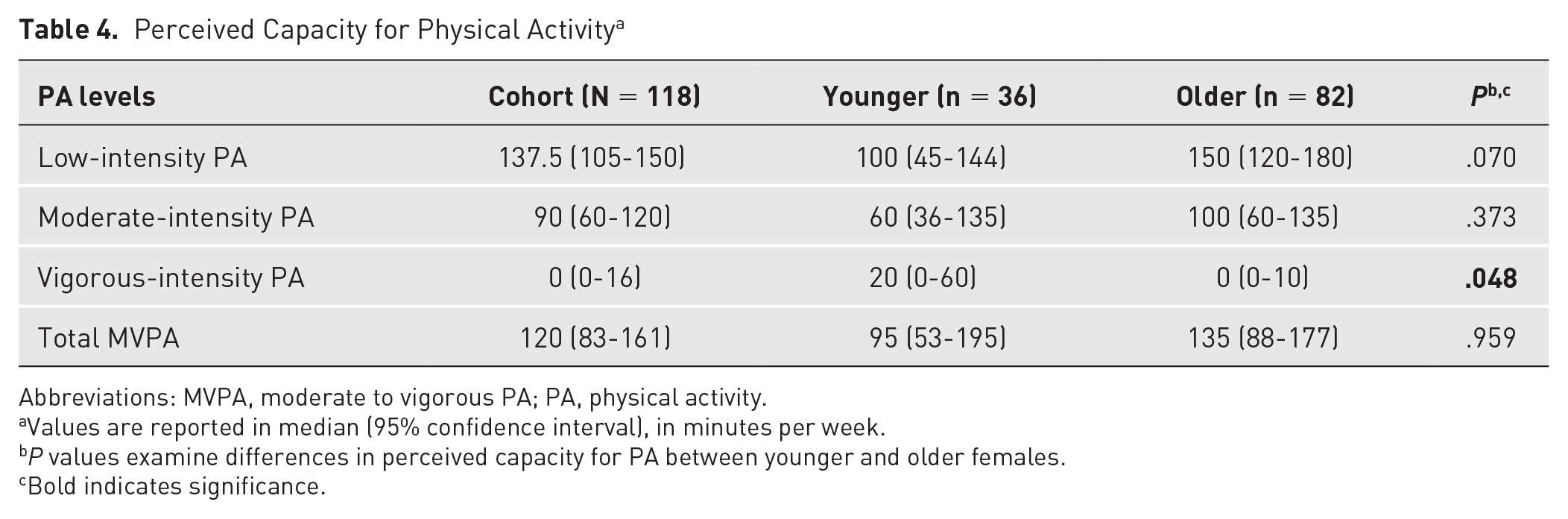
Abbreviations: MVPA, moderate to vigorous PA; PA, physical activity.
Values are reported in median (95% confidence interval), in minutes per week.
P values examine differences in perceived capacity for PA between younger and older females.
Bold indicates significance.
Exercise barriers
The most frequently reported barriers were low motivation (64.7%), cost (42.0%), lack of time (37.8%), and lack of social support (32.8%; Figure 1). Significant differences between age groups were identified for lack of time, χ2(1) = 14.922, P < .001; lack of social support, χ2(1) = 4.162, P = .041; not knowing how to start, χ2(1) = 2.744, P = .098; and lack of transport, χ2(1) = 4.579, P = .032. Older females more frequently reported barriers of social support (38.6% vs 19.4%, P = .001) and starting exercise (31.3% vs 16.7%, P = .003) but less frequently reported time (26.5% vs 63.9%, P < .001) and transport (4.8% vs 16.7%, P < .001; Figure 1). Unsurprisingly, lack of time was a greater barrier for females who were employed (full-time or part-time; both, P < .001) or had caregiving responsibilities (P = .001).

Proportions (%) of reported exercise barriers by age group.
Females who were currently inactive more frequently reported low motivation (78.4% vs 54.4%, P = .005), insufficient social support (45.1% vs 23.5%, P = .010), not knowing how to start (43.1% vs 14.7%, P = .003), physical discomfort (41.2% vs 23.5%, P = .019), and lack of access to tailored programs and advice (31.4% vs 13.2%, P = .017) as barriers to exercise. Perceived MVPA capacity was significantly lower if females reported barriers of physical discomfort (median: 50 minutes vs 160 minutes, P < .001), existing health concerns (50 minutes vs 148 minutes, P = .017), or low self-efficacy (33 minutes vs 140 minutes, P = .006). Females who reported physical discomfort or health concerns as exercise barriers had significantly higher BMI values compared to those without these barriers (median: 34.3kg/m2 vs 29.4kg/m2, P = .004 and 32.9kg/m2 vs 29.7kg/m2, P = .017, respectively). The median number of comorbidities was higher for barriers related to physical discomfort (4 vs 2, P = .004), health concerns (4 vs 2, P = .001), untailored programs/advice (4 vs 2, P = .006), and lack of health care provider support (3 vs 2, P = .018) but lower for those reporting time constraints (2 vs 3, P = .001).
Discussion
This study comprehensively explored barriers to exercise among younger and older females with T2D. The key finding was significant age-related differences in perceived barriers. Specifically, younger females more commonly reported time constraints (63.9% vs 26.5%) and transport barriers (16.7% vs 4.8%), whereas older females more frequently cited insufficient social support (38.6% vs 19.4%) and uncertainty about how to initiate an exercise routine (31.3% vs 16.7%). Additionally, exercise knowledge and self-efficacy were low across age groups. Despite 57.1% of participants reporting being physically active, 77.1% of these individuals were not meeting the recommended MVPA. Furthermore, only 42.9% of the cohort believed they could realistically achieve the PA guidelines. These findings highlight critical areas for targeted interventions to improve PA participation and health outcomes in this population.
The most commonly reported barriers among participants were low motivation, cost, and lack of time, consistent with challenges faced by the general population.15,16 Additional barriers included insufficient social support, the physical discomfort of exercise, and self-consciousness, which reflect the additional challenges faced by females managing T2D.4,14 This study builds on previous research by highlighting significant age differences in exercise barriers, underscoring the necessity of considering age-appropriate solutions.
For younger females, who were more frequently employed or caregiving, time constraints were their primary challenge. This contrasts with previous research on exercise barriers in females with T2D, which has primarily focused on older age groups. 4 However, these findings align with a prior investigation in individuals with diabetes (45% female), where perceived time barriers were significantly associated with physical inactivity in those younger than 60 years but not in older adults. 17 Providing flexible and time-efficient exercise options may be key to increasing exercise participation among younger females. Given that younger females in the current study perceived greater capacity for vigorous-intensity exercise, low-volume high-intensity interval training (HIIT; <15 min/session at 80% to 100% VO2max or HRmax) may be an effective time-efficient strategy, offering comparable benefits to high-volume HIIT and moderate-intensity continuous training.18-20 Although transport barriers were more commonly reported by younger females, they appeared to play a minor role across age groups. Home-based programs and digital technologies (eg, apps, wearable devices) can enhance accessibility and convenience, addressing multiple barriers, such as transport, time constraints, cost, and feelings of self-consciousness.21,22 These strategies have demonstrated effectiveness in improving PA levels and health outcomes in older adults with T2D and may hold promise for younger females.23-25
In contrast, older females more frequently reported barriers related to a lack of social support and uncertainty around starting an exercise routine. Strategies to address these barriers could include encouraging family involvement and promoting peer support initiatives. Family support in diabetes self-management has been linked to benefits such as improved glycemic control, lipid profile, and compliance with diet and exercise recommendations. 26 Moreover, partner involvement in diabetes exercise management has been associated with greater perceived social support and increased engagement in self-reported leisure-time MVPA and objectively measured energy expenditure.27,28 Because older females in the current study were more likely to live with a partner, integrating partner encouragement or coparticipation into exercise routines presents a promising opportunity. However, females may prefer to seek support outside the family.29,30 Peer support initiatives, such as peer-led self-management programs and diabetes support groups, can address this need 31 and may also reduce uncertainty about initiating an exercise routine through exercise education and support. Such initiatives have been shown to improve self-efficacy and self-management in people living with T2D. 31 Despite these benefits, the present findings suggest that diabetes education and support groups are underutilized by Australian females with T2D, highlighting the need for greater promotion and integration of these resources into routine care.
Females with T2D predominantly relied on their GP for exercise advice, with approximately three-quarters never consulting an exercise professional, such as an accredited exercise physiologist (AEP), for their T2D management. This aligns with research on low GP referrals to AEP services in Australia.32,33 GPs often lack the time and training to provide individualized exercise prescriptions. 34 Therefore, strengthening referral pathways to AEPs (and other allied health services, eg, diabetes educators) could ensure patients receive specialized care to overcome barriers and support their exercise adherence. In Australia, the Medicare system covers up to 5 AEP sessions annually, which can help alleviate financial barriers. 34 Exercise referral schemes to improve access to exercise specialists and support PA participation are also available in countries such as the United States, Canada, Europe, and New Zealand. 35
In addition to perceived exercise barriers, the findings revealed significant knowledge gaps that can further hinder exercise engagement among females with T2D. 36 Although most recognized exercise as important for T2D management, their understanding of specific benefits, PA guidelines, and self-management skills was limited. Participants primarily associated exercise with weight management and glycemic control, with little awareness of its role in managing other comorbidities and CVD risk. These findings align with prior research indicating that health care provider discussions with females often focus on exercise and weight management while overlooking comprehensive CVD risk management.37,38 Additionally, nearly half of respondents (49.6%) reported low knowledge of exercise recommendations for managing T2D, which was also reflected in the substantial discrepancy between self-reported PA levels and the exercise guidelines. Knowledge deficits were also evident in areas essential for self-management, including timing exercise around meals and medications, monitoring and responding to hypoglycemic/hyperglycemic events, and appropriate exercise frequency, types, and intensities, which may reduce confidence and limit independent exercise participation. Given that few studies have assessed participants’ deeper comprehension of exercise benefits or practical aspects of exercise self-management,36,39 these findings highlight critical knowledge gaps that if addressed, could improve long-term adherence and disease management in females with T2D.
Several limitations warrant consideration when interpreting these findings. The reliance on self-reported data may introduce social desirability bias, whereby participants respond in a manner they perceive as more socially acceptable. 40 Additionally, the use of an online survey can lead to challenges in adequately describing the population because there is no clear sampling frame. 41 The self-selection nature of online surveys also introduces sampling bias because individuals more motivated or interested in the topic may be more likely to respond. 41 As a result, findings may not be generalizable to all females with T2D in Australia, particularly those from ethnic minorities backgrounds, who were underrepresented. Moreover, PA levels were only collected from participants who self-reported as physically active, which may limit the generalizability of the conclusions. Finally, challenges recruiting younger participants restricted the exploration of more nuanced age-related differences, particularly in the context of the menopausal transition in middle-aged females. Nonetheless, this comprehensive exploration of exercise barriers among females with T2D provides actionable insights to guide the development of tailored interventions for this disproportionately affected population. Future studies should aim for targeted recruitment strategies to better represent younger females, allowing for more detailed comparisons between age groups. Additionally, efforts to validate self-reported data against objective measures (eg, accelerometers) could enhance the reliability of findings. Finally, complementing surveys with qualitative interviews could offer deeper insights into the unique barriers faced by females with T2D and help to further tailor interventions to address these challenges.
Conclusions
This study provides novel insights into the unique exercise barriers among females living with T2D and across different age groups. The findings suggest that Australian females with T2D would benefit from exercise self-management programs tailored to address both age-specific barriers and broader gaps in knowledge. Such programs should emphasize education on appropriate exercise prescription and self-management skills to help females with T2D meet PA guidelines. Further research is warranted to evaluate the efficacy of targeted exercise support programs in improving exercise participation and cardiovascular outcomes in females living with T2D.
Footnotes
Author Contributions
SO, MK, KW: conception and design of research and survey; SO: data collection and analysis; SO: drafted manuscript; SO, MK, KW: edited and revised manuscript and approved final version.
Declaration of Conflicting Interest
The authors declare no conflicts of interest, financial or otherwise.
Funding
No external funding was received for this study.
Ethical Approval and Informed Consent
This study was approved by the Deakin University Human Ethics Advisory Group (reference: HEAG-H 116_2020). All participants provided informed consent before taking part in the study.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.