
Abstract
Purpose
The purpose of this study was to explore the determinants of diabetes self-management education and support (DSMES) program engagement among Asian Americans with type 2 diabetes living in California.
Methods
A qualitative descriptive study was conducted to explore DSMES experiences. Semistructured interviews with Filipino, Korean South Asian, Cambodian, Taiwanese, and Vietnamese Americans were conducted. Participants were recruited through outreach, referrals, and social media. All 12 interviews were audio-recorded and transcribed verbatim. The data analysis used a rigorous, iterative approach, beginning with open coding to generate initial codes, developing a codebook, and proceeding to a second coding level and thematic analysis to interpret key patterns.
Results
Analysis revealed 4 major themes and 10 subthemes organized using the ecological model. The major themes are (1) individual-level barriers and facilitators (microsystem), (2) cultural and social influences (mesosystem), (3) structural barriers (exosystem), and (4) optimizing DSMES for inclusive diabetes care (macrosystem).
Conclusion
Study findings highlight the need for culturally responsive DSMES programs, emphasizing family-centered approaches and prioritization of cultural beliefs. Improving DSMES engagement among Asian Americans requires multilevel interventions addressing systemic and individual barriers, highlighting the complex interplay of cultural, social, and structural factors in diabetes management.
Diabetes has become a quiet epidemic in the United States. Approximately 38 million Americans have it, and about 90% to 95% have type 2 diabetes mellitus (T2DM). 1 T2DM is a progressive disease that can lead to heart disease and stroke, kidney disease, neuropathy, eye damage, dementia, and amputations. An additional 97.6 million adults have prediabetes, a condition in which it could potentially be reversed or managed, yet many remain unaware of their status. 2 T2DM disproportionately affects historically and contemporary marginalized groups, such as Asian Americans. The disparity in T2DM burden in Asian Americans, the second largest minoritized group in the United States, is clear: Asian Americans are 40% more likely to be diagnosed with T2DM and 60% more likely to have end-stage renal disease compared to non-Hispanic White individiuals. 3 As an aggregate, Asian Americans tend to have a lower prevalence of T2DM compared to other racial or ethnic groups in the United States. However, when data are disaggregated, it reveals significant disparities within the Asian American subgroups. For instance, Filipino Americans (12.2%) and South Asian Americans (10.8%) have some of the highest prevalence rates of T2DM, often exceeding those of the general population. 3
Diabetes Self-Management Education and Support Programs
Effective diabetes self-management approaches have been shown to reduce complications and morbidity 4 ; however, these approaches require sustained efforts because T2DM necessitates extensive medical and self-management. 5 Adding to this complexity are the social determinants of health in which individuals work and live. 6 Ethnic enclaves, where many Asian Americans reside, are frequently associated with disparities in health care access and quality due to geographic, economic, and sociopolitical barriers that shape health care delivery and health outcomes within these communities.7,8 Such disparities include the availability and utilization of various health care resources, such as diabetes self-management education and support (DSMES) programs. 9
Evidence suggests that DSMES programs are an essential health care resource for helping individuals with T2DM navigate the complexity of diabetes management. 5 DSMES programs connect individuals with clinical services in their communities, offering support at diagnosis, annual assessments, during critical transitions, or at the onset of new complications affecting self-management. Grounded in evidence-based guidelines, these programs provide knowledge, promote self-management skills, and facilitate sustainable behavioral changes to improve diabetes outcomes.
Although DSMES is critical, engagement in these programs is poor and underutilized. 5 There are gaps in our knowledge of how Asian Americans use DSMES programs despite research that has previously examined factors such as programmatic, systemic, and individual characteristics as potential reasons for underengagement in DSMES.4,10,11 More specifically, many of the current studies lack diversity in participant samples, frequently omitting Asian Americans. There is also a lack of infrastructure describing DSMES availability and participation rates and the exclusion of Asian Americans’ voices when determining the factors that facilitate or hinder DSMES engagement.12-15 Many studies also focus on barriers and facilitators to self-management but not particularly on structured or formal DSMES programs. Therefore, the purpose of the study was to explore the determinants of DSMES program engagement among Asian Americans with T2DM.
Methods
Research Design
The Consolidated Criteria for Reporting Qualitative Research 16 reporting guideline was followed to report the study and results (see Supplemental Information 1). This research employed a qualitative descriptive design 17 to provide a detailed and comprehensive description of the facilitators and barriers to participating in DSMES programs and capture a rich and straightforward account of participants’ experiences. The interviews were in-depth, semistructured, and virtually conducted. This research was approved by the University of California, Los Angeles Institutional Review Board (IRB), and all procedures followed were in accordance with the ethical standards of the IRB and the Helsinki Declaration of 1975, as revised in 2000.
Settings and Participants
The study was conducted with participants living in California. Through a combination of purposive and modified snowball sampling, we recruited adult Asian Americans (≥18 years old) diagnosed with T2DM who were available for one-on-one interviews and able to speak and understand English.
Procedures and Data Collection
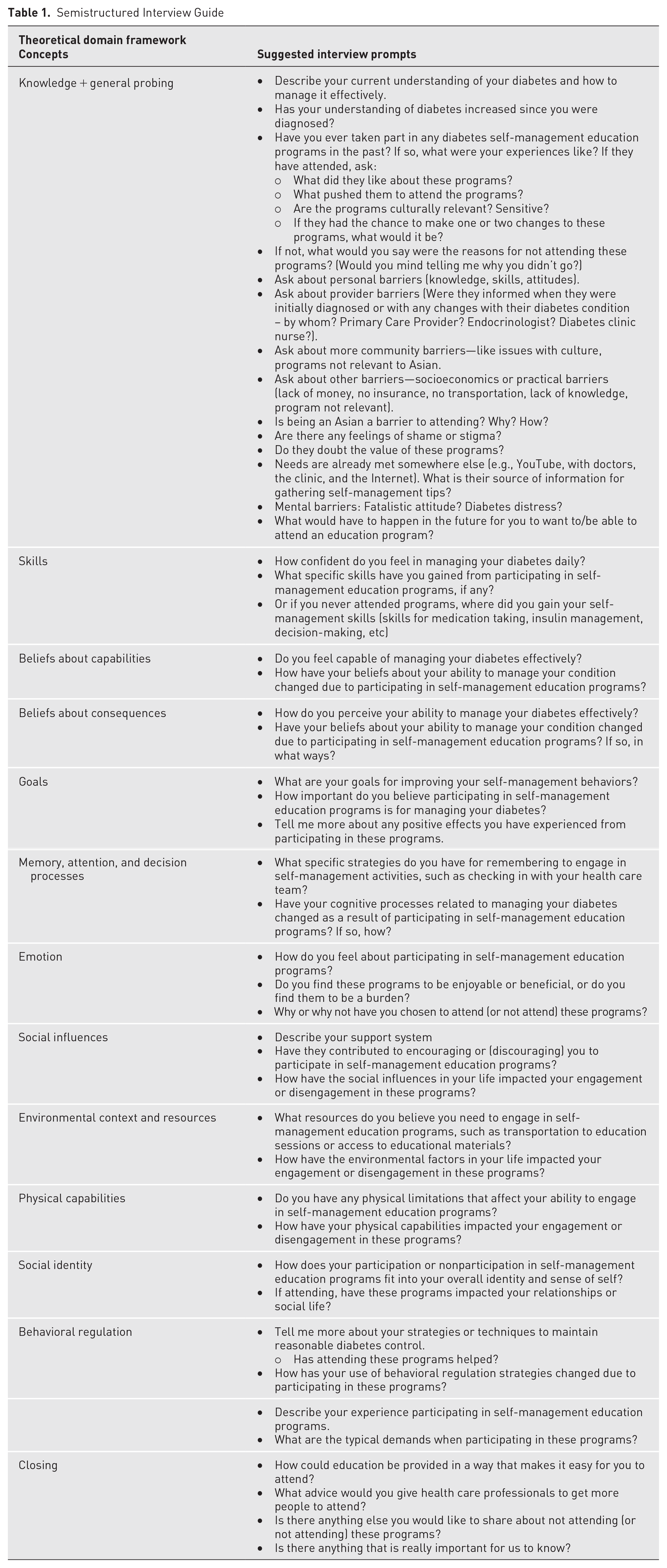
A study team member (RPERIII) initially developed the semistructured interview guide, which was informed by the theoretical domains framework (TDF), 18 and was revised through team discussion. By using the TDF, key constructs from multiple domains that might influence DSMES program engagement were integrated and considered, such as knowledge, beliefs about capabilities, environmental context, and social influence. A semistructured interview guide was used (see Table 1) to ensure consistency across interviews while allowing for open-ended discussions to elicit rich and descriptive narratives from the participants. Follow-up probes were also used to explore participant experiences in-depth, ensuring that the interviews remained flexible and participant driven. This enabled the identification of specific facilitators and barriers to DSMES participation.
Semistructured Interview Guide
Potential participants were directed to an online survey (Qualtrics, Provo, UT) to determine eligibility. Eligible participants were then asked to read the study information sheet and give their informed consent online. After acknowledging consent, they were prompted to complete a brief online demographic survey. They were then contacted via email to schedule their one-on-one interviews at a convenient time. Four trained study team members (DAT, SNL, RPERIII, MP) conducted virtual interviews with each participant following the semistructured interview guide. Interviews were conducted between March 2024 and August 2024. There were no repeat interviews with the same participants. The virtual interviews had an average duration of 60 minutes. Sampling saturation related to the description of the different facilitators and barriers to DSMES was reached after 10 interviews, aligning with the 9 to 17 participants often used in qualitative research. 19 An additional 2 interviews were conducted to confirm information power was sufficient. 20 Information power is a model used to evaluate the sufficiency of qualitative findings, particularly in interview-based studies. It considers factors such as the aim of the study, the specificity of the sample, the type of study, and the quality of the interviews. 21 Transcripts were not returned to participants for comment or correction. Participants received a $100 gift card as compensation for their time and participation.
Data Analysis and Trustworthiness of Data
All interviews were audio-recorded with the permission of participants, professionally transcribed, and then anonymized. Two random transcripts were verified for accuracy against audio recordings, and no corrections were made. In the first-cycle coding, 3 study members (DAT, PB, SNL) coded 3 interviews individually using open coding to derive the initial codes. 17 Codes were attached to data units of varying sizes that formed a straightforward descriptive label. This was done through careful reading and reflection on the data’s core content and meaning. A total of 517 codes emerged. The team then met to discuss the emergent codes and collectively developed a working codebook with definitions. The codebook was tested on 2 transcripts by the primary author (DAT), and it was revised as needed to enhance the credibility of data analysis. 22 Each analytical team member (DAT, PB, SNL) was then assigned multiple transcripts using the codebook to code all the interviews with regular feedback from the analysis team.
Second-cycle coding or pattern coding was then conducted to group the codes generated from first-cycle coding into categories, subthemes, and themes. This allowed us to condense large amounts of codes into a smaller number of categories and themes using thematic analysis. 23 The thematic analysis included familiarization of the data through first- and second-cycle coding and organization of these codes into overarching themes that captured the key aspects of participants’ experiences and perspectives with DSMES. Codes were collaboratively reviewed and categorized by the group, making changes as needed to ensure the credibility and confirmability of the data. 22 To further enhance the trustworthiness and clarity of the thematic analysis, aside from researcher triangulation of reviewing, defining, and naming themes, visual tools such as color coding, Sankey diagram, and force-directed graph were employed. These tools helped identify patterns; clarified relationships between codes, themes, and subthemes; and provided a structured and dynamic representation of the data.
Because the study focused on participants’ perspectives on DSMES through their narratives, participant observations were not conducted. Key insights, contextual factors, and emerging themes through notetaking were documented after each interview, ensuring a rigorous analytical process. Participants did not provide feedback on the findings, although credibility was strengthened through reflexive journaling, peer debriefing, and iterative data analysis. ATLAS.ti v24.2.1 for Mac was used to support coding and thematic data analysis.
Researchers’ reflexivity
Representation and inclusion in research teams enhance diversity and foster participant trust. All team members identify as Asian Americans, including the Filipino American lead author. A team of 4 researchers with nursing backgrounds conducted interviews: 1 PhD, 2 doctoral students, and 1 master’s student, all trained in qualitative methods and experienced in conducting interviews in health-related settings. The team, comprising both genders, built rapport during consent and prior to the interview to create a comfortable environment. Participants were informed of the study’s purpose, and reflexive awareness was maintained throughout the interviews to minimize biases. Field notes were taken to document contextual observations but were not formally analyzed.
Results
Participant Characteristics
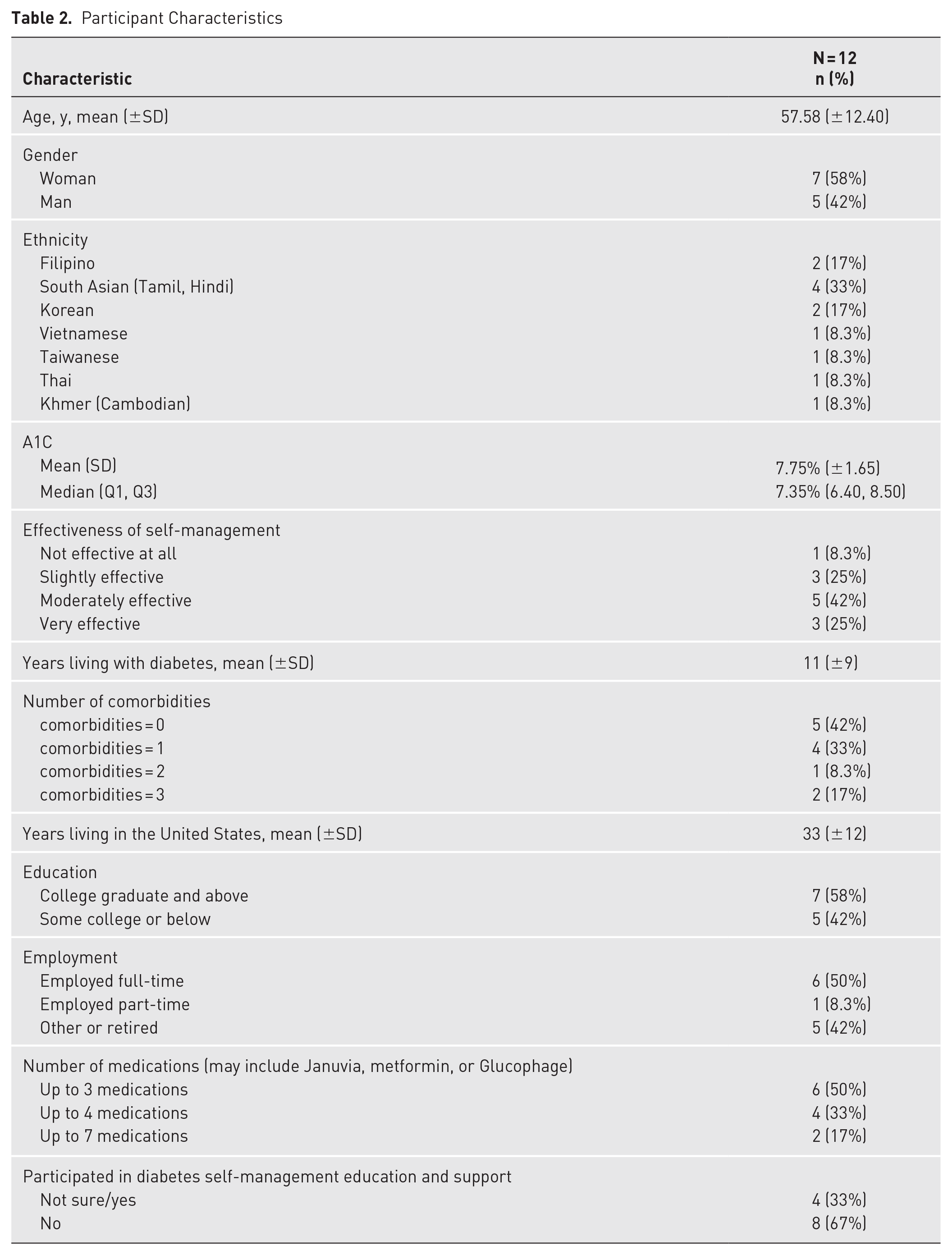
Thirty-nine individuals completed the initial survey; 12 were interviewed. The average age was 57.6 years (range 46-80), with 7 women and 5 men. Participants self-identified as Filipino (n = 2), South Asian (n = 4), Korean (n = 2), and others (Vietnamese, Taiwanese, Thai, Cambodian). The average A1C was 7.75%, with 41.7% of participants having controlled levels (<7.0%) and 58.3% uncontrolled (≥7.0%). Self-management ratings were 25% “very effective,” 41.7% “moderately effective,” 25% “slightly effective,” and 8.3% “not effective.” The average diabetes duration was 11.3 years, with 25% reporting hypertension as the most common comorbidity. Table 2 details additional demographics, including gender, education, and employment.
Participant Characteristics
Themes and Subthemes
Four overarching themes with multiple subthemes across the data were identified: (1) individual-level enablers and constraints, (2) cultural and social influences, (3) systemic and structural barriers, and (4) optimizing DSMES for inclusive diabetes care. Through this process, it became apparent that these themes could be meaningfully grouped using the concepts in Bronfenbrenner’s ecological framework. 24 However, this framework was not used as an initial guiding structure (see Figure 1).

Themes and subthemes describing and illustrating the conceptual factors contributing to diabetes self-management education and support program engagement. The inner ring represents broad thematic domains such as “microsystem,” “mesosystem,” “macrosystem,” and “exosystem,” corresponding to levels of influence. The outer ring further breaks down each domain into more specific factors. The size of each panel represents the proportion of occurrences for each code relative to the total number of codes applied. Copyicon was used to create the figure.
Participant quotes are presented with an identifier (e.g., P1) and gender (M for male, F for female) in parentheses; for example, “P1, M” indicates a quote from Interview 1 with a male participant. To protect participants’ identities and due to the relatively small sample size, additional demographic characteristics, such as age and ethnicity, were not included. Supplemental Information 2 gives an overview of the detailed qualitative results with additional representative quotes, which are described in the following.
Individual-Level Factors (Microsystem)
The microsystem level encompasses personal factors influencing individuals’ participation in DSMES, including intrinsic drivers, personal agency, lifestyle, and competing priorities. This theme reflects a complex interplay of lifestyle constraints, confidence in managing T2DM, and a belief that it is chronic yet controllable, leading to a carefree attitude and disengagement from DSMES programs. These internal dynamics, sometimes conflicting, shape how individuals perceive and respond to opportunities to engage in DSMES.
Intrinsic drivers and perceptions
This subtheme emphasizes the variability in how individuals engage with DSMES and self-management, ranging from conditional engagement to full disengagement to fear-driven responses. Conditional engagement refers to a pattern of participation where individuals engage in DSMES only under specific circumstances, such as worsening health, increased perceived risk, or immediate need. Some participants expressed feelings of detachment, disinterest, or lack of investment in DSMES programs or advice. One participant remarked, “Boy, there’s too much information. I don’t pay attention” (P9, M). Similarly, another said, “It was all discussing about exercise, food intakes, and then diet. I said, ‘Ah,’ ‘Eh’” (P3, M). Fear of family history and fear of potential complications also influenced participants’ conditional engagement with DSMES and diabetes management. For example, one participant reflected, Before, I wasn’t very careful about it. I mean, I feel like I’m not careful enough yet. Since my mom has diabetes, my dad is in prediabetic stage, I think, but she’s been having diabetes for a long time, and now she’s in her late 70s and having a lot of complication, I guess. That just made me look at it a little bit differently now. I’m trying to walk out more. (P5, F)
Many participants expressed fear of complications, saying, “the things that I won’t be able to do like I don’t want to be on dialysis” (P1, F), “I’m scared. I might die because of complication on diabetes” (P3 FA), and “It’s also knowing that with diabetes, the problems you can have with neuropathy and your kidneys and your eyesight and so many things” (P7, M). Although these fears motivated some individuals to take action, they often did not translate into proactive behaviors. Instead, many participants described conditional engagement, stating that they would prioritize self-management or follow medical advice if signs of complications became more immediate or severe. As one participant explained: Probably if my blood A1C go up again, that’s the time I might be thinking to follow the doctor’s advice. Been telling me to exercise, walk every day, but I hope it will keep that way if my A1C’s down. That’s the only thing gonna make me worried if my A1C go up again. (P3, M)
The emotional and behavioral variability in DSMES engagement reflects how individuals choose to participate—or not—based on their internal attitudes, perceptions of urgency, and motivational triggers.
Personal agency in diabetes management
This subtheme of personal agency refers to participants’ autonomy and initiative in managing their diabetes and overcoming DSMES barriers through independent learning, improvisation, and resourcefulness. Participants demonstrated personal agency and adaptability by setting goals, educating themselves, and implementing self-management strategies independently, even if they had not attended formal or structured DSMES programs. For example, one participant, who transitioned to a new physician after living with T2DM for several years and had never attended a formal program, shared: I mean, even this doctor, the new one, which was like one year, he said, I did speak to a dietician, but, you know, like I told you, by then I had read up so much. I had so much information myself, uh, you know, that like really, I mean, I know all the right things. (P11, F)
Personal motivation was rooted in the desire to achieve better health and well-being, with many participants recognizing the value of education, whether structured or self-directed. One participant expressed, “I think education about how generally we can prevent those things, so you don’t have to be fearful” (P2, M). Another shared, “I’m doing this on my own. I just read what I suppose to do. With the people who has the diabetes and high blood pressure and cholesterol” (P8, F). Similarly, another participant stated, “We did our own research” (P7, M). These reflections demonstrate participants’ determination to maintain control over their condition and strive for better outcomes. Their willingness to seek diabetes-related knowledge, even beyond structured DSMES programs, reflects their resourcefulness and proactive attitude toward self-management.
Lifestyle demands and competing priorities
Although many participants felt they already possessed the knowledge to manage T2DM, lifestyle demands and competing priorities—such as work, stress, and caregiving responsibilities—often led to the deprioritization of attending DSMES. This was especially true when DSMES programs were perceived as irrelevant, overly general, or lacking practical impact on their condition. One participant shared, “I was too busy with school, so I missed the appointment” (P4, F), and another reflected on the challenges of balancing life responsibilities: I don’t know what the average age where people initially [get diagnosed]; I would think probably it’s 30-40 years old more common; that’s the stage where most people are really busy at life. You usually have your kids you need to take care of, your work, you may have your parents you need to take care of. (P2, M)
Participants also noted the importance of personalization in DSMES programs. One participant remarked, “I feel like not everything is geared towards me and my situation” (P1, F), and another emphasized, “I think it would be more effective . . . ideally if it is personalized, it’s better” (P6, F). This duality underscores a tension between participants’ perceived self-sufficiency in managing their condition and the unmet need for tailored, personalized support that aligns with their unique circumstances and priorities.
Cultural and Social Influences (Mesosystem)
This theme captures the cultural and interpersonal factors that shape DSMES engagement, highlighting both potential motivators and barriers rooted in societal, familial, and cultural norms and relationships.
Cultural norms and perceptions
Cultural norms and perceptions encompass both the stigma surrounding diabetes and preferences for culturally tailored DSMES or support systems, including the use of online resources. Participants described experiencing stigma through negative perceptions and judgments from others about having diabetes, which led to feelings of shame and reluctance to disclose their condition. This often decreased their engagement in DSMES programs. As one participant shared, “My diabetes is secret to everyone—everyone else. I don’t know. It’s just like—I feel like I don’t wanna be judged” (P1, F). Another expressed: It’s not something I should feel ashamed about things that people say, and now I’m okay, but at the same time, I was a little bit ashamed of having diabetes. Which is type 2. I’m overweight. I don’t really have this control about myself. All those things. It was not something that I would like to talk about with others. (P5, F)
Additionally, many participants noted that diabetes education programs lacked cultural tailoring, particularly in dietary guidance and cultural congruence. One participant explained their reluctance to attend: They say about setting up with a nutritionist and everything. I was like, “It’s okay. Nah. It’s okay.” I did it, but at the same time, the reason that I did it was more about the food that I ate. I eat more Korean food. I felt like the nutritionists wouldn’t really know about Korean food. I just didn’t really bother to go. (P5, F)
Another participant said: I have a new one, but back then it was this doctor that I have. They give you that look like, “Are you doing the way I tell you to?” Basically, they call you lying, but I have to admit when I’ve looked back, oh, the way I eat is very bad, but this is—if you know my background, you have to understand what I’ve been through to understand my eating habit. When I was in [my native country], I had no childhood. We were starving ’cause there’s no food during the communist regime. (P12, F)
As a result, participants often turned to online and social media platforms for culturally relevant education. They described searching for resources that better aligned with their needs, stating, “I searched things online” (P1, F); “Yeah, through Google search. A lot of times it comes from WebMD, sites that are medical” (P2, M); and “Okay, send me the TikTok and Reels. Those are the good things I think” (P8, F).
Many participants expressed that social media is emerging as a valuable resource for diabetes information, providing more personalized and culturally relevant content compared to the generic advice typically offered by health care providers and DSMES programs. These platforms allow individuals to access information that resonates with their cultural preferences and lived experiences, bridging gaps left by traditional DSMES programs.
Family and community support as informal proxies for DSMES
In addition to accessing information online, family and community support serve as informal sources of diabetes information, acting as substitutes for structured DSMES programs. Many participants described how family members provided essential information that influenced health behaviors and decision-making. One participant shared, “I have to change my diet. My wife helped me search. She searched all the what to eat” (P7, M). Similarly, friends, acquaintances, or peers with diabetes offered valuable insights, shared experiences, and emotional support, shaping participants’ approaches to managing their condition. When asked where they received their education without attending DSMES, one participant explained, “Basically from a group of friends, including the co-worker before. Then I tried friends on the other side of the [country] communities” (P8, F). This reliance on social networks highlights an alternative and accessible source of education for individuals who may not engage in formal DSMES programs, reflecting the significant role of interpersonal relationships as informal proxies to DSMES.
Structural Factors (Exosystem)
These barriers reflect the structural factors that impact Asian Americans’ engagement with diabetes self-management programs. Collectively, they illustrate accessibility issues such as information gaps about DSMES, limited access to traditional programs, and the high cost of health care that hinders their participation in DSMES.
Accessibility barriers
This subtheme captures a range of barriers that hinder individuals from engaging with DSMES programs, including information gaps, limited accessibility of traditional DSMES, and perceptions of DSMES irrelevance. Notably, a majority of participants (82%) reported being unaware of DSMES programs. Participants frequently expressed that DSMES was not discussed with them by health care providers. When asked if DSMES was mentioned during their initial visit with a primary care provider, one participant stated, “He didn’t offer it to me” (P1, F), and another remarked, “Never mentioned. I don’t think so” (P4, F).
Limited accessibility was a significant barrier to sustaining participation for those who had the opportunity to attend DSMES. Many highlighted constraints related to the availability, scheduling, or delivery formats of face-to-face DSMES programs. These barriers also led participants to suggest ways to optimize DSMES, which are further explored at the macrosystem level (see Theme 4).
Participants were further disengaged from DSMES due to perceptions that the content lacked relevance, specificity, or practical value. Many emphasize the importance of ensuring that DSMES content is aligned with their personal needs. One participant explained, “If it’s something beyond what I already know, such as exercise or regular meal. If it provides more than that, I think I would definitely be willing to take those classes” (P4, F). Another shared, “I feel like not everything is geared towards me and my situation” (P1, F), and another added, “The other thing is I need to feel comfortable that the knowledge base is good, also personalized to my need” (P2, M). These findings highlight the importance of improving communication, accessibility, and personalization in DSMES programs to address barriers preventing engagement in DSMES.
Financial barriers to DSMES participation
This subtheme highlights the prohibitive cost of health care as a significant deterrent to DSMES participation. It reflects the inadequate dissemination of DSMES information and the failure of the US health care systems to promote and provide affordable access to these programs effectively. Participants emphasized barriers to traditional face-to-face DSMES and advocated for more accessible and financially feasible education programs and the integration of cost-effective technologies, such as continuous glucose monitors (CGMs). Financial challenges were frequently discussed, with participants sharing concerns about affordability: “I searched for classes, and I asked if there was any copayment.” (P1, F) “I think the broader issue is the cost in the US. Whether those programs are affordable for most people is also important.” (P2, M)
Many of the participants also noted that although CGMs were helpful decision-making tools for managing their diabetes, the high cost often limited their sustained use. One participant explained: My insurance company stopped my glucose meter [CGM], uh, paying payment, you know, I mean, and then it jumped to 200 bucks or something, which I could not—I didn’t want to pay for that. I couldn’t afford that, so then I stopped the glucose meter. (P11, F)
These findings reflect the need for more affordable and accessible DSMES programs and technologies to support diabetes self-management in a financially sustainable way.
Optimizing DSMES for Inclusive Diabetes Care (Macrosystem)
This theme highlights participants’ vision for more optimal DSMES programs, emphasizing systemic-level improvements with changes in program accessibility, informational needs, and the need for health care provider alignment.
Program accessibility
This subtheme captures participants’ logistical and practical preferences for DSMES programs that align with their lifestyles, work schedules, and accessibility needs. Accessibility was a major barrier to engaging in DSMES, with participants emphasizing the importance of convenience, proximity, and flexible delivery formats. One participant explained, “If it’s relatively close either to where I work or where I live, then I think yeah, I’d definitely participate” (P2, M). Participants also highlighted the need for shorter sessions that could fit into their schedules without disrupting their daily lives. One participant shared, “I think 30 minutes to an hour per session is pretty good” (P5, F). Online format was another key preference, with participants valuing the flexibility and convenience it offered. As one participant noted, “Oh, I mean, if it would be virtual, that would be—that would so much. I could attend in the convenience of my home” (P1, F). Another added, “I would prefer a Zoom class” (P4, F). Participants also stressed the importance of incorporating visual aids in DSMES programs to enhance engagement and comprehension.
Tailored and actionable program content
This reflects the participants’ desire for DSMES programs to provide specific, actionable, and relevant content that aligns with their individual health and lifestyle needs. Many participants expressed the importance of receiving scientifically grounded information to help manage their condition effectively. One participant shared, “I wanted something more of a scientific base and something that would stimulate me” (P1, F). Participants also highlighted the need for practical, real-world guidance tailored to their daily lives. For example, one participant said, “I want to hear about, you know, a lot of stuff that I cannot find. Uh, you know, what this thing—like a burrito, you know? Know how many—you don’t know there’s no label on it” (P9, M). The value of DSMES was emphasized by participants who believed tailored and actionable content could significantly improve their self-management efforts. One participant explained, “If it’s gonna provide a lot of information about diabetes on how to manage it, and if it’s something beyond what I already know . . . Like me who are a little paranoid of their health and are very interested in this program” (P4, F). However, not all participants found DSMES programs useful. As one participant stated bluntly, “Not useful at all” (P8, F). These varied perspectives highlight the need for DSMES programs to focus on delivering individualized, practical, and engaging content to better meet the diverse needs of Asian Americans.
The role of health care providers in DSMES participation
This refers to the pivotal role health care providers play in fostering trust and providing structured guidance to encourage participation in DSMES programs. Many participants emphasized the need for providers to inform their patients about DSMES because a lack of awareness or information gap was a common barrier. One participant shared, “Doctors, if they tell the patients when they come into the office, I think that’s the most effective way” (P6, F). Participants also stressed the importance of cultural sensitivity and knowledge among DSMES instructors. For some, cultural concordance between the instructor and participant was seen as vital. As one participant explained, “Generally, I think it would be good if Indians were talking to Indians. I think it would be good” (P7, M). Similarly, another shared their hesitation with a nutritionist, stating, “They say about setting up with a nutritionist and everything. I was like, ‘It’s okay. Nah.” . . . I eat more Korean food. I felt like the nutritionists wouldn’t really know about Korean food. I just didn’t really bother to go” (P5, F). Another participant said, “I don’t care what people say to me or what doctor tell me to do. If it work for me, I’m just gonna keep doing it” (P12, F). For some participants, language was less of a concern compared to cultural understanding. One participant noted, “Actually, the language, I’m not worried too much as the understanding my culture and Asian . . . some of them, they don’t understand our culture” (P8, F). It is important that health care providers not only promote DSMES but also ensure that instructors are culturally sensitive and knowledgeable, which can enhance trust, engagement, and relevance for Asian Americans.
Discussion
This study identified and provided insights on key facilitators and barriers to DSMES program engagement among Asian Americans, a population with specific sociocultural and systemic challenges with T2DM management. 25 Structured using an ecological framework, the findings of the study highlighted the interplay of individual and interpersonal factors with broader cultural, social, and systemic factors in DSMES engagement. As with other prior research exploring patient-, provider-, and program-related factors influencing DSMES participation, key barriers and facilitators included logistical factors (time, transportation, scheduling), lack of perceived benefit or information, low prioritization of DSMES, financial factors, a knowledge or information gap, and cultural, emotional, and linguistic factors.4,11,26-28 This study provides a deeper exploration of these factors, particularly in the context of Asian American experiences.
At the microsystem level, personal agency and intrinsic motivation emerged as key determinants of engagement. Participants demonstrated self-directed learning of self-management by independently seeking self-management information, setting goals, and implementing self-care strategies. Personal agency and self-directed learning in diabetes management were apparent among the participants even without formal DSMES program participation. Additional individual-level barriers that limited participation included competing priorities, fear of complications, and a perceived lack of personalized relevance in existing programs. These findings are consistent with previous research indicating that lifestyle constraints significantly impact chronic disease self-management behavior, including fear of complications, which is a strong predictor of behavior change.13,29,30 Although participants demonstrated a proactive approach to self-management, the challenge often lies in translating that knowledge into actionable steps given that individuals frequently encounter barriers such as limited health literacy, competing responsibilities, and inadequate support systems. 31
Societal factors such as cultural stigma and a preference for culturally tailored information, often obtained through online resources and informal networks, played a significant role in DSMES disengagement. Participants highlighted the role of stigma and shame tied to diabetes, which diminished their willingness to engage in structured DSMES programs, a phenomenon less explored in other populations. Culturally, many Asian Americans tend to seek medical care only when symptoms become severe. 32 The stigma associated with diabetes compounded by competing priorities and perceptions of DSMES as lacking personal relevance likely limited participants’ engagement in DSMES programs. Many participants reported reluctance to disclose their diabetes status due to fear of judgment or shame, underscoring the influence of societal perceptions on their willingness to seek formal support and interventions. A study on Korean Americans with T2DM explicitly highlighted that seeking support is viewed negatively and that individuals may avoid disclosing their concerns. 33 This reluctance to disclose stems from a desire to avoid “losing face,” worrying others, disrupting harmony, and receiving criticism. However, the study 33 found that disclosure of diabetes was the strongest predictor of receiving spousal support. This suggests that although cultural norms may discourage open communication about health concerns, doing so is crucial for obtaining support.
The preference for culturally tailored dietary and educational guidance emerged as a critical need, with many participants turning to online resources and community networks to address gaps left by traditional programs, emphasizing the importance of culturally congruent approaches in improving engagement. The absence of culturally relevant guidance in DSMES programs led participants to seek alternative sources, such as social media and community networks, which they found more relatable to their lived experiences. This reliance on informal networks—often nonevidence-based resources—underscores the need for DSMES programs to incorporate cultural sensitivity and personalized content to better address the unique needs of the Asian American community. The study also highlights how family and community support act as informal proxies for DSMES. This supports previous findings that family is a facilitator of self-care.26,34,35 This is an important finding because it may suggest that among Asian Americans, support networks play a critical role in diabetes management.
Structurally, health care providers contributed to the lack of participation in DSMES among our participants. A substantial proportion of participants were unaware of DSMES programs and frequently reported that their health care providers failed to initiate discussions about DSMES. This is consistent with prior research, with the lack of referrals from providers as a key barrier. 11 This issue often depends on the type of care setting given that many Asian immigrants seek care from private practice providers in their ethnic enclaves, who may lack awareness of DSMES programs or access to the necessary resources to refer patients. Our findings underscore not only the importance of provider awareness but also cultural sensitivity in fostering engagement with DSMES. A study done by Koh and Park 36 identified that prior negative experiences of Asian Americans with health care providers contribute to feelings of marginalization and distrust of the health care system.
Furthermore, participants in this study emphasized that a lack of cultural understanding from providers often diminished the perceived relevance of DSMES, making it less likely for individuals to participate. Feelings of mistrust, lack of provider initiation, and an overall negative experience unfortunately amplify the barriers mentioned for commencing DSMES programs. Research indicates that culturally incongruent care can lead to feelings of being misunderstood or overlooked, further discouraging engagement with these structured health programs. 37 Tailoring provider communication to reflect cultural sensitivity and actively promoting DSMES can help mitigate these barriers, fostering a stronger patient-provider relationship and improving participation rates.
The perception of in-person DSMES formats as the only option for DSMES coupled with cultural gaps and cost posed challenges for DSMES participation. The participants emphasized the need for shorter sessions, flexible delivery formats, and online options to encourage DSMES participation. The COVID-19 pandemic significantly accelerated the adoption of telehealth, enabling digital health care delivery, and many participants expressed openness to the online delivery of DSMES. The Centers for Disease Control and Prevention 38 underscores the effectiveness of telehealth in providing DSMES through virtual platforms, such as videoconferencing. As anticipated, cultural influences played an important factor in facilitating DSMES engagement among Asian Americans. Participants emphasized the importance of culturally tailored education and the availability of online resources that align with their personal preferences and lived experiences.
Participants strongly emphasized using technology, including CGMs, online resources, and social media, for education and support in diabetes management. Although prior studies have talked about technology and media in diabetes management,4,11 social media is increasingly beginning to be a source of education. The increasing reliance on social media is not surprising given that many participants highlighted their desires for personalized DSMES content, which includes a preference for actionable, specific, and relevant information tailored to their individual health and lifestyle needs. DSMES programs must begin leveraging social media platforms to develop and deliver short, culturally tailored, evidence-based content that resonates with the community’s preferences and behaviors, ensuring greater accessibility and engagement.
This study provides rich qualitative insights into Asian American experiences framed in an ecological model but has limitations. Despite efforts to diversify recruitment, some Asian American subgroups and individuals with varying educational backgrounds and resources were underrepresented, limiting transferability. The focus on English-speaking participants excluded non-English speakers, and many participants lacked prior DSMES program experience, restricting insights into program quality and engagement. Broader subgroup perspectives could reveal additional facilitators and barriers to DSMES participation.
Future Directions
Increasing DSMES program utilization among Asian Americans requires a multilevel approach, prioritizing culturally specific and personalized self-management strategies. As indicated by prior research, culturally tailored programs have been found to be a priority for Asian Americans. 25 This study further underscores the value of incorporating social media education, personalized tools such as CGMs, and familial support. Strategies include enhancing accessibility through health care providers, virtual sessions, and targeted social media outreach. Initiatives like Diabetes@Work, a culturally tailored, self-paced platform, exemplify efforts to make diabetes education accessible and understandable for Asian Americans. 39 By addressing participants’ preferences for accessibility, such programs can effectively bridge gaps in diabetes education.
Additionally, DSMES programs should involve family members and educate participants on using evidence-based and credible online resources to support their diabetes management needs. Future research should explore the long-term impact of integrating culturally tailored DSMES with virtual programs or social-media-based education platforms. Evaluating the effectiveness of culturally tailored programs for different Asian American subgroups will provide further insights into improving diabetes self-management across diverse populations.
Conclusion
This study employed a systems-level approach to identify key barriers and facilitators in DSMES engagement in Asian Americans. It allowed us to examine factors across microsystem to macrosystem levels, providing a holistic understanding of the individual, contextual, and structural influences that shape DSMES engagement. Building and rebuilding trust through culturally sensitive approaches, including proactive engagement, is important to ensure that Asian Americans avail of DSMES programs. Health care providers should prioritize promoting DSMES during patient visits and ensure that programs are accessible, culturally sensitive, and tailored to individual needs. There is a need to move to a new paradigm of having DSMES that is limited to only a brick-and-mortar format. Collaborating with community organizations to share accurate, culturally tailored diabetes information through different modalities, such as social media, is needed.
Supplemental Material
sj-docx-1-tde-10.1177_26350106251337487 – Supplemental material for Navigating Type 2 Diabetes Care: Asian American Perspectives on Self-Management Education and Support
Supplemental material, sj-docx-1-tde-10.1177_26350106251337487 for Navigating Type 2 Diabetes Care: Asian American Perspectives on Self-Management Education and Support by Dante Anthony Tolentino, Paul Boy, Sorina Neang Long, Rey Paolo Ernesto Roca, Matthew Peña, Gillkaitlyn Mary Gaw Palao, Gilkevyn Joseph Gaw Palao, Marjorie Rose Uy De Ong Luzuriaga and Sarah E. Choi in The Science of Diabetes Self-Management and Care
Footnotes
Acknowledgements
Dr Tolentino reports support from the NIH/NIMHD No. P50-MD017366 UC END-DISPARITIES Pilot Award, NIH National Center for Advancing Translational Science: UCLA CTSI UL1TR001881. We express our sincere gratitude to all participants and community partners who generously shared their time and experiences during the interviews for this study. We also thank Drs Manpreet Sidhu and Barbara Roces for their invaluable assistance in recruiting participants for this study.
Author Contributions
Conceptualization: [Dante Anthony Tolentino]; Methodology: [Dante Anthony Tolentino, Paul Boy, Sorina Neang Long, Rey Paolo Ernesto Roca III, Matthew Peña, Gillkaitlyn Mary Gaw Palao, Gilkevyn Joseph Gaw Palao, Marjorie Rose Uy De Ong Luzuriaga and Sarah E. Choi]; Formal analysis and investigation: [Dante Anthony Tolentino, Paul Boy, Sorina Neang Long]; Writing - original draft preparation: [Dante Anthony Tolentino, Paul Boy, Sorina Neang Long]; Writing - review and editing: [Dante Anthony Tolentino, Paul Boy, Sorina Neang Long, Rey Paolo Ernesto Roca III, Matthew Peña, Gillkaitlyn Mary Gaw Palao, Gilkevyn Joseph Gaw Palao, Marjorie Rose Uy De Ong Luzuriaga and Sarah E. Choi]; Funding acquisition: [Dante Anthony Tolentino, Sarah E. Choi]. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors have no relevant financial or nonfinancial interests to disclose.
Funding
Dr Tolentino reports support from the NIH/NIMHD No. P50-MD017366 UC END-DISPARITIES Pilot Award, NIH National Center for Advancing Translational Science: UCLA CTSI UL1TR001881.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the University of California, Los Angeles (IRB No. 23-0072).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
N/A.
Data Availability Statement
The data supporting the findings of this study are not publicly available due to privacy and confidentiality restrictions. However, they may be made available from the corresponding author on reasonable request and with appropriate permissions, where applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.