
Abstract
Purpose:
The purpose of this study was to describe the information needs and examine its association with depressive symptoms in people with type 2 diabetes (T2D).
Methods:
A descriptive, correlational design was used. People with T2D (N = 358) were recruited from 12 communities in Shanghai, China. Self-reported information needs and depressive symptoms were measured using the Information Needs in Diabetes Questionnaire and Patient Health Questionnaire-9 (PHQ-9), respectively. Multivariate linear regression analysis was performed.
Results:
The participants were 64.8 years on average, and 46.6% were men. One hundred fifty-one (42.2%) had depressive symptoms (PHQ-9 ≥ 5). Participants had the least knowledge about “diabetes research,” “acute complications,” and “lifestyle adjustment.” The sample had the highest levels of information needs about topics including “mental strain,” “treatment/therapy,” and “diabetes in everyday life.” Compared to those without depressive symptoms, those experiencing depressive symptoms were less informed and had higher levels of need for further information. Controlling for covariates, higher levels of need for further information were significantly associated with greater depressive symptoms (B = 0.368, 95% CI, 0.155-0.582, P = .001).
Conclusions:
This study demonstrated areas that should be prioritized when meeting patients’ information needs. It also showed the potential negative effect of unmet information needs on depression. These findings may help develop a more tailored intervention for people with T2D.
Introduction
Worldwide, 1 in 10 adults had diabetes in 2021, and the proportion of people with type 2 diabetes (T2D) is increasing, 1 contributing to increased mortality and disability. 2 Depression is common in people with T2D and is twice as common as in the general population. 3 The pooled prevalence of depressive symptoms in people with T2D was 28% across the world. 4 Depressive symptoms have been linked to an increased risk for cardiovascular diseases and incident macro- and microvascular diseases in T2D.5,6 Reducing depression may reduce A1C, an indicator of overall diabetes control. 7 Thus, effective management of depression is critical.
Depression in T2D could be due to demographic and clinical factors (eg, age, gender, body mass index, and glucose level). 8 Information needs, defined as a recognition that knowledge is inadequate to meet one’s goal at a specific time point under a certain circumstance, 9 may also be associated with depressive symptoms in people with T2D. Based on previous studies, cancer patients who had more needs for further information experienced higher levels of depression 10 and psychological strain. 11 Similarly, access to health information was associated with quality of life, and this association was mediated by depression. 12 Cancer survivors who did not receive adequate support for health information from medical staff tended to have a lower sense of personal and treatment control and increased helplessness, 13 which were found to be related to depressive symptoms.14,15 In addition, caregivers of cancer survivors with higher levels of unmet information needs were more likely to experience depression. 16
The management of T2D requires lifelong diabetes self-management tasks, including healthy eating, regular exercise, self-monitoring, and effective coping. Effective self-management requires making daily complex decisions that can be influenced by the level of information about diabetes patients have acquired.17,18 There is early evidence that people with diabetes had higher levels of information needs (eg, information about acute and late complications, course of diabetes, and mental strain) than people with cancer or endocrine, cardiovascular, or respiratory diseases, but there was no indication regarding which information needs should be prioritized.19,20 Additionally, there has been little research about the relationship between unmet information needs and depressive symptoms, creating a large gap in the current literature. Thus, the aim of this study was to describe the diabetes-related information needs and examine their association with depressive symptoms among people with T2D. This study may add to current knowledge about the areas that need to be prioritized when designing health education programs to meet patients’ information needs. It may also provide evidence for interventions designed to alleviate depressive symptoms among people with T2D.
Hypothesis
The hypothesis was that in people with T2D, being less informed and having more unmet information needs were associated with higher levels of depressive symptoms while controlling for potential confounders (eg, age and sex).8,21
Methods
Design
This cross-sectional study was approved by the Institutional Review Board of Shanghai Jiao Tong University School of Medicine (No. SJUPN-201811). A correlational design was used. This study was reported following the STROBE checklist. 22
Sample
The sample was recruited from 12 communities in Shanghai, China, using convenience sampling. The inclusion criteria included a self-reported diagnosis of T2D and age between 18 and 85 years. The exclusion criteria included being pregnant, doing shift work during the past 6 months, or having severe comorbidities, including heart failure, kidney failure, or cancer. Shift workers were excluded because shift work can influence both mental health (eg, depression) and diabetes management.23,24 Assuming a small effect size (0.02) and setting α = 0.05, 1 – β = 0.8, the number of predictors = 5, an a priori sample size of 311 was determined. A total of 436 participants were screened, among which 35 were not eligible due to age, 22 due to night shift jobs, and 10 due to severe comorbidities. A total of 369 participants were enrolled. Among them, 11 had a significant amount of missing data on key variables of interest (eg, depressive symptoms) and thus were excluded. Thus, the final sample size was 358.
Procedures
Participants were recruited during free annual nursing health checks (eg, blood glucose and blood pressure monitoring) held at 12 communities in Shanghai between May and June 2021. The checks were part of the volunteer work organized by the Shanghai Nursing Association-Diabetes Care Sub-Committee. Participants were screened by nurses using a checklist during their visits. Verbal consent was obtained from all participants prior to data collection. Data were collected using paper-and-pencil questionnaires. The participants were instructed to complete the questionnaires on their own, which took approximately 10 to 15 minutes to complete. Trained nurses were present to provide assistance and answer any questions the participants encountered.
Measures
The following instruments were used to measure the demographics and clinical characteristics of the participants, information needs, and depressive symptoms.
Baseline questionnaire
A questionnaire was developed to measure demographic and clinical characteristics. Key variables included age, gender, marital status, employment status, self-reported height and weight, diabetes duration, treatment regimen, current smoker, drinking (current), and hypertension. Body mass index (BMI) was calculated from weight and height.
Information Needs in Diabetes Questionnaire
Information needs were measured by items from the Information Needs in Diabetes Questionnaire (INDQ). 19 The INDQ was developed by Chernyak and colleagues from Germany in 2016. The INDQ consists of 3 questions in total. The first one asks the participants to choose 3 topics that they would like to have further information about from a list of topics. They were then asked to write down what particular interests they have in these topics. The second question asks participants to specify how well informed they are on 11 topics using a 4-point Likert scale (1 = not informed at all, 4 = very well informed) and then determine if they need further information on each of these topics (yes/no). The 11 topics include causes of diabetes; course of the disease; treatment/therapy; acute complications; late complications; diabetes in everyday life; mental strain; lifestyle adjustment: health promotion and prevention; support, helplines, and information sources; social and legal aspects; and diabetes research. The third is an open-ended question: “What do you consider to be particularly important with regard to information on diabetes?” In this study, only items from the second question were used. They were translated into Chinese by a bilingual researcher proficient in both English and Chinese. The translated items were reviewed by the research team. Given the cultural difference, the 10th item, “social and legal aspects,” was not applicable. Thus, only 10 topics were included in this study. When assessing “how well informed,” the original rating was used. When assessing “need for further information,” the original “yes/no” response was changed to a 0 to 10 visual analog to evaluate the degree to which further information was needed (0 = no need at all, 10 = very much need). A composite score for how well informed and need for further information was calculated separately by averaging the 10 items for each. Higher scores indicate more informed or higher levels of needs for further information. The original questionnaire has been used in previous studies and showed excellent internal consistency.25,26 In this study, the international consistency of INDQ was excellent (Cronbach’s α was 0.94 for the how well informed question and 0.98 for the need for further information question).
Patient Health Questionnaire-9
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9). 27 The PHQ-9 is a self-report questionnaire to evaluate the frequency of depressive symptoms over the past 2 weeks. It was derived from the DSM diagnostic criteria for depression and consists of 9 items. Each item is scored on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Adding all the items results in a total score between 0 and 27. Higher scores indicate higher levels of depressive symptoms. Interpretations of the score are: 0 to 4 (no depression), 5 to 9 (mild), 10 to 14 (moderate), 15 to 19 (moderately severe), and 20 and over (severe). The PHQ-9 has been translated into Chinese and validated in Chinese populations. In this study, the PHQ-9 demonstrated good internal consistency (Cronbach’s α = 0.89). In this study, participants were divided into 2 groups based on their PHQ-9 score: T2D only (PHQ-9 < 5) and T2D with depressive symptoms (PHQ-9 ≧ 5).
Data Analysis
Statistical analyses were performed using SPSS version 26.0 (IBM, Armonk, NY, USA). Missing data, normal distribution, and outliers were checked prior to data analysis. Mean substitution was used when missing data was less than 5%. Data were presented as mean (SD) or frequency (%). Independent sample t test and chi-square test were performed to examine the group differences for continuous and categorical variables, respectively. Bivariate associations between 2 continuous variables were examined by Pearson correlation analyses. Multivariate linear regression analysis was performed with the severity of depressive symptoms (PHQ-9 scores) as the dependent variable. The model was examined for collinearity, normal distribution, and heteroscedasticity of the residuals. Covariates (ie, age, sex, and diabetes duration) were determined based on current literature and the bivariate results (P < .2).8,28,29 Statistical significance was set at P < .05 (2-tailed).
Results
Demographics and Clinical Characteristics of the Sample
The participants were 64.8 years (SD 10.2), and 46.6% were males. BMI was 23.9 kg/m2 (SD 3.0), and diabetes duration was 10.6 years (SD 8.9), respectively. Their random glucose was 9.3 (SD 3.2) mmol/L, on average. The mean PHQ score was 4.8 (SD 5.3), and 151 (42.2%) had depressive symptoms (PHQ ≧ 5). See Table 1.
Demographics and Clinical Characteristics of the Sample

Abbreviations: BMI, body mass index; PHQ-9, Patient Health Questionnaire-9.
n = 350.
n = 300.
n = 304.
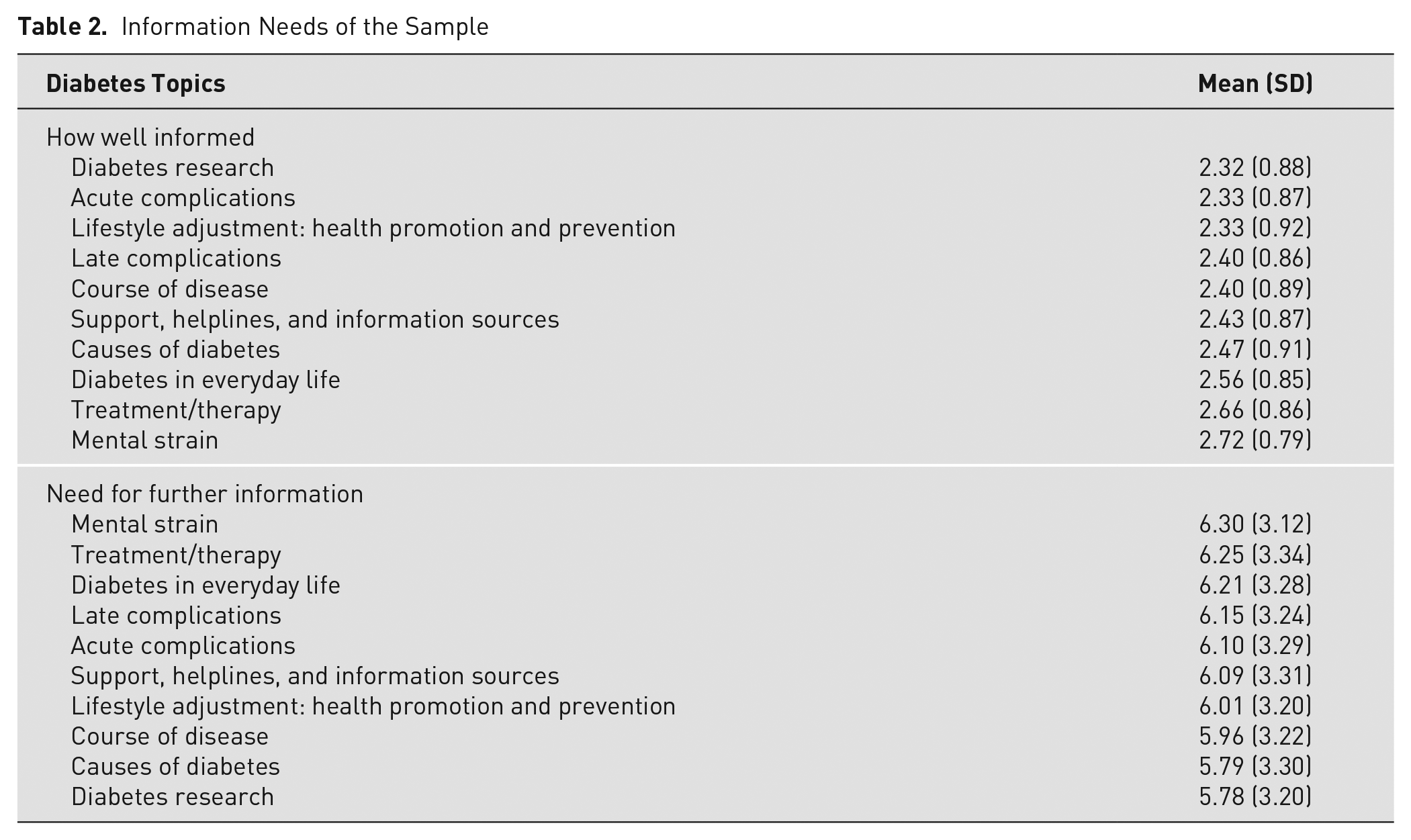
Information Needs of the Sample
Participants were least informed about diabetes research, acute complications, and lifestyle adjustment, and they had the highest levels of information needs on the topics of mental strain, treatment/therapy, and diabetes in everyday life. See Table 2.
Information Needs of the Sample
Bivariate Associations Between Demographics and Clinical Characteristics with Depressive Symptoms
Compared to those without depressive symptoms, those with depressive symptoms had significantly longer diabetes duration, were less informed, and had higher levels of needs for further information (P < .01). See Table 3.
Comparison of Demographics and Clinical Characteristics in Participants With and Without Depressive Symptoms

Abbreviations: BMI, body mass index; PHQ-9, Patient Health Questionnaire-9; T2D, type 2 diabetes.
n = 350.
n = 300.
n = 304. Bold values indicates a significance level of <0.05.
Multivariate Associations Between Information Needs and Depressive Symptoms
Age, sex, diabetes duration, how well informed, and information needs accounted for 14.9% of the variance in depressive symptoms (Table 4). After adjusting for covariates (ie, age, sex, and diabetes duration), a higher composite score of needs for further information was significantly associated with higher severity of depressive symptoms (B = 0.368, 95% CI, 0.155-0.582, P = .001). No collinearity and heteroscedasticity was detected.
Multivariate Linear Results of Information Needs Predicting Depressive Symptoms a

Model statistics, R2 = 14.9%, P < .001. Bold values indicates a significance level of <0.05.
Discussion
There are few studies investigating information needs in people with T2D. This study was among the first to examine the association between information needs and depression in people with T2D. The results showed that unmet information needs were significantly associated with depressive symptoms. These results further highlight the importance of addressing information needs in adults with T2D.
In a prior study conducted among 220 people with T2D in Ireland, participants indicated they most needed diabetes information about causes and risk factors, prevention and diagnosis, disease distribution, treatment, and complications measured by open ended-questions. 30 Adults with newly diagnosed diabetes (N = 138, 54% T2D, 64% males, 46.3 years) in Germany were best informed of the following diabetes-related topics measured by INDQ: treatment/therapy, causes of diabetes, and long-term complications; they were least informed of topics including support and helplines, mental strain, and diabetes research. 31 In comparison, in a recent study conducted among patients with diabetes and atherosclerotic cardiovascular disease in Germany (N = 210, 71% males, and 75 years), the patients were best informed of lifestyle adjustment and least informed of support and helplines measured by a shorter version of INDQ. 26 This study demonstrated that participants were best informed about mental strain, treatment/therapy, and diabetes in everyday life and least informed of diabetes research, acute complications, and lifestyle adjustment. When asked to rate their need for further information, participants chose mental strain, treatment/therapy, and diabetes in everyday life as the top 3 topics for which they needed information. These differences may be due to different baseline characteristics such as age (46.3 vs 64.8 years), diabetes duration (newly diagnosed vs 10.6 years), 31 and culture, which may influence information sources, people’s health beliefs, and motivation to seek for information. 32
In this study, participants were least informed about diabetes research, which is consistent with the study about newly diagnosed diabetes in which 68% were not well or not informed at all on this topic. 31 Despite being least informed about diabetes research, participants rated their needs for further information about diabetes research lowest among all categories. This is in sharp contrast with findings from the newly diagnosed patients in that 86% of participants rated information needs about diabetes research as the highest among the topics. 31 It is possible that diabetes research is not intuitively related to patients’ daily self-care behaviors and diabetes management. When they cannot benefit directly from diabetes research, their needs may not be high. People in developing countries (eg, China) have less knowledge about research than those in developed countries, which may also explain their low need for this topic. A gap has been reported between Asian and other ethnic groups in terms of research involvement. 33 Based on a qualitative study conducted in Singapore, 34 there are cultural, social, and political challenges specific to Asian populations for patient involvement in research. Collectively, these findings suggest a need to raise the public’s awareness of getting involved in research in this cultural background. Such efforts may increase patients’ needs for information about diabetes research.
Noticeably, the top 3 best-informed diabetes-related topics remained the top 3 that were of the highest levels of needs for further information among participants in this study. They were mental strain, treatment/therapy, and diabetes in everyday life. This finding is in contrast to the one found in the earlier German study. 26 In that study, the best informed topic was the one of the lowest level of needs for further information (ie, lifestyle adjustment). Findings from this study may indicate that although patients had the knowledge about those topics, the information was not internalized. It is also possible that the information they received was not sufficient for them to fully incorporate diabetes self-management into their daily routines. In fact, based on responses to questions about what information they needed, many patients reported the need for information tailored to their existing knowledge of diabetes. 31 Together, these findings suggest that more personalized diabetes education should be developed so that patients will have sufficient information and will be able to use this information to meet their unique needs or management goals.
Findings from this study showed that those with depressive symptoms were significantly less informed and had higher levels of needs for further information. After controlling for covariates (eg, age, gender, diabetes duration), unmet information needs remained a significant predictor of depressive symptoms, consistent with previous findings in other populations. For instance, in caregivers of renal cancer survivors, unmet information needs were significantly associated with higher levels of depressive symptoms (OR = 2.02, 95 % CI, 1.08-3.79). 16 In a recent study of people with brain tumors, patient information needs were also significantly related to depressive symptoms measured by PHQ-9 (OR = 3.01, 95% CI, 1.175-7.695). 35 This may be because unmet information needs are the reflection of patients’ difficulties in processing information 36 or applying them into daily practice to fulfill their goals. Based on a study conducted among cancer survivors, having depressive symptoms was negatively associated with perceived helpfulness of the received information and satisfaction with information. 37 It is likely that those with depressive symptoms were less satisfied with the information they received and thus have higher information needs than those without.
A major strength of this study was the use of a representative sample from 12 communities across Shanghai, China. However, there are several limitations. One limitation was the high number of missing values in need for further information. A similar pattern was observed in an earlier study. 21 Demographics of those with missing and those with no missing data were compared. These 2 groups only differed in age and smoking. These 2 factors were controlled in the multivariate analysis. Thus, it was assumed that the results were not likely to be biased. In addition, this study was cross-sectional in design, which limited the causal inference. Future interventional studies targeting information provision will help to unveil the causal relationship between information needs and depressive symptoms. Another limitation was the lack of objective measures. Although random glucose level was available for 300 participants, the data were not aligned with other measures. Thus, it cannot be included in the multivariate analysis. Future studies with objective measures of glycemic control (eg, H1C) are warranted.
Despite the aforementioned limitations, this study has implications for clinical practice and future research. Current practice guidelines recommend diabetes educators deliver individualized diabetes education, among which providing sufficient information is a major component. This study shed light on areas that should be prioritized in clinical practice and demonstrated that unmet information needs predicted depressive symptoms. Diabetes educators thus should address patients’ information needs, especially on mental strain, treatment/therapy, and diabetes in everyday life, and consider taking information needs into account when designing interventions for depression. Specifically, diabetes educators should provide information suitable for the individuals’ conditions or preferences so that they can process and apply it in daily practice.
Future research with longitudinal or interventional design is warranted to examine the impact of changes in information needs on depression and related self-care behaviors. Meanwhile, studies are needed to investigate the trajectory of information needs during the course of diabetes development and its associated factors and health outcomes. Such investigations will help diabetes educators to provide need-driven information and develop tailored diabetes education to better meet the needs of specific groups.
Conclusions
In summary, findings from this study revealed that unmet information needs were associated with depressive symptoms among people with T2D. These results highlight the need to meet health information needs in people with T2D when designing mental health interventions and provide guidance for the development of targeted diabetes education.
Footnotes
Acknowledgements
We thank all participants who joined the study. We thank members of the Shanghai Nursing Association-Diabetes Care Sub-Committee for their assistance with data collection.
Conflicting Interests
The authors declare that they have no conflict of interests.
Funding
This work was supported by the National Natural Science Foundation of China (71904119) and Innovation Research Team of High-Level Local Universities in Shanghai (SHSMU-ZDCX20212800). Bingqian Zhu was supported by Shanghai Municipal Education Commission Young Eastern Scholar and Shanghai Jiao Tong University School of Medicine-Nursing Development Program. The funding sources have no roles in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.