
Abstract
Purpose:
The purpose of the study was to understand the extent to which organizations offering the Centers for Disease Control and Prevention’s (CDC) National Diabetes Prevention Program (National DPP) lifestyle change program implement session zero (a pre-enrollment session designed to recruit, engage, and enroll participants in programs), the stated purpose(s) for offering session zero, the content of session zero, and best practices for using session zero for recruitment.
Methods:
Researchers conducted a survey of all organizations offering the National DPP lifestyle change program that were registered with the CDC’s Diabetes Prevention Recognition Program and their affiliated delivery locations.
Results:
Most (79.5%) delivery locations reported implementing session zero; of these, most used session zero as a recruitment strategy (81.1%) and orientation session (72.8%), whereas few (17.7%) used session zero solely to complete participant enrollment paperwork. Most (60.7%) delivery locations that implement session zero offer all their sessions at the same location, offer one session per upcoming participant cohort (66.7%), and use a consistent agenda (83.0%). Out of a list of activities informed by behavior change theory, the most common was offering an opportunity to enroll in the year-long lifestyle change program at the end of session zero (71.1%).
Conclusions:
Most National DPP delivery locations implement session zero as a recruitment and orientation session. Most delivery locations reported including some activities informed by behavior change theory, but delivery locations could offer more theoretically informed activities during their session zero. The findings provide practice-based considerations for implementing session zero for recruitment into lifestyle change programs.
An estimated 96 million US adults (38% of the US adult population) have prediabetes, a serious health condition where blood sugar levels are higher than normal. 1 Prediabetes can progress to type 2 diabetes, placing individuals at increased risk for heart disease, vision loss, and kidney disease, among other serious complications. 2 Fortunately, previous studies show that lifestyle change interventions are effective in reducing the risk of type 2 diabetes among people with prediabetes.3,4 Consequently, the Centers for Disease Control and Prevention (CDC) established the National Diabetes Prevention Program (National DPP), a partnership of public and private organizations working to build the infrastructure to support nationwide delivery of a structured year-long lifestyle change program proven to prevent or delay the onset of type 2 diabetes in adults.5,6
The CDC has made great strides in scaling and sustaining the National DPP. 7 However, expanding enrollment in the lifestyle change program remains a priority. 8 Offering a “session zero” is one promising strategy to increase engagement in the National DPP lifestyle change program and other chronic disease programs.9 -13 Session zero (a presession or introductory session) is a pre-enrollment session used to recruit, engage, or enroll participants into the National DPP lifestyle change program. The session introduces potential participants to the program before the start of the formal year-long class. To the authors’ knowledge, no systematic assessment has been conducted of how many organizations delivering the National DPP lifestyle change program offer session zero, how these sessions are conducted, how these sessions may vary across organizations, or whether these sessions include activities informed by behavior change theory.
Incorporating a theoretical approach to the design and implementation of behavior change interventions is helpful for understanding, explaining, and predicting individual behaviors and behavior change.14,15 Previous studies have shown that interventions informed by behavior change theory may increase the likelihood of intervention success.14 -18 For example, principles from behavioral economics suggest that using “nudges” that influence behavior by changing the way choices are presented without affecting an individual’s freedom of choice can improve the uptake of healthy lifestyle change behaviors,19 -21 including improving enrollment in diabetes interventions.22,23 In this case, delivery of session zero offers a timely opportunity to incorporate strategies informed by behavior change theory that may increase the likelihood of an individual enrolling in the National DPP lifestyle change program. Understanding the current landscape of how and why National DPP delivery organizations implement session zero may provide important practice-based considerations for the optimal use and implementation of session zero as a recruitment strategy.
Research Questions
This article summarizes findings from a landscape assessment conducted to assess the use of session zero and answers the following questions:
What proportion of National DPP delivery organizations’ class locations offer session zero?
How is session zero being offered?
What proportion of delivery locations offer session zero for recruitment versus an opportunity for individuals who have already enrolled to complete their enrollment paperwork?
What activities are offered during session zero?
Do delivery locations that offer session zero include activities informed by behavior change theory during their session zero?
Methods
Research Design
The authors conducted a cross-sectional survey in 2 phases from July to October 2020. All organizations delivering the National DPP lifestyle change program registered with CDC’s Diabetes Prevention Recognition Program (termed “CDC-recognized organizations”) as of June 2020 were eligible and invited to participate in the first phase conducted in July and August 2020. Any additional delivery locations reported by CDC-recognized organizations during the first phase of the survey were also eligible and invited to participate in the second phase conducted in September and October 2020. RTI International Institutional Review Board approved this study.
Sample and Setting
CDC-recognized organizations (n = 1545) were invited to participate using contact information in the CDC Diabetes Prevention Recognition Program database, and 584 additional delivery locations were invited to participate using contact information supplied by organizations that responded to the first phase of the survey. Twenty-two CDC-recognized organizations and 25 different delivery locations needed valid contact information. A total of 706 CDC-recognized organizations completed the first phase of the survey, either online or through paper-based submission, and 164 additional delivery locations completed the second phase of the survey, for response rates of 46.3% and 29.3%, respectively.
Data Collection Procedures
The authors programmed the survey instrument using the Voxco Survey suite and sent an electronic invitation. The authors sent 3 reminder emails to respondents to complete the survey. If respondents did not complete an electronic survey within 6 weeks, the authors mailed them a paper questionnaire.
Survey Development
Although the survey was conducted during the COVID-19 pandemic, survey instructions asked respondents to respond about implementing their lifestyle change program before the pandemic. The survey items assessed the following: organization characteristics, including organizational type, duration of time offering the National DPP lifestyle change program, number of participant cohorts offered in the past year, and participant demographics; session zero characteristics, including whether CDC-recognized organizations offer session zero and the average number of participants attending a session zero; session zero delivery characteristics, including delivery logistics, staffing, and activities delivered; and the impact of COVID-19.
The prevalence of session zero was assessed by asking CDC-recognized delivery organizations the question, “Do you offer an introductory session (also known as ‘session zero’) to potential participants?” Items related to session zero activities were assessed using the following question: “Which of the following elements are included in your program’s introductory/information session? Please check all that apply.” Some response options included activities focused on providing information or that were more structural in nature, such as offering light snacks. Other response options measured the prevalence of activities consistent with behavior change theories, including social cognitive theory,24 -26 the transtheoretical model, 27 and behavioral economics.28 -31 These items were adapted from previous work on session zero. 32 This work identified the most common behavioral barriers to enrollment in the National DPP lifestyle change program, including those that could be addressed in session zero using behavioral economic principles. These barriers include a lack of urgency regarding the need to make a lifestyle change; misperception of one’s type 2 diabetes risk; perception that the commitment costs of participating in a lifestyle change program outweigh future benefits of the program; lack of social influence, where individuals did not know anyone like themselves who had successfully participated in and completed a lifestyle change program; and a lack of self-efficacy for reducing one’s risk. 32 For example, to address the lack of social influence, session zero could include multiple social activities and invite a successful program graduate to discuss their experience with participants. Table 1 maps session zero activity response options to the behavior change theory that informed them.
Session Zero Activities Informed by Behavior Change Theory
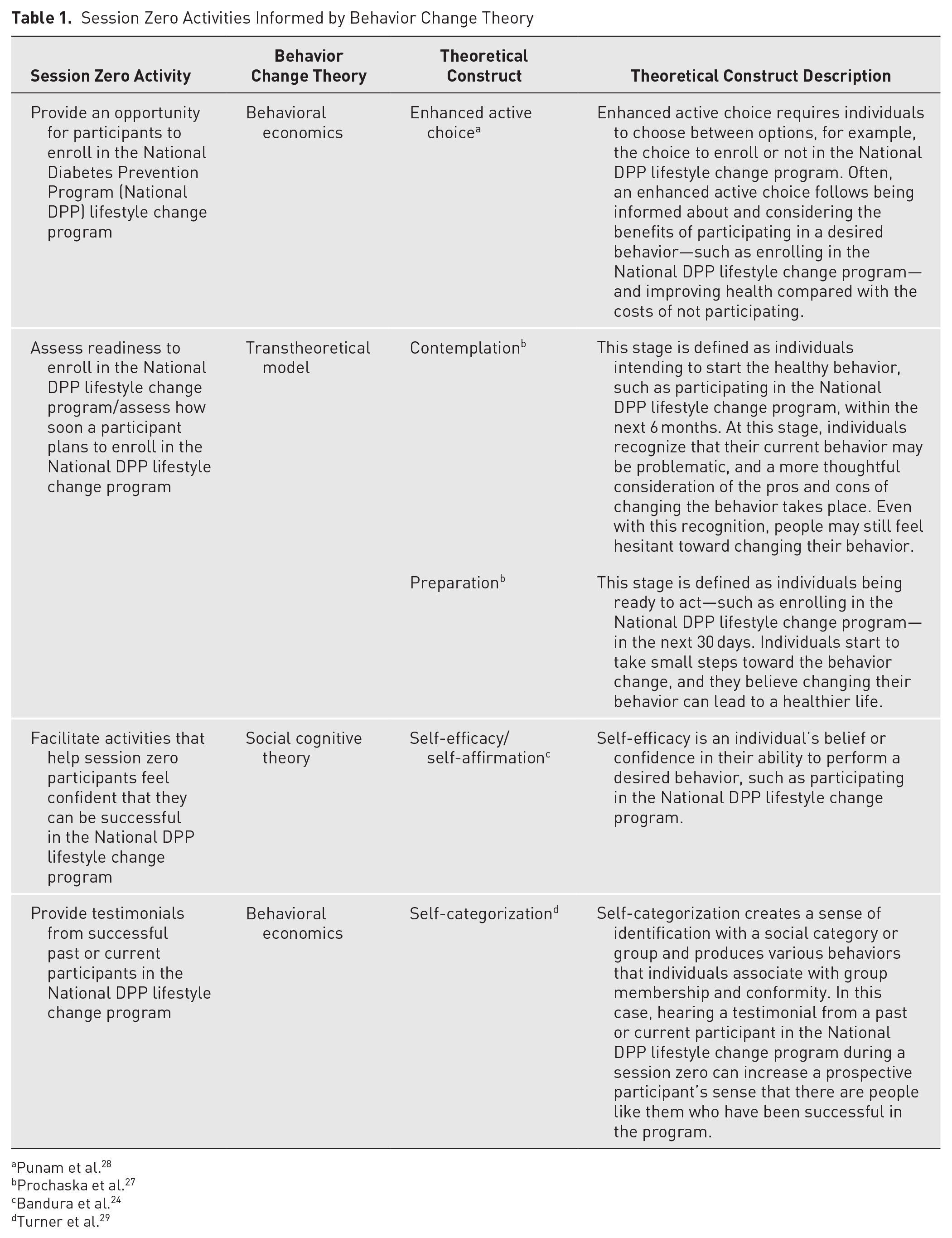
Punam et al. 28
Prochaska et al. 27
Bandura et al. 24
Turner et al. 29
Statistical Analysis
The unit of analysis was individual delivery locations. Delivery locations were defined as CDC-recognized organizations offering the lifestyle change program at their primary location during the first phase of the survey or additional delivery locations offering the lifestyle change program responding to the second phase of the survey. The authors conducted univariate descriptive analyses using Stata version 16, reviewed open-text survey responses, and recoded them as needed.
Results
Of the 706 respondents from CDC-recognized organizations completing the first phase of the survey, 662 reported offering the lifestyle change program at their primary location. The remaining 44 respondents reported that they did not offer the lifestyle change program at their primary location but provided contact information for their delivery locations who completed the second phase of the survey. One CDC-recognized organization was excluded from analysis due to the presence of extreme outliers in its responses. Taken together with the responses from the delivery locations completing the second phase of the survey (N = 164), the analytic sample resulted in a total of 825 unique National DPP delivery locations. Figure 1 displays the respondent flow diagram for the first and second phases of the survey.
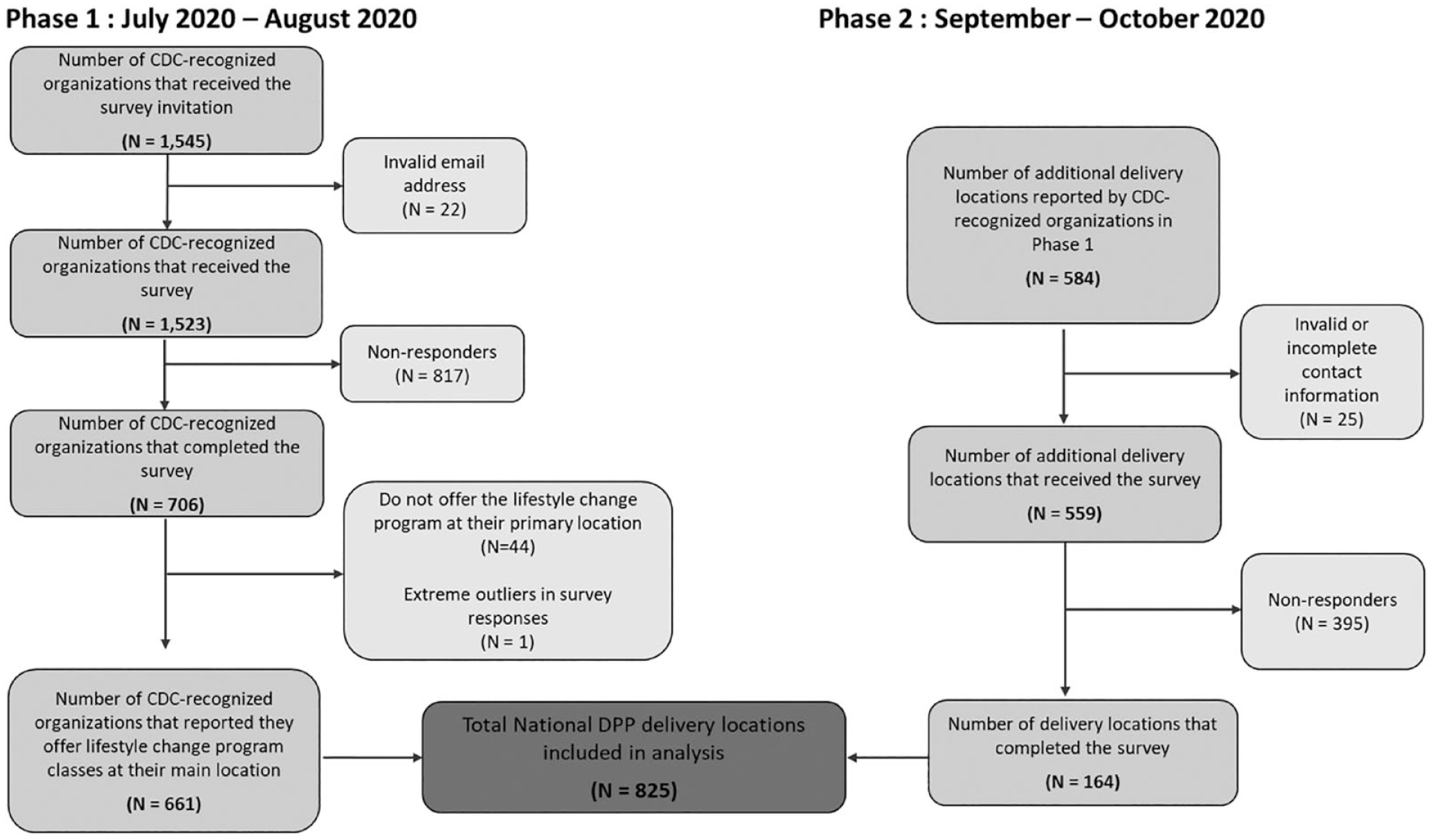
Flow diagram of survey responses.
Characteristics of National DPP Delivery Location Sample
Delivery locations offering the National DPP lifestyle change program most commonly characterized themselves as health care facilities, such as hospitals, health care systems, medical groups, or physician practices (n = 286, 34.7%); YMCAs (n = 98, 11.9%); and community-based organizations (n = 96, 11.6%). Delivery locations reported offering the National DPP lifestyle change program for an average of 34.3 months, with a median of 2 year-long participant cohorts in the prior 12 months. Most delivery locations served a population that was predominately 45 to 64 years old (n = 613, 74.3%), female (n = 703, 85.2%), and White (n = 460, 55.8%). The vast majority offered only in-person classes before the COVID-19 pandemic (n = 600, 85.1%). During the pandemic, however, they shifted away from this teaching mode, with in-person classes becoming one of the least common program delivery modes (n = 44, 6.2%). Instead, offering only distance learning classes (i.e., virtual live video sessions; n = 193, 27.4%), combination classes (mix of in-person, distance learning, or online classes; n = 163, 23.1%), online-only classes (n = 118, 16.7%), and not offering classes (n = 173, 24.5%) became more commonplace during COVID-19. Most expected to provide combination classes in the future (n = 408, 57.9%). Table 2 presents the delivery location characteristics, and Figure 2 illustrates the impact of COVID-19 on lifestyle change program delivery.
Characteristics of Delivery Locations Offering the National Diabetes Prevention Program Lifestyle Change Program a
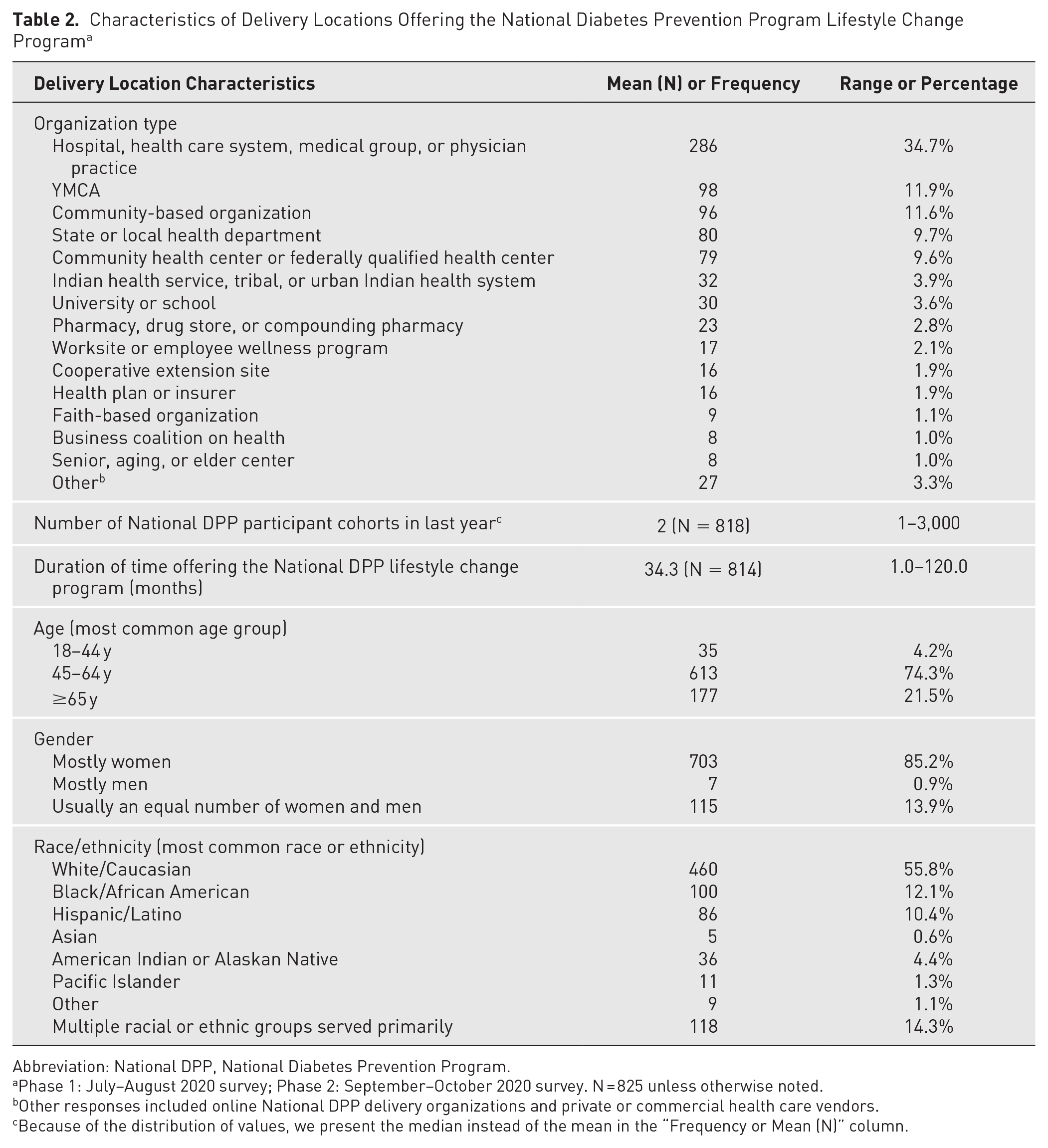
Abbreviation: National DPP, National Diabetes Prevention Program.
Phase 1: July–August 2020 survey; Phase 2: September–October 2020 survey. N = 825 unless otherwise noted.
Other responses included online National DPP delivery organizations and private or commercial health care vendors.
Because of the distribution of values, we present the median instead of the mean in the “Frequency or Mean (N)” column.
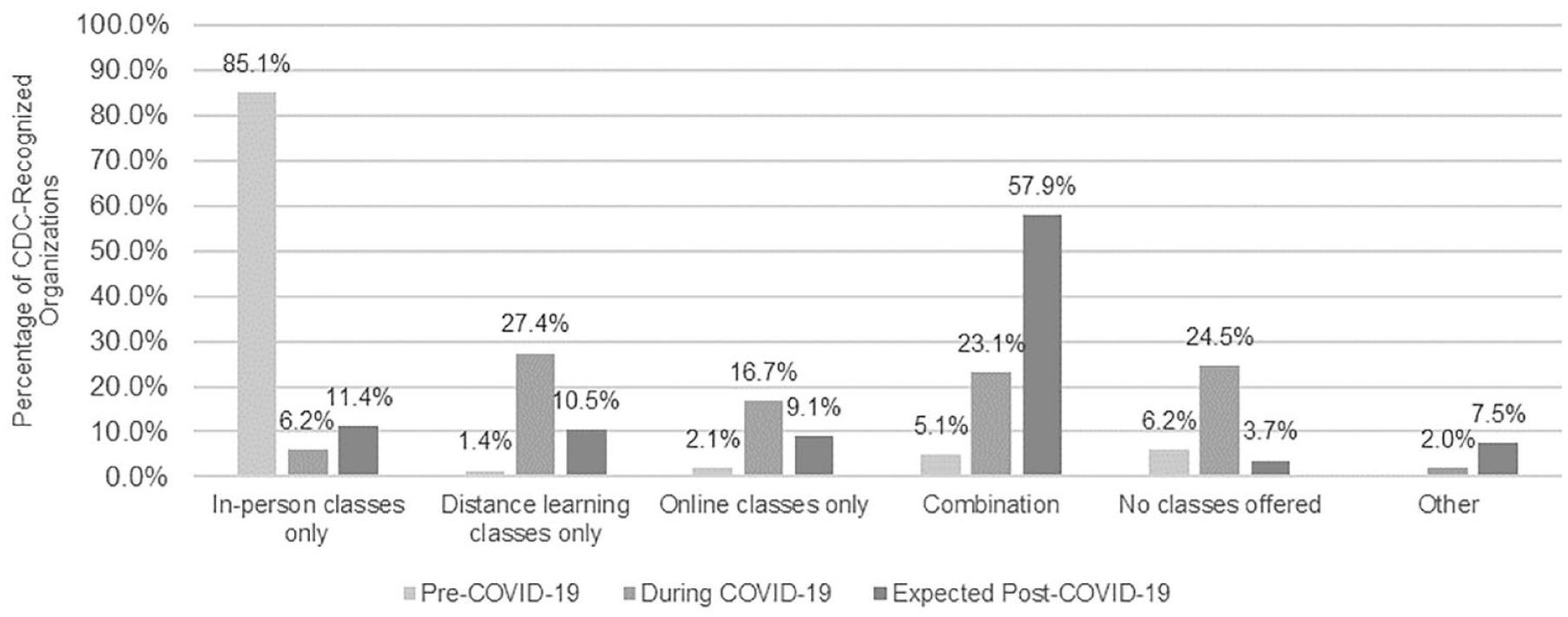
Impact of COVID-19 on National Diabetes Prevention Program lifestyle change program delivery. July–August 2020 Survey (Phase 1). N = 705.
Offering Session Zero
Among the 826 respondents, 657 delivery locations (79.5%) reported implementing session zero. Most locations that implemented session zero used them as a recruitment strategy (n = 533, 81.1%) and/or as an orientation session (n = 478, 72.8%; Table 3). Only 17.7% (n = 116) of delivery locations that implemented session zero indicated that they offered session zero solely as an orientation session to help participants who had already enrolled and committed to the year-long lifestyle change program complete remaining paperwork. Only 18 delivery locations (2.7%) offered session zero as a retention tool. Delivery locations that offered session zero reported offering it an average of 4.1 times in the past year to an average of 17.6 (median 10) participants at each session.
Characteristics of Session Zero Offerings and Participant Engagement Among National Diabetes Prevention Program Delivery Locations Offering Session Zero a
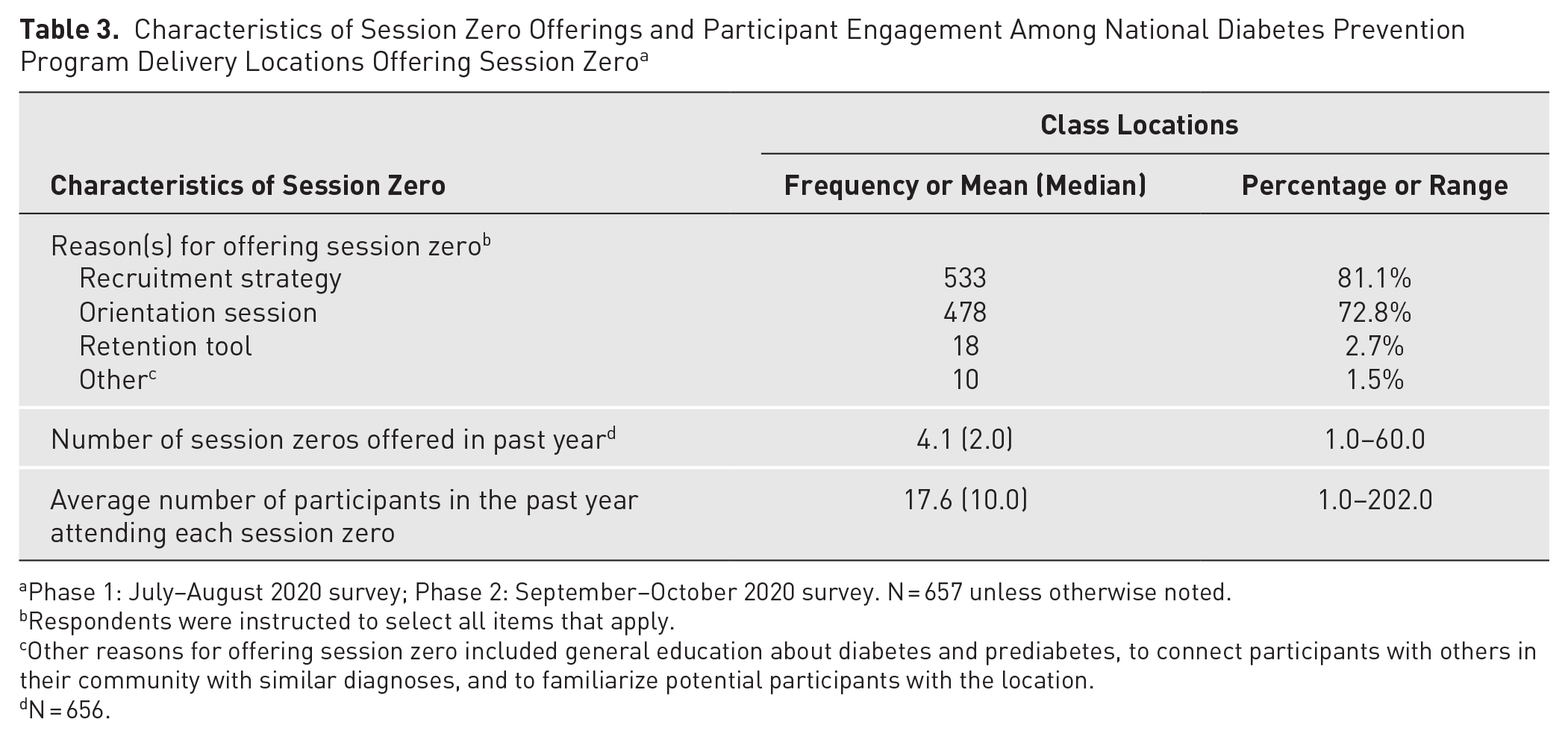
Phase 1: July–August 2020 survey; Phase 2: September–October 2020 survey. N = 657 unless otherwise noted.
Respondents were instructed to select all items that apply.
Other reasons for offering session zero included general education about diabetes and prediabetes, to connect participants with others in their community with similar diagnoses, and to familiarize potential participants with the location.
N = 656.
Characteristics of Session Zero Delivery
Table 4 presents data on the 657 delivery locations that implemented session zero. Most delivery locations offered session zero at the same location for all session zero offerings (n = 399, 60.7%), offered one session zero per upcoming participant cohort (n = 438, 66.7%), and used a consistent agenda (n = 545, 83.0%). The most frequent duration of these sessions was 45 to 59 minutes (n = 284, 43.2%).
Characteristics of Session Zero Delivery Among National Diabetes Prevention Program Delivery Locations Offering Session Zero a
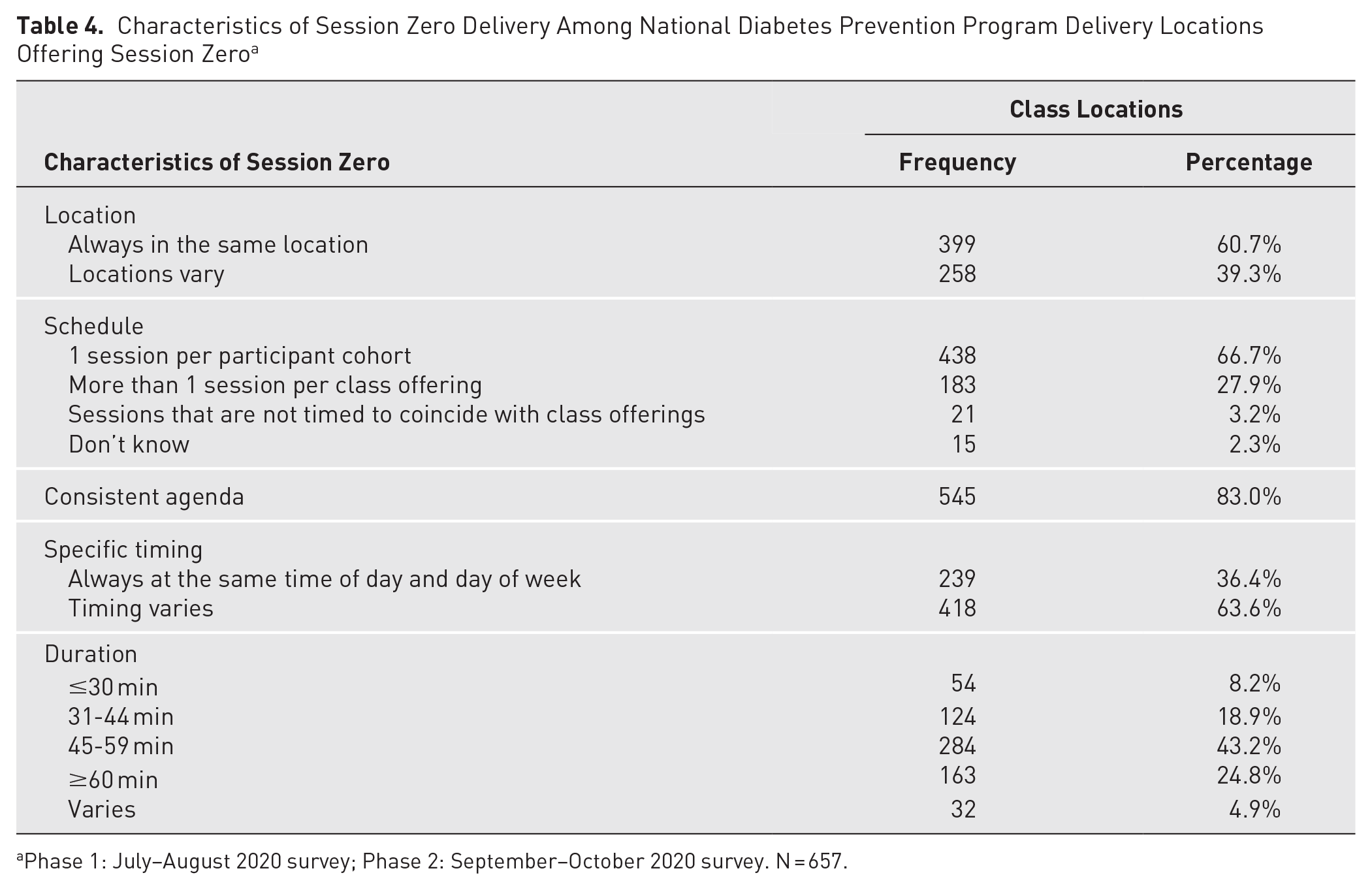
Phase 1: July–August 2020 survey; Phase 2: September–October 2020 survey. N = 657.
Staffing for Delivering Session Zero
Table 5 describes session zero staffing characteristics. Nearly all the 657 delivery locations (n = 617, 93.9%) that implemented session zero reported that lifestyle coaches delivered session zero. Most respondents also used program coordinators to provide session zero (n = 396, 60.3%). Past participants (7.9%), medical or clinically trained staff, and other staff also delivered session zero, although at a much lower frequency than lifestyle coaches and program coordinators. On average, delivery locations used 1.9 employees to deliver session zero.
Staffing for Delivering Session Zero a
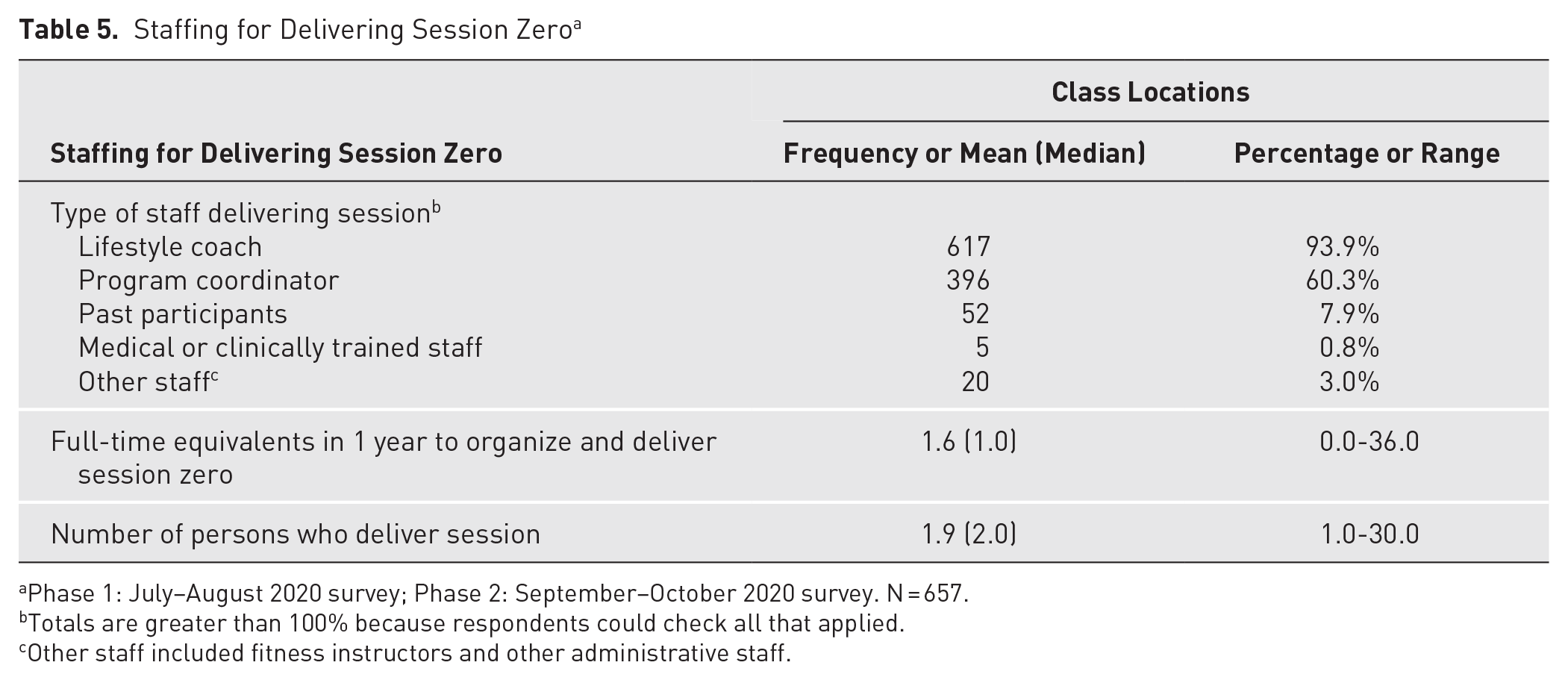
Phase 1: July–August 2020 survey; Phase 2: September–October 2020 survey. N = 657.
Totals are greater than 100% because respondents could check all that applied.
Other staff included fitness instructors and other administrative staff.
Session Zero Activities
Nearly all delivery locations (n = 643, 97.9%) included an overview of the National DPP lifestyle change program, including what to expect, time commitment, cost of the program, and date, time, and location of classes (Figure 3). The next most common activity was the opportunity to meet the lifestyle coach (n = 566, 86.1%), followed by information about type 2 diabetes, type 2 diabetes prevention, and prediabetes (n = 526, 80.1%). The least common activity was assessing how soon a participant plans to enroll in the lifestyle change program (n = 170, 25.9%). Offering activities informed by behavior change theory was reported less often compared with the other types of activities provided during session zero. Of the activities informed by behavior change theory (those shaded gray in Figure 3), offering an opportunity to enroll in the year-long lifestyle change program at the end of session zero was most commonly reported (n = 467, 71.1%), followed by offering opportunities to assess readiness to take part in the lifestyle change program (n = 420, 63.9%), providing activities to help session zero participants feel confident they could be successful in the lifestyle change program (n = 268, 40.8%), providing a testimonial from successful past or current lifestyle change program participants (n = 252, 38.4%), and assessing how soon a participant plans to enroll in the lifestyle change program (n = 170, 25.9%).
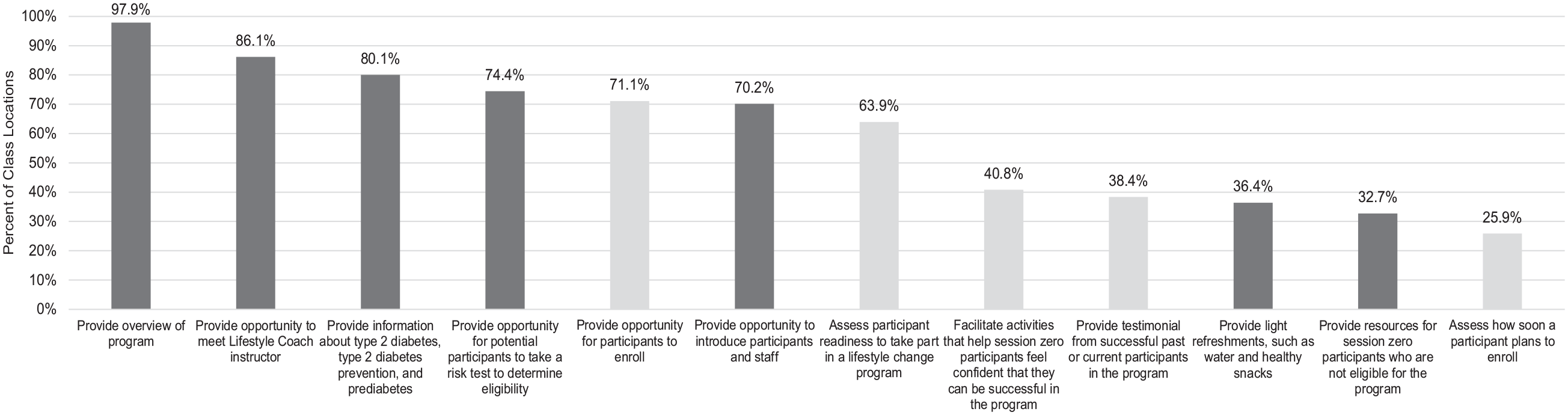
Frequency of specific activities included in session zero.
Discussion
This study deepens knowledge of the extent to which CDC-recognized organizations delivering the National DPP lifestyle change program are using session zero, the purposes for offering session zero, and the activities involved in session zero. The authors present data from the most comprehensive national survey to date of National DPP delivery organizations—662 CDC-recognized organizations and an additional 164 affiliated delivery locations—on their use of session zero. To the authors’ knowledge, this is the first prevalence data on session zero being offered among all CDC-recognized organizations (in 2020), with approximately 80% of responding delivery locations reporting they implement session zero. This study differs from an older, smaller study assessing a subset of 165 CDC-recognized organizations, which found that only 54% used session zero as a recruitment method in 2017. 33 The study findings described here show that a majority of delivery organizations offer session zero and predominantly do so to bolster recruitment. These findings align with prior work that suggested session zero as a promising strategy for increasing engagement in lifestyle change programs.9 -13
To the authors’ knowledge, this is also the first time data were comprehensively collected on how National DPP delivery organizations implement session zero for recruitment. Based on the study findings, session zero is implemented fairly consistently across all delivery organizations, with most offering session zero at the same location for every offering (60.7%), offering a single session zero prior to each upcoming participant cohort (66.7%), delivering it using a consistent agenda (83.0%), and having lifestyle coaches deliver it (93.9%). For National DPP delivery organizations considering offering session zero for recruitment, these findings provide important practice-based considerations, including insight on the number and type of staff and types of activities needed for implementation of session zero as a recruitment strategy.
The study findings also revealed that while most organizations reported that they include some theoretically informed activities—such as offering an opportunity to enroll in the lifestyle change program and assessing participant readiness to take part in the lifestyle change program—delivery locations could offer more theoretically informed activities. Only 40.8% of delivery locations reported including activities to help participants feel confident that they can be successful in the lifestyle change program. Adding these types of activities during a session zero can increase participants’ self-efficacy, which may increase their likelihood of enrolling and participating in the National DPP lifestyle change program.24 -26 In addition, only 38.4% of delivery locations reported providing a testimonial from a successful past or current lifestyle change program participant. In doing so, individuals can have an increased sense that they are like a former or current participant and can see themselves participating and being successful in the lifestyle change program. Behavior change, such as deciding to enroll and participate in a lifestyle change program to prevent or delay type 2 diabetes, is a process, and incorporating theoretically informed activities into behavior change interventions may increase the likelihood of programmatic success. The theoretically informed activities examined in this study incorporated constructs from multiple behavior change theories that may address common barriers to enrollment (see Table 1).
Since implementation of the survey, CDC developed a theory-based session zero titled “Discovery Session” that incorporates the theoretically informed activities mentioned previously. 34 For example, the Discovery Session includes an activity where attendees work together to discuss how they might be able to add physical activity into their daily routine. By sharing ideas with group members and getting feedback from the lifestyle coach and others like them, they can begin to feel confident in their ability to add small healthy changes into their daily routine even before the start of the lifestyle change program and become more familiar with the types of activities provided during the program itself. CDC’s Session Zero Guide for Live Videoconferencing 34 (i.e., Discovery Session) provides everything a National DPP delivery organization needs to deliver a 60-minute session zero. This can be a useful resource for National DPP delivery organizations that want to include theoretically informed activities in their session zero or for those that want to implement session zero but do not know where to start.
Although including theoretically informed activities to overcome behavioral barriers to enrollment is important, it is not the only predictor of behavior change. An individual is most likely to change behavior when they have a strong intention to perform the behavior and the skills and abilities required to perform the behavior and when there are no environmental or other constraints preventing the behavior change. 35 A study assessing perceived barriers to engagement in the National DPP lifestyle change program found that difficulty in scheduling around other commitments, such as work, school, caregiving, and vacations; transportation; difficulty changing health behavior; and the presence of other health conditions were anticipated barriers to participation. 36 Only a quarter of these barriers were related to individual health behavior change—lack of knowledge, low motivation or self-efficacy 37 —implying that additional considerations are needed. Work also needs to be done to address barriers to participation other than individual behavioral barriers, such as social determinants of health.
Overall, the study findings highlight opportunities for future session zero implementation. Given the staffing needed to plan for and deliver session zero, organizations interested in delivering session zero for their lifestyle change programs may wish to partner with other organizations to do so. Specifically, smaller programs may benefit from umbrella hub arrangements where a central CDC-recognized organization could deliver a standardized and behaviorally informed session zero for multiple delivery organizations.
The findings reported here may have implications for virtual National DPP delivery organizations now that many more groups offer the program virtually because of the COVID-19 pandemic. Increased hybrid or virtual programs offer opportunities for more than 1 session zero per participant cohort, which may help with recruitment for upcoming sessions. A 2017 meta-analysis found that diabetes prevention lifestyle interventions delivered solely via electronic, mobile, and certain types of telehealth (stand-alone eHealth interventions) delivery modes had a smaller yet similar effect on weight loss than interventions with behavioral support given by a counselor remotely (distance learning) and interventions with behavioral support given by a counselor in person. 37
Limitations
Several study limitations should be noted. First, data collected from CDC-recognized organizations and affiliated delivery locations were self-reported; however, data were rigorously assessed for quality and completeness. Second, the response rate was 42%; nonresponse bias may still influence the estimates reported. We found minimal differences in key characteristics of responders and nonresponders (not reported), although there may be differences in implementation of session zero between those who did and did not respond to the survey. It is possible that nonresponders were not inclined to respond to the survey because they do not offer session zero. Consequently, the estimate of prevalence of offering session zero may be an overestimate, and the survey findings may not be generalizable to all organizations offering the National DPP lifestyle change program. Third, because of the timing of the survey, class locations described their lifestyle change program and session zero offerings before the COVID-19 pandemic, the vast majority of which were offered only in person. However, they may have shifted their lifestyle change program and session zero delivery, purpose, and content because of the pandemic. At the time of the survey, more than half of CDC-recognized organizations indicated that they planned to offer a combination of in-person and virtual classes in the future, which implies that many organizations may have made substantial programmatic changes as they moved to virtual delivery of the lifestyle change program. Finally, although the authors included all National DPP lifestyle change program delivery modes in the study sample, this did result in some wide variations for some of the characteristics, specifically, lifestyle change program class size, session zero attendance, and number of staff required to implement and deliver session zero. Because delivery of the National DPP lifestyle change program online likely differs from distance learning or in-person program implementation, the study findings are likely more applicable to the latter delivery modes.
Conclusions
With 96 million US adults estimated to have prediabetes and the effectiveness of the National DPP lifestyle change program in preventing or delaying type 2 diabetes well established, identifying effective strategies that increase enrollment in lifestyle change programs is imperative. This is the first systematic assessment of how many CDC-recognized delivery organizations offer session zero, how they are conducted, how they vary across organizations, and whether they include activities grounded in behavior change theory that may increase the likelihood of intervention success. It is also the first survey of National DPP delivery organizations to report data at the delivery location level. This study increases understanding of how and why these organizations implement session zero and provides important practice-based considerations for the use and implementation of session zero as a recruitment strategy for organizations offering the National DPP lifestyle change program.
Footnotes
Acknowledgements
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Renée A. Skeete was affiliated with CyberData Technologies at the time of the study and is currently affiliated with Sapodilla Group, LLC. We wish to acknowledge our RTI International colleagues Chris Carson and Nikie Sarris Esquivel for supporting data collection and Zohra Tayebali and Kathleen Axelrod for supporting data analysis. This study was presented in part at the American Diabetes Association Annual Conference, June 10-13, 2021 (virtual).
Funding
This work was supported by the U.S. Centers for Disease Control and Prevention under Contract No. HHSD2002013M53964B, Order No. 75D30118F03500.