
Abstract
This article examines the research and development of a mixed realities play-kit to prepare children for an MRI scan to be undertaken without the need for a General Anaesthetic. The kit uses three different types of play; augmented, virtual reality and physical to help children become familiar with the look of an MRI scanner, the noises it makes, the role of the radiographer, what to expect when they go to hospital and to practise staying still. We reflect on the initial multimodal research methods that were used to bring children into the first stages of the design and development process. These included, model making, drawing, play and informal conversations. From which, data were analysed with visual and thematic means to make an original contribution to the field of medtech design for children, in that we found young children (aged six and under) prefer to receive medical information through opportunities for multimodal play and storytelling. As a direct result of this finding, we matched different play types to the various areas of preparation outlined above. In doing so, paying attention to the specific affordances of the different ways in which modes are combined depending on if physical, augmented or virtual reality play are used. Such findings are likely to be useful to other researchers and developers creating medtech products for young children. For those interested in multimodality specifically, this article also provides insight into the connection between information, modes of communication and play and the application of these to research design.
Introduction
This article reports on co-design methods used with 4-10-year-olds during a research and development project, funded by Innovate UK, to produce a play-kit to prepare children to undergo a Magnetic Resonance Imaging (MRI) scan without a General Anaesthetic (GA) and the ways in which these highlighted storytelling and play to be children’s preferred way of receiving medical information. The overarching intention of the project was to find new ways for children to prepare at home for having an MRI scan. In order to do this, we drew on concepts of cultural probes to include children in the design process (Gaver et al., 1999; Wyeth and Diercke, 2006), which is a method that uses design props and prompts to discover the unknown (Gaver et al., 1999). This works particularly well for including research participants who are not designers in design processes. Importantly, cultural probes ‘elicit inspirational responses from people’ (Wyeth and Diercke, 2006) which in turn can provide step changes in the design of new technologies for users who have different demographics from members of the design team. This was the case with our project where the intended young users had different perspectives from the adult designers and developers.
The probes we designed were all multimodal including drawing, model making, play, and sorting activities. In relation to this we report on the various ways in which we included children in the first stage of research and development of the play-kit. Each probe was designed in order to elicit knowledge about how best to design methods for preparing to complete a successful MRI scan. These were; (1) keeping still for prolonged periods within a confined space, (2) feeling prepared for exposure to loud noises produced by the scanner, and (3) being familiar with the steps involved in the MRI process from initially entering the hospital reception to completing a scan. The latter included form filling, being weighed, removal of magnetic possessions that cannot be taken into scanners, as well as introducing the various hospital staff involved in the process. We focused specifically on these areas because literature and our medical partners told us these are the main obstacles that must be overcome in order to complete an MRI scan. This in turn would reduce the need for many young children to be routinely given a General Anaesthetic (GA) as a solution to these barriers which is important because GAs come with (albeit rare) substantial health risks and longer periods of time in hospital (Heales and Lloyd, 2022). In the initial stages of formulating the product concept, we heard from specialists at our partner organisation the Sheffield Children’s Hospital NHS Trust about how specially trained hospital play therapists, who although limited in numbers were one of the most successful resources in helping children prepare for a scan and minimising the need for a GA.
In response to this, we proposed that the development of a play-kit could potentially prepare children in a similar way. Based on our expertise in the design of play for children, as well as in researching with children, we framed the success of the play-kit as needing to uniquely include insight into young children’s own ideas and knowledge. Although we had not previously designed play for health care contexts, we saw this as particularly important given that Greenhalgh et al. (2017) found ‘many promising technological innovations in health…are characterised by non-adoption’ (p.365). Thus, we reasoned that playful co-design methods, suitable for younger children could be used to gain deep insights into children’s interests and knowledge and thereby ensure a match between our play-kit design and future child-users.
The findings of these co-design methods highlighted the importance of play and storytelling to young children when preparing for an MRI scan; findings that we would not have discovered without the co-design and multimodal methods. Such findings provide valuable insight for other child health applications which tend to be top heavy on factual medical information, rather than designed with play and storytelling in mind. We illustrate this by outlining how these findings informed our own product.
The article is structured firstly to review the literature on current means for preparing children to undertake an MRI scan, including comparable technology and games aimed at children, before outlining the final design for our play-kit. The second section describes the co-design methods used with school children aged 4 to 10-years-old. Then we describe how these methods were able to draw out a unique understanding of children’s desire to prepare for an MRI scan using play and storytelling that combines fact and fiction. Finally, we outline how we mapped these findings to specific elements of preparation and the unique affordances of different combinations of modes in three types of play; physical, augmented, and virtual reality. In doing so, we also make a contribution to the field of multimodal communication to show how combinations of particular modes best fit with specific types of information when disseminated through platforms of play.
Current means of preparing children for an MRI scan
Just before the project began the most recent MRI activity data available in the UK (where this study took place), states that in 2016-17, OECD, 2023 data suggests MRI rates in much of Europe are similar to those in the UK (40–50/1000 population). The same UK data also showed the rapid expansion of MRIs, with an increase of 9% reported on the previous year. The resource intensive methods that are currently available to prepare children for an MRI scan have had, and are likely to continue to have, limited impact on reducing General Anaesthetics (GA) rates which may be as high as 65% (Dixon, 2017). High GA rates have clear cost implications, alongside the potential side effects and longer recovery period (Heales and Lloyd, 2022; Runge et al., 2018). There is therefore a clear and urgent healthcare need. Further, alternative options for preparation have significant limitations in that none offer start-to-finish preparation that includes all aspects of having a scan, but instead a variety of options that focus on just one part. Many are also unsuitable for the younger age range of 4–10 years, where we identified the greatest potential benefit. In the context of rapidly accelerating health care costs in the UK and elsewhere, health providers require support strategies that are accessible and save costs. However, currently the most common means of preparation that are available are resource intensive, either in terms of labour, as in the case of Radiographic Aids and Hospital Play Therapists, or in time and space such as mock scans and model scanners. There is also a patchwork of other means that can be used away from a hospital setting such as apps, 360-degree videos and animations.
To manage their imaging procedure, children need clear information, encouragement and confidence-building using distraction techniques and constructive play (Hallowell et al., 2008). Current provision tends to focus upon information giving, with imaging services using various media to illustrate patient journeys. These make limited use of distraction or play. For example, McGlashan et al. (2018) and Szeszak et al. (2016) evaluated the use of an Internet based educational animation video that children would access prior to attending for their MRI. Other provision utilise gaming through interactive apps with mini games that are designed to prepare children for their MRI (e.g. Williams and Greene, 2015) Interventions using mini/toy MRIs (see for example Morel., 2020) or Mock MRIs (e.g. Thung et al., 2018) allow children to explore what will happen to them in a scanner: these have been shown to reduce GA rates. However, they are highly resource intensive, requiring significant input from play specialists who are seldom available in adult hospitals where the majority of child scans take place. The space and cost requirements of model and mock MRIs also limit their usability. Finally, although the importance of including children’s carers in preparation for MRI is acknowledged, current applications focus predominantly or exclusively on the child. To this end, a German research VR game prototype (Liszio and Masuch, 2017) and a Canadian interactive VR application (Stunden et al., 2021) represent the nearest, current state of the art. Yet, the prototype described by Liszio and Masuch (2017) is used in hospitals immediately prior to an MRI, provides no continuity between home and hospital and limited opportunities for children to engage, disengage and re-engage with the experience. There is no development of active coping strategies. Exposure to scan noises and the scanner environment is limited. There is no familiarisation with the language/instructions during scanning and no interaction with parents. The game is aimed at 8–15-year-olds for whom GA rates are lower. The VR simulation app described by Stunden et al. (2021) is aimed at 4–13-year-olds and appears to address some of these limitations through a virtual MRI experience and real time feedback game. Yet, the product has been designed without the direct input of children and young people. Our research and development project sought to address these limitations and importantly to do so by including children in the design process. In relation to this, the next section provides an overview of the means we developed to prepare children for an MRI scan, before going on to outline the co-design methodology used to achieve this.
Our means of preparing children for an MRI scan
In order to fully understand the co-design methods we used, this section provides an overview of our final play-kit. We knew from the start that the play-kit would include various characteristics; as these were stipulated in our funding application. These included that the play-kit could be sent to patients in the post and used at home without needing to be returned, would provide start-to-finish preparation that included sharing the entire process that would be required of each patient from receiving an appointment letter to being scanned, and finally, that we would explore the use of various play types for preparation. These included physical, augmented and virtual reality play. In doing so, we sought to find the best match between dissemination of medical information about aspects of the MRI scan process and play types. The final play-kit produced this in three ways. Firstly, a flat-packed cardboard kit that patients receive by post and can build into a toy MRI scanner using instructions on an accompanying mobile app (Figure 1). The scanner is designed to be slightly too difficult for a child to build alone, thereby encouraging conversation between a child-patient and their parent/carer as they build, which in turn helps reduce anxiety about their upcoming MRI scan. Further, because this part is made of cardboard it is accessible to children who do not have access to their own smartphone (such as is the case for most children in this age category). Thus, promoting repeat play without barriers caused by the need to access technology. Cardboard toy MRI scanner.
Each child also receives a cardboard VR headset. This can be used with the VR part of the mobile app that allows children to undertake a hospital walk through accumulating in entering the MRI scanner. The VR app also contains four virtual mini games; one where the user completes a form at reception, one to understand that they would need to be weighed, another to learn about removing magnetic objects from their clothing and belongings before entering the scanner, and the fourth to practise staying still (Figure 2): Virtual Reality mode.
The VR experience allows children to become familiar with hospital spaces, the procedure of having an MRI scan and to practice staying still which is essential for the production of successful images. The inclusion of VR also extends the age range of the playkit as it is appealing to older children (in this study those aged 9–10 years) but because it is made of cardboard it is lightweight for posting and also age-appropriate.
The third element of the play-kit uses augmented play. Here, children slot a smart phone in the side of their built cardboard MRI scanner and take on the role of the radiographer and scan a small toy figure or teddy (Figure 3): Augmented Reality mode.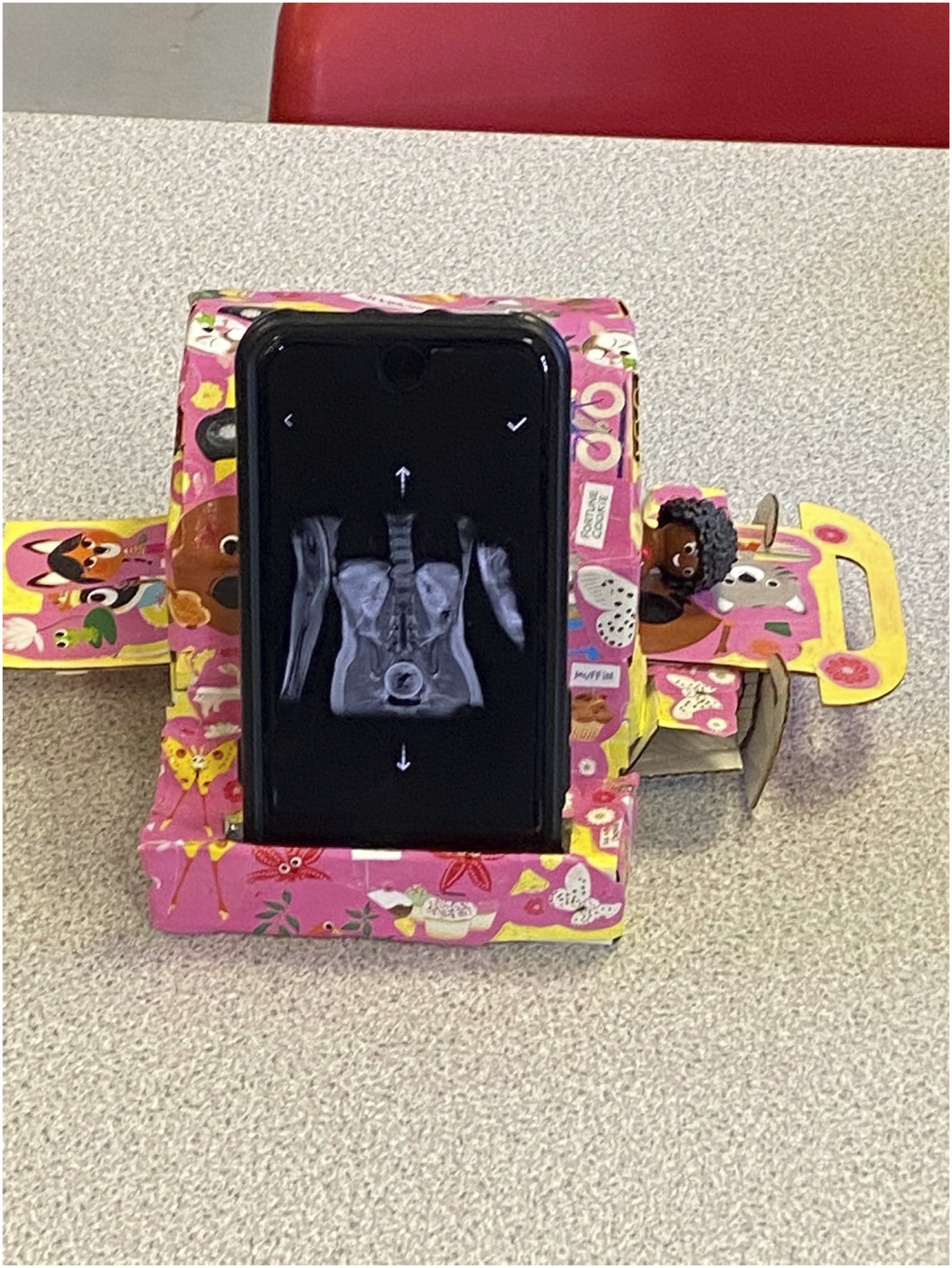
Understanding the role of the radiographer is also part of familiarisation and this reduces anxiety. As can be seen in Figure 3, the AR app uses realistic scan images which help children understand what the radiographers will see when they are scanned. All three types of play and their intended purpose and instructions are linked by a mobile app we developed for Android and ios.
Our decisions for producing this design were influenced by the co-design workshops we undertook with children which also ensured it is age appropriate. These are described next. After which the findings are outlined before it is shown how these fitted with the development of the final design outlined above.
Co-design methodology
As part of the remit of designing and producing a play-kit the project began by using co-design and participatory methods to include children in the design process from the start (e.g., Yanki 2008; Birch et al., 2017). To do so, we worked with four classes of children across three primary and junior schools (children aged 4–10-years-old): two in Sheffield and another in Glasgow (totalling 120 children). The children were selected for participation using a convenience sampling approach. The methods were designed to understand the audience, their attitudes to MRIs and to analyse existing apps used for the purpose of preparing children for an MRI scan. Using school children rather than patients at the start of the project meant we could focus on collecting data to feed into an age-appropriate design with an emphasis on engagement without worrying about the topic being sensitive or triggering, in the way that it might be to patients. Further down the line we tested the product with patients to make sure it met their needs, however this data is beyond the scope of this paper.
Before beginning data collection, University ethical approval was gained. Later, we applied for NHS ethical clearance, however the research included in this paper was from before we began working with patients. Thus, for the stages of research reported on here the risks to children were minimal as none of the participants were scheduled to have an MRI scan. This meant we applied BERA (2018) procedures of good ethics for research with children that included providing information sheets to schools, parents and an age-appropriate version for children, offering opportunities to ask questions before asking for written or verbal consent. Therefore, children in the schools whose parents (or primary caregivers) gave their consent were allowed to take part in the workshops; all children were given permission so no one was excluded from the workshops. Further, ethical issues were also addressed by the incorporation of participatory research methods, which, can also respond to the fact that inclusion of art and design-based subjects are increasingly being diminished from school curricula, and so this type of research can also be seen as offering creative opportunities that might not otherwise be available to some children (Atkinson, 2018).
Following this, we adopted a stance similar to that of Birch et al. (2017) who believe the direct involvement of children in the design process can afford valuable and unique insights when the model used for inclusion breaks traditional patterns and power relationships between them and the designer/design process. Thus, we began the project by undertaking research in schools to inform the initial stages of the design process. Workshops in schools allowed us to gain an understanding of the target audience in a familiar environment, whilst reaching children of varying developmental and socio-economic backgrounds. The workshops included drawing, model making and play, all of which are described in the next section.
The researchers involved in running the workshops had extensive experience of working on both UKRI funded research projects and commercial research and development co-design projects with children. Their expertise also includes the analysis and interpretation of data collected in these types of studies.
The workshops were between and hour and an hour and half in length, sometimes with a break when one occurred naturally in the school timetable. This accumulated in approximately 20 h of recorded data, as multiple audio recorders were placed in each workshop.
Drawing
In the first instance, we adopted drawing as a method (Mitchell et al., 2011) and asked the child-participants to draw themselves and their favoured forms of physical and digital play. Whilst they drew, their ongoing conversations were captured using a voice-recorder placed in the middle of each group of children. As well as children’s spontaneous conversations about their drawings, the voice-recorders captured answers to researchers’ specific questions about their favoured types of play. Such as, why they liked the play they had drawn, where and who they played with. This method was intended to produce insight into children’s existing play practices so that we could build on these when developing the play-kit design. The intention was that a product that tied in with children’s existing interests would be more likely to be used after production.
Model making
A verbal explanation of the MRI process along with photographs of scanners were shown to each class. Following this, children were separated into small groups of 4–5 children and asked to assemble a model MRI scanner from pre-cut cardboard pieces prepared by the design team. Pictures of an MRI scanner and a premade kit were shown to children as a template for completing their own. Additionally, each group was provided with decorative items, such as coloured pipe cleaners, paper, pens and tape to customise the MRI scanner they had built. In order to offer motivation and further understanding of the purpose of what they were building each group was also given a small toy character that needed an MRI scan. In relation to this, the child-participants were asked to consider how their character might feel if they were to have an MRI scan, and if there was anything, they could do to customise the scanner to allow their character to feel more comfortable. We observed common barriers and motivators for constructing the kit, and roles taken by children when constructing, customising and playing. These were recorded as field notes in the moment and also more extensively by audio-recorders placed in the middle of each group of children. Additionally, the completed models provided a dataset that gave insight into common features children felt would be useful for staying calm.
This method was based on the notion that ‘design development activities, such as model-making were reported to be more enjoyed and appreciated by children’ (Birch et al., 2017: p.249). Further, providing each group of children with a set of pre-cut materials acted as a form of cultural probe that Gaver et al. (1999) describe as an assemblage of materials ‘designed to provoke inspirational responses’ (p.22). This in turn is a method that combines well with the strong correlation between making and thinking (Ingold, 2013; Mäkelä, 2007). It was deemed that such ideas were important given the young age of children who might find verbal, written or more traditional means of offering their ideas to researchers challenging. Thereby fitting better with what James (2013) describes as the ‘fundamental embodied’ ways young children exist and make sense of the world. Further, in his seminal text ‘Before Writing’, Kress (1997) also suggests that different modes of communication beyond speech and writing ‘give rise to their specific forms of thinking’ (p.xvii). Finally, participatory design methods were used as a way of addressing the inability of traditional research methods to address what is needed for design and development (Van Den Akker et al., 1992).
Play
The final method used play as a two-fold form of data collection. As a means of understanding the strategies children already use for remaining still which is a vital skill needed to complete a successful MRI scan, because high quality images for medical diagnosis requires patients to stay still typically for 40 min to an hour and a half. To this end, a well-known game in the UK called ‘Sleeping Lions’ was played. In this game children lie on the floor as still as they can without responding to adult-players who try to make them move by pulling silly faces or coming in close proximity without actually touching. At the end of the game the researchers asked children to share their ideas about how they managed to stay still; their responses were voice-recorded.
The second means of play involved asking the child-participants to try two existing apps designed to familiarise children with the MRI process: ‘My MRI at King’s’ (Kings College Hospital) and ‘MRI Scan Experience’ (Siemens Healthineers). Both apps were preloaded onto tablets and smartphones. Users, the youngest of whom were 4-years-old, also had access to a cardboard Virtual Reality (VR) headset, to experience each app in VR mode. Participants were asked to share their thoughts of each app, including what they could see, what they liked and disliked, how the experience made them feel about getting an MRI scan, and what they learned from the app. Close observation of children’s use of these apps were designed to identify features that encouraged or limited understanding and preparation for an MRI scan, and children’s responses towards the two experiences, or if they had any follow-up questions regarding the process.
Data analysis
Three means of analysis were applied to the data. First, the audio recordings taken alongside each of the data collection methods were transcribed using a professional transcriber and analysed by one of the researchers trained in both social science and art and design research methods using thematic analysis (Braun and Clark, 2006). The drawings made by the child-participants were analysed using Visual Content Analysis that seeks to quantify variables in images (Bell, 2001). For example, variables such as inside or outside were applied to children’s drawings of play, as well as the specific play types as defined by Hughes (2006). The number of times these variables appeared in children’s drawings were then counted in order to understand the most popular. Finally, children’s model scanners were analysed using van Mechlen’s (2016) toolkit for analysing the products of child co-design activities. This is similar to visual content analysis but for physical objects to make it possible to quantify the occurrence of specific design choices made by children. In doing so, ‘the making and the products of making are seen as an essential part of research: they can be conceived both as answers to particular research questions and as artistic or designerly argumentation’ (Mäkelä, 2007: p.157). These methods highlighted how the child-participants made sense of non-fiction medical information through storytelling and play. This is described next in relation to key areas of preparation for the MRI process. It could be said that the art and design methods were playful and thus promoted this type of interaction, even so the findings stand in stark contrast to common means of communicating medical information to young children which is top heavy on serious information. Our findings showed that this seemed to go against the ways in which children naturally wanted to become aware of this type of information, as will be shown next. It is followed by a section that discusses how this fed into the final design of our mixed-realities play-kit.
The potential of play and storytelling in preparing children for an MRI scan
Bayer (2014) suggests that there are several frequently asked questions by children and young people in relation to preparing for an MRI scan. These are concerned with what an MRI is, whether it will hurt, its safety, including whether the noise can damage hearing, who performs the scan, how an MRI works and how long it takes before the patient can return home. We found that these were also largely the concerns of the participants in our study. However, the key difference is that our findings highlighted that children’s preferred way to receive this information was in a playful means that provides opportunities for creativity and storytelling. Our study data showed children included fictional elements into their play and story worlds in order to make sense of the factual medical information they were presented with. This desire to engage with factual information in this way has also been found by a range of researchers who have studied how children make sense of other fact-based subjects such as science education (Andree and Lager-Nyqvist, 2013; Caiman and Lundegard, 2018; Jakobson and Wickman, 2015; Siry and Max, 2013). These findings suggest that other available means for preparing children to undertake an MRI scan such as were outlined in the literature review that take a purely fact-based approach do not meet young children’s needs, also highlighted by Bhadwaj and Thompson (2021). In order to expand on this point this section is divided firstly to consider the role of play, storytelling and creativity in children’s exploration of core aspects of the MRI process, that is; (1) the workings of the MRI scanner, (2) the process, (3) staying still, and (4) noise levels to show how the child-participants, particularly the youngest were interested in making sense of these topics more in keeping with the findings of researchers into science education who demonstrated the importance of imagination to sense making.
The scanner
As was described in the methodology section, having been shown various photographs of MRI scanners and given an explanation of the process, the noise it makes and the need to stay still, the child-participants went on to build a scanner out of pre-cut cardboard pieces. Children created stories as they built which helped them process the information they were receiving about the MRI process. This is similar to findings by Caiman and Lundegard (2018) who found ‘children’s processes of imagination…come into play when they invent, anticipate and explore a problem important to them’ (p.687). The designs that the children made went along with storytelling and play which seemed to give rise to the particular process of the MRI scan they understood well or would be worried about. One recurring theme was around the tunnel to the MRI scanner, some groups modified the design to make it more colourful and appealing to enter. Another group talked about the need for different sized tunnels for different sized patients to enter. The data findings showed how the child-participants appeared to use the process of making to make sense of what they had learned. This is similar to Mäkelä’s (2007) investigation into ‘the ways in which art can be understood as a process of inquiry’ (p. 157), as is shown by children’s discussion on whether the entrance to the MRI needs a door: Child 1: “This can be a door.” Child 2: “We don’t need a door.” Child 1: “Well maybe I can do a different kind of door.” Child 3: “Well I don’t know about a door.”
Like the quotes above, the centre of much of the conversation between children while they made the scanner centred on the tunnel. The data showed that children clearly understood that in order to have an MRI scan a patient would need to lie in the tunnel showing they understood the factual information. However, their conversation extended beyond the factual and there were many playful examples of children extending this narrative into imaginary worlds. For example, one group of 4-5-year-olds speculated on whether there should be multiple tunnels for different sized humans and animals to enter. They did not really think they would be scanned with a giraffe but exploring the idea seemed to make the factual medical information palatable, as Olsson (2013) describes children’s questions are always much larger, much more playful and at the same time much more serious than we imagine’ (p.230).
The tunnel was also a key area of focus when decorating the MRI scanner such as can be seen in Figure 4 below where a group of 5-6-year-olds ignored the design of the tunnel we had given them and used colourful pipe cleaners to build a rainbow tunnel which they felt children (or indeed animals) would prefer to enter. Rainbow tunnel.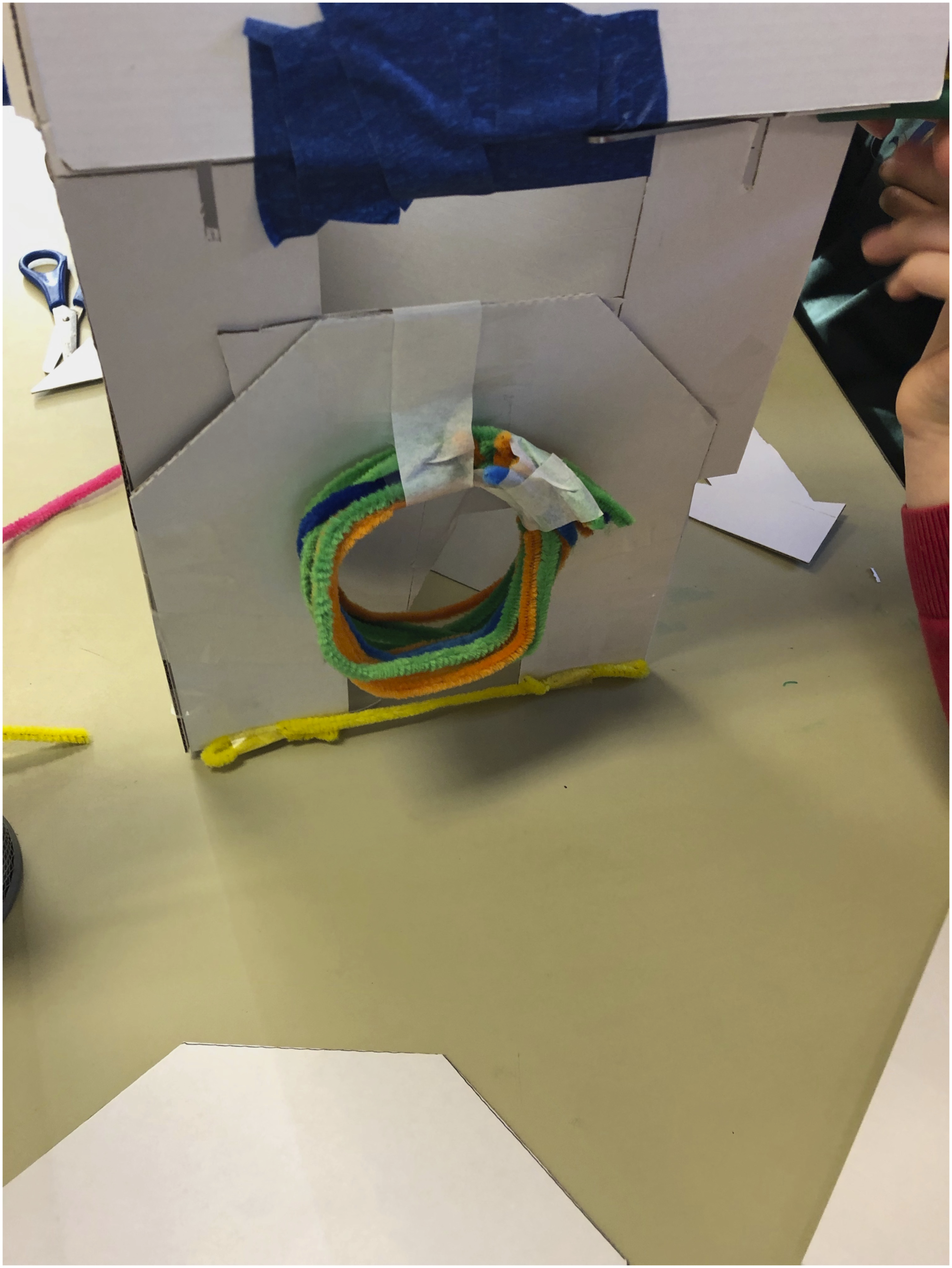
It could be argued that the design features children focused on showed them processing what it might mean to have an MRI scan and things that could be done to make them feel more comfortable. In a discussion of literature about makerspace practices Marsh et al. (2018) outline a range of studies that show how makerspaces can engage people not only in creative, but also critical practices (e.g., Hughes, 2016; Ratto, 2011). In this case the child-participants focus on improving the tunnel, fit with the conversation we had with one of our project partners who is Head of Radiology, who said that getting children into the scanner was the biggest challenge. Thus, the chance for the youngest children aged 4-years-old to undertake physical processes of making appeared to be important for their knowledge acquisition, and give a sense that it might address one of the key hurdles of getting into the tunnel.
Purpose
Perhaps because none of the children were anticipating having an MRI, their understanding of the purpose of the MRI was in relation to how it works rather than what it meant for their health. This they explored in relation to a series of toy characters they were given to put into the scanner once they had built it. This is similar to the Teddy Bear’s Hospital that allows children to understand medical interventions by modelling them with teddy bears (Warburton et al., 2022). The children’s role-playing with the toys produced fantastical rather than factual narratives about why they needed a scan: Child 1: [Picks up a toy to scan] “Oh no it looks like his feet are loose he needs a doctor.” Child 2: [Singing dramatically] “Dun duuuuun! He needs a scan.” [The toy is pulled out of the scanner] Child 1: “We can take his feet off and put robotic feet on.” Researcher: [After the toy has been scanned] “What was wrong with him?” Child: “He’s eaten a daddy dog.” Researcher: “No wonder he feels sick.” Teacher: “What’s wrong with the Penguin?” Child: “He couldn’t draw any more, he’s hurt his hand and can’t draw.” Teacher joining the group: “Right let’s see if it works then. You put them in and let’s see if they can get their scan done.” Child 2: “They are going to come out.” Teacher: “Ok bring them out then. They have had their scan. Are their brains looking OK? Are their bodies looking OK?”
The children look on the computer Child 1: “Yes…” Child 2: “I want to scan the bottom of their feet” [He uses a piece of cardboard to put under the toy character’s feet]. Teacher: “That is really inventive. So do they just stand on it?” Child 2: “Yeah and then it just scans their feet like this. Their feet will just be scanned in a second.” Child 1: “I am going to make a play arena for after.” Teacher: “Oh yes they will want to play after, good thinking.”
The teacher quoted above described the children’s ideas as inventive. This is important given that Caiman & Lundgård (2018) state ‘imagination is fundamental to integrating experience in the learning process’ (p.688). In other words, imagination demonstrated by the child-participants in combining model making and storytelling shows how children were active learners in the process of exploring medical information. Thus, the toy prompts given to children in this process were important.
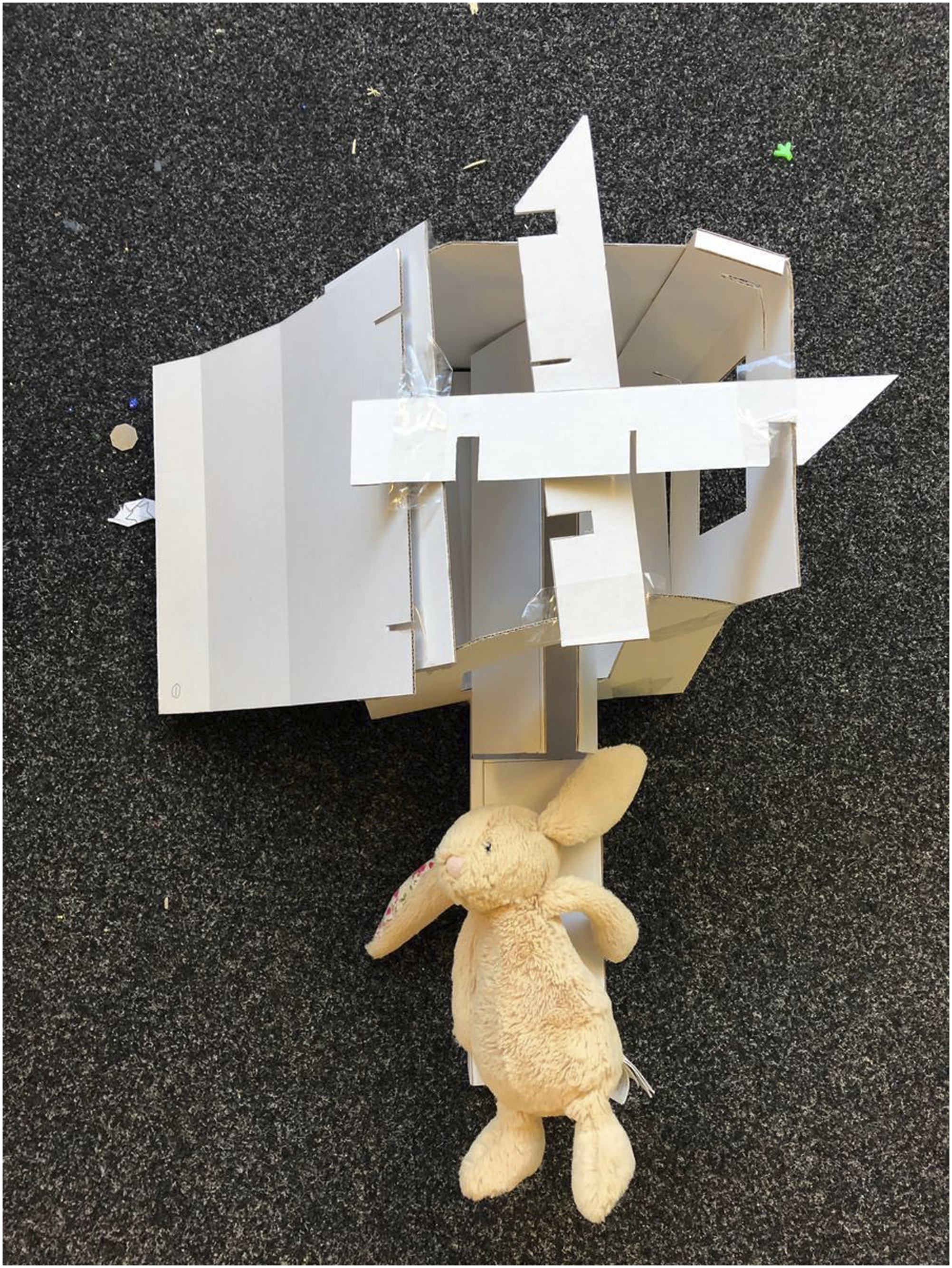
As well as demonstrating creativity in storytelling. The model making was also a form of play, and different aged children went about building the MRI scanner in different ways. The youngest children (4-5-years-old) were not interested in following the designer’s intentions and instead used the various cardboard sections of the scanner to build their own design, as is shown in the following examples: “We’ve made an MRI scanner and a computer to look at their brains and bodies (Figure 5 MRI scanner and computer. “You can look through the top to see if Rabbit is OK (Figure 6 Flip top MRI scanner.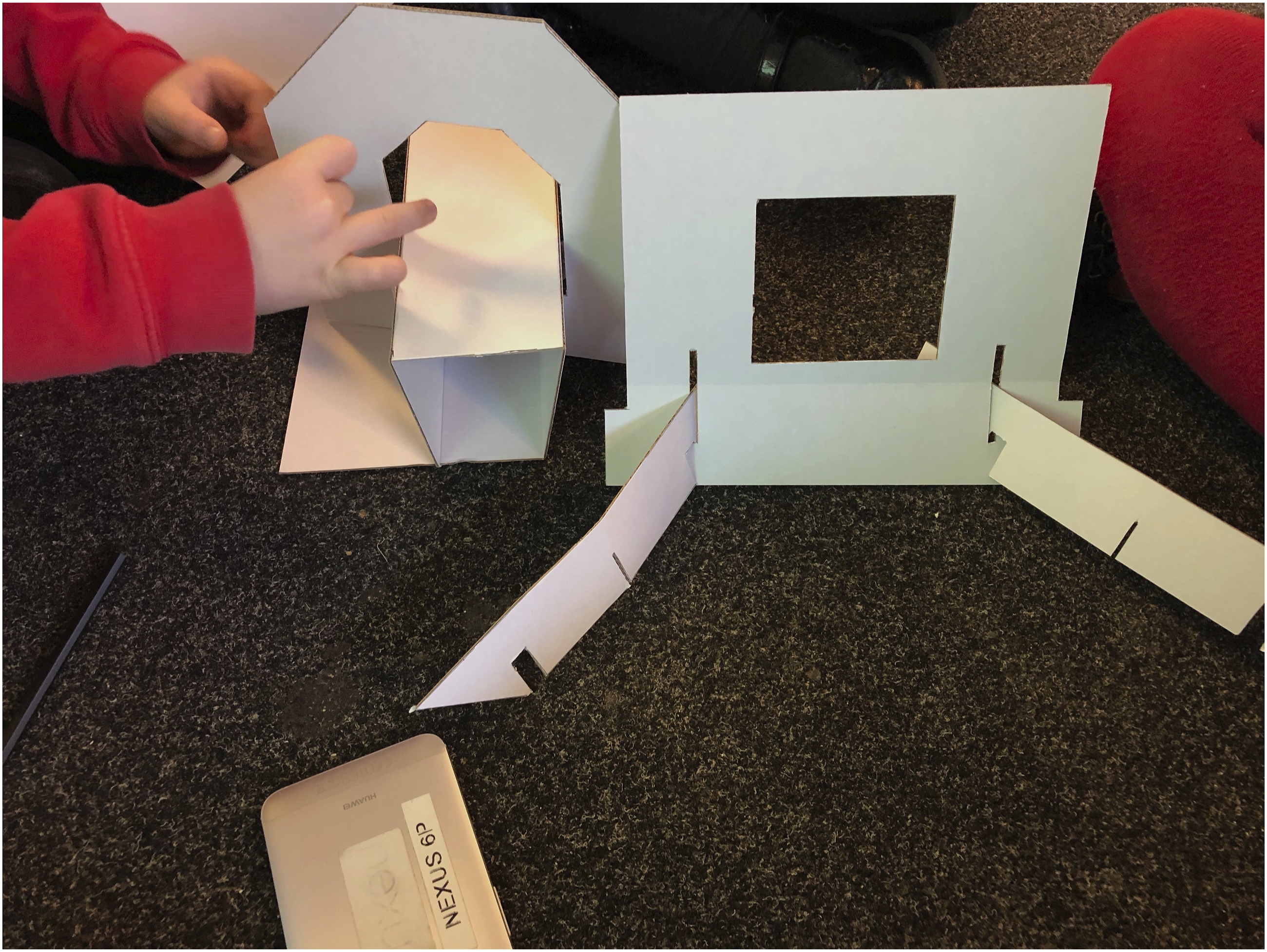
However, the 10–11-year-olds wanted to build the scanner kit to the specifications made by the designer. To do so they employed techniques that included careful observation and measuring: “This is the top because I just measured it.”
There was no originality in the construction process but there was in the ways they decorated the scanner (Figure 7): A range of decorated scanners.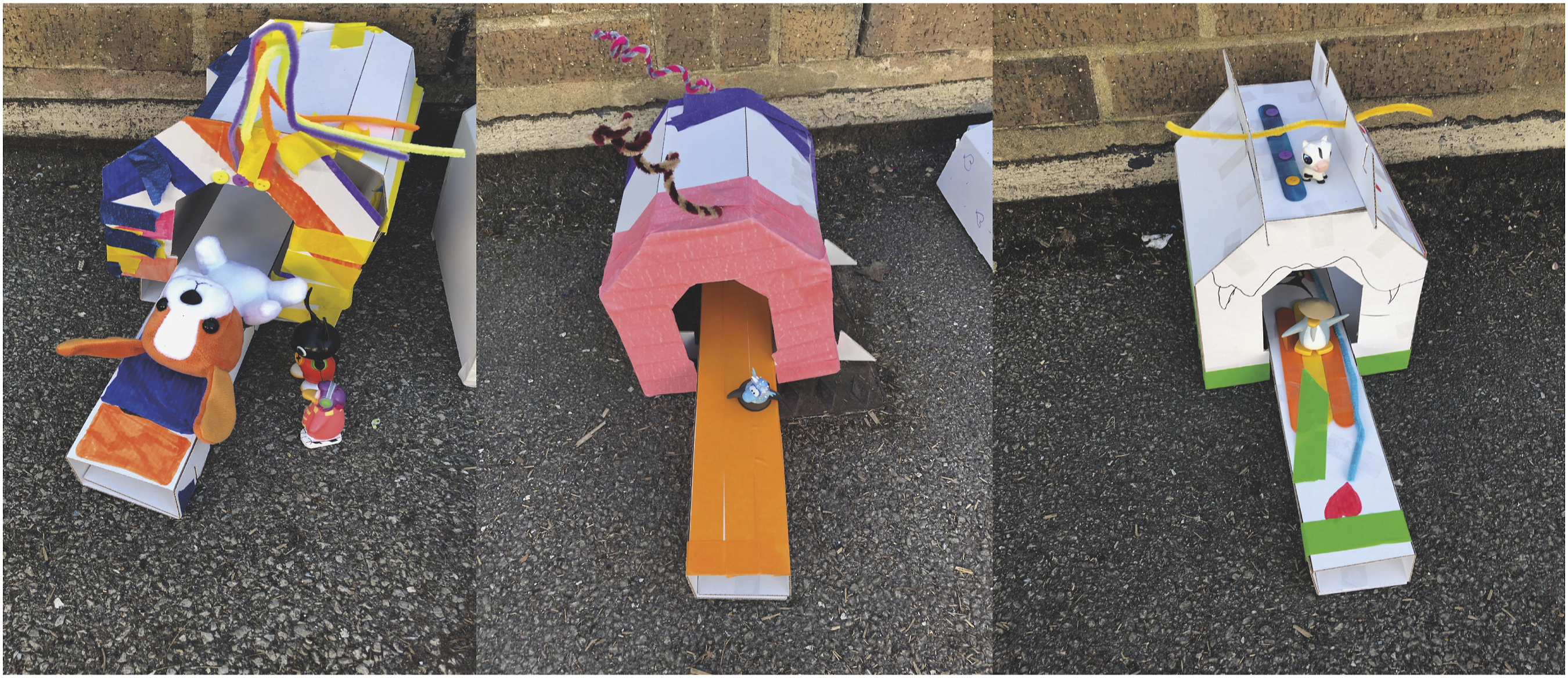
The participants’ enthusiasm for personalising the scanners was reflected in their requests for a larger range of materials to decorate with and other tips offered to the designers: “Make the cardboard colourful.”
Kress (2010) and Van Leeuwen (2013) show how the objects of play and the practices associated with them reflect wider social and cultural practices. The findings of this study also seem to illustrate this. In particular for the youngest children aged 4-years-old their teacher described how junk modelling, that is the use of recycled materials for school art projects, was part of their regular classroom practice and enjoyed by many of the children. For the oldest children (10–11-years-old) junk modelling was no longer a part of their schooling. Further many of the toys aimed at them are based on kit building rather than free play.
Staying still
The findings from playing the Sleeping Lions game to understand if children already had strategies for staying still indicated they used various methods of distraction, but that older children’s ideas were more sophisticated and were influenced by Mindfulness lessons that focus on being in the moment and keeping calm they had previously received in school: “I zoned out and focused on another thing.” “I was meditating- thinking of donuts.” “If you keep your eyes open just look at one thing as it shuts off everything else around you.” “In my house I have a really nice chair and I imagined myself in it.” “I put my tongue to the roof of my mouth.”
Although simpler, the youngest children (aged 4-years-old) still had means they employed to allow them to stay still during the game: “Bite my lip.” “Try to pretend to be asleep.” “Close my eyes really tight.” “Try not to move my finger.”
Ideas were also evident in children’s model making: Child 1: “This a cover and a strap.” Teacher: “To strap you in?” Child 1: “Yeah, so you don’t move around.”
Noise levels
Only one child out of four classes of children had undergone an MRI scan. None of the others were aware of the high volume of noise that an MRI scanner gives out. As a result, children first came across a representation of the scanner noises in the nearest competitor apps they tested, of which they enjoyed the way in which this was explained in the Siemens MRI Experience app the best because it gamified the process. It did this by asking children to guess how loud a scanner is compared to other noise objects/animals: Children aged 10: “I liked all the different noises and that you had to guess how loud it was” (Year 6).
Further, some of the noises made Y1 students laugh: A child aged 6: “A Hoover! hahahaha.”
Again, this is evidence of children’s desire to receive medical information in a playful manner.
This feedback illustrates how the child-participant’s interest in the information of having an MRI scan was linked to core aspects of the process such as the scanner, noise levels and the need to stay still. It also shows their preference for engaging with this information was in relation to opportunities to play, tell stories and be creative. Further, the youngest participants in our study (4-6-years-old), blended facts with make believe in the process of exploring medical information. This links with other literature that has stated that ‘when children create meaning there is no obvious dividing line between fact, fiction, sense and nonsense’ (Caiman and Lundegard, 2018). Campagna (2018) believes this is the case even for adults (though perhaps we do not verbalise it) and he describes how not all knowledge can be dissected into facts and so humans co-exist with two simultaneous realities, the factual/scientific which he describes as ‘technic’ and the other ‘magic’ reality. Perhaps because children’s understandings of the world are newer than those of adults it could be argued that children move between these two worlds more frequently. Giddings (2007) writes that the surrealist art movement’s ‘central concern with the contestation of conventional concepts and experiences of reality was pursued through the identification of alternative realities’ something he links as being parallel to how we play (p.397). Thus, akin to childhood meaning-making practices. Likewise, Bachelard (1953) also draws our attention to the two-fold nature of the engagements and techniques he discusses, drawing together the outer world of sensory encounter with the inner world of thought and imagination. This two-fold nature arises from ‘the total separation between the rational life and the life of dreams, thus accepting a double life; that of the existence of the night, and that of the existence of the day, the double foundation of a complete anthropology’ (Bachelard, 1953: p. 19). The next and final section looks at how we harnessed these ideas around making medical information playful and offer spaces for creativity and imagination to thrive in the decisions we made to match aspects of the medical information, to particular play platforms and the unique combinations of communicative modes within these.
Matching medical information to multimodal platforms of play
This section focuses on the unique affordances deriving from different combinations of communication modes foregrounded by three play platforms: physical, augmented and virtual play, and how these can best be used for the dissemination of medical information. As will be shown the decisions we made for using these three platforms in relation to preparing children for specific aspects of the MRI scan process came about in relation to the research findings and matching these to specific combinations of modes and their affordances in each of the three play types. This is important because with regards to the dissemination of information, Kress and Van Leeuwen (2005) write that the selection of modes for communication, such as image, writing, and sound affects how information is received: Like linguistic structures, visual structures point to particular interpretations of experience and forms of social interaction. (Kress and Van Leeuwen, 2005: p.3)
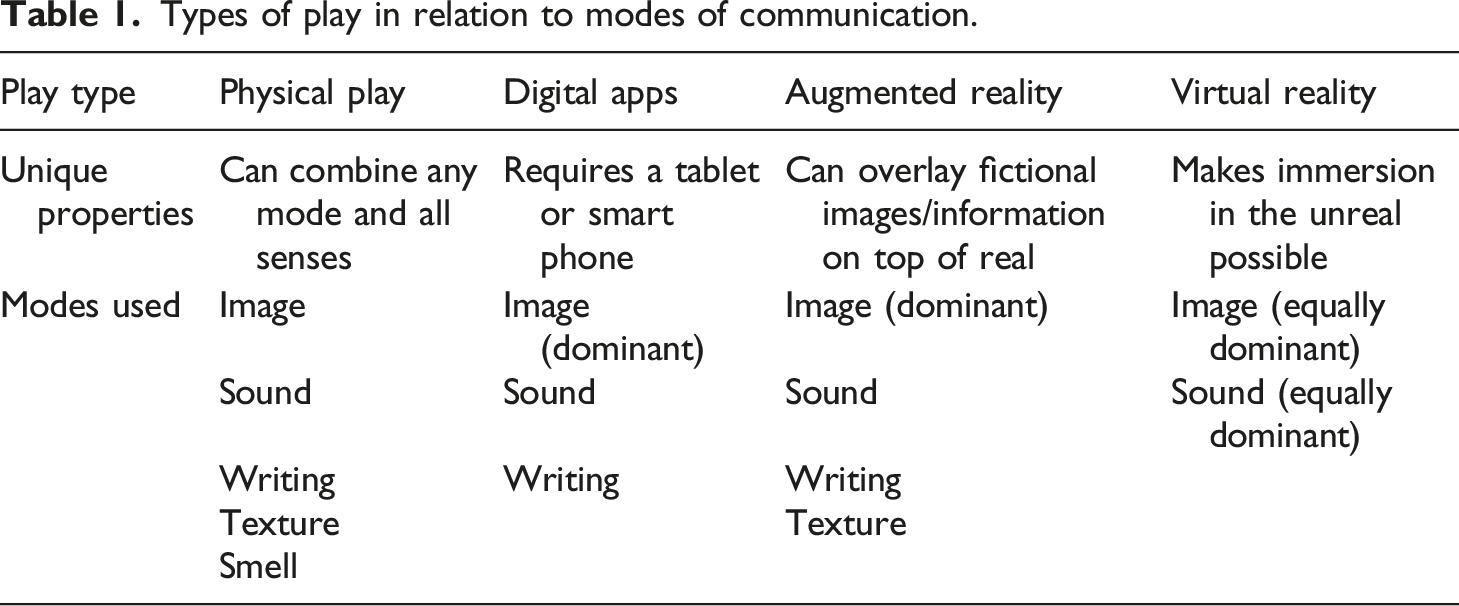
Types of play in relation to modes of communication.
The remainder of this section will show how each of these platforms and their corresponding combinations of modes was incorporated into the play-kit design in order to disseminate particular types of medical information relating to having an MRI scan.
Physical play: the MRI scanner
The analysis of children’s drawings of their preferred types of play showed differences based on age. Specifically, the youngest children, aged 4-5-years-old, were more interested in physical than digital play, which included playing outside; balls, climbing frames, slides and scooters were the most frequently mentioned. They also played traditional games such as hide and seek and expressed a joy of the natural environment. Further, physical toys were described in more detail than digital content. For example, they described their favourite toys such as Pokemon teddy bears, LEGO sets and Power Ranger figurines by name as well as more detailed information about other favourite toys. “Megazoyd- It’s my biggest toy you can fit 6 figures in it.”
By contrast, when they talked about digital play they described their interest in devices, such as ipads and smartphones but were less confident when asked about specific content they liked, suggesting they had less exposure to a range of content and/or ability to critique it.
The data showed that digital play became a more dominant part of children’s lives from five- years-old upwards. In the class of five to 6-year-olds, children continued to describe the physical toys they liked but they also described access to a wider range of digital platforms for play that included Nintendo Switch games consoles, smart phones, tablets and Sony PlayStations. Additionally, this age group were also much more enthused by specific pieces of digital content that they were now able to describe by name and in detail: “Subway Surfers-It is like someone who has a hoverboard. It is too easy. You just have to tap it.”
By the time children had reached 10–11-years-old their interest in physical toys had diminished. When asked about physical play they described sporting activities and clubs they took part in. Girls also mentioned other activities such as drawing and cooking. Instead, 10–11-year-olds articulated what they liked to play across a range of different platforms and devices. Their access to digital platforms had also widened to include Xbox, hand-held devices such as Nintendo DS and Nintendo Switch, as well as laptops and VR headsets. The content children were using also had more sophisticated gaming mechanics and narratives, as is evident in the examples they gave, including FIFA, Fortnite, Rocket League, Overwatch and Mario. Finally, social media also played a role in these children’s lives and they described favourite YouTubers.
This data was important to the design of the play-kit which needs to engage children across the age spectrum of 4-10-years-old. Thus, on a practical level, including physical and digital play would help to span the age range. However, there are other reasons for including a physical play aspect. Firstly, the youngest children did not have access to their own digital devices but they were the age range most likely to be given a General Anaesthetic as a precaution to keep them still in the MRI scanner. Thus, including physical play in the design would increase opportunities for repeat play and give them agency as to when they played. Out of all the medical information that needed to be conveyed, physical play seemed best suited to the look of the scanner. Our partner radiographer told us that getting young children to enter the scanner was the hardest part of the process, and that once inside they were likely to be able to complete a scan. Thus, we matched the most accessible play type to fulfil this need. Our design of a flatpack cardboard kit for children to build into a model toy scanner allows patients to become familiar with the shape and structure of the scanner. Once built, children would also be able to return to the model scanner and play with it more freely than if it was a digital representation. This also responded to the findings that showed how the combination of physical model making in relation to toys and small teddies to be scanned seems to promote imagination, verbalisation and play all of which help to familiarise children with the MRI process. Finally, Yamada-Rice et al. (2020) described ‘how physical making is equally as immersive to younger children as VR’ (p.63).
Augmented Reality play: the radiographer’s role
Augmented Reality (AR) play was used to allow the user to slot a smartphone into the side of the cardboard scanner and take on the role of the radiographer. This decision was taken in relation to the research findings that showed children preferred to see realistic scan imagery rather than illustrations. Children wanted to be completely aware of what the radiographer does in order to feel fully prepared to undertake a scan. In previous work undertaken by one of the authors (Marsh and Yamada-Rice 2017) they reviewed a range of literature on the benefits of AR play on creativity and cognition for young children. The benefits included better retention of educational information (Hinske et al., 2010), a finding also important to the retention of medical information. Another advantage of AR play is that it promotes expression and understanding of emotion and the verbalisation of their play when children see physical toys transformed by a digital add-on (Bai et al., 2015), and that in general augmentation of physical objects with a digital platform enhanced play (Bai et al., 2015).
Virtual reality play: The hospital experience
As Liszio and Masuch (2017) write VR ‘worlds represent completely controllable environments, which can be explored safely and independently of time and place’ (n.p.). Thus, making it a useful play platform for child-participants to undertake a walk through of a hospital in the comfort of their home. We also took the decision to combine the virtual hospital walk through with a series of interactive mini games to help prepare patients. Firstly, we created a game for children to practise staying still that built on ideas that emerged directly from the research findings. Children already told us that they had successful ways of staying still that included “I zoned out and focused on another thing.” Or “I was meditating-thinking of donuts”, so we designed an interactive game in VR that would allow children to focus on butterflies landing on a plant (Figure 8): VR butterflies.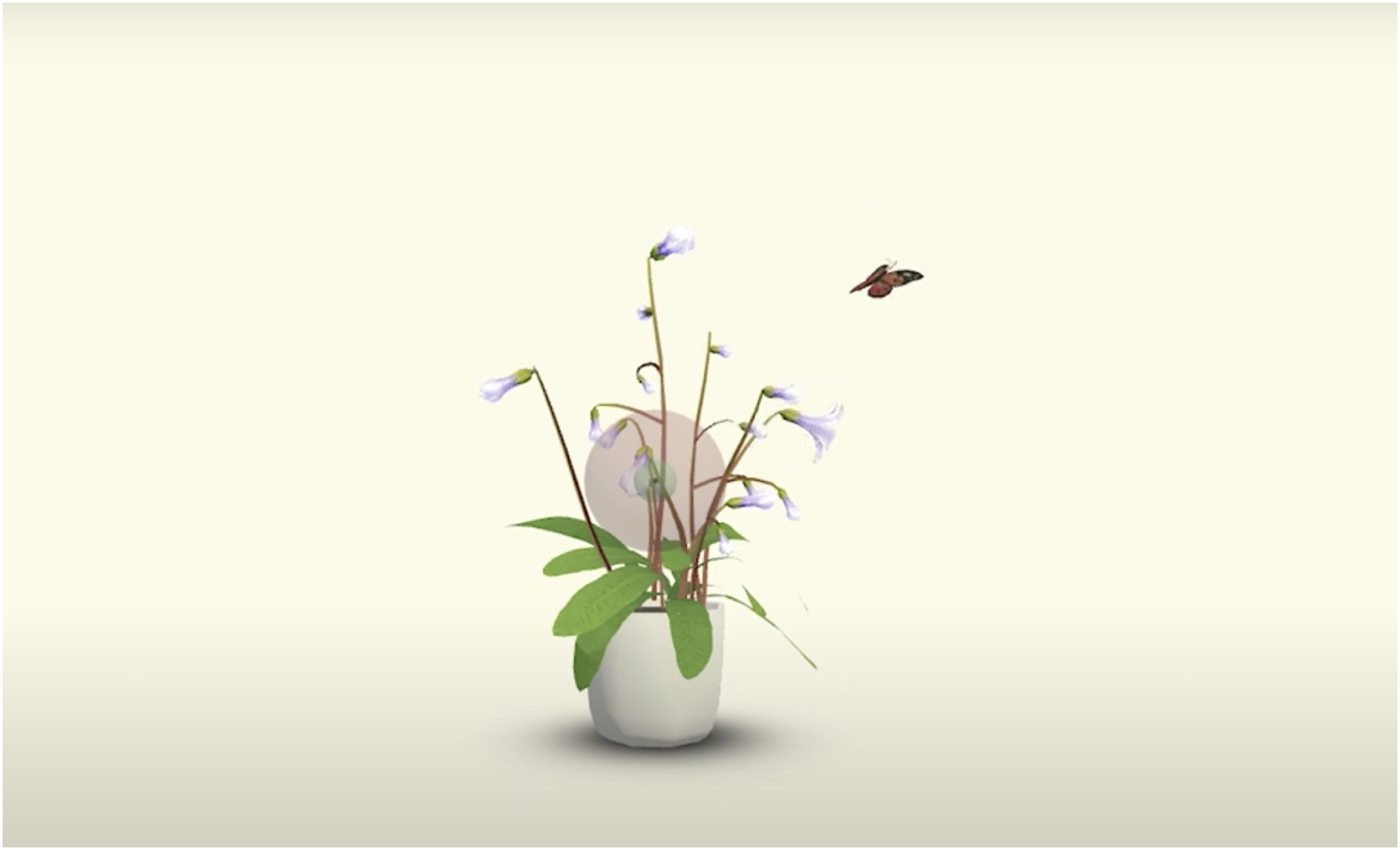
At the same time, we were able to make use of the affordances of inbuilt gyroscopes in smartphones to encourage stillness. The gyroscope, which is able to measure movement, is used to make the virtual butterflies fly away when the child-user does not stay still. Conversely, the insects land on the plant when the user is completely still. Thus, rather than telling children factually that they must be still, this could be practised through game play that used fictional storytelling and principles of mindfulness that research participants told us were useful to them in the co-design research stage.
Also, in the virtual space we created another mini game that allowed children to understand that they would not be able to take metal into the MRI scanner. Again, rather than just providing factual information, we followed children’s interest in combining fact and fiction by asking them to empty their pockets and place any metal items into a tray. This is the same as what happens to patients in hospital. However, we had a fictional twist, in that their pockets contained normal everyday objects children might carry but also included surreal items such as a large dog, a massive diamond ring and a bar of gold (which is not ferromagnetic). These were designed to be playful and we hoped would make users laugh in the same way as they had responded to the unusual being compared to an MRI scanner when exploring our competitor apps, such as the Hoover example outlined above.
These decisions show how play can be defined as an interactive multimodal means for disseminating factual information. In relation to this, it is possible to see how different platforms for play each combine modes differently which in turn will also affect how the medical information is received. This is because ‘interactivity has the potential of increasing enjoyment, and fostering new forms of creativity, social activities and learning’ (Garzotto, 2014: p.5–6).
Conclusion
This article has reported on the first stage of research that led into the development of a mixed realities play-kit to prepare children aged between 4–10-years-olds to have an MRI scan. Specifically, at this stage of the research we sought to understand children’s current favoured types of play and their attitudes to learning about the MRI scan process in order to apply this knowledge to the design of the play-kit. Data were collected using art and design methods such as drawing and model making, alongside observations of children’s play with existing apps about the MRI process. These methods are multimodal by nature and thus fit well with design processes and development which are also multimodal.
The data collected using these multimodal methods and the means of analysis applied to them illustrate how play, storytelling and creativity have a substantial role in how children interacted with medical information. In doing so, the article makes a contribution to the field of child health technology design, which to date appears to prioritise medical information above the child’s desired interaction experience even when such information is disseminated via technologies such as apps which children are more used to consuming in playful ways.
We went on to show how although physical, augmented and virtual reality are all multimodal forms of play, these different types of play do not combine modes in the same way as one another. As a result, our research and development of the play-kit sought to use the unique possibilities for play and storytelling in relation to the affordances of the specific combinations of modes on each platform of play. This was then matched to the specific elements of preparation children needed to complete in order to become familiar with the processes and elements involved in having an MRI scan. Thereby having the best possible chance of completing an MRI without the need for a General Anaesthetic. To this end, we hope the processes we have shared here will be useful to others developing medtech products for young children. Likewise, we hope that showing how we matched multimodal methods as part of research and co-design processes might also be useful to other researchers. Future publication will highlight our project findings from research with patients and the effectiveness of the play kit for medical contexts specifically.
Footnotes
Declaration of conflicting interests
Author Dylan Yamada-Rice is a member of the Editorial Advisory Board of Multimodality & Society. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovate UK (74311 and 104547).
Correction (January 2026):
Author disclosure statements have been updated.