
Abstract
Platelet-rich plasma (PRP) is an autologous blood-derived product utilized nowadays as a treatment for various non-hemostatic, orthopedic, and muscular injuries. Although the exact mechanism of PRP use and effectivity is not yet fully understood, PRP applications are extensively developing and expanding. PRP, as the name implies, contains mostly platelets; thus, platelets are the main players in this therapeutic management for numerous tissue disorders and conditions. Platelets are known to facilitate wound healing and tissue repair through the various growth factors present in their granules. The growth factors in platelets also act on cells found in tissues other than those involved in wound repair, resulting in an increased interest in PRP use as a regenerative therapy for various disorders. In this paper, we discussed platelets and its morphology, and the various growth factors present within the platelet granules. The effects of these growth factors on tissue recovery are highlighted. PRP components, preparation considerations and classifications are presented here to showcase PRP differences and complexity.
Keywords
Introduction
Platelet-rich plasma (PRP) is a form of an autologous biological product utilized as an alternative treatment to various injuries. Platelets, as the main player of PRP treatment, secrete various growth factors, contain phospholipids, and have receptors for plasma proteins necessary for the overall platelets functions.1-3 Platelets which mainly involved in wound healing and tissue repair, 4 abundantly contain the alpha (α)-granules, one of the three types of secretory granules found in platelet cytoplasm. The α -granules contain numerous growth factors such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), insulin-like growth factor 1 (IGF-1), epithelial growth factor (EGF), and transforming growth factor (TGF) that contribute significantly to wound healing and tissue repair. 5
The term “platelet-rich plasma” was coined in the 1970s to refer to a plasma product with a platelet count higher than that of whole blood. 6 While the use of PRP for regenerative purposes has begun in the late 1980s 7 and its popularity has increased ever since, there is still contention among experts as how to truly define “platelet-rich plasma”, as different established PRP preparation protocols result in PRP products that vary in composition and concentration, making standardization of PRP preparation difficult. In this review, we aim to discuss PRP, its composition, and methods of preparation. The studies reviewed in this article were identified through PubMed and Crossref using the syntax search terms: platelets, platelet composition, or platelet structure; growth factors, cytokines; PRP, or PRP applications or PRP preparation; and process of tissue healing.
Growth Factors in Platelets
It is evident that the platelet is essential in maintaining body homeostasis, with its various components contributing to cessation of bleeding. One of its main roles is to promote the regeneration of endothelial tissue when blood vessels are compromised. The platelet, specifically the growth factors found in the α-granules of the platelet, promote mitogenesis and angiogenesis, 8 restoring the affected tissue and ultimately reducing blood loss.
Despite what the review has insinuated up to this point, some of the growth factors released by platelets are also found in other cells, and these act on a more diverse population of cells, not just on endothelial cells. What makes platelets interesting is that the growth factors are self-contained and can be released during circumstances beyond those observed during endothelial injury. Because of this, the growth factors found in platelets may also contribute to the healing and repair of other tissues. Some of these growth factors are described below, with their mechanisms of action and individual actions in tissue repair explained further.
Platelet-Derived Growth Factor
The growth factors in the platelet-derived growth factor (PDGF) family of mitogens, originally discovered in α-granules of platelets but found in many cell types, influence the reproduction and growth of undifferentiated mesenchymal cells. 9 Their main role in wound healing is to promote vascular formation and regeneration, while also affecting the movement of cells to the site of injury. 10 Isoforms of PDGFs can either be a heterodimer or homodimer, depending on the genes that encode for PDGF protein subunits. The common isoforms are PDGF-AA, PDGF-BB, and PDGF-AB, with PDGF-CC and PDGF-DD being recently discovered. 11
PDGFs act as ligands and interact with tyrosine kinase receptors called PDGF receptors (PDGFRs). PDGFRs, when not activated, are monomeric and, as of this publication, can either be of the alpha-type (PDGFRα) or beta-type (PDGFRβ). PDGF-AA, PDGF-BB, PDGF-AB, and PDGF-CC activate PDGFRα), while only PDGF-BB and PDGF-DD activate PDGFRβ. 12 Activation of PDGFRs begins when two PDGF protomers are brought together by PDGFs, forming PDFGR dimers, and the resulting transphosphorylation plays a role in the mediation of cofactor binding and signal transduction by either the PI3 K pathway or the STAT3 pathway.13–15
PDGFs play key roles in the different stages of maturation. During embryonic development, PDGFs stimulate the production of certain progenitor cells, resulting in angiogenesis and the formation of mesenchyme.9 As the organism matures, PDGF results in cell differentiation and tissue remodeling. During wound healing, PDGF acts to promote fibroblast division and increased ECM and collagen formation by fibroblasts and macrophages.16,17
Insulin-Like Growth Factor 1
The insulin-like growth factor 1 (IGF-1) hormone is similar in structure to insulin, one of the main anabolic hormones of the body, and can thus also activate insulin receptors at a reduced affinity.18,19 Although mainly produced by the liver, IGF-1 is also found in platelet α-granules. IGF-1 stimulates cell growth as it is a potent signaling molecule, increasing nutrient uptake of target cells.20,21
IGF-1 can either bind to insulin receptors or its specific receptor, IGF-1 receptor (IGF1R). Like insulin, IGF-1 can also promote the activation of insulin receptors through the phosphorylation of the tyrosine residues, resulting in the activation of the PI3 K pathway.22,23 The mechanism for IGF1R activation is similar to that of the insulin receptor, but insulin receptors are known to be regulators of glucose and lipid metabolism, 14 while IGF1R results in the growth and differentiation of cells. 15
Production of IGF-1 is stimulated by growth hormone. As an anabolic hormone, IGF-1 affects skeletal muscle growth and regeneration by promoting hypertrophy, which is essential in the development of various organs. And also exhibits immunomodulating properties. 16
Transforming Growth Factor beta
Two classes of growth factors belong to the transforming growth factor (TGF) family: TGF-α and TGF-β. While TGF-α, as an epidermal growth factor, is associated with the proliferation of epithelial cells, 17 TGF-β and its subtypes are associated with the differentiation of precursor cells which contribute to embryonic development and tissue regeneration.
As a cytokine, TGF-β is mainly produced and released by immune cells and platelets, and is known to have three isoforms. 18 The most abundant isoform, TGF-β1 is associated with the growth and differentiation of connective tissue, being in high concentrations in cartilage, bone, and skin. TGF-β2 is known to inhibit cell differentiation of interleukin-2 (IL-2) dependent CD4 + and CD8 + naïve T cells by inhibiting the expression of activators. TGF-β3, being highly expressed in the umbilical cord, is a regulator of cellular adhesion and ECM formation, which influences palate and lung development, and enhances epidermal and dermal repair. 19
Epithelial Growth Factor
Human epithelial growth factor (EGF), previously known as urogastrone, was first isolated in murine submaxillary glands but is now known to be found in most tissues and body fluids. Upon binding with its associated receptor on cells, the subsequent increase of tyrosine kinase activity results in increased survivability and production of cells, as well as angiogenesis. 20
EGF is first synthesized as an inactive transmembrane precursor. After being cleaved by an endopeptidase, the resulting soluble form functions as a ligand, which further binds with receptors, resulting in the activation of cell signaling cascades and subsequent response leading to cell development. Due to its concentration in saliva and salivary glands, EGF enhances ECM mineralization of dental pulp found within teeth24,25 by enhancing the differentiation of stem cells. 23 Recombinant human EGF is also used to improve wound healing while reducing scarring.26,27
Vascular Endothelial Growth Factor
The vascular endothelial growth factor (VEGF) family is a collection of growth factors involved in the formation of blood and lymph vessels during embryonic development 28 and as a response to increased demand due to decreased oxygen supply and delivery. 29 VEGFs are specific to receptors found on vascular endothelial cells, inducing tyrosine kinase activity which results in angiogenesis 30 and organ-specific blood vessel maintenance. 31
At least five members of the VEGF family are found in mammals, with VEGF-A being the most potent in promoting vessel formation, migration, and mitosis of endothelial cells. 32 Other members of the VEGF family include VEGF-B, a cardioprotective growth factor that promotes hypertrophy during increased demand; 24 VEGF-C, a potent lymphangiogenic protein; 25 VEGF-D, which acts similar to VEGF-C but have suggested links to lymphatic system adaptation in response to cardiovascular disease; 33 and placental growth factor (PlGF), playing a role in trophoblast differentiation and vessel formation. 26
Platelet-Rich Plasma (PRP)
Due to the abundance of growth factors in platelet α-granules and the self-contained structure of platelets allowing for the induction of a localized action, there is increasing interest in using platelet-based products for regenerative purposes other than acute wound healing. One of these products is platelet-rich plasma or PRP. PRP is an autologous blood product, wherein a patient's whole blood is processed through careful centrifugation, resulting in a plasma with an increased platelet concentration and decreased concentration of red blood cells (RBCs) and white blood cells (WBCs). Unlike platelet concentrate, a similar blood product that is administered intravenously to patients with abnormal bleeding due to decreased platelet count, platelet-rich plasma is used to promote a localized increase of growth factors in the affected area, thereby accelerating tissue healing. This section will discuss the specific composition of PRP, PRP preparation, and PRP classification.
Components of PRP
The American Red Cross defines PRP as a blood product containing greater than or equal to 5.5 × 1010 platelets/50 mL of solution. The final concentration, however, varies depending on the preparation method, as platelet concentrations in PRP are found to range between 2.5 to 8 times higher than that found in whole blood. 27 Because of this, evidence for the optimal concentration of platelets in PRP is lacking and platelet count yields vary greatly among the different published PRP protocols.
The presence of erythrocytes may be detrimental to tissues, as erythrocytes can rupture as a result of immune-mediated mechanisms or during PRP preparation, releasing hemoglobin into the product. Extracellular, or free, hemoglobin increases oxidative stress and could damage tissues. 34 Free hemoglobin may deplete nitric oxide levels, causing vasoconstriction 35 which could decrease blood flow to the site of injury. Hemoglobin release due to hemolysis may damage chondrocytes and synoviocytes by inducing the expression of proteinases that negatively affect cartilage repair. 36 It is therefore imperative that most modern PRP preparations ensure very minimal contamination of erythrocytes.
Another component that may or may not be found in PRP are leukocytes. Also known as white blood cells (WBCs), leukocytes have a diverse set of roles that serve to maintain normal body function. 37 Primarily responding to immunity-related conditions, leukocytes also either release and respond to cytokines that promote various biological processes, including inflammation, 38 and promoting the function of other cell types, 39 including platelets and cells that compose tissue.
Normally, fibers composed of collagen, a major component of the extracellular matrix (ECM) of connective tissue, are arranged in a weave-like network. 40 This mesh-like conformation is important in maintaining the structural integrity and elasticity of the connective tissue, and facilitates other essential physiological processes that occur from and in the ECM. 41 However, fibrosis occurs due to chronic inflammation, which is regulated by leukocytes, resulting in scar tissue. Scar tissue is an inferior arrangement of collagen fibers in a regular, organized structure parallel to the surface. This is not as efficient as regular connective tissue in providing structural integrity, elasticity, and overall homeostasis. 40
An increase in scar formation and a decrease in ECM synthesis indicators were observed when levels of pro-inflammatory cytokines are increased in fibrin scaffolds of PRP that contain leukocytes. 42 During tissue injury, neutrophils are attracted to the site of injury by damage-associated molecular patterns (DAMPs) like DNA, IL-1α, and ATP. 43 Neutrophils then promote local inflammation and apoptosis through the release of cytokines like IL-1 and tumor necrosis factor-alpha (TNF-α), proteases like matrix metalloproteinases (MMPs), and reactive oxygen species (ROS), which primarily serve to clear the area of damaged tissue and infected cells, but may damage healthy tissues when present in excess. 44 The production and release of ROS further promote tissue injury and perpetuate the local inflammatory response. 45
Monocytes and macrophages primarily remove cellular debris and pathogenic substances through phagocytosis, 46 but these are also capable of releasing cytokines like IL-1 and TNF-α. 47 IL-1, which increases leukocyte adhesion factor expression and subsequently promotes diapedesis of cells to the site affected, has different subtypes that can either be proinflammatory or anti-inflammatory. 48 Meanwhile, TNF-α, also being released by other cells, 49 acts on TNF receptor 1 (TNFR1), which leads to the release of pro-inflammatory cytokines, triggering a cascade that results in either tissue repair or further injury. 50 Additionally, macrophage release of TGFβ and an increase in TGFβ receptor expression on fibroblasts, either through Smad or non-Smad pathways, promote the production of fibrotic tissue. 51
The contributions of lymphocytes to fibrosis also vary, with T helper 1 (Th1) cells and T helper 2 (Th2) cells being the most relevant. 52 Th1 cells release IL-10 that regulates inflammatory responses, reduces activation of macrophages and their infiltration to the site of injury, and inhibits activation of pathways that result in cell death. 53 Th2 cells, meanwhile, release IL-4 and IL-13. Overactivation of both IL-4 and IL-13 promotes the IL-4/IL-13 axis, which leads to increased transcription of genes for type I collagen and TGF- β. 54
As a result, most PRP preparations also allow for the recovery of leukocytes due to the regenerative and anti-inflammatory action of certain cytokines. 55 However, leukocytes may also release cytokines that are pro-inflammatory and can promote the proliferation of scar tissue. 56 Because the presence of leukocytes in PRP may positively or negatively affect tissue repair, preparation of PRP and whether or not to include leukocytes depend entirely on the type of injury or condition to be treated. Current evidence shows that PRP with leukocytes demonstrated statistical improvement for tendinopathies and PRP without leukocytes for cartilage pathology like knee osteoarthritis. 57 However, varying results were observed when testing the effectiveness of either for acute muscle injuries. 58
Preparation Considerations
Although the use of PRP as an aid to therapy is increasing worldwide due to its promising results, there is no standardized method of PRP preparation due to the inadequate reporting of PRP preparation procedures. Several tweaks in PRP preparation may result in different compositions and concentrations in the end product. As a result, components of PRP may vary widely, depending on the preparation method used.
One of the regulatory issues that PRP as a product faces is the differences in PRP preparation methods. Although numerous studies on PRP effectiveness and preparation have already been published, the PRP collected may vary widely due to the different conditions and methods used. A review article by Wang enumerated six possible PRP-related factors explaining the conflicting results on the efficacy of PRP treatment for various musculoskeletal conditions. These include the following: 1) type of preparation, 2) platelet concentration, 3) use of activated or non-activated PRP, 4) method of PRP activation, 5) mode of application; and 6) frequency of PRP application during treatment (Wang, 2014). The influence of these PRP-related factors on the effectiveness of the treatment could also be due to the absence of a standardized protocol for PRP preparation and other factors, like the type of condition treated, patient case, and individual response to treatment.
In the pursuit of standardization, there have been numerous attempts to present a methodological approach to ensure a consistent manner of reporting in journal articles on how PRP was prepared. Marx proposed that the prepared PRP should have a minimum of 1,000,000 platelets/uL (Marx, 2001). Chahla et. Al reported heterogenous reports on 1) initial whole blood volume, 2) type of anticoagulant used, 3) equipment used, including centrifuge process ie, spin time, spin rate, and number of spins, 4) activation method used and 5) interval time between PRP processing to injection. 59
The report prepared by Chahla in 2017 emphasizes the ambiguity and heterogeneity of the reviewed PRP preparation protocols. Out of the 105 data sets analyzed, only 17 studies reported PRP composition measurements, while only 11 studies have preparation protocols comprehensive enough for investigators to replicate. The researchers reported an average initial whole blood volume of 60.8 ± 68.9 mL; however, the measured initial whole blood volumes range as low as 8 mL and as high as 450 mL. The average initial platelet concentration was 381 ± 391 × 103/μL, and the average final platelet count of 1473 ± 2211 × 103/μL, an average increase of about 4.7 ± 1.96 times. The average final PRP volume was also reported to be at 6.5 ± 5.5 mL. 60 Despite the obvious disparity in measured initial blood volume among protocols, the effectiveness of the PRP depends on the final concentration of platelets, as a 2020 study reported that the optimum concentration of platelets in PRP to stimulate the proliferation of mesenchymal stem cells was 1500 × 109/μL, with no marked increase in proliferative action beyond 1500 × 109/μL. 61
Because the presence of leukocytes in PRP preparations affects tissue regeneration and repair differently, these are usually classified as either leukocyte-poor (LP, also known as “pure PRP”) or leukocyte-rich (LR). It is therefore essential to identify which type of PRP to use for each condition that could improve the patient's condition and simultaneously minimize adverse effects such as fibrosis. Current evidence based on numerous in vitro studies and clinical trials suggests the therapeutic use of LP-PRP for cartilage pathologies like osteoarthritis, while LR-PRP is recommended for tendinopathies.62,63 The effects of leukocytes on the recovery of muscle injury are yet to be fully understood. While a 2018 meta-analysis of six studies on PRP use for muscle injuries reported a significantly shorter time to return to sport, this also reported a non-significant difference in re-injury rate. 64 Further research on the effect of PRP, including the presence of leukocytes in PRP, in promoting muscle recovery is needed.
The type of anticoagulant is an important factor in preparing PRP, as it can also influence its regenerative effect. Earlier preparations of PRP utilized citrate-based anticoagulants because a known blood unit used to mitigate serious bleeding incidents, that is the platelet concentrate, is prepared using this anticoagulant. If the intent of PRP preparation is solely to increase platelet yield, ethylenediaminetetraacetic acid (EDTA) is the most effective, but this effect is only monitored in vitro; EDTA is not used by current PRP preparation kits available.65,66. However, platelet yield, platelet function, and growth factor release also affect PRP quality and effectiveness. An in vitro study in 2016 compared the effects of PRP with either sodium citrate (SC), acid citrate dextrose (ACD), or EDTA, on mesenchymal stromal cells (MSCs). Although platelet counts were higher in PRP with EDTA, the average platelet recovery of SC was 5.06% higher than of EDTA. 65 However, another study, EDTA provided higher superiority in terms of obtaining higher platelet recovery with preserved functionality. 66 Despite this result, most studies will not recommend the use of EDTA due to its potential harm to platelet membrane. 65 Studies have shown that EDTA anti-coagulated blood samples showed increased expression of platelet activation markers P-selectin (CD62p) and granulophysin (CD63), which potentially causes spontaneous platelet activation aside from affecting membrane fluidity and glycoprotein structure. 67 Note that most studies were done in vitro, and the impact of the anticoagulant in the body was not well studied, probably, because the concentration of these will be too minimal when compared to the body's total blood volume. Also, citrate is an already accepted anticoagulant for a blood product used for transfusion, and EDTA is a known medication in the management of heavy metal poisoning.62,68
Platelets in EDTA were also observed to have an increase in mean platelet volume compared to SC and ACD. TGF-β1 was found in higher concentrations in PRP with SC (48,559.10 ± 12,839.86 pg/mL), while the most amount of VEGF was released from PRP with ACD (362.70 ± 77.95 pg/mL). 65 In 2020, a comparative study between pure PRP and resulting PRP releasate (PRPr) obtained with SC and ACD demonstrated that a ½ ACD preparation yielded the most PDGF (32,445 ± 1598 pg/mL). However, the same study also assessed PRPr-mediated regeneration in wounds in mice. Only tissues treated with ACD PRPr exhibited delayed granular tissue formation and an increase in WBC infiltrates, indicative of inflammation. 63
It is worth noting that a product similar to PRP is also being applied as a regenerative biotherapy. Platelet-rich fibrin (PRF) is considered a second-generation PRP product rich in platelets and also promotes the release of growth factors; however, PRF does not contain an anticoagulant, and the formation of a fibrin clot matrix rich in leukocytes and platelets is promoted. 69 The resulting clot prevents PRF from being injected, so the mass is applied directly at the injury site. The applied fibrin matrix acts as a physical scaffold for tissue regeneration, and a slower rate of degradation of embedded formed elements and bioactive compounds is observed, resulting in a delayed but sustained release of growth factors for up to 7 days. 70 PRF is being used extensively in dentistry, and its potential use for other conditions is being explored.
Although numerous studies show that double centrifugation results in increased platelet and growth factor concentration, both the speed and time of centrifugation for both instances vary among published findings. The findings of Kececi et al show that after initial centrifugation of whole blood at 250 x g for 10 min, variations in the speed of the second spin led to an observable increase in platelet concentration. When compared to basal values, platelet concentrations increase by a factor of 2.16 at a speed of 500 x g, 2.80 at a speed of 750 x g, and 3.48 at a speed of 1000 x g. 71
The speed of centrifugation (expressed in revolutions per minute, or RPM) and the relative centrifugal force (RCF, expressed in x g) also influence both platelet count and morphology, and removing other components of plasma such as the neutrophils and buffy coat. Although either RPM or RCF is reported in PRP preparation protocols, it is important to note that RPM is not the same as RCF. This is because RCF is a measure of force, and is, therefore, a derived measurement. RCF is dependent on both RPM and radius of rotation, 72 When developing PRP preparation protocols, it is important to manually compute the RCF if the centrifuge used does not automatically measure it, as it allows for better replicability regardless of centrifuge models used. As a result, when discussing centrifugation, the RCF should be commonly reported alongside RPM.
Increased speed of centrifugation may be useful in increasing the recovery of more platelet, thus increasing platelet concentrations; however, it may result in shear stress due to increased RCF, affecting the quality of platelets recovered. 73 Shear stress may also cause early activation of platelets, as a 2014 study showed an increase in platelet activation due to centrifugation at 800 x g and 1200 x g (Perez et al, 2014). The researchers then suggest performing a first spin at 100 x g (as a decrease in platelet concentration was observed at speeds above 190 x g) and a second spin at 400 x g, each for 10 min. The first spin separates the red blood cells; the second spin (including only the plasma) will concentrate the platelets and allow the removal of the other plasma components. 74 The idea of platelet activation via increased centrifugation speeds was supported two years later, as an increased expression of P-selectin was observed after centrifuging PRP for 10 min at 2000 x g (citrated plasma = 43% increase; EDTA plasma = 56%). 75 A study performed in 2017 suggests that a first spin at 160 x g for 10 min followed by a 250 x g spin for 15 min resulted in the optimum concentration of platelets and growth factors. 76
There is also increased interest in the difference in effectiveness between activated PRP and inactivated PRP. Activated PRP is defined as PRP that has been activated ex vivo, before injection, while inactivated PRP relies on activation in vivo, thereby having no additives. Activation factors that could be added to prepared PRP include thrombin, calcium chloride, a combination of calcium chloride and thrombin, and type 1 collagen. A study done by Lee et al in 2013 showed a nonsignificant increase of PDGF in activated PRP as compared to inactivated PRP. 77 Another study in 2016 showed that when PRP is activated with either thrombin, calcium chloride plus thrombin, or collagen type I, an immediate release of PDGF and TGF-β1 was observed, and the levels of these growth factors remained stable over time. 78
Temperature is also a key variable in PRP preparation, as platelets subjected to different temperatures may influence platelet function variably. The American Association of Blood Banking (AABB) recommends a temperature ranging between 20 °C-24 °C for PRP preparation. 79 However, the dynamics between temperature and other variables like the number of centrifugation processes, centrifugation speed, and platelet activation have yet to be fully understood, as these interactions may affect the overall effectiveness of PRP. Previous research has suggested improvements in PRP preparation by subjecting it to different temperatures, like increased platelet yield at around 12 °C-18 °C, 80 a rewarming step done at 37 °C for additive-free platelet activation, 81 or a 4 °C pre-incubation resulting in increased angiogenic properties. 82
The 2017 review performed by Chahla et al reported only 27 studies that discussed interval time between PRP processing and administration, with a mean interval time of 14 ± 33 h. 60 The efficacy of PRP is dependent on the interval time between preparation and administration, as growth factor release and concentration are affected by time. In-room temperature conditions, a steady release of PDGF-AA and VEGF were reported throughout the 7 days of storage. IGF-1 levels saw a slight but gradual increase on day 7, while FGF-B levels saw a gradual decrease after 24 h of storage. What is interesting is that TGF-β1 levels saw a slight decrease in concentration 24 h after storage, followed by a gradual increase as storage was prolonged. 83 It is therefore beneficial to administer the PRP as soon as possible to ensure that the optimal growth factors are delivered to the site of injury.
Classifications of PRP
Because of the variations in PRP preparation methods among different publications, different classifications for different PRP formulations have been proposed. One of the first PRP classification systems were proposed by Dohan Ehrenfest, Rasmusson, and Albrektsson in 2009, and is commonly used (Table 1). Their classification was based on the commercially available PRP preparation kits at the time. The following parameters were considered: preparation kits and centrifuge, platelets and leukocytes, and fibrin. While the subparameters (like cost and duration of procedure) may vary among PRP preparation protocols, the platelet concentrations for all three categories should be >80% of the initial platelet count in whole blood. However, the concentration of leukocytes varies widely from <40% to 80%, which can be influenced by the initial leukocyte concentration in whole blood. 84
PRP Classification System Used to Define Leukocyte-Rich Platelet-Rich Fibrin (LR-PRF), Leukocyte-Rich Platelet-Rich Plasma (LR-PRP), and Leukocyte-Poor-Platelet Rich Plasma (LP-PRP).

This classification system was used to define PRP into three general categories: leukocyte-rich platelet-rich fibrin (LR-PRF), leukocyte-rich platelet-rich plasma (LR-PRP), and leukocyte-poor-platelet rich plasma (LP-PRP). LR-PRP should have a minimum of 40–80% of leukocytes collected, while LP-PRP should have less than 40% of leukocytes present. LR-PRF should have a high density of fibrinogen as well as a minimum of 40–80% leukocytes present.
In 2012, DeLong, Russell, and Mazzocca suggested the PAW (platelet, activation, WBCs) classification, which is based on the concentration of platelets, the method of activation, and the presence of white blood cells in PRP. 85 The PAW system is shown in Table 2. Platelet concentration in PRP are relative to the baseline concentrations in whole blood. For the activation method, the letter “x” is added when PRP is activated exogenously, like when an additive is added, while there is no designation when platelets in PRP are not activated. White blood cell concentration in platelets is based on the total WBCs and neutrophils present. Total WBC count can either be classified as A (above baseline) or B (below or equal to baseline), while neutrophil concentration can either be α (above baseline) or β (below or equal to baseline).
The PAW Classification System.

In the same year, Mishra et al (2012) proposed a similar classification to the PAW classification (Table 3). However, their classification, called the “Sports Medicine Platelet Rich Plasma Classification System”, also defines their parameters differently based on whether or not the PRP has a considerable increase or decrease from baseline platelet and WBC levels, and whether or not an exogenous activator is introduced. 86
The Sports Medicine Platelet Rich Plasma Classification System.

The previous three classifications were determined to have deficiencies, as these do not consider the final volume of the product, the proportion of formed elements relative to the final volume of the product, and the presence of other formed elements, like RBCs. Because RBCs may be toxic to cartilage tissue and could promote inflammation, a 2015 paper by Mautner et al recommend reporting the presence or absence of RBCs when preparing PRP (Table 4). As a result, the PLRA (platelet, leukocyte, RBC, activation) classification was proposed. 87 Platelet parameters should be based on the actual platelet concentration, the injected volume of PRP, and the total number of platelets delivered. WBC parameters are defined by the presence and absence of WBCs. The percentage of neutrophils should also be reported, as neutrophils may increase inflammation and contain hydrolytic enzymes, both of which could inhibit proper healing. Similarly, the presence and absence of RBCs are also reported. Lastly, the use of activators should also be reported, and the type of activator should be described.
The PLRA Classification System.

The DEPA (dosage, efficiency, purity, activation) classification, proposed by Magalon et al in 2016, introduced two new concepts that were absent from previous classifications: the efficiency of PRP production and the purity of PRP (Table 5). 88 Platelet dosage is based on the number of platelet times the volume of PRP injected to the injury site. The efficiency of platelet recovery is based on the percentage of platelets recovered compared to the baseline levels measured in whole blood. The purity of PRP is the percentage of platelets in relation to other formed elements, like WBCs and RBCs. PRP activation is also reported as being present or absent, similar to previous classifications.
The DEPA Classification System.

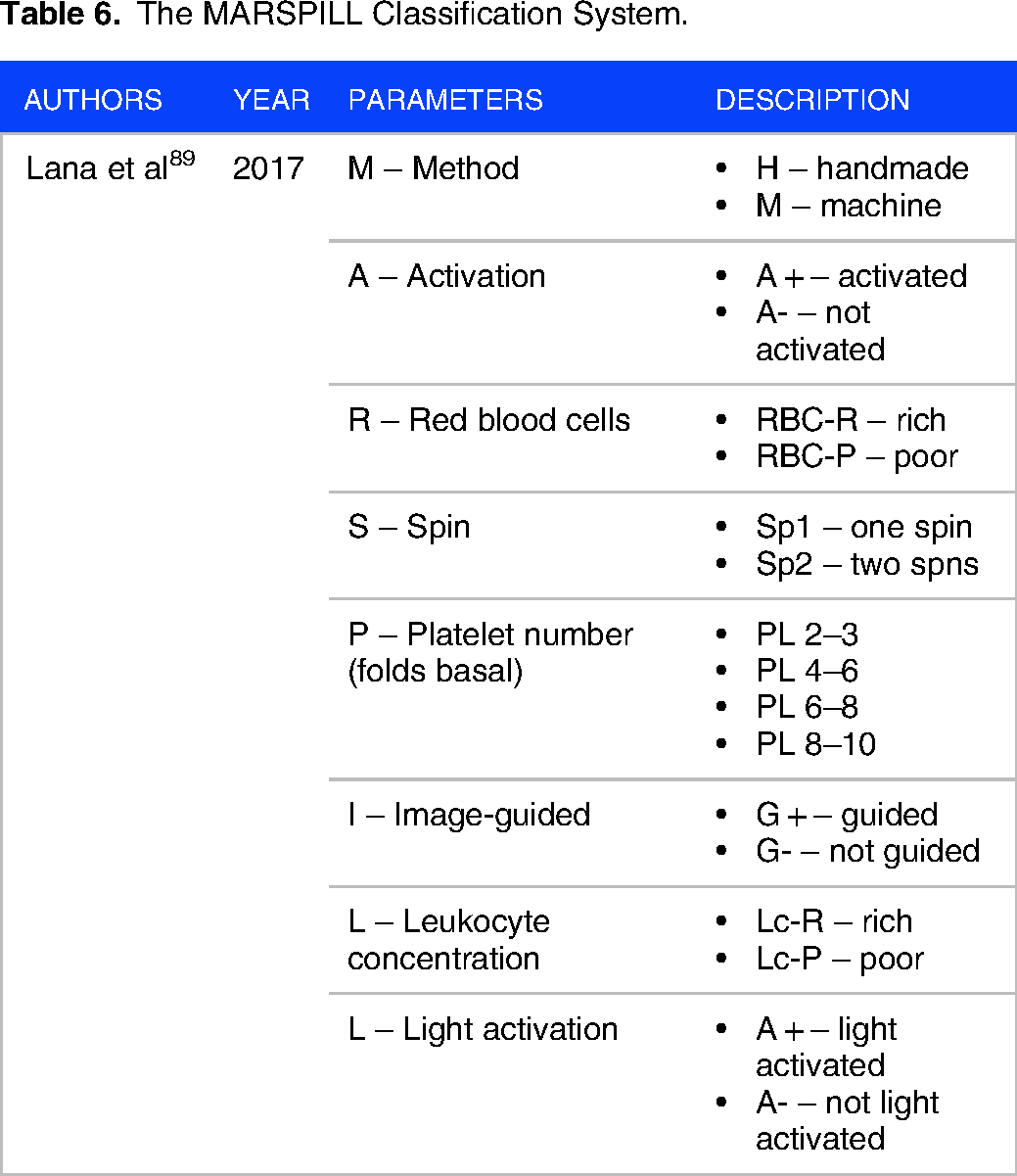
The MARSPILL classification (Table 6), proposed by Lana et al in 2017, improved on the established criteria by adding four new parameters. 89 The first parameter added pertains to whether or not the PRP was prepared manually or using an automated machine. The second parameter involves reporting the number of spins, since newer PRP preparation protocols may involve a second centrifugation step. The third parameter involves the use of ultrasound to guide the delivery of PRP to the injury site. The final parameter added describes light activation, as photoactivation of bioactive cells may influence their actions.
The MARSPILL Classification System.
In 2018, the Platelet Physiology Subcommittee of the Scientific and Standardization Committee (SSC) of the International Society on Thrombosis and Haemostasis (ISTH) introduced a new system that streamlines PRP classification, as seen in Table 7. 90 Using the RAND method to assess the scientific evidence present relating to PRP preparation, the classification system considers newer activation techniques like freeze-thaw activation, and specifies the PRP produced based on the principle used to prepare the PRP. However, image-guided PRP delivery and light activation are not reported.
The ISTH SSC Classification System.

Further streamlining PRP classification methods, Kon et al, in collaboration with previous experts on PRP classification like Mishra and Magalon, developed an entirely new code system. 91 This new code system, as shown in Table 8, consists of 6 digits grouped in pairs that correspond to the following parameters: platelet composition, purity, and activation. The first pair denotes platelet composition, indicating basal platelet concentration in blood and platelet concentration in PRP. The second pair reports the presence of RBCs and WBCs in PRP. The third pairing indicates whether or not the PRP was activated, and if calcium-based activators like calcium chloride were used instead of other activators like thrombin or type I collagen.
The PRP Preparation Classification Coding System.

Conclusion
Platelet-based biotherapies are promising approaches to promote and enhance tissue repair, as both platelet composition and mechanisms of action during activation result in a multipotential effect on a plethora of tissue types. Because of this, the use of PRP in particular is already being adopted for the management of conditions in tissues other than endothelial tissue. Its ease of preparation and use also lends to its ever-increasing popularity as a treatment method.
Further research has uncovered several factors that add to the complexity of PRP preparation. The dynamics between the other formed elements in blood and platelets, as well as how the presence of these affects tissue repair, should be considered. The conditions during PRP preparation may also affect platelet function, which could influence its regenerative effect. The variability that may arise due to the aforementioned factors led to the development of different preparation procedures for PRP, which hinder its standardization. Due to the complexity of preparation and composition resulting in varying effects, further research on the applicability of PRP to other conditions may be warranted, as well as more clinical studies.
Footnotes
Acknowledgements
The authors would like to thank the Department of Science and Technology—Philippine Council for Health Research and Development for the support given to the research program, without which the authorship of this article would be difficult.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Availability of Data and Materials
Not applicable.
Consent for Publication
Not applicable.
Ethical Approval and Consent to Participate
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is part of a research program entitled “Research Center for the Rehabilitation/Sports Medicine (Oplan Atletang Pinoy)”, funded by the Department of Science and Technology—Philippine Council for Health Research and Development (Ref. No. 001911).