
Abstract

The use of individual patient pharmacokinetic (PK) data to inform prophylaxis dose and dosing frequency has the potential to help optimize care for people with hemophilia A, by ensuring each patient achieves a predetermined FVIII trough level and protection from bleeding. The NuPreviq study evaluated the safety and efficacy of PK-guided personalized prophylaxis with Nuwiq® (simoctocog alfa), a 4th generation recombinant FVIII product produced in a human cell-line without chemical modification or protein fusion, in 66 previously treated adults with severe hemophilia A.1-3
Following a 1- to 3-month standard prophylaxis phase (30-40 international units [IU] kg-1 every other day or 3 times per week), patients in the NuPreviq study received personalized prophylaxis for a mean of 6.2 months. As previously reported, 73.8% of patients remained bleed free and 83.1% were free from spontaneous bleeds during personalized prophylaxis with Nuwiq®. 2
Based on the PK analysis, 44 (66.7%) of the 66 patients in the NuPreviq study changed to a different regimen, while 22 (33.3%) remained on the same dosing regimen. Of the 44 patients who changed prophylaxis regimen in the study, 40 (90.9%) completed the personalized prophylaxis phase of the study according to the assigned dosing and treatment scheme. To assess the impact of adjusting prophylactic dosing with Nuwiq® based on PK assessment, we performed a post hoc analysis of these 40 patients who adhered to the assigned dosing and treatment scheme.
The dosing frequency was decreased after PK assessment for 39 of the 40 patients, and 34 (85%) were treated twice weekly or less. The dosing frequency was increased in 1 patient from 3 times per week to every other day, but with a decrease in weekly dose from 100.2 to 85.4 IU/kg. The 40 patients remained on the assigned dosing regimen for a median of 5.8 months.
Whilst being treated with the assigned regimen, 33 (82.5%) of the 40 patients did not experience any bleeds and 36 (90.0%) had no spontaneous bleeds. The mean (SD) annualized bleeding rate (ABR) during this period was 1.2 (3.9) (median 0) for all bleeds and 0.94 (3.76) (median 0) for spontaneous bleeds. Figure 1 shows the mean ABR for all bleeds and spontaneous bleeds by dosing interval. The mean (SD) dose of Nuwiq® was 52.5 (12.2) IU/kg/injection and 99.7 (25.6) IU/kg/week. FVIII doses per week by dosing interval are shown in Figure 2.
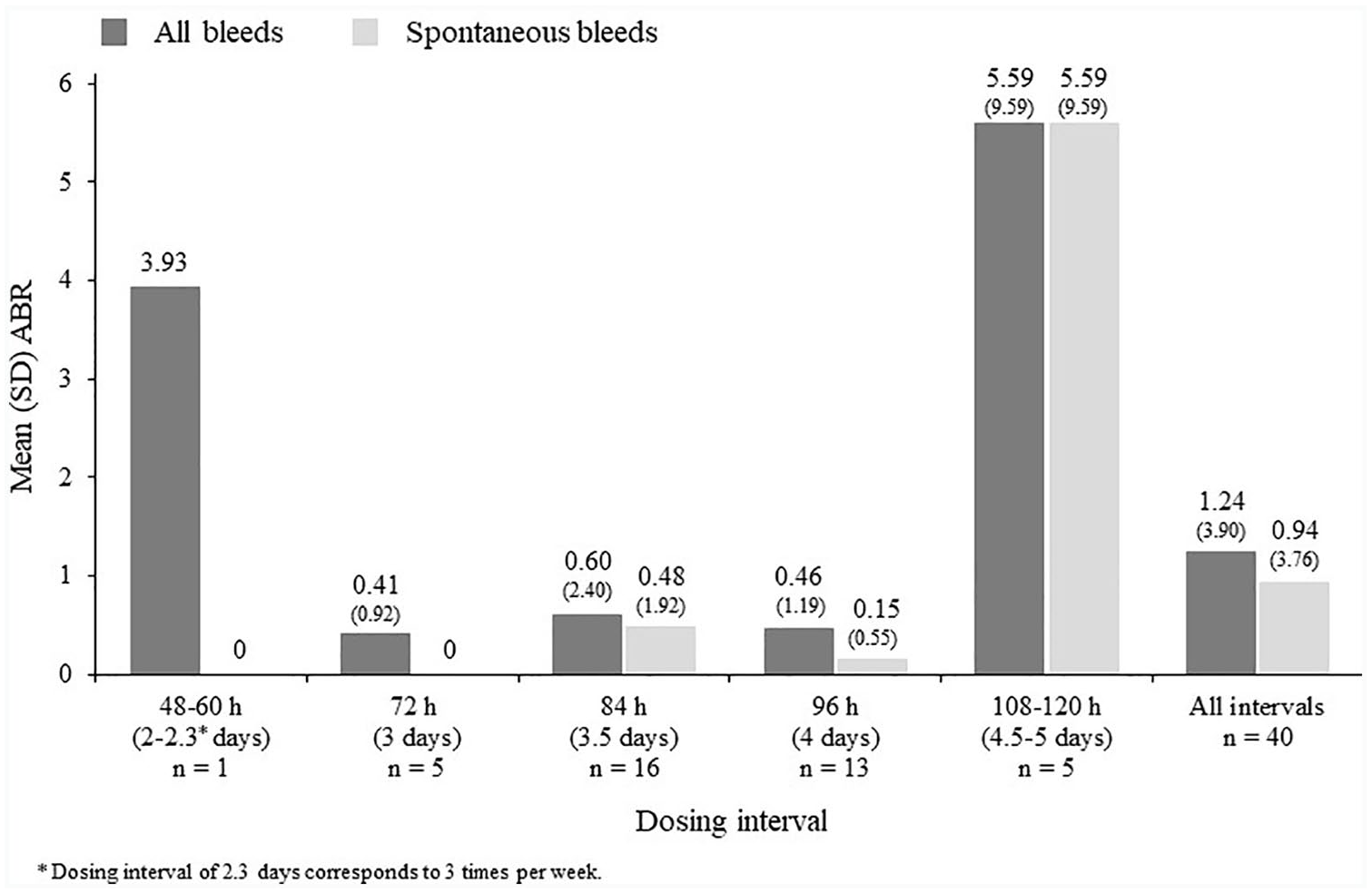
ABR for all bleeds and spontaneous bleeds by dosing interval during prophylaxis with the assigned regimen after PK assessment.

Actual dose of Nuwiq® per week and per infusion by dosing interval during prophylaxis with the assigned regimen after PK assessment.
There are no direct head-to-head comparisons of the efficacy of bleed prevention between rFVIII products. Indirect comparisons are made difficult by differences in patient populations, study methodologies, durations of follow-up, and dosing regimens. In this analysis, 82.5% of patients had no bleeds during treatment on the assigned regimen and the mean ABR was 1.2 for all bleeds. In studies of other rFVIII products, the percentage of patients with no bleeds was 39% to 45% over a period of approximately 6 to 8 months4-9 and ABRs ranged from 2.9 to 3.75-10 although these studies did not report data for adherent patients only.
In conclusion, personalized prophylaxis may allow many patients with hemophilia A to achieve effective bleed protection with a lower treatment burden than with standard prophylaxis protocols. Our analysis demonstrates that PK-guided personalized prophylaxis with Nuwiq® is effective in patients able to adhere to their assigned regimen and supports the use of PK assessment to inform prophylactic dosing regimens in patients treated with Nuwiq®.