
Abstract
Background:
Esophageal visualization is an important aspect of the Modified Barium Swallow Study (MBSS). Sequential swallows have an impact on esophageal clearance; however, standard cueing for esophageal clearance does not limit the number of times a patient swallows. We aimed to determine the potential impact of providing additional verbal cues related to the number of times to swallow on impressions of esophageal clearance during the MBSS.
Methods:
Standard of care MBSS were performed using the Modified Barium Swallow Impairment Profile (MBSImP). In the standard MBSImP condition, participants were instructed to “swallow when you’re ready.” Whereas, in the experimental condition, participants were instructed to “only swallow one time.” We report a combination of MBSImP component 17 scores (esophageal clearance) for both conditions. We performed tests of association and determine if statistically significant associations exist between MBSImP component 17 scores under two conditions.
Results:
Thirty-six participants qualified for this study. Esophageal clearance scores changed in 14 (38.9%) of participants when comparing between the two conditions. For participants with score change, 57.1% had an increase (more altered clearance) and 42.9% had a decrease (more typical clearance) in scores. A significant association was identified for esophageal clearance (component 17) scores in the standard versus experimental conditions (P < 0.0001).
Conclusion:
Impressions of esophageal clearance (component 17) changed in 38.9% of participants in the experimental condition, with over half of those whose score changed indicating more atypical esophageal clearance. Our results illuminate the need for further study into the contexts in which impressions of esophageal clearance during the MBSS are made.
Introduction
The Modified Barium Swallow (MBSS) study is an important exam for the assessment of swallow function. The MBSS study traditionally involves examination of the swallowing continuum (eg, oral cavity, pharynx, and esophagus) with various liquid viscosities and food textures with the patient seated or standing unless positioning techniques are being trialed. 1
Historic expert opinion and early work identified interrelationships between aspects of the swallowing continuum, oropharyngeal and esophageal, as early as 1985.2 -4 More recently, the scientific evidence which supports incorporating esophageal visualization into standard MBSS practice continues to grow.5 -11 However, practices relating to the fluoroscopic imaging of the oropharynx/pharynx and esophagus vary significantly in the literature.2 -4,6,10 -21
Non-diagnostic visualization of the esophagus falls within the scope of practice for speech-language pathologists (SLP) according to the American Speech-Language Hearing Association (ASHA).22 -24 The American College of Radiology (ACR) states that the assessment of esophageal clearance falls within the scope of the MBSS, whereas diagnostic assessment of the esophagus falls to other radiographic studies (eg, esophagram). 25 Both Watts et al 11 and Miles et al 19 demonstrated that SLPs are capable of learning esophageal physiology and demonstrated their ability to identify abnormal esophageal bolus transit and need for further assessment (eg, Gastroenterology [GI] referral).11,19 Non-diagnostic esophageal visualization during an MBSS is well-supported.5,8 -11,16 -18,20,26,27 While several standardized MBSS protocols exist, currently, the MBSImP is the only standardized, validated, and reliable protocol and scoring system that assess the physiology of swallowing components across all domains (oral, pharyngeal) for the MBSS and includes an esophageal visualization component. 18 The MBSImP identifies the 17 physiologic components of swallowing, including the determination of esophageal clearance (component 17) in the upright position. 18 For the judgement of esophageal clearance, the MBSImP protocol includes two swallows in the anterior-posterior plane with 5 mL of nectar-thick Varibar® (barium sulfate) and 5 mL pudding Varibar. Per the standard MBSImP protocol, the patient is instructed to perform an oral bolus hold and then to “swallow when you’re ready.” 28 The bolus is then followed through the esophagogastric junction (EGJ) and bolus clearance though the esophageal body is judged. MBSImP component 17 (esophageal clearance) score has five possible scores: 0, or “complete clearance; esophageal coating,” 1, or “esophageal retention,” 2, or “esophageal retention without retrograde flow through the pharyngoesophageal segment (PES),” 3, or “esophageal retention with retrograde flow through [the] PES,” and 4, “minimal to no esophageal clearance.” Though esophageal visualization is non-diagnostic, scores are considered hierarchical. In the MBSImP protocol, the patient receives no other instruction other than to hold the bolus in the oral cavity until directed to “swallow when ready.”29 -35
During swallowing, a bolus is propelled through the oropharynx and into the esophagus. Once in the esophageal body, the swallowed bolus is propelled by primary peristalsis where pressure is applied to the tail of the bolus as it moves through the length of the cervical and thoracic esophagus. 32 Once the bolus is in the most distal esophagus it moves through the open LES through the esophagogastric junction (EGJ) and into the gastric cardia. Primary peristalsis is only initiated with a bolus that passes through the upper esophageal sphincter (UES). If this first wave is ineffective at clearing the bolus, a secondary peristaltic wave should be initiated to help clear the bolus through the EGJ. Non-propulsatile contractions of the esophagus are referred to as “tertiary contractions” if seen radiographically. These incomplete contractions may be consistent with ineffective esophageal motility (IEM) if certain manometric thresholds are met. 36 Though, weak, or failed swallows can occur in healthy normal patients. Per the Chicago Classification v4.0 for high-resolution esophageal manometry (HRM), it is normal to have up to 30% of swallows that are weak or “failed.” 36 However, there is some evidence to suggest that this is much higher in some healthy normal adults.37,38 Deglutitive inhibition is a normal phenomenon resulting in the cessation or alteration of peristalsis in the case of “dry” swallows or rapid drinking.29 -35 Meyer et al 33 identified 20 to 30 seconds as the time that it takes for the distal esophagus to “recover.” Importantly, not all swallows which follow less than 20 to 30 seconds after an initial swallow will result in inhibition, but rather an attenuation.33 -35 If only two oropharyngeal swallows occur, there may be no significant esophageal consequence (inhibition or alteration of peristalsis) in healthy adults. 38
Patients with dysphagia, particularly if oropharyngeal in nature, may elicit multiple swallows for a single bolus.39 -42 Patients without identifiable oropharyngeal pathophysiology who report oropharyngeal symptoms (eg, globus) may also elicit multiple swallows per bolus. Because oropharyngeal and esophageal physiology swallowing are interrelated—primary peristalsis can only be initiated by a bolus that passes the esophageal sphincter (eg, a swallow originated in the mouth); thus, the influence of multiple swallows on impressions of esophageal clearance is unknown. Therefore, we sought to investigate the influence of a cueing for single swallows on impressions of upright esophageal clearance during the MBSS. We hypothesized specific cueing, to swallow only once, would eliminate multiple swallows, and thus would result in a different determination of esophageal clearance compared to an un-cued condition for participants who swallow more than once per bolus.
Methods
Study Design
Between April 1, 2021 and July 15, 2021, participants were recruited from the Medical University of South Carolina (MUSC) speech-language pathology (SLP) clinics where MBSS are performed. Informed consent procedures were completed within all ethical standards and written consent was obtained prior to participation in study procedures. This study was approved by the MUSC Institutional Review Board (IRB) (Pro 00106650).
Inclusion and Exclusion Criteria
Inclusion criteria were established to include adults (18+ years) who were referred for an outpatient MBSS for an assessment of swallowing function as a standard of care. Those participants with any past medical history for altered oral, pharyngeal, and/or esophageal anatomy (eg, tongue resection, laryngectomy, or fundoplication) were excluded. Participants who were unable to follow or execute the instructions for the experimental (cued) condition were excluded.
All eligible participants had a Modified Barium Swallow Study (MBSS) using the MBS Impairment Profile (MBSImP™©) protocol and scoring system. 18 Participants whose MBSS reports did not include any MBSImP scores or lacked an MBSImP component 17 (esophageal clearance) score under both conditions were excluded.
Modified Barium Swallow Study
All participants were referred for an MBSS as part of the standard of care for patients with complaints of, or concerns for, dysphagia. MBSS were performed at 30 pulses per second (pps) and were recorded at 30 frames per second (fps) according to best practices.43,44 All MBSS were conducted using the Modified Barium Swallow Impairment Profile (MBSImP™©) 18 protocol and scoring metric which measures 17 distinct physiologic components of swallowing. The core protocol uses 12 swallows across varying liquid and solid consistencies, the initial 10 in the lateral view, the last 2 in the anterior-posterior view. The standard MBSImP component 17, our outcome measure, is determined by the esophageal bolus clearance patterns through the esophageal body and lower esophageal sphincter (LES) in the A-P view with 5 mL nectar and 5 mL pudding contrast Varibar® (Bracco Diagnostics Inc.). Per the standard MBSImP protocol, the patient is instructed to “Hold this in your mouth until I ask you to swallow,” and then, to “swallow when you’re ready.” 28 In the experimental condition, the participant was prompted by the clinician saying, “For these next two swallows I want you to swallow only one time.” For each bolus provision the participant was instructed to hold the bolus in their mouths until directed to “swallow once and only once, then keep your mouth open and focus on your breathing and don’t swallow again.” A period of 30 seconds was provided between the 5 mL nectar and 5 mL pudding boluses in the experimental condition. The standardized score was recorded in the MBSImP database and in the electronic health record (EHR), and the experimental score was recorded only in the MBSS EHR documentation and separately from other MBSImP scores. One-third of the studies were re-rated by the first and senior authors for reliability. Any discrepancies in scoring were rated by consensus between these two authors. If unable to reach a consensus, a third author was tasked with rating the swallow.
Statistical Analysis
Analysis was performed using SAS (v9.4, Cary, NC). Summary statistics were calculated for all variables collected (mean, median, the standard deviation for continuous variables and frequency, median, and mode for categorical variables). Our statistical hypothesis (H0) was that there would be no statistically significant differences in MBSImP component 17 (esophageal clearance) scores in un-cued (standard MBSImP) versus cued (experimental) conditions. Fisher’s exact tests were used to describe categorical variables (eg, MBSImP component 17 scores) and determine if associations exist between scores in the two conditions (standard versus experimental). Our hypothesis was that there were no statistically significant associations. Mann-Whitney U/Wilcoxon Rank Sum tests were used to describe continuous variables (eg, age) Chi-Square or Fisher’s Exact tests were used to describe categorical variables. Findings reflect the overall statistical significance and for all statistical analyses, the alpha was set at 0.05 with P values of ≤0.05 indicating statistical significance.
Results
Participants
A total of 36 participants met study inclusion criteria. The average age of participants was 64 years (range 33-94). The majority (55.6%) of participants were female. Most participants were white (83.3%), and none identified as Hispanic. Most of the participants were referred by Laryngology (52.9%), followed by Primary Care (17.7%). While only 27.8% of participants’ medical records included a diagnosis of gastroesophageal reflux disease (GERD), 61.1% of participants were on a proton pump inhibitor (PPI) (eg, omeprazole) and 33.3% were on an H2-receptor antagonist (eg, famotidine). Of these patients, 9/25 (36%) were on both a PPI and an H2-receptor antagonist. Only 11/36 (30.6%) participants were not prescribed either medication. The most common participant-reported symptom was dysphagia to solids (55.6%), followed by coughing with eating (44.4%), dysphagia to pills (36.1%), and globus (27.8%). See Table 1 for further detail. Appendix A reports all MBSImP scores for this cohort.
Participant Demographics, Characteristics, and Baseline Data by Influence of Cueing on MBSImP Component 17 (Esophageal Clearance) Score.

Chi-Square or Fisher’s exact for categorical variables, Wilcoxon Rank-Sum for continuous variables. Alpha set at 0.05 to determine statistical significance.
Data not available for all participants.
Impressions of Esophageal Clearance Under Two Conditions
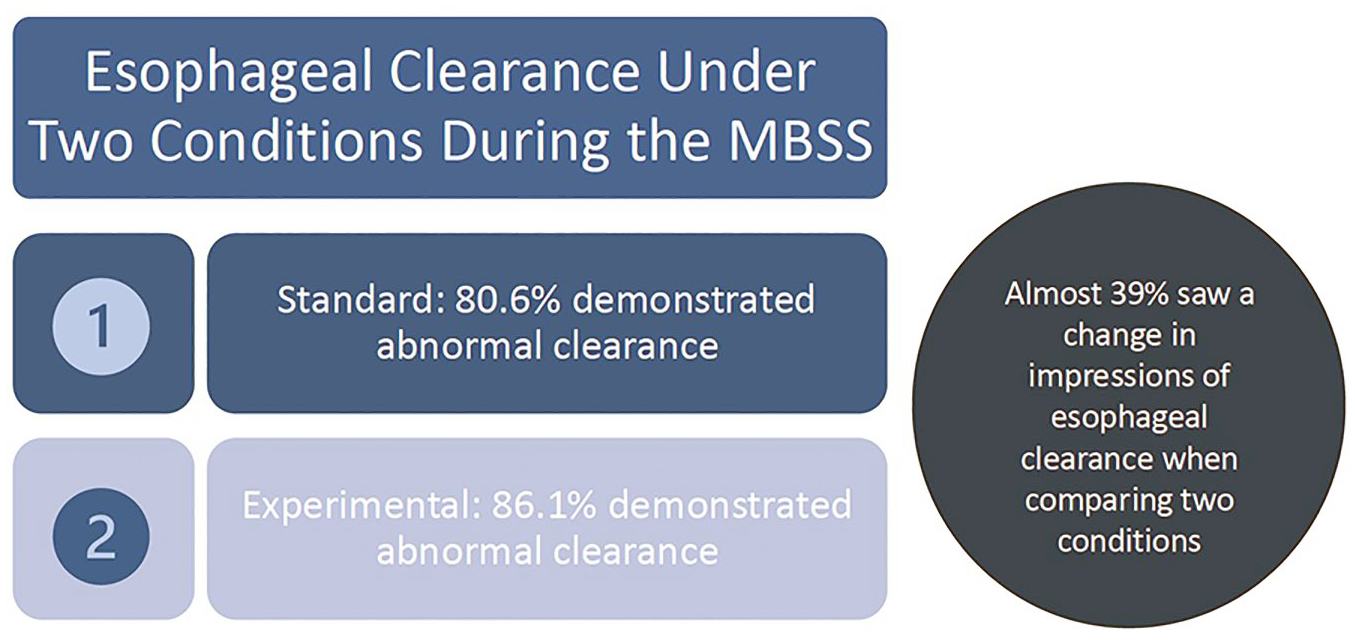
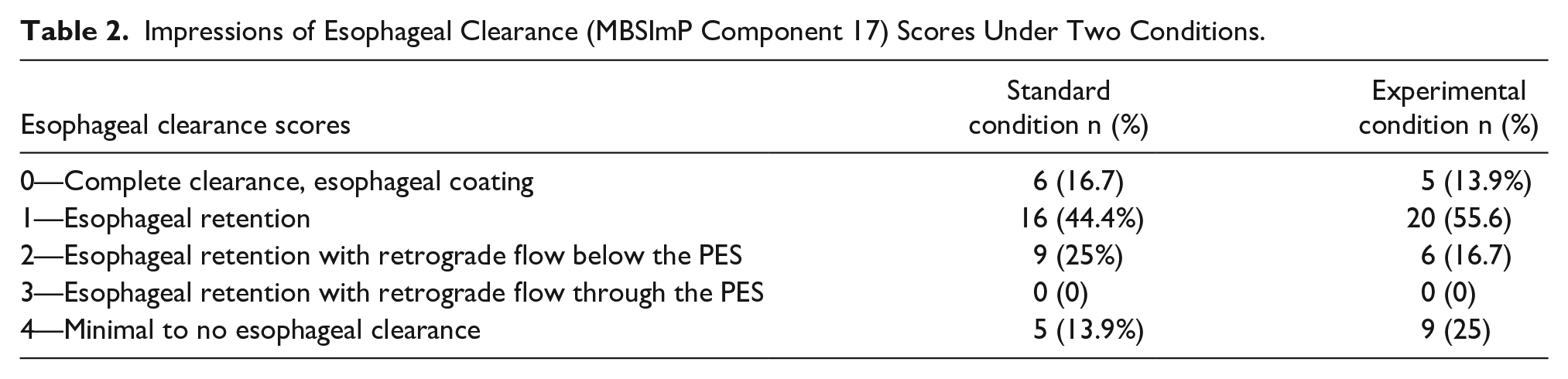
Component 17 (esophageal clearance) scores under the standard MBSImP protocol (un-cued) ranged from 0 to 4. Component 17 (esophageal clearance) scores changed between the standard and experimental conditions in 38.9% (14/36) of participants. For those with a change in component 17 scores, 42.9% (6/14) had a decrease (improvement in clearance) and 57.1% (8/14) had an increase (decline in clearance) in scores. A statistically significant association was identified for esophageal clearance (component 17) scores in the standard versus experimental condition (P < 0.0001). See Table 2.
Impressions of Esophageal Clearance (MBSImP Component 17) Scores Under Two Conditions.
Sub-Group Analysis of Participants with a Change in Component 17 (Esophageal Clearance) Scores Given Cueing
Fourteen participants were identified as having a change in component 17 scores in the cued (experimental) versus un-cued (standard) condition. The mean age for participants with a change in scores was 63.9 years (range 36-76, standard deviation ± 11.7). Most participants with a score change were female (57.1%) and almost all (85.7%) were white.
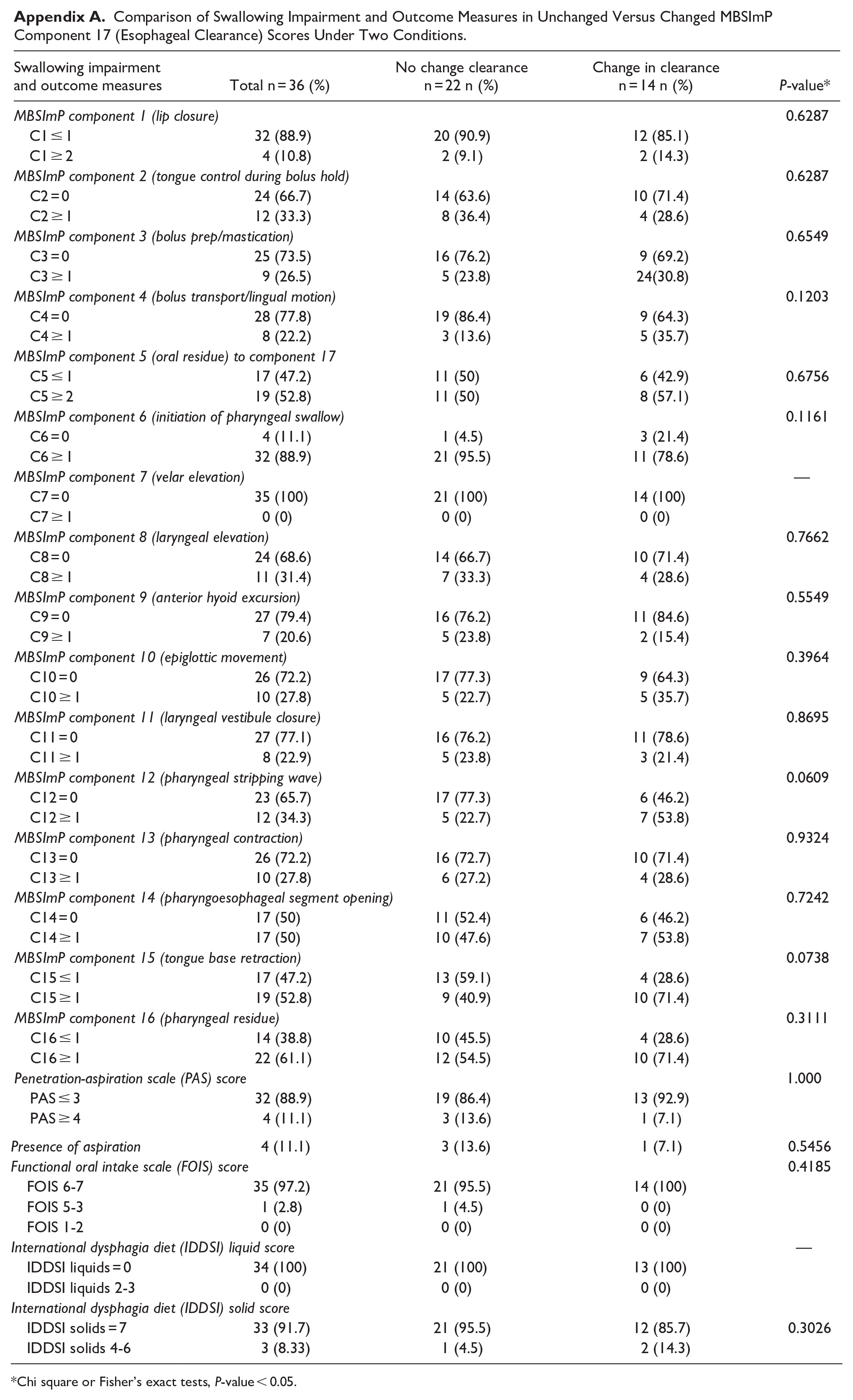
No statistically significant differences were seen between any of the other MBSImP components or swallowing outcome measures. However, results from comparisons with component 12 (pharyngeal stripping wave) might indicate a trend toward significance (P = 0.0609).
Decrease in Esophageal Clearance Scores
Six participants (6/14, 42.9%) were found to have a decrease in component 17 scores in our two study conditions indicating an impression for more typical esophageal clearance in the experimental (cued) condition. The mean age for participants who were found to have a decrease in component 17 scores was 64.8 years (range 53-74, standard deviation ± 9.5). Most, 5/7, (83.3%) participants in this subgroup of decreased scores were female and all were white.
Two (2/6, 33.3%) participants went from a score of 1 to a score of 0, thereby changing binary classifications from “atypical” to “typical” scores when comparing standard to experimental (cued) conditions. The remaining four participants (4/6, 66.7%) went from a score of 2 to a score of 1. This last change type represents a change in bolus retention patterns within the esophagus where patients in the cued condition no longer demonstrated retrograde flow.
Increase in Esophageal Clearance Scores
Eight participants (8/14, 57.1%) were found to have an increase in component 17 scores between the standard and experimental conditions indicating a more atypical impression of esophageal clearance in the experimental (cued) condition. The mean age for participants with an increase in component 17 scores was 63.1 years (range 36-76, standard deviation ± 13.7). Slightly fewer participants (3/7, 37.5%), in this subgroup of participants with an increase in scores, were female and almost all (6/7, 75%) were white.
A change from 0 to 1 was seen in 3 (3/8, 37.5%) participants, representing a change in binary classification from “typical” to “atypical” clearance when comparing the standard to the experimental conditions. One participants (1/8, 12.5%) demonstrated a change from a score of 1 to a score of 2. And three participants (3/8, 37.5%) changed from a score of 2 to a score of 4. This last change type representing the most “dramatic” of score changes (eg, largest score changes range) of this subgroup indicating that patients who had retention with retrograde flow within the esophageal body in the standard condition had minimal to no clearance in the experimental condition.
Discussion
When participants were provided a specific cue to swallow only once, impressions of esophageal clearance (component 17) changed in 38.9% of participants. In this small sample, providing an additional cue to swallow only one time resulted in more atypical clearance in the majority (57.1%) of our participants which contradicted our pre-study hypothesis that cueing would result in a reduction (improvement) in clearance. Our results, therefore, highlight the need for further study into the conditions under which impressions of esophageal clearance in the upright position are made during the MBSS.
Our cohort had very mild to no identifiable oropharyngeal swallowing impairments which likely influenced our findings of esophageal clearance. Most participants were classified with MBSImP oral total scores that indicated a mild/functional impairment and all participants had pharyngeal scores that were classified as mild/functional. Therefore, our cohort of participants with relatively “normal” oropharyngeal swallow function may not demonstrate meaningful relationships between oropharyngeal measures and impressions of esophageal clearance (component 17 scores) in our two conditions. Significant findings may be identified in a more heterogeneous sample representing a wider range of swallowing impairments from multiple primary etiologies (eg, stroke, neurodegenerative disease, head and neck cancer).
The evidence for co-occurring esophageal abnormalities identified during MBSSs is mounting.
Reported esophageal abnormality identified during the MBSS ranges from 26% to 100% in the literature.11,12 In our systematic review, we identified that when esophageal visualization was completed during the MBSS, 48.7% of participants had some type of esophageal abnormality. 9 Studies that report MBSImP scores demonstrated that populations whose acute impairment is traditionally thought to be for solely for oropharyngeal have evidence for abnormal esophageal clearance (component 17). Our work in stroke identified abnormal esophageal clearance in 57.9% of patients. 27 The majority of patients pre- and post-lung transplant have been identified with abnormal esophageal clearance.45,46 Similarly high prevalence for abnormal esophageal clearance was reported by Fong and colleagues in patients post-nonsurgical nasopharyngeal cancer treatment. 47 In the current study, abnormal esophageal clearance was identified in both standard MBSImP and experimental conditions (80.6% and 86.1%, respectively). The high proportion of esophageal findings may reflect that many patients referred for an MBSS, particularly outpatients, may have a primary esophageal etiology for their complaints of dysphagia but be referred first for an MBSS, likely due to ordering provider concern for potential aspiration or a lack of awareness in how to stratify risk for oropharyngeal versus esophageal disorders. It should be acknowledged that the participant-reported symptoms in our cohort could indicate a primary esophageal etiology, particularly as most of our cohort had no documented etiology that would predispose them to oropharyngeal dysphagia. Most participants reported dysphagia to solids (55.6%), followed by coughing with eating (44.4%), dysphagia to pills (36.1%), and globus sensation (27.8%). Studies attempting to study patient localization of dysphagia symptoms, specifically globus and a “sticking” sensation, have found poor correlation. Madhavan and colleagues identified esophageal abnormality in 69.5% of their participants presenting with globus sensation. 17 Ortiz and colleagues found that in 90% of their participants with globus had retained contrast in the esophageal body. 20 Though when patient symptoms were grouped into above the thyroid notch to below the thyroid notch, there was poor correlation to fluoroscopic findings. However, Ashraf et al 48 reported that the exact nature of anatomic abnormality or physiologic impairment influenced localization. For example, participants with an obstructive pathology in the proximal esophagus were the most accurate (81.7%) at identifying the level of their dysphagia. Overall, participants were determined to have an accuracy of 48.2% in identifying the level of their dysphagia.
There are many different factors that may influence esophageal visualization during the MBSS including positioning, protocol (eg, order of presentation, types of barium stimuli used, and under what conditions). Deglutitive inhibition, the alteration or cessation of peristalsis with swallows that occur quickly together, is relatively unexplored in visualization protocols and its influence is unknown in our sample owing to not counting the number of swallows in the standard (un-cued) condition. Both of Miles et al’s6,7 studies on esophageal bolus transit time report a patient directive to swallow a 20 mL bolus “all in one go,” potentially to address deglutitive inhibition. Miles et al 6 protocol specified a cue of “try hard not to swallow a second time,” and Watts et al 11 protocol included a cue to “only swallow one time.” Though cueing was included, the patient’s ability to adhere to the protocol was not recorded. To our knowledge, our study is the first of its kind investigating the potential influence of swallowing only once on impressions of esophageal clearance during the MBSS.
There is limited research that compares esophageal visualization during the MBSS to the standards of dedicated esophageal testing (eg, barium esophagram, high-resolution esophageal manometry). In their study comparing an esophageal screening protocol to a barium esophagram, Allen et al 5 reported a 62.8% specificity, 100% sensitivity, though both reported 95% confidence intervals had a range greater than 20%. Gullung et al 16 identified abnormal component 17 (esophageal clearance) MBSImP scores in 63.4% of their participants which correlated to a 78% sensitivity for detecting abnormality when compared to HRM-MII. No confidence intervals were reported for reference. Watts et al 10 reported a 100% agreement of abnormality identified during esophageal visualization when compared to dedicated esophageal testing (HRM, timed barium esophagram, esophagogastroduodenoscopy [EGD]), though only for a subset (52.5%) of their participants. More recently, Watts et al 11 reported a sensitivity of 83.7% and specificity of 73.7% when their Robust Esophageal Screening Test (REST) was compared against HRM or a timed barium esophagram; Though the 95% confidence intervals reported were greater than 20% sensitivity and greater than 30% for specificity.
While the esophageal visualization portion of the MBSImP is non-diagnostic, it provides relevant information to be correlated clinically to help determine those patients who would benefit from dedicated esophageal testing. It is important to acknowledge that an abnormal esophageal clearance in the upright position may not be indicative of a disorder. Only Gullung et al 16 has compared MBSImP findings against a gold-standard for esophageal assessment (HRM-MII). However, the study did not focus on this finding alone and did not further investigate findings by score, rather, by a dichotomized normal versus abnormal esophageal clearance (component 17) score. It is important to note that the MBSImP differs from other standardized assessments of esophageal visualization in its strict parameters for judging only esophageal clearance, whereas other protocols have been designed as an adjunct to a standard MBSS and is intended to assess esophageal function and/or anatomy.
What can be translated from this work is the nuances of assessing patients with symptoms of dysphagia. Given the interconnections between the oropharynx, esophagus, and the broader respiratory and digestive (aerodigestive) system; a multidisciplinary or transdisciplinary approach is ideal for ensuring proper work-up. Gregor and colleagues recently published their systematic approach to multidisciplinary care (SLP, ENT, GI) for patients with swallowing disorders and highlight the importance of contributions from many different specialties to enhance patient care and outcomes. 49 Every perspective is critical to acknowledge as each of us view the patient through our own discipline-specific lens.
Future Considerations
Future research into the parameters for judging esophageal clearance during the MBSS should consider patient factors and refine the assessment of swallowing. Standardized cognitive screening tests such as the Mini Mental Status Exam (MMSE) 50 should be considered in protocols where cognition may influence outcome. The process of counting swallows should be refined, such as by including sEMG which would register submental and laryngeal activity related to oropharyngeal swallowing. Additional metrics such as temporal and kinematic measures would help better describe the impact of different conditions on judgements of esophageal clearance during the MBSS. Future work using simultaneous manometry and fluoroscopy that examines different conditions on esophageal function is planned. Ultimately, our findings compel further research into the conditions in a more rigorous manner.
Limitations
This study has several limitations. First, as a pilot study no threshold was set for participant recruitment, and we only achieved a small sample size for this cohort. We did not address cognition as a potential influence on the participants’ ability to follow directions. The number of swallows in the standard (un-cued) MBSImP condition was not counted and, therefore, we were unable to compare if multiple swallows occurred in the un-cued condition; and if more than one swallow did occur, the time between swallows was not measured.
Conclusion
This study contributes to our knowledge about esophageal visualization and determinations of clearance during the MBSS. This study found that 38.9% of participants had a change in scores when provided a verbal cue to swallow only one time to account for deglutitive inhibition. Most of those with a change in scores demonstrated an increase indicating that impressions of esophageal clearance were more atypical in our experimental condition, which given the sample size and limitations should be interpreted with caution. Our findings highlight the importance of future work investigating the influence of cueing to account for the effect of deglutitive inhibition on impressions of esophageal clearance.
Footnotes
Appendix
Comparison of Swallowing Impairment and Outcome Measures in Unchanged Versus Changed MBSImP Component 17 (Esophageal Clearance) Scores Under Two Conditions.
| Swallowing impairment and outcome measures | Total n = 36 (%) | No change clearance n = 22 n (%) | Change in clearance n = 14 n (%) | P-value* |
|---|---|---|---|---|
| MBSImP component 1 (lip closure) | 0.6287 | |||
| C1 ≤ 1 | 32 (88.9) | 20 (90.9) | 12 (85.1) | |
| C1 ≥ 2 | 4 (10.8) | 2 (9.1) | 2 (14.3) | |
| MBSImP component 2 (tongue control during bolus hold) | 0.6287 | |||
| C2 = 0 | 24 (66.7) | 14 (63.6) | 10 (71.4) | |
| C2 ≥ 1 | 12 (33.3) | 8 (36.4) | 4 (28.6) | |
| MBSImP component 3 (bolus prep/mastication) | 0.6549 | |||
| C3 = 0 | 25 (73.5) | 16 (76.2) | 9 (69.2) | |
| C3 ≥ 1 | 9 (26.5) | 5 (23.8) | 24(30.8) | |
| MBSImP component 4 (bolus transport/lingual motion) | 0.1203 | |||
| C4 = 0 | 28 (77.8) | 19 (86.4) | 9 (64.3) | |
| C4 ≥ 1 | 8 (22.2) | 3 (13.6) | 5 (35.7) | |
| MBSImP component 5 (oral residue) to component 17 | ||||
| C5 ≤ 1 | 17 (47.2) | 11 (50) | 6 (42.9) | 0.6756 |
| C5 ≥ 2 | 19 (52.8) | 11 (50) | 8 (57.1) | |
| MBSImP component 6 (initiation of pharyngeal swallow) | 0.1161 | |||
| C6 = 0 | 4 (11.1) | 1 (4.5) | 3 (21.4) | |
| C6 ≥ 1 | 32 (88.9) | 21 (95.5) | 11 (78.6) | |
| MBSImP component 7 (velar elevation) | — | |||
| C7 = 0 | 35 (100) | 21 (100) | 14 (100) | |
| C7 ≥ 1 | 0 (0) | 0 (0) | 0 (0) | |
| MBSImP component 8 (laryngeal elevation) | 0.7662 | |||
| C8 = 0 | 24 (68.6) | 14 (66.7) | 10 (71.4) | |
| C8 ≥ 1 | 11 (31.4) | 7 (33.3) | 4 (28.6) | |
| MBSImP component 9 (anterior hyoid excursion) | 0.5549 | |||
| C9 = 0 | 27 (79.4) | 16 (76.2) | 11 (84.6) | |
| C9 ≥ 1 | 7 (20.6) | 5 (23.8) | 2 (15.4) | |
| MBSImP component 10 (epiglottic movement) | 0.3964 | |||
| C10 = 0 | 26 (72.2) | 17 (77.3) | 9 (64.3) | |
| C10 ≥ 1 | 10 (27.8) | 5 (22.7) | 5 (35.7) | |
| MBSImP component 11 (laryngeal vestibule closure) | 0.8695 | |||
| C11 = 0 | 27 (77.1) | 16 (76.2) | 11 (78.6) | |
| C11 ≥ 1 | 8 (22.9) | 5 (23.8) | 3 (21.4) | |
| MBSImP component 12 (pharyngeal stripping wave) | 0.0609 | |||
| C12 = 0 | 23 (65.7) | 17 (77.3) | 6 (46.2) | |
| C12 ≥ 1 | 12 (34.3) | 5 (22.7) | 7 (53.8) | |
| MBSImP component 13 (pharyngeal contraction) | 0.9324 | |||
| C13 = 0 | 26 (72.2) | 16 (72.7) | 10 (71.4) | |
| C13 ≥ 1 | 10 (27.8) | 6 (27.2) | 4 (28.6) | |
| MBSImP component 14 (pharyngoesophageal segment opening) | 0.7242 | |||
| C14 = 0 | 17 (50) | 11 (52.4) | 6 (46.2) | |
| C14 ≥ 1 | 17 (50) | 10 (47.6) | 7 (53.8) | |
| MBSImP component 15 (tongue base retraction) | 0.0738 | |||
| C15 ≤ 1 | 17 (47.2) | 13 (59.1) | 4 (28.6) | |
| C15 ≥ 1 | 19 (52.8) | 9 (40.9) | 10 (71.4) | |
| MBSImP component 16 (pharyngeal residue) | 0.3111 | |||
| C16 ≤ 1 | 14 (38.8) | 10 (45.5) | 4 (28.6) | |
| C16 ≥ 1 | 22 (61.1) | 12 (54.5) | 10 (71.4) | |
| Penetration-aspiration scale (PAS) score | 1.000 | |||
| PAS ≤ 3 | 32 (88.9) | 19 (86.4) | 13 (92.9) | |
| PAS ≥ 4 | 4 (11.1) | 3 (13.6) | 1 (7.1) | |
| Presence of aspiration | 4 (11.1) | 3 (13.6) | 1 (7.1) | 0.5456 |
| Functional oral intake scale (FOIS) score | 0.4185 | |||
| FOIS 6-7 | 35 (97.2) | 21 (95.5) | 14 (100) | |
| FOIS 5-3 | 1 (2.8) | 1 (4.5) | 0 (0) | |
| FOIS 1-2 | 0 (0) | 0 (0) | 0 (0) | |
| International dysphagia diet (IDDSI) liquid score | — | |||
| IDDSI liquids = 0 | 34 (100) | 21 (100) | 13 (100) | |
| IDDSI liquids 2-3 | 0 (0) | 0 (0) | 0 (0) | |
| International dysphagia diet (IDDSI) solid score | ||||
| IDDSI solids = 7 | 33 (91.7) | 21 (95.5) | 12 (85.7) | 0.3026 |
| IDDSI solids 4-6 | 3 (8.33) | 1 (4.5) | 2 (14.3) | |
Chi square or Fisher’s exact tests, P-value < 0.05.
Acknowledgements
The authors would like to acknowledge the MUSC Health and Rehabilitation Sciences department for PhD funding. A special thanks to the Speech-Language Pathologists who contributed to this study: Melissa Cooke, Kate Davidson, Olivia Bupp, and Mary-Chase Godwin. Further, the authors would like to acknowledge the MUSC Speech Language Pathology department, MUSC Laryngology department, and MUSC Gastroenterology Manometry Lab for their immense support of this work.
Author Contributions
Study design, data acquisition, and drafting of the original manuscript were performed by first author, E.L.R. Both E.L.R. and A.N.S. completed data analysis and contributed to the interpretation of this work. A.K.O and senior author, H.S.B., contributed substantially to study conceptualization and edition of earlier versions of the manuscript. All authors read and approved of the final manuscript.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.
Data Availability
Reasonable requests for data can be made to corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided for first-author’s doctoral studies through the Health and Rehabilitation Sciences Department in the Collage of Health Professions at the Medical University of South Carolina.
Ethical Approval
All ethical standards for research were maintained throughout this study. Written informed consent was obtained from all participants. Approval from the Medical University of South Carolina’s Institutional Review Board was received.