
Abstract
Chevalier Jackson (1865-1958), a pioneering physician and innovator of the endoscope, revolutionized the management of esophageal injuries and is regarded as the father of endoscopic surgery. At the dawn of the 20th century caustic lye ingestion was the leading cause of esophageal injury and stricture, while peptic injury had not even been recognized. Jackson defined peptic ulcers as a clinical entity and correctly surmised that the etiology was due to gastroesophageal reflux. Moreover, his groundbreaking techniques introduced direct examination of the esophagus and intervention under visualization, replacing the dangerous blind bougienage that dominated the 19th century. His public health advocacy culminated in the Federal Caustic Poison Act of 1927, mandating poison and antidote labels on household products and nearly eliminating caustic esophageal injury as a major public health issue. This review highlights Jackson’s enduring legacy, from transforming the esophagus from the “no man’s land” of medicine to the “every man’s playground” to demonstrating the profound societal impact of physician-led public health reform.
Introduction
Since the turn of the 21st century the most common cause of esophageal injury has been gastroesophageal reflux disease (GERD), accounting for approximately 75% of all esophageal pathology. In North America, GERD affects about 1 in 4 adults, with 20% to 40% of these individuals presenting with erosive esophagitis.1,2 In contrast, caustic esophageal injury is rare, accounting for approximately 7.7 per 100 000 emergency room visits, only 16% of which require admission. 3 However, at the dawn of the 20th century the epidemiology of esophageal injuries was quite different. Physicians had not even recognized GERD and its complications as a distinct clinical entity, instead, they viewed peptic ulcers in the distal esophagus as more of a postmortem finding than as a recognized disease process. 4 Caustic esophageal injury was a common and devastating problem, with some esophagologists in the 1920s reporting caustic injury constituting up to 1 in 10 of all their diagnosed esophageal disorders.5,6 The historic mortality of caustic esophageal injury was 50%. 7 The advent of modern endoscopic techniques and physician-led public health reforms revolutionized clinical outcomes for caustic esophageal injury and increased recognition and understanding of peptic injury. Chevalier Jackson (1865-1958), the innovator of the endoscope, a globally recognized professor of endoscopic techniques, and the father of endoscopic surgery was central to this transformation 8 (Figure 1).

Chevalier Jackson (1865-1958).
This review explores 2 key pillars of Chevalier Jackson’s legacy. First, his groundbreaking innovations in the treatment of esophageal injury and its cicatricial sequelae, stemming from both caustic and peptic etiologies. Second, his transformative work in public health, culminating in the Caustic Poison Act of 1927, which mandated poison and antidote labels on hazardous household products. 9 Jackson’s work, from pioneering endoscopic techniques to spearheading legislative change, reflects a deep understanding of the interconnectedness between individual care and societal well-being. His achievements serve as a testament to the power of physicians to not only alleviate suffering, but to address the deeper, root causes of preventable harm. His story offers a lens through which we can reflect on the enduring role of medicine in shaping a healthier, safer world.
Historical Context of Caustic Esophageal Injury
From 2012 to 2014, Poison Control Centers received nearly 14 000 reports of laundry detergent pod ingestion in children under the age of 6. 10 These brightly colored, candy-like pods, initially packaged in transparent containers resembling “gum-ball machines,” were often accidentally consumed by curious children, leading to esophageal injuries. Fortunately, the issue was quickly recognized and hospitalizations related to these ingestions declined by 69% within 5 years. 11 This decline was made possible by a change in packaging with more pronounced warning labels, the well-established poison control system and the readiness of media to spread the news of the danger. However, these infrastructures were not in place 150 years ago. Nevertheless, in the late 19th and early 20th centuries children had an equally dangerous curiosity for cleaning chemicals, an issue that was even more problematic then than it is today. A different product dominated household injury: lye. This colorless odorless common household product, nearly indistinguishable from sugar, was commonly sold in grocery stores, stored in the kitchen and mixed with animal fats at home to make soap. 12
A major contributor to caustic lye injury was a lack of education exacerbated by misinformation on the part of lye packers. People were familiar with skin irritation from “potash,” potassium hydroxide lye made from wood ash, but sodium hydroxide lye was not as common in the early 19th century. This changed with the advent of Thomas Edison’s central power station in 1882, facilitating electrolytic production of sodium hydroxide from common table salt.12,13 The ease of mass manufacture led to an expansion of commercial sodium hydroxide lye products. Without regulation, lye-packers marketed their products as harmless, often with claims like “Will not hurt the hands” or “Impossible to harm the most delicate of fabrics”; however, even their most dilute formulations were no less dangerous to the sensitive mucosa of the esophagus (Figure 2). Unaware of the potential dangers, parents often left this caustic alkali within reach of their children, leading to thousands of accidental ingestions. While most of these incidents involved children, even adults occasionally suffered caustic esophageal injuries when they unknowingly drank from mixing cups that still contained residue of the alkali.
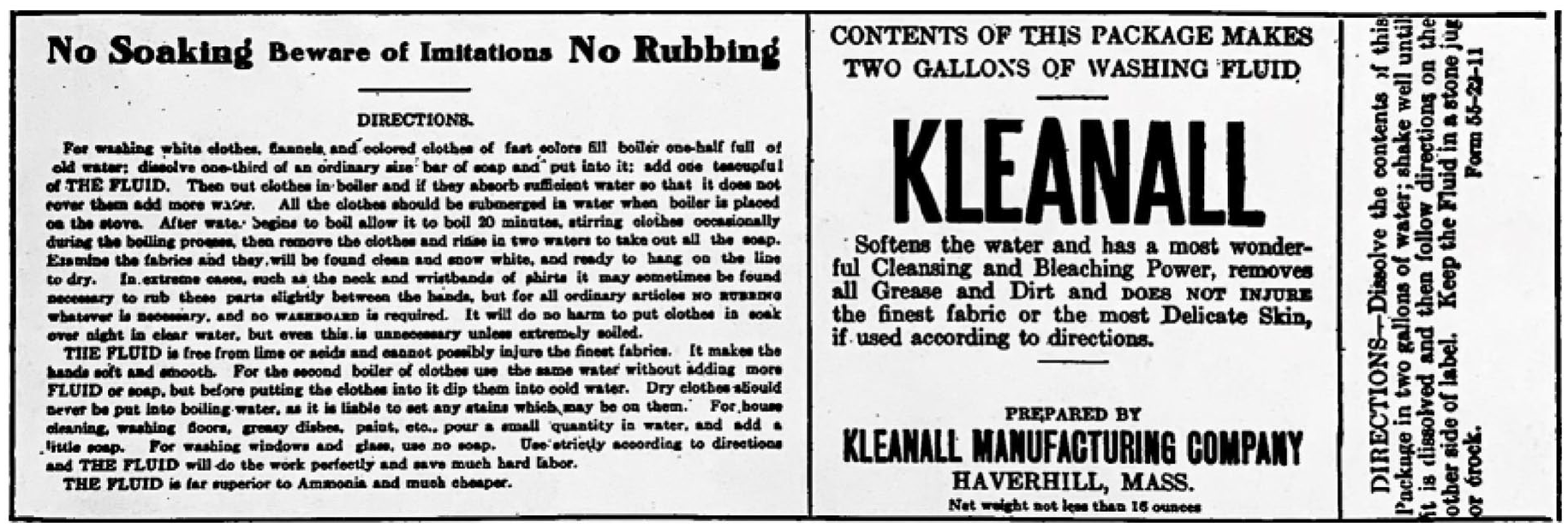
Replication of KLEANALL brand lye label with no hint of warning and including the misleading phrases “DOES NOT INJURE the finest fabric or the most Delicate Skin,” “free from lime or acids and cannot possibly injure the finest fabrics,” and “It makes the hands soft and smooth,” implying that there is no danger. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
The moment caustic lye is ingested it causes immediate and devastating tissue damage. Lye ingestion affects the mucosa in 3 ways: (1) the hydroxide group undergoes a saponification reaction with triglycerides in the cell membrane, leading to a breakdown of the phospholipid bilayer and cell lysis, (2) the localized increase in pH disrupts salt bridges and hydrogen bonds denaturing tight junction proteins, increasing permeability of the mucosa, and (3) neutralization of weak acids with a strong base is exothermic with potential to cause further thermal injury. 14 The ultimate result is rapid liquefactive necrosis, which allows the alkali to penetrate deeper into the esophageal wall. This causes burns that could extend into the submucosa, muscularis and in severe cases result in perforation. The extent of the damage varies with the concentration, quantity and form (powder or solution). Additionally, factors such as the presence of food and the duration of contact with the tissues, a function of esophageal peristalsis and bolus clearance, affect the extent of the damage. In the 19th and early 20th centuries esophageal perforation, often led to fatal sequelae like mediastinitis or peritonitis. Indeed, this injury was fatal in 50% of patients during the initial stages of presentation.15-17
As patients recovered from the initial injury, and the acute inflammatory reaction subsided over the course of 1 to 3 weeks, they often enjoyed a latent period without any symptoms. 18 During this time the necrotic tissue sloughs away leaving the ulcerated surface with granulation tissue. However, 3 to 4 weeks later, scar tissue begins to replace the damaged submucosa and muscularis. As the scar tissue matures and contracts, it can form a stricture. This cicatricial narrowing of the lumen of the esophagus is prone to obstruction. Poorly masticated food can get stuck, causing dysphagia and weight loss. Stagnant food ferments in the esophagus, leading to proximal sacculation and esophagitis, which ultimately accelerates the progression of cicatricial narrowing in the stricture. As a result, a patient who initially experienced dysphagia to solid foods may progress to the point where they can no longer tolerate liquids or even their own salivary secretions. Without adequate treatment patients would die of starvation or dehydration. Among recognized causes of cicatricial stenosis in the 19th and 20th century (household ammonia, salts of tartar, washing soda, mercuric chloride, strong acids, tuberculosis, lues, scarlet fever, diphtheria, enteric fever, esophagitis secondary to spasmodic stenosis and peptic ulcer of the lower esophagus) ingestion of lye was by far the most common cause. 18
Historical Management of Esophageal Strictures
The exact date of the first description of esophageal strictures is difficult to determine, as a definitive diagnosis was not possible until Chevalier Jackson introduced endoscopy and described their appearance. However, indirect detection and treatment of strictures potentially dates back thousands of years. In the second century Galen first described esophagitis and linked it to the symptom “kardialgia” (heart pain). He also described “fleshy growths” in the esophagus that led to obstruction, which may be the first description of esophageal stricture or cancer. 19 Abu-Marwan Abdel-Malik Ibn Zuhr (often latinized as Avenzoar) of the 12th century Western Caliphate described the use of a silver or tin cannula placed into the throat of a patient with dysphagia to aid in ingestion of liquids, the first attempt at a stent and possibly the first treatment of esophageal stricture. 20 The first clear description of the management of esophageal stricture was in 1801 by Antoine Vareliaud (1776-1840) who demonstrated the efficacy of blind bougienage for the management of presumptive stricture. 21 Vareliaud built on the works of prior esophageal interventionists. The 16th century Italian anatomist and surgeon Hieronymus Fabricius (1537-1619) used a thin length of wax to push a foreign body into the stomach, inventing the bougie.22,23 The word “bougie” comes from the French word for candle, etymologically derived from the Algerian town of Boujiyah, the medieval center for the wax trade. Around the same time, the anatomist and Parisian surgeon-barber Ambroise Pare (1510-1590) developed leather tubes and wands covered in gut for the purpose of pushing foreign bodies into the stomach. Dilation of the esophagus was first introduced by the English anatomist and physician Sir Thomas Willis (1621-1675) who used a whale bone blunted with a sponge to forcibly dilate the esophagus of a patient with achalasia. 24
In the 19th century, physicians had to rely on patient history, subjective symptoms and inductive reasoning to diagnose stricture and other esophageal diseases. 25 Symptom presentations were often intermittent and sometimes confusing. Large particles of food could stimulate spasmodic stenosis, which holds the obstructing foreign body at the level of the stricture until relaxation. Additionally, edema associated with stasis esophagitis narrows the lumen prolonging symptoms until the esophagitis subsides. Without the ability to directly examine the esophagus, physicians could only speculate about the underlying condition. Blind bougienage offered the first piece of objective evidence of potential stricture and became the predominant procedure for both diagnosis and treatment. The physician would take a long thin instrument, often self-crafted, and push it down the patient’s esophagus. If resistance was encountered, it was thought to be either a foreign body (if the resistance yielded with slight pressure) or a stricture (if the resistance persisted). 18 Patients with strictures frequently required multiple blind dilations, and some pressure was necessary to dilate a stricture. Naturally, this blind approach was both imprecise and dangerous. At one time or another the point of the bougie was certain to be engaged in a pocket instead of the stricture, resulting in a fatal perforation. In fact, the French Internist Armand Trousseau (1801-1867) famously lamented, “sooner or later all cases of stricture of the esophagus die by the bougie.” 26
While blind bougienage became the most prevalent technique in the 19th century, there was some experimentation with a variety of different interventions. A case report from an 1821 issue of the New England Journal of Medicine described the management of a patient with esophageal stricture by first bleeding the patient to cure their nausea followed by blind bougienage. 27 However, when the patient couldn’t tolerate the bougie any longer the physician recommended esophageal application of caustic alkali. The dysphagia resolved, and the patient resumed sporadic bougienage, which may have hindered further stricture from the therapeutic caustic. Another unusual case report from 1884 described the use of home-made galvanic batteries and a bougie with an electrode at its tip to run a current through an esophageal stricture 3 times a week for 6 to 12 minutes at a time. 28 On the 15th visit, the patient was able to eat solid food again, likely more due to inadvertent dilation with the electrode than the current itself. These treatments did not become prominent; however, they illustrate the rogue medical landscape that Chevalier Jackson entered when he graduated from medical school in 1886.
Endoscopy and Chevalier Jackson’s Management of Esophageal Strictures
In 1868, Kussmaul became the first to peer into the esophagus of a living patient using a sword-swallowing technique with a modified Desormeaux urethroscope. 29 In 1881 Mickulicz and Mackenzie developed their own crude esophagoscopes. The works of the latter had fascinated Chevalier Jackson while in medical school and in 1886 he voyaged to England to study under Sir Morell Mackenzie. 12 During this trip he was able to observe Mackenzie’s skeleton endoscope, which could barely see past the distal pharynx. Upon his return to Pittsburgh, Chevalier Jackson began to work on his own design. In 1890 he was able to craft an endoscope “worthy of its name.” His scope uniquely incorporated a distal light source, a separate channel for suction, and a groove for instrumentation in addition to visualization. Armed with this tool, Chevalier Jackson began a prolific career in bronchoesophagology, pioneering safe and consistent endoscopic examination, as well as developing the first endoscopic surgeries. Before Chevalier Jackson the esophagus was the “no man’s land” of medicine. 30 He induced a paradigm shift in the treatment of esophageal disease from pure inference to direct examination of the esophagus and stomach. His scientific contributions and excellent patient outcomes garnered him national and international recognition. Much of his notoriety came from his dedication to disseminating his safe and consistent endoscopic techniques. He established the first bronchoesophagoscopy clinic at Western Pennsylvania Hospital in Pittsburgh and later expanded his teaching clinics to all 5 medical colleges in Philadelphia, as well as teaching many endoscopy courses across the globe (Figure 3). He never patented any of his scopes or endoscopic tools to facilitate the free dissemination of endoscopy. From “no man’s land” Chevalier Jackson made the esophagus “every man’s playground,” as surgeons, otolaryngologists, internists, thoracic surgeons, and eventually gastroenterologists picked up the scope. 30
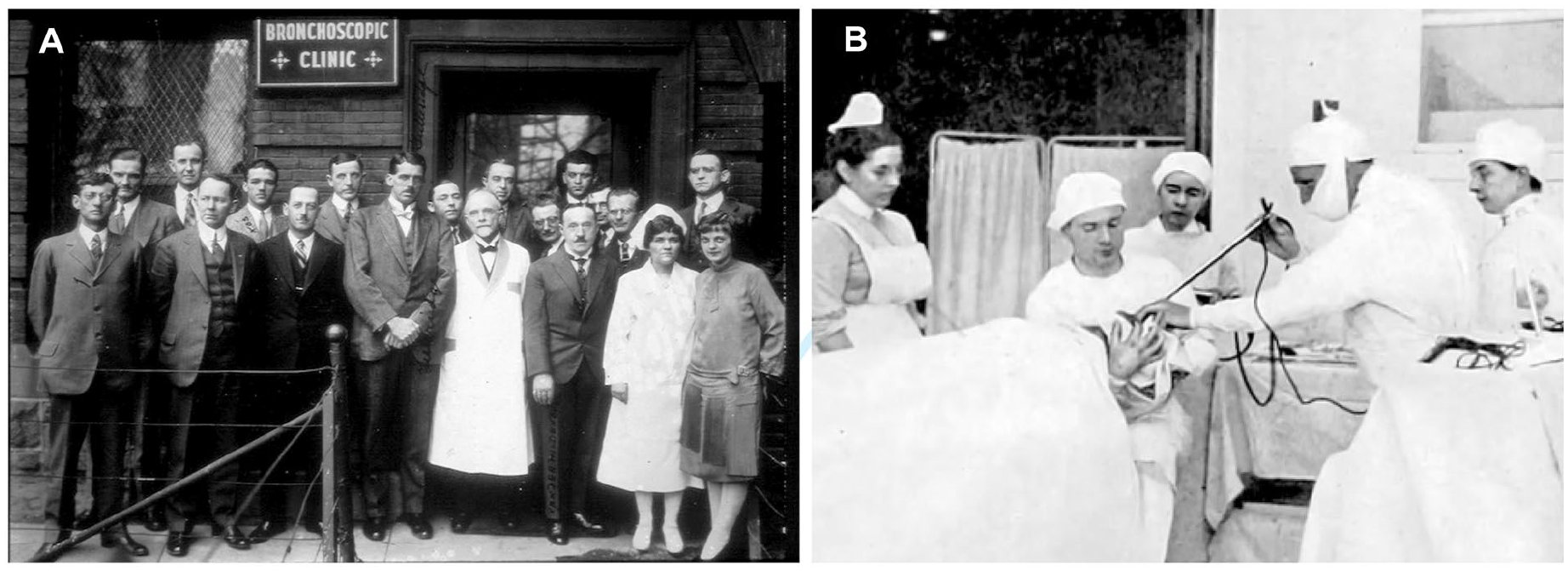
(A) The Jackson clinic where he performed his endoscopic and bronchoscopic procedures and (B) rigid endoscopy at the Jackson clinic. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
Blind bougienage could only detect resistance due to stenosis. With the endoscope, Chevalier Jackson was able to see and diagnose the cause of stenosis. He published detailed descriptions and highly accurate chalk drawings of his endoscopic findings to enable other endoscopists to recognize and distinguish cicatricial stricture from stenosis due to tumor, compression, or spasm (Figure 4).18,25 Chevalier Jackson became the physician to see if your child was unable to swallow several weeks after ingesting lye. Endoscopy eliminated the risks of blind bougienage, as Chevalier Jackson did not have a single mortality as the result of his examination or treatment. In fact, Chevalier Jackson found his technique so superior to blind bougienage that he denounced the practice as a “time-wasting, misleading and utterly useless” recommending that it “should be discarded as obsolete and very dangerous.” 18 Additionally, accurate diagnosis and precise intervention drastically improved overall patient outcomes. Prior to endoscopy, mortality from caustic ingestion was estimated to be 50%. With endoscopic intervention, Jackson reported that mortality was near 0. His excellent results were owed in parcel to his standardized methodology with a diligent focus on safety.18,25
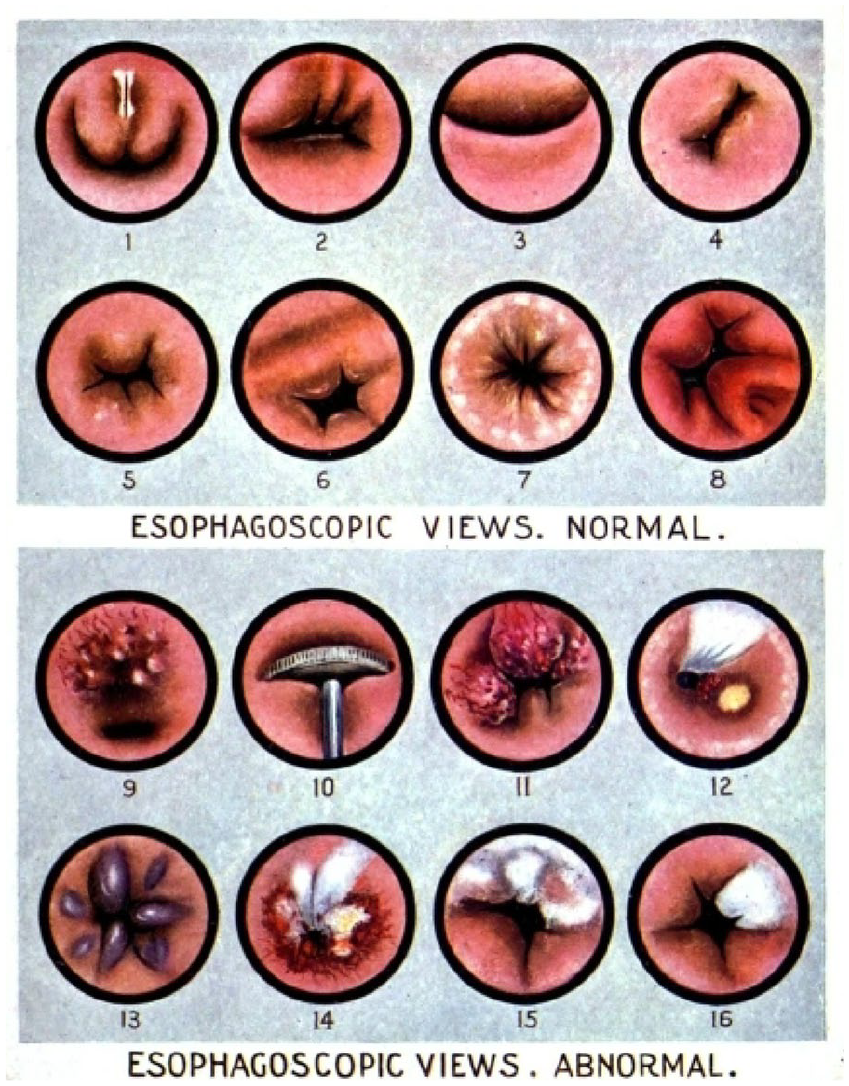
Chevalier Jackson’s drawings of the endoscopic views of: (1) Laryngopharynx. (2) Right pyriform sinus at level of cricoid. (3) Cricopharyngeal constriction. (4) Through right pyriform sinus. (5) Cervical esophagus. (6) Thoracic esophagus at level of left bronchus. (7) Hiatus. (8) Stomach. (9) Sarcoma. (10) Half-dollar foreign body. (11) Squamous cell epithelioma. (12) Cicatricial stenosis of 4 -year old due to swallowing of lye. (13) Angioma. (14) Luetic ulcer. (15) Tuberculosis. (16) Leukoplakia. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
His initial treatment of acute caustic injury was neutralization with vinegar for alkalis and sodium bicarbonate for acids. This treatment was later discontinued once the risk of thermal injury from exothermic neutralization was recognized. Mercuric bichloride, a common disinfectant before the advent of antibiotics, was combined with eggs or flour mixed in water or milk and swallowed to coat the esophageal ulcers with disinfectant. Bismuth subcarbonate was then washed down every 30 minutes for 2 hours and then every 3 to 4 hours for the next couple of days. Early endoscopy was delayed for fear of perforation but was first performed within 2 to 3 weeks. Thereafter, the patient was scoped weekly to prevent stricture. For acute inflammation and ulceration, the treatment was bed rest with a restricted liquid diet. Medications included small and frequent doses of Bismuth and Calomel, a mercurous chloride-based laxative popular in the 18th and 19th centuries. Calomel was largely discontinued by the mid-20th century following the recognition of mercury toxicity. Ulcers were also treated topically, with endoscopic application of Argyrol, a silver protein antiseptic. Later in his career Chevalier Jackson abandoned local application of medications, favoring giving the patient a bismuth marshmallow instead, which was more popular among his largely pediatric population.
Though the first horse-drawn ambulances were created in 1865 during the Civil War, emergency medical services were not readily available in Pittsburgh until the 1967 establishment of the Freedom House Ambulance Service. This entirely Black paramedic corps, born out of the Civil Rights Movement, paved the way for modern EMS systems. 31 At the start of the 20th century limitations in transportation meant that most patients who ingested lye could not see a physician immediately. The majority of Chevalier Jackson’s patients presented with chronic severe strictures, often dehydrated and starving to death, despite access to food and water. As such, the first line treatment was gastrostomy. For severe dehydration, Jackson used a Murphy drip and hypodermoclysis for resuscitation. Normal saline formulations were not available until the 1930s and sterile technique for routine intravenous administration was not available until the 1940s.32,33 If the patient was unable to swallow even their saliva, they were encouraged to spit into the funnel of the gastrostomy tube to avoid dehydration (Figure 5). Frequently dysphagia to liquids was not due to a completely obstructive stricture, but a narrowing blocked by piece of food. In these cases, the foreign body was simply uncorked with endoscopic forceps allowing liquids to pass. As a result, gastrostomy was rarely necessary. At the time, there were no consumer tube feeds or liquid diet formulas. The endoscopy clinic made feeds by straining fruit and vegetable juices, with the thickest food allowed being sieved mashed potatoes. Most patients remained on a liquid diet throughout the initial treatment period, with solids added only after demonstrating that no stagnation occurred. Patients were educated on the importance of thorough mastication and advised to eat slowly, taking small quantities at a time. These nutritional interventions were all pioneered at Dr. Jackson’s clinic. Chevalier Jackson was an early proponent of multidisciplinary care, recommending consultation of the pediatrician to aid in nutritional optimization.
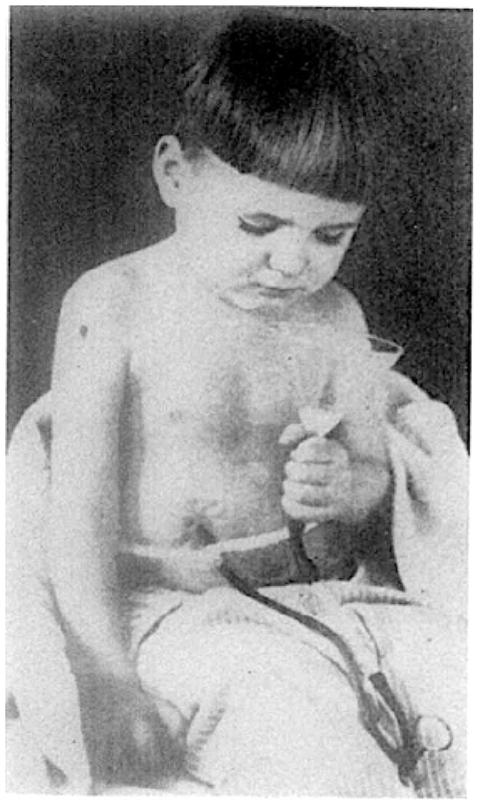
Pediatric patient with complete esophageal obstruction secondary to ingestion of caustic lye. The patient has been nutritionally resuscitated through a gastrostomy tube and is avoiding dehydration by clearing salivary excretion into a funnel going back into the stomach. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
Wary of dilation with intent to restore the full luminal diameter due to the risk of perforation, Chevalier Jackson found that most cases could be managed with a relatively small lumen. Dilation size was based on the size of the sacculation just proximal to the stricture. Large sacks required large dilations, whereas minimal sacculation was only dilated to about 6 to 7 mm. The goal was not restoration of anatomy, but restoration of function. Therefore, he would dilate only until his patients could demonstrate functional swallowing, without the need for endoscopic retrieval of retained food particles. Roentgen discovered X-rays in 1895, and Dawson described the first radiographic diagnosis of esophageal stricture in 1907. 34 Following these innovations, Jackson also incorporated confirmation of functionally adequate patency with a bismuth esophagram.
The preferred method of dilation was bouginage under direct endoscopic observation with filiform bougies of his own design (Figure 6). Diets during dilation were restricted in quantity and consistency. Only liquids and “semi-solids,” that is, soft-boiled eggs, custards, and ice cream, were permitted. If the patient felt food getting stuck, they were instructed to regurgitate and take a glassful of sodium bicarbonate to lavage the esophageal mucosa. All dilations were performed without any anesthesia. Once adequate deglutition was achieved, patients were instructed on self-dilation with a traditional bougie (Figure 7). They were advised to never use force to push the bougie down and to swallow 10ccs of olive oil for lubrication. Patients would continue self-dilations 3 times per week for 3 to 4 months and then continued weekly for a year. After that he recommended monthly self-dilation for early detection of recurrence. His practice was an early example of patient centered care.

The Jackson bougie was made of gum elastic over a woven silk base. The tapered end design harks back to the original wax bougies. He developed the olive-shaped distal end, which was safer than a conical tip and less likely to cause a false passage. The length of the dilating portion was 7 cm, with a rounded proximal end so as to not catch an edge on withdrawal. In each session the bougie was replaced 3 to 4 times with successively larger sizes. The largest bougie was placed and left inserted for 20 minutes. Patients required dilations every couple of days until the largest size could be inserted and removed without resistance on the first pass.
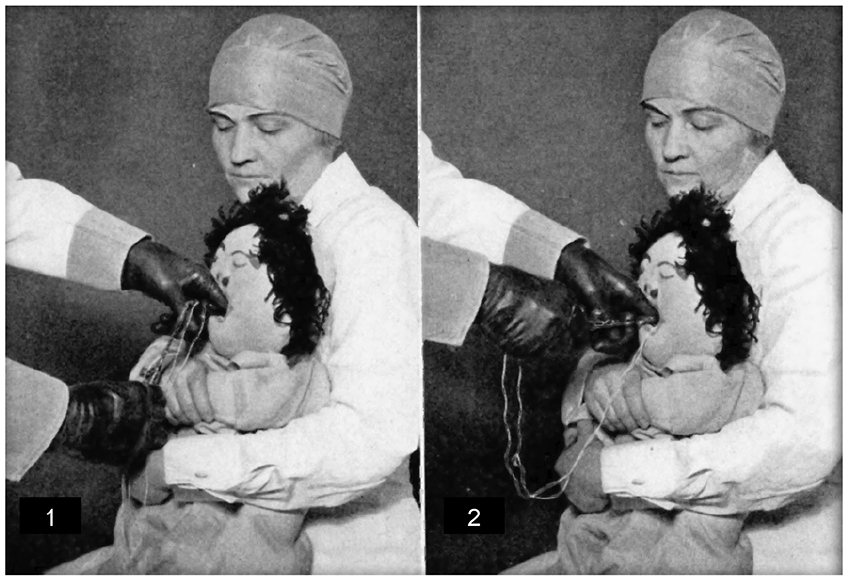
Jackson created a variety of teaching dolls to help educate his largely pediatric population on their care. This doll was designed to demonstrate the self-dilation technique, which Jackson treated as a sword swallower routine that helped the children turn what is a challenging healthcare procedure into playtime. This patient centered approach was key to the excellent efficacy of his treatment protocols. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
Cases of combined antegrade-retrograde rendezvous dilation have recently been described in the literature, with some suggesting the technique is relatively novel. Certainly, with the modern fiberoptic scope it may be however, Chevalier Jackson described his technique for endoscopic rendezvous dilations of complex esophageal strictures in 1915. 18 Distal esophageal strictures were approached endoscopically from both ends, per oral and through a gastrotomy. The surgeon would feel for the endoscope pressing against the stricture and then would cut through into the lumen of the endoscope. G-tubes would be left in place for 4 weeks to allow the esophagus to heal and then the patient would undergo the regular dilation procedures.
While many of the patients with strictures he treated were children, some were adults. One such patient was admitted to Western Pennsylvania Hospital with 20 years of dysphagia following a trauma, which more recently had progressed until only liquids could go down. On endoscopic evaluation the patient had developed a diverticulum proximal to an ulcerated thick and tight stricture, which later proved to be squamous cell carcinoma. Chevalier Jackson recognized this as evidence that chronic inflammation can lead to cancer.
Chevalier Jackson and the Recognition of Peptic Strictures
Chevalier Jackson also played an integral role in our understanding of peptic strictures. Peptic ulcers in the distal esophagus were thought to be a postmortem finding, believed to result from gastric regurgitation. 35 However, this understanding changed with Chevalier Jackson’s presentation before the Section on Gastroenterology and Proctology at the 79th Annual Session of the AMA in 1928. 4 He reported his series of distal esophageal “peptic ulcers” in 88 living patients, becoming the first to recognize this as a distinct clinical entity. He correctly speculated that these ulcers might be the result of retrograde flow of acidic gastric juices into the esophagus. He also suggested that this finding may be associated with heartburn symptoms, esophagitis, and peptic strictures. His management of these strictures was the same as with caustic strictures, bougienage under direct endoscopic examination, followed by self-bougienage to maintain patency.
Jackson’s suspicions about the relationship between reflux and peptic ulcers were later substantiated by Asher Winkelstein who at the 1935 annual session of the American Medical Association presented his case series describing “peptic esophagitis.” 36 He used Roentgen exam, endoscopy, biopsy and chemical sampling in patients with non-ulcerative esophagitis despite the absence of any clear irritant, infectious, spastic, neoplastic or structural cause. Each had distal esophageal inflammation with acidic hyperchlorhydria, suggestive of damage from hydrochloric acid and pepsin. Chevalier Jackson was in the audience and rose to give a “hearty accord” with Winkelstein, going on to say that his “experience coincides with that of the author that the cause of this kind of esophagitis is similar to the causes of gastric ulcer. . . and is often seen at the lower end of the esophagus in cases of herniated stomach.”
Despite Jackson’s astute insights into the etiology of peptic ulcers and strictures, physicians remained perplexed by the condition for decades. One case from 1946 detailed the management of a 33-year-old woman with strictures that returned after bougienage. 37 Unsure of the cause of the recalcitrance, the surgeon elected to perform a thoracic exploration, which was fruitless, and 9 months later elected to perform an esophagectomy. It wasn’t until Allison described the association between hiatal hernia and peptic esophagitis that interest in correcting anatomic disturbances of the gastroesophageal junction started to grow. Surgeons initially began to try simple hernia repairs but were disenchanted with their unsatisfactory results. Throughout the 1950s a variety of surgeries were attempted to adequately address acid including vagotomy, gastrectomy and partial esophagectomy and gastroenterostomy. Eventually, Nissen decided to repair an esophageal perforation by wrapping the fundus of the stomach around the hole. The patient happened to have heartburn, which resolved after the surgery. He reported his initial series of Nissen fundoplication for reflux in 1956.
Chevalier Jackson’s Advocacy for Public Health and Patient Safety in Lye Legislation
One of Chevalier Jackon’s earliest lye patients was brought in by 2 nuns who had been visiting a woman dying of pneumonia. 12 They discovered an emaciated little girl, desperately trying to drink water from a tin pail, but unable to get it down, regurgitating water all over her clothes. Chevalier Jackson promptly scoped her and removed a small piece of food matter that had corked a narrow stricture. The little girl drank a little water with trepidation, and when the liquid went down, she drank a little more. Then she pushed away the hand of the nurse feeding her the cup, took Chevalier Jackson’s hand, and kissed it. Chevalier Jackson took no money from this patient or indeed from many of his patients. Nevertheless, the memory of the kiss on his hand was a source of persistent satisfaction for years to come. However, the needlessness of this little child’s suffering disturbed him and inspired him to take up the cause of prevention.
Jackson’s practice was flooded with children who had ingested lye (Figure 8). He could not sit idly by while so many preventable accidents left children at death’s door, narrowly saved by Jackson and his endoscope. He knew that if mothers were aware of the dangers of lye, they would keep the poison out of reach of their children and take more care in thoroughly rinsing cups and containers. Warning labels were the answer. He appealed to the lye packers to voluntarily provide a warning. He was told “No such thing as a poison label can be put on my preparation unless it is put on every preparation in the market, because such a label would single out my preparation as dangerous and people would shun it in favor of unlabeled preparations. Even if all packers now in business agreed, there would be new concerns constantly bringing out unlabeled preparations. If you spent all your time at it, you could not keep up with the flood of new concerns..” 12 Legislation was clearly required. Laws were in place to label phenol and other drugs as poison, but nothing was required for household poisons.

Twelve children under treatment in the esophagobronchoscopy clinic at one time in the era before the passage of the Federal Caustic Poison Act. All had been unable to swallow food or water because of strictures from burns caused by swallowing household lye from containers that had no warning labels. They were safely over the emergency and had gained weight when this photograph was taken. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
A childhood friend of Jackson’s, George von Bonhorst and his associate Chris Magee had grown into political powerhouses in Pennsylvania, and Jackson was hopeful that he could leverage this connection to raise the issue of lye legislation before the State. However, he was told “Chev, I am sorry for the children, and I would like to help in your effort to help them; but I must tell you that you would have a long and expensive way to travel before you could get a bill like that through the State Legislature. . . Nothing but money and lots of it would get your bill up for consideration, let alone have it passed. Unless you have a wealthy philanthropist with loose purse strings to help you, don’t attempt it. Sorry, Chev, but such is Pennsylvania politics today..” 12
Chevalier Jackson was not born wealthy. His family struggled with finances his whole life, and he couldn’t bear to charge patients for his services if he felt that they couldn’t pay. He had no mind for business and estimated that 95% of his medical practice was charity. Bonhorst’s response disgusted him, but it didn’t dissuade him. He became determined to devote a large part of his life to the prevention of the causes of needless suffering. He believed that the value of “The work of physicians in prevention equals their work in curing disease..” 12 In preparation for the day when he had the resources to tackle this problem in earnest, every poisoned starving child that came to his clinic was photographed with the often-misleading label of the lye container responsible for the suffering. He continued collecting these photos for 15 years. During this time, he married a business-minded woman and became globally renowned for his endoscopic technique. The prestige brought in enough patients of means that he began to develop the wealth necessary to address the problem of poisoning in earnest.
In a post-COVID world, where a “face-to-face” meeting is a click away, it is difficult to imagine what it took to run a national campaign in the early 1900s. Travel was expensive and difficult. The first commercially successful automobile, the Model T, was not available until 1908. To achieve success, Chevalier Jackson would need to embark on multiple journeys from Pittsburgh to Washington DC and various states on horseback, by car and by train over many years. In 1910 Jackson succeeded in convincing the Pennsylvania state government to require poison labels. However, to reach other states he needed resources. He presented the problem to the American Medical Association (AMA). In 1910 he published an article first describing the public health problem. 38 He highlighted the needless starvation of children, the reckless abandon of the manufacturer and the misleading labels. He reported that he had the so-called “safe” dilute preparations chemically analyzed and found the proportions of caustic alkali to vary from 8% to up to 50%, none of which are so diluted as not to be caustic to the delicate esophageal mucosa of a child. Most importantly he brought attention to that fact that on not one of these containers was there even a hint of the dangerous nature of the contents, and no advice for the “child dying of the agonizing burns, or the subsequent ulcerative esophagitis or stricture.” Rather they were marketed as “harmless.” He called on his colleagues to take up the cause with him, and they answered.
The AMA appointed him as Chairman to organize a Committee on Lye Legislation (Figure 9). One of the efforts of the committee was to survey the lye packers to ascertain what they might be willing to do out of conscientious concern for the consumer and their children. 39 Only one responded, saying that poison labels on lye were no more necessary than a warning label on a can of soup against the danger of cutting one’s hand on the edge. This survey served as conclusive evidence that legislative regulation was necessary to ensure compliance with common sense safety precautions. Over time Jackson accrued a committee member from all 48 states in the Union (Alaska and Hawaii not admitted until 1959). Assembling the committee was only a tiny fraction of the work to be done. A national campaign was started with 2 goals: “to educate the people on the dangers of household lye, and to obtain state legislation requiring a poison label on this and similar caustics..” 40 This campaign required many letters, photographs, interviews, lectures, talks, exhibitions, and clinics. In aggregate, thousands of senators and representatives were interviewed and informed of the necessity of the proposed legislature. Running alongside this legislative gauntlet was a 25-year national educational campaign (Figure 10). There was no financial compensation for any of this work. Each committee member bore the expense in their local activities.
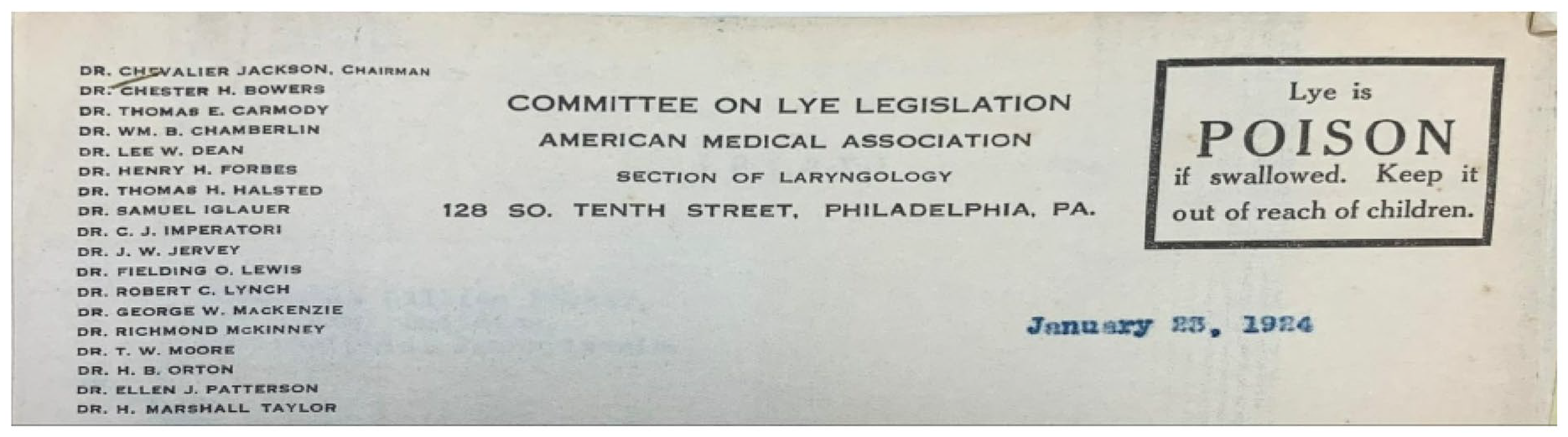
The official letter head of the Committee on Lye Legislation. The members of the committee are listed on the left. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
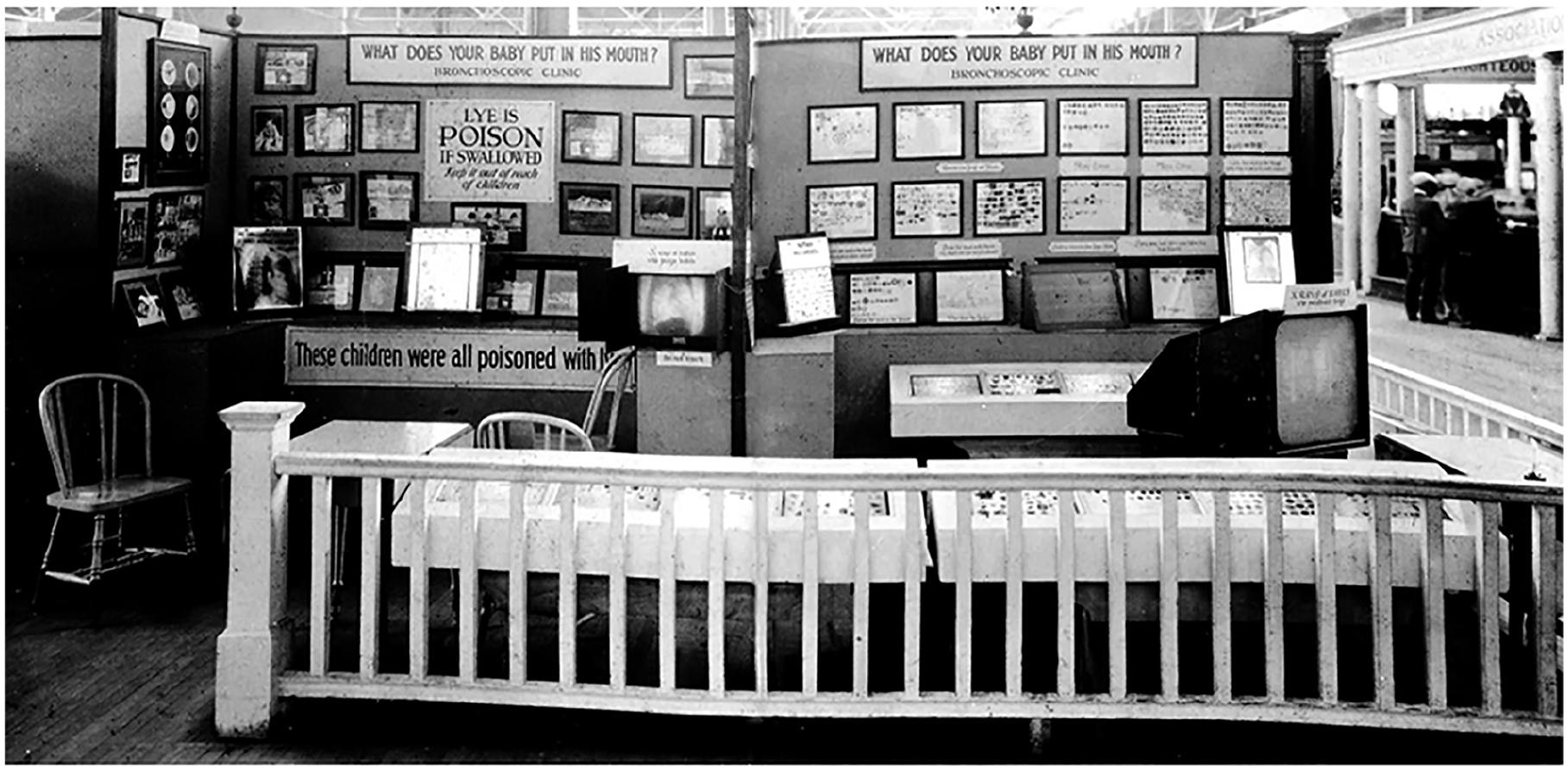
In addition to legislative change, part of the mission of the Lye Committee was public education. This public booth highlighted many of the dangers of caustic esophageal injury and also warned of the dangers of foreign body ingestion. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
While the focus of the committee was lye, the legislation they proposed applied to hydrochloric acid, sulfuric acid, nitric acid, carbolic acid (phenol), oxalic acid, oxalates, acetic acid, hypochlorous acid, potassium hydroxide, sodium hydroxide, silver nitrate, and ammonia. 9 The requirements were a conspicuous, easily legible label with the common name of the substance, the word “poison” and directions for treatment of accidental injury (Figure 11). The legislative road was not a smooth one. The bill died in many states, and entered a 2 year wait period before it could be reproposed. It took 20 years to get the law passed in only half the states. However, by 1925 two developments were noted by the Committee, which worked in their favor 1 : Local packers of household lye were being replaced by great corporations that distributed millions of packages of poison across state lines; and 2 there was increased interest by the Federal Government in controlling interstate commerce. These developments opened an avenue for Federal legislation; however, this avenue was no less tortuous. There were about 96 senators and 400 representatives that had to be reached, some in their home states and some in Washington.

Labels from early 20th century lye packers who were compliant with poison label regulations. Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
Chevalier Jackson went before Committees of Interstate Commerce in both the House of Representatives and then again for the Senate with Dr. W. C. Woodward and Dr. Charles W. Richardson. 41 Part of the struggle was convincing the legislature that a physician would willfully leave his practice and spend time and money in Washington without an ulterior motive, remarking “Evidently altruistic motives were rarely encountered” in Washington. 12 However, once he presented hundreds of photographs of children near death from hunger and thirst, along with the corresponding label showing no warning of the poisonous nature of the substance that left them in that state, they started to pay attention (Figure 12). He showed them the resemblance to sugar and highlighted that he was driven by the hundreds of children he had personally seen needlessly suffering. Once they recognized his motives as humanitarian the Chairman of the committee James E Watson an Indiana Senator said “Doctor Jackson, I cannot see from what source any objection could be raised to the enactment of such a law..” 39
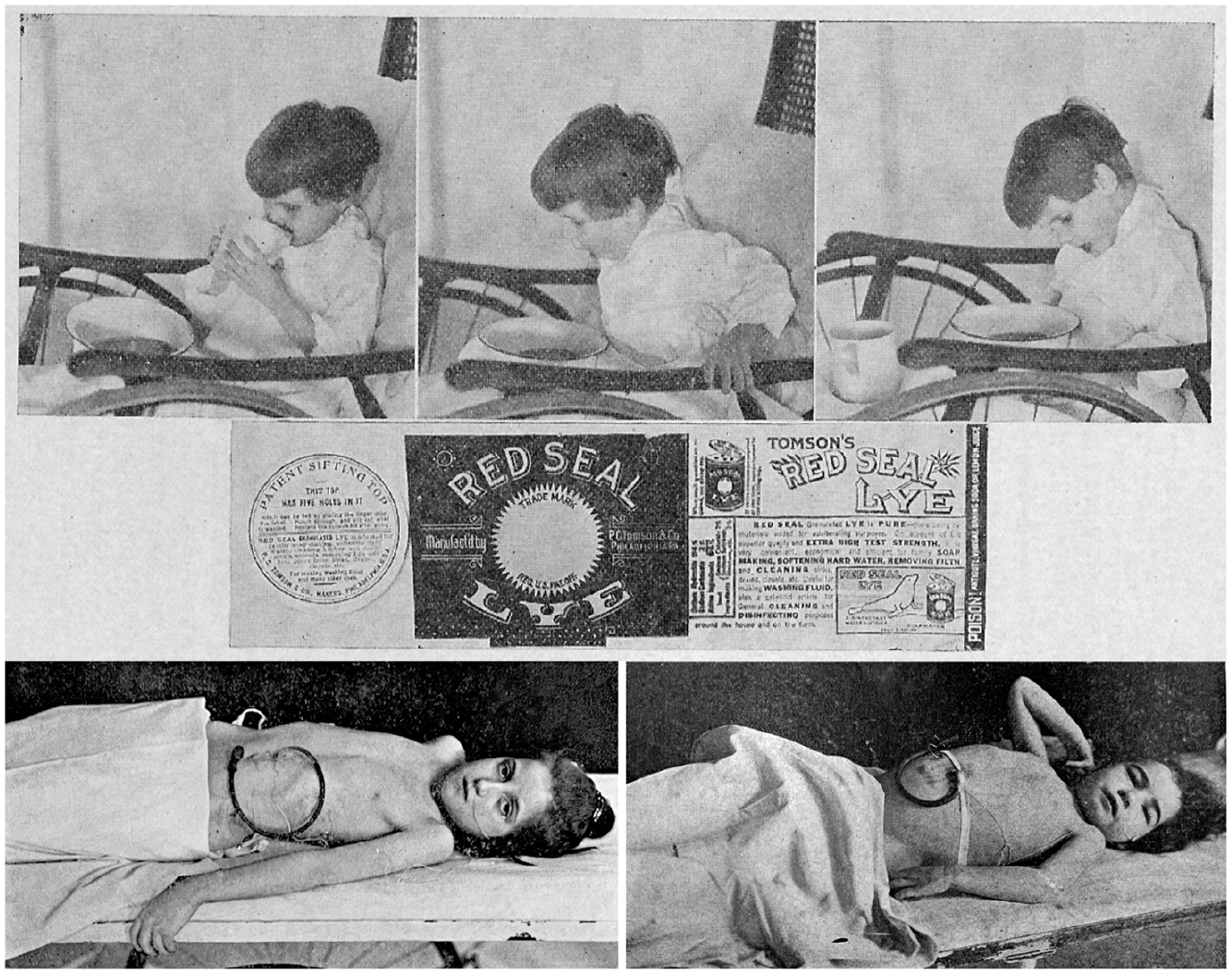
Example of the hundreds of figures presented before congress. The top photos were accompanied by the following text: “Case No L. C. 106, age 4 years, drank from a glass containing a solution of “Red Seal Lye.” This was followed by severe burns of the mouth and throat with inability to swallow any food. Later, liquids could be taken with difficulty. Esophagoscopic findings: Ulceration with cicatricial stricture. (A) Flossie, burnt with “Red Seal Lye.” Throat closed. Trying to swallow. Flossie is famished for food and dying of thirst. (B) Flossie is retching to bring up food that is lodged in the esophagus because it cannot reach the stomach through the ulcerated and scarred strictures following the lye burns. (C) Flossie, worn out with hours of piteous efforts to swallow water, gives it up and will die of hunger and thirst if not operated upon to put a rubber tube in the stomach to tide her over until the stricture in her esophagus could be opened up. After months of treatment, she was discharged improved; treatment by retrograde Tucker bougies to be continued by the family physician..” The bottom photographs were accompanied by the following text “Photograph of a child whose gullet was closed by drinking a small amount of lye solution. This photograph was taken after the child had recovered general health by feeding through the rubber tube put into the stomach by operation. She was emaciated by starvation when she came to the Hospital.” Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
Both the House and Senate committees unanimously voted in favor of the bill; however, even that did not mean smooth sailing toward enactment. In addition to opposition from the unconscientious lye packers, the pharmacists began to oppose the bill. Apothecaries in Europe and United States had begun storing poisons in distinctively shaped bottles in the 18th century, and by the late 19th century the word poison with a skull and cross bones was on every poison sold in the pharmacy. 42 The issue was that pharmacists were allowed to dispense poisons, whereas grocers generally were not. Because grocers had begun selling over the counter medicines at that point, pharmacists saw this bill as a harbinger of grocers replacing pharmacists as the dispensers of poisonous substances and medications. They succeeded in adding an amendment that would essentially nullify the efficacy of the bill. Subsequent amendments to remove this language from the legislation had to be approved. The bill endured a gauntlet of amendments and competed with other bills for attention over the course of 2 years, during which Dr. Jackson made numerous trips to Washington. Finally on March 2nd, 1927, the Federal Caustic Poison Act was signed into law by President Calvin Coolidge. The pen he used to sign the bill was sent to Chevalier Jackson as a token of appreciation for his humanitarian and public health efforts (Figure 13).
“Pen with which President Coolidge signed the Federal Caustic Act. The pen was presented to Dr. Chevalier Jackson by Dr. Charles W. Richardson as a souvenir of the ultimate success of Dr. Jackson’s prolonged efforts to obtain enactment of this piece of welfare legislation.” Photos obtained from Chevalier Jackson papers. 1890 to 1964. Located in: Modern Manuscripts Collection, History of Medicine Division, National Library of Medicine, Bethesda, MD; MS C 292.
The Impact of Lye Legislation
Less than a decade after enactment, the incidence of accidental ingestion of caustic poison dropped by 50%, and Chevalier Jackson reported a corresponding 90% decline in patients presenting to his own clinic. 43 This dramatic improvement in patient outcomes underscored the act’s immediate impact, sparing countless families from the devastating consequences of caustic esophageal injuries. Building on the tradition of physicians like John Snow, who identified and addressed the 1854 cholera outbreak through improved sanitation practices, Chevalier Jackson systematically tackled a preventable cause of childhood suffering. He demonstrated that physician-led public health reform could bring about tangible and lasting change. 44
The legislation also signified a substantial shift in societal attitudes toward consumer safety. Throughout the 19th century much of the onus of protecting the family from accidental harm fell on homemakers, who were expected to manage risks within the home. The lion’s share of cautionary information came from magazines like Good Housekeeping, which employed Harvey Wiley, a former USDA chief chemist, consumer activist, and leading advocate for the Wiley act, which prohibited adulteration of food and drugs. 42 Jackson emphasized that ignorance, not negligence, was often the root cause of accidents. A social study on accidental poisoning later corroborated Chevalier Jackson’s subjective assessment. The study found that true negligence by parents is not a common cause of poisoning; rather, many parents were unaware that numerous common household substances were poisonous until after accidents occurred. 45 Therefore, the homemaker cannot be held solely responsible for the safety of the family. By mandating poison and antidote labels, the law established that the manufacturer must bear the responsibility to warn and protect the consumer from harm. Poison labels in conjunction with Jackson’s national education campaign on the dangers of esophageal injury brought the risks of lye to the forefront of public discourse and created a high demand for nontoxic alternatives. 46 This demand served as a catalyst for innovation, with manufacturers developing safer products. The modern cleansers, detergents, shampoos and solvents that we enjoy today—most of which are actually more effective at cleaning than traditional lye-based soaps—owe their existence in part to Chevalier Jackson’s concern for his patients.
The Federal Caustic Poison Act laid the foundation for several subsequent pieces of legislation focused on protecting consumers. It influenced the 1938 Food Drug and Cosmetic Act, formalizing the FDA and granting oversight and regulatory power of hazardous products. 47 In 1947 the Insecticide, Fungicide, and Rodenticide Act, mandated colorants be added to white powdered poisons after a cook mistook insecticide for powdered milk and fatally poisoned 50 people in Oregon. 48 In the 1950s physician advocacy helped establish the poison control system. 49 Finally, in 1960 the Caustic Poison Act was expanded to become the Hazardous Substances Act, providing jurisdiction over any product deemed hazardous, defined as “toxic, corrosive, irritant, flammable, strong sensitizers or pressure generating in addition to those that may cause substantial personal injury or illness during or as a proximate result of any customary or reasonably foreseeable handing or use including reasonably foreseeable ingestion by children.”50,51 These ripple effects illustrate how Jackson’s work reshaped public health policy, establishing a legacy of physician-led advocacy that continues to inspire systemic change today.
Conclusion
The impact of the legacy of Chevalier Jackson extends across multiple avenues including healthcare, public health and modern society. This impact is exemplified in his approach to esophageal strictures. His endoscope utterly transformed the diagnosis and management from dangerous guesswork into precise methodical life-saving interventions. In the process he introduced the medical profession to what has become the most common cause of stricture today: reflux. But he did not stop there. Paying attention to prevention, he identified and described a public health crisis, bringing it to the attention of all who would listen. He sacrificed tremendous amounts of time and money in tireless advocacy for patient safety and public health. His efforts culminated in the landmark Caustic Substances Act of 1927, which paved the way for public health reform and consumer safety, showcasing the fruits of dedication to addressing the root causes of preventable harm. Jackson’s career highlights the critical interplay between clinical expertise and societal responsibility, demonstrating how a physician’s influence can extend beyond individual care to drive broader advocacy and healthcare reform. This ethos resonates today, as modern healthcare challenges demand physicians to leverage their insights and authority to address systemic issues, from health equity and affordability to patient safety. Dr. Jackson launched his career at Western Pennsylvania Hospital, where he invented the endoscope. The Chevalier Jackson Research Fellowship at AHN Western Pennsylvania Hospital honors this enduring legacy, fostering the next generation of clinician-advocates dedicated to advancing esophageal health and patient-centered care. As we reflect on Jackson’s achievements, we are reminded of the physician’s unique capacity to enact meaningful change by uniting medical innovation with a commitment to public welfare.
Footnotes
Acknowledgements
We would like to thank the National Library of Medicine and Heinz History Museum for their assistance with archival research in this work. We also would like to thank Andrew Lang, Curator of the Sunrise Mill Museum in Montgomery County, PA, for his assistance with historical research. Finally, thank you to Frank Bugbee and Sue Ruby for their unique insight into the physician who inspired this work—their great-grandfather, Chevalier Jackson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.