
Abstract
Squamous dysplasia precedes invasive squamous cell carcinoma of the esophagus, but there is limited evidence on its surgical management. The “field change effect” further complicates matters, causing multifocal or second primary neoplasms in the esophagus and upper aerodigestive tract. While endoscopic procedures are the primary treatment, surgical resection, either alone or in combination with endoscopy, must be considered given the extent of the disease and organ involvement. This chapter summarizes multifocal squamous dysplasia scenarios and highlights the role of esophagectomy or surgical resection.
Keywords
Key Learning Points
The field change effect often leads to multiple squamous neoplasms in the esophagus and head and neck region.
Endoscopic treatment is limited by the extent and technical challenges of recurrent disease, while surgical resection has a distinct role to play.
The surgical approach, combined with endoscopic therapy, varies based on the neoplasm’s location and invasiveness.
Introduction
Squamous dysplasia is a known precursor of invasive squamous cell carcinoma of the esophagus. Overall, the evidence and literature on the surgical management of esophageal squamous dysplasia are scarce. The picture is further complicated by the “field change effect,” which can lead to multifocal or second primary neoplasms in the esophagus and the rest of the upper aerodigestive tract. The primary treatment mainly involves endoscopic procedures. However, considering the extent of the disease and the organs involved, surgical resection (either as a stand-alone procedure or in combination with endoscopy) must be considered. This chapter summarizes the different scenarios of multifocal squamous dysplasia and aims to highlight the role of esophagectomy or surgical resection.
Precursor and Risk
Esophageal squamous dysplasia arises through a multifaceted process involving various environmental and physical risk factors that contribute to chronic inflammation and the intake of carcinogens, such as nitrosamines. Among these risk factors, smoking and alcohol consumption are the predominant ones, exhibiting synergistic effects. Exposure to elevated levels of acetaldehyde, which is the primary metabolite of alcohol, may contribute to an increased risk of cancer. The ALDH2 gene encodes the ability to metabolize acetaldehyde. East Asian populations have a high prevalence of the mutated ALDH2 allele, producing an inactive protein subunit that is unable to effectively metabolize acetaldehyde. An individual’s genotype at this gene locus can increase the risk of esophageal cancer by the level of acetaldehyde in their body. 1 With the advancement and availability of high-resolution or image-enhanced endoscopy, an increasing number of early neoplastic lesions can be detected either during health checks or through surveillance after treatment of primary cancers. 2 A multicenter cross-sectional study conducted in China, involving 44 857 screening endoscopies in a population screening, showed an incidence of 4.18% for low-grade intraepithelial neoplasia (LGIN) and 0.9% for high-grade intraepithelial neoplasia (HGIN). 3 Another community-based long-term study on the incidence of progression to invasive cancer from LGIN, with or without endoscopic surveillance, showed that patients with LGIN, regardless of surveillance, had a higher risk of esophageal squamous cell carcinoma (ESCC) than the general population. Patients in the surveillance group had a 31% decreased risk of ESCC incidence compared to those in the non-surveillance group, after adjusting for baseline risk factors.4,5
Indications for Surgery
The aim of surveillance or screening is to identify early treatable lesions and preserve organ function. Endoscopic resection or ablation has been proven to be highly effective in treating precancerous intraepithelial dysplasia or even early mucosal cancers. However, there are factors that limit the effectiveness of this approach. The guidelines provided by the Japanese Esophageal Society and the Japan Gastroenterological Endoscopy Society suggest that endoscopic resection may be considered as the primary treatment for non-circumferential Stage0/T1a esophageal squamous cancer. However, there are limitations for more extensive lesions, specifically those with a lesion length longer than or equal to 50 mm, and extra precautions must be taken when dealing with lesions involving the entire circumference of the esophagus. To prevent stenosis, oral prednisolone, submucosal triamcinolone injection, or a combination of oral prednisolone and submucosal triamcinolone injection is recommended when the post-resection ulcer is expected to affect ≥ 3/4 of the esophageal circumference.6,7 Despite these prophylactic measures, the rate of stenosis after resecting circumferential lesions can be as high as 55% to 100%. For whole circumferential lesions longer than 5 cm, the Japanese guidelines recommended surgery, chemoradiotherapy or radiotherapy.6,8 Another indication for surgery would be the recurrent neoplasm adjacent to or at the site of previous endoscopic treatment. In such cases, repeat endoscopic treatment would be technically demanding as the submucosal layers will have extensive scarring. A higher complication rate of perforations or incomplete resection may be expected, and it can also pose difficulties for pathologists to accurately assess the pathology. While some investigators may advocate radical chemoradiation therapy as an organ-preserving treatment for early superficial cancers, there is currently no evidence supporting its use in esophageal squamous intraepithelial dysplasia. Radiation oncologists are generally hesitant to administer a radical dose of radiation for precancerous lesions, as these lesions may often be widespread exceeding the tolerable radiation field, and are poorly localizable by radiological investigations. Multifocal dysplasia with scattered distribution along the length of the esophagus is not uncommon. Furthermore, synchronous multifocal dysplasia can also be found alongside another invasive primary lesion in the esophagus or hypopharynx, which may impact the initial treatment plan and resection area (Figure 1).
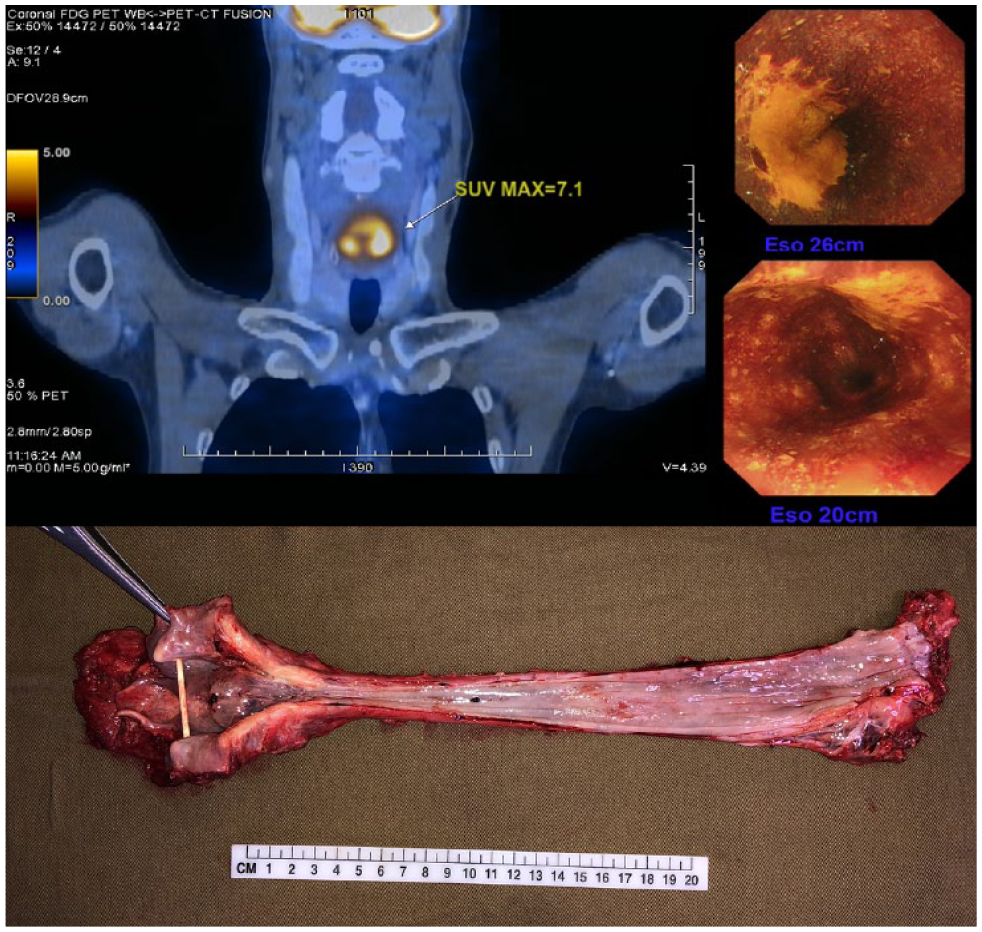
A primary advanced hypopharyngeal tumor is shown in the PET-CT scan (top left). Endoscopic images reveal synchronous multifocal esophageal squamous dysplasia at 2 0 and 26 cm from the incisors during chromoendoscopy with Lugol’s solution injection (top right). The pharyngolaryngoesophagectomy specimen displays an invasive tumor in the hypopharynx and dysplastic lesions in the mid-esophagus (bottom).
The diagnosis of intraepithelial dysplasia relies on a combination of endoscopic findings and histopathological evaluations, which are subject to operator expertise and sampling error. To improve diagnostic accuracy, endoscopic ultrasound (EUS) and magnifying endoscopy can be used to assess cancer invasion depth. The rate of upstaging from clinically diagnosed T1a-epithelial/lamina propria (EP/LPM) lesions is 7.5% with magnifying endoscopy and 16.1% with EUS (Table 1). 6 Consequently, there is still a possibility of missing invasive foci based on clinical diagnosis, Consequently, there is still a possibility of missing invasive foci based on clinical diagnosis, therefore necessitating subsequent surgery or adjuvant treatment.
Diagnostic Accuracy of Cancer Invasion Depth Using Magnifying Endoscopy and Endoscopic Ultrasound for Clinical T1a-Epithelial/Lamina Propria (EP/LPM) Lesions.

Surgical Approach
Similar to esophagectomy for diffuse early esophageal cancers that are not suitable for endoscopic treatment, a simple McKeown (3-phase) esophagectomy would provide an adequate resection margin and remove the majority of the mucosa at risk of future development of neoplasms. For true intraepithelial dysplasia, the risk of lymph node metastasis is essentially negligible, and therefore, lymph node dissection is usually not a concern. A safe peri-esophageal dissection to remove the primary lesions would be sufficient. Alternatives to McKeown esophagectomy can include transhiatal esophagectomy or eversion stripping of the esophagus. As only blunt dissection is required in the posterior mediastinum, one-lung ventilation is not necessary, making it a flexible option for patients with marginal lung function. A retrospective analysis using the American College of Surgeons National Surgical Quality Improvement Program database, with a total of 4053 transhiatal and transthoracic esophagectomies, has shown that both approaches have a similar incidence of anastomotic leakage and mortality rate, but a lower incidence of postoperative pneumonia.9,10 Eversion stripping was first described by Akiyama in 1975 as a downward extraction of the esophagus after transection at the neck. Another approach involves an upward extraction after transection of the esophagus in the abdomen. A small comparative study involving 70 patients with stripping and transhiatal esophagectomy (Orringer’s Technique) showed that stripping had a shorter operative time and lower blood loss, favoring the stripping technique.11-13
At our center, we advocate minimally invasive or robotic McKeown esophagectomy as a treatment option for multifocal esophageal dysplasia that is not suitable for endoscopic resection. Total minimally invasive or hybrid esophagectomy has consistently demonstrated a lower rate of pulmonary complications compared to open esophagectomy. Although there is no direct comparison data on minimally invasive transthoracic esophagectomy versus transhiatal esophagectomy with regard to pulmonary complications, meta-analyses have indicated a favorable trend toward minimally invasive esophagectomy. 14 On the other hand, the transhiatal approach generally has a shorter operative time.14,15 The transthoracic approach offers the advantage of mediastinal lymph node sampling or dissection, particularly when the risk of missed invasive foci is not negligible. Studies, including meta-analyses, have suggested the feasibility of sentinel lymph node mapping in early esophageal cancer.16,17 With the availability of high-resolution operative imaging systems, equipped with near-infrared fluorescent imaging, further advances are expected with this approach. Additional validation studies are still required 18 (Figure 2).
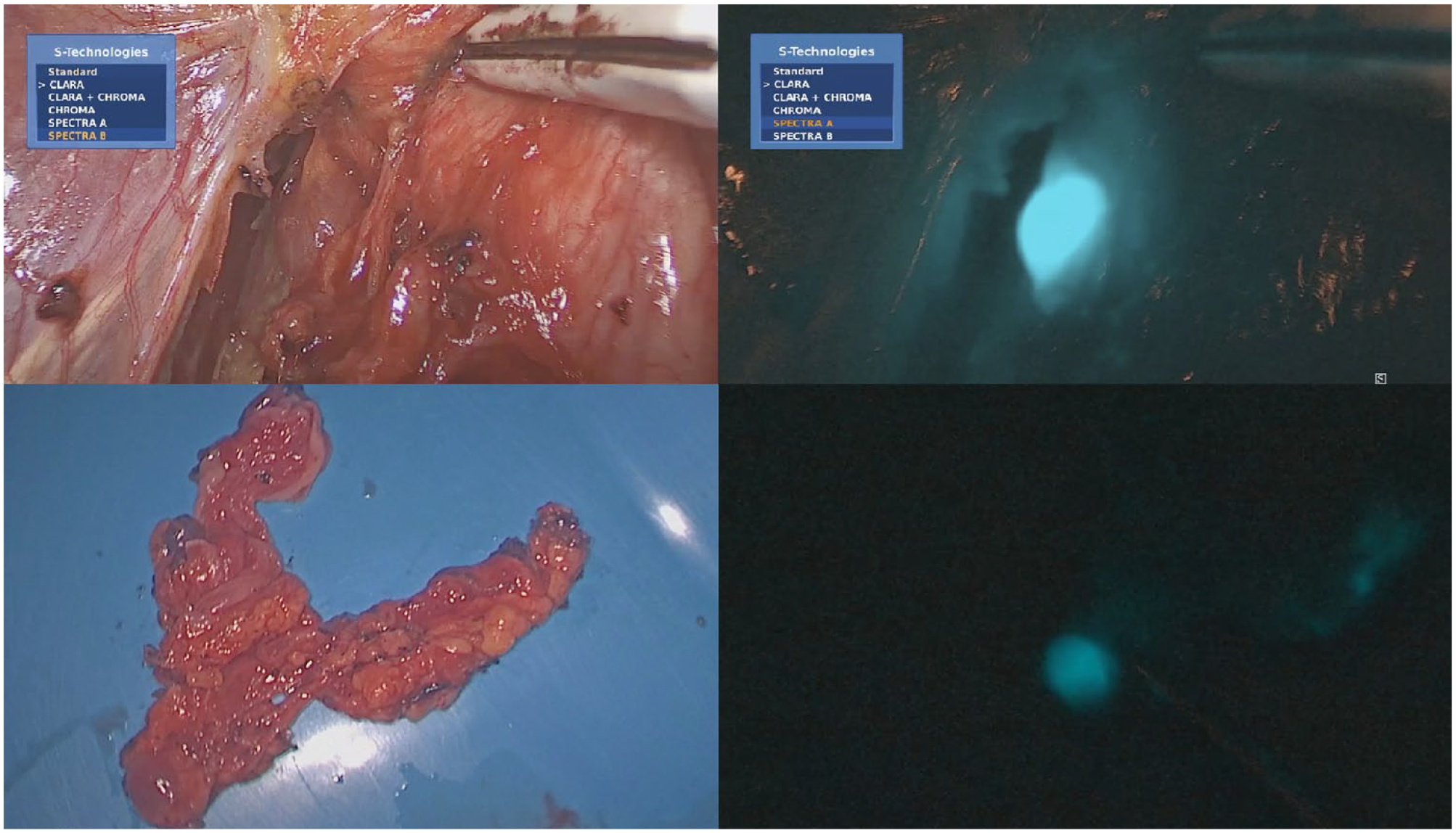
Right recurrent laryngeal nerve lymph node dissection was performed during white light videoscopic-assisted esophagectomy after peritumoral injection of indocyanine green (top left). The same surgical view was inspected using a near-infrared camera, revealing fluorescence-enhanced right recurrent laryngeal nerve lymph node (top right). An ex vivo specimen of the right recurrent laryngeal nerve lymph node basin was examined under white light (bottom left). The same ex vivo specimen was inspected using a near-infrared camera, showing the same fluorescence-enhanced right recurrent laryngeal nerve lymph node (bottom right).
Multifocal Dysplasia With Second Invasive Primary Tumor
The underlying concept of multifocal squamous dysplasia is the field change effect. These dysplasias can be detected during the workup of a primary invasive cancer and during screening for second primary neoplasms. When the primary tumor is located at the hypopharynx and there is diffuse esophageal intraepithelial dysplasia, pharyngo-laryngo-esophagectomy (PLE) would be the most oncologically appropriate option in order to achieve an adequate margin. PLE with single-staged gastric pull-up was pioneered by Ong in 1960. 19 However, this operation still carries a high morbidity rate even by current standards. The quality of the harvested gastric conduit strongly correlates with the success of the surgery. There can be a size discrepancy between the pharyngeal stump and the narrowed gastric tube. The perfusion of the conduit can be confidently assessed using real-time indocyanine green angiography.20,21 However, in situations where the conduit length is marginal, the anastomosis would be under tension, increasing the risk of leakage. In cases where obvious length discrepancy exists, we recommend a single-stage free jejunal interposition graft with microvascular anastomosis (Figure 3). Other options included free myocutaneous flaps, such as the Anterolateral Thigh (ALT) or Pectoralis Major (PM) flap, 22 or single organ pull-up, such as colonic interposition reconstruction.23,24 Another approach in managing multifocal hypopharyngeal and esophageal neoplasms would be a combination of pharyngo-laryngo-cervico-esophagectomy with endoscopic treatment for esophageal dysplastic lesions. Definitive surgery can be offered to selected patients with short-segment cervical esophageal cancer, such as patients with vocal cord palsy, where the laryngeal-preserving benefits of definitive chemoradiotherapy were less apparent, or as salvage surgery for patients who had persistent or recurrent disease after definitive chemoradiotherapy. The pharyngoesophageal defect can be reconstructed using a free jejunal flap or a tube or patch myocutaneous flap as described above. The advantage is minimizing the need for gastric pull-up, preserving the esophagus, and avoiding mobilization of the thoracic esophagus or stomach. However, the extent of esophageal dysplasia must be amenable to endoscopic treatment, preferably before pharyngo-laryngo-cervico-esophagectomy, to minimize disruption of the pharyngo-jejunal and jejuno-esophageal anastomosis during endoscopic resection or ablation. In the case of incomplete resection or disease recurrence in the remaining esophagus, completion total esophagectomy with anastomosis to the transposed jejunum or skin flap is still possible. Despite technical success, the operation is usually technically challenging, as these patients typically present late with a bulky hypopharyngeal tumor, requiring concomitant manubrium resection (64.5%) and tracheal resection (32.3%) for an adequate margin. In our center’s series, the complication rate was 25.8%, and the anastomotic leakage rate was 9.7%. The median time to swallow was 14.5 to 17 days, and the median hospital stay was 28.5 to 35 days in patients with salvage and definitive treatment, respectively. 22 We have also investigated the role of subserosal injection of Botulinum Toxin A (Botox) injection into the free jejunal flap in decreasing asynchronous contractions and improve swallowing function and transit times. 25
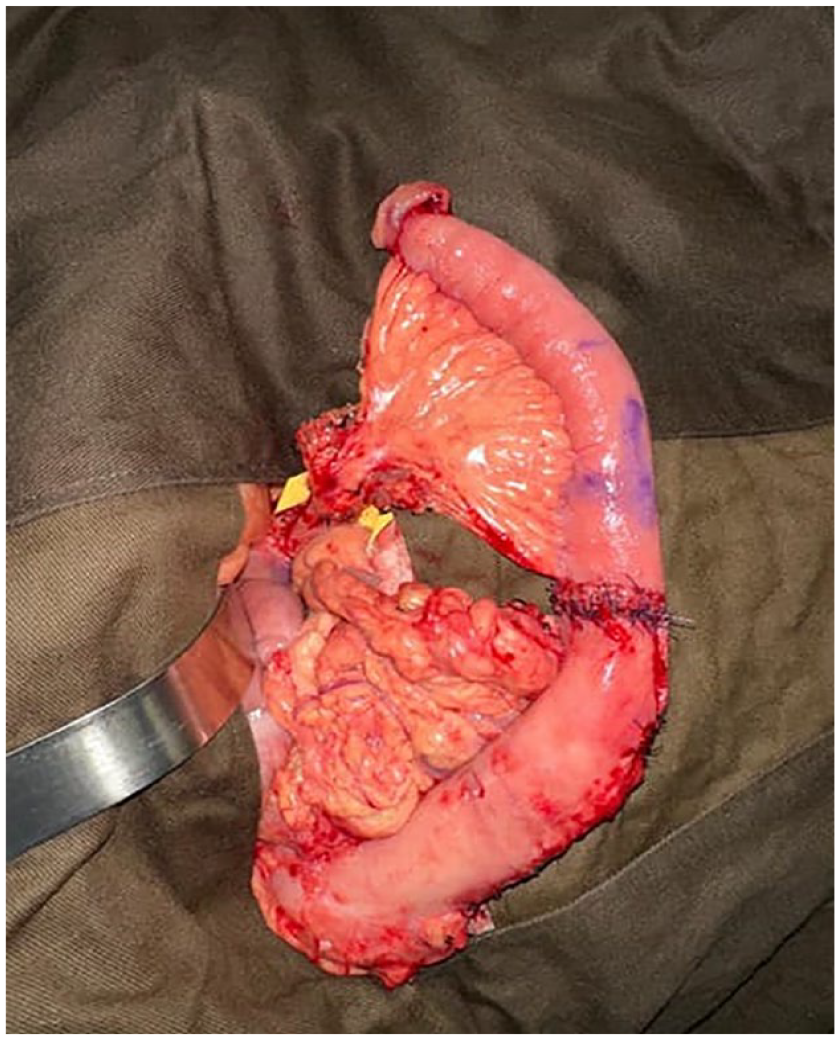
Due to the limited length of the gastric conduit for reconstruction following esophageal resection, an interposition free jejunal flap (superior) was anastomosed to a narrow gastric tube (inferior). This picture was taken before the microvascular anastomosis of the vascular pedicle and delivery to the neck.
On the other hand, where the primary invasive tumor is in the esophageal body and there is synchronous squamous dysplasia in the hypopharyngeal region, a hybrid approach combining conventional McKeown esophagectomy with complete mediastinal lymph node dissection and endoscopic laryngopharyngeal surgery (ELPS) would be appropriate.26,27 This operation involves collaboration between a head and neck surgeon and an intervention endoscopist. A special retractor is used to elevate the laryngeal apparatus (Sato retractor), providing exposure to the post-cricoid area. With appropriate retraction and dissection using micro-laryngoscopic instruments and endoscopic magnification, mucosal lesions with challenging contours can now be resected in a minimally invasive manner (Figure 4). The treatment priority is usually given to the invasive disease determined by prognosis. However, if, for logistical reasons, a formal esophagectomy needs to be postponed due to neoadjuvant therapy, ELPS is a minimally invasive procedure with a low complication rate and quick recovery.

A picture displaying the setup of Endoscopic LaryngoPharyngeal Surgery (ELPS) is shown. It illustrates the collaboration between the Otolaryngologist (left) and the Intervention endoscopist (right). A specially designed rigid curved laryngopharyngeal retractor was used to elevate the laryngeal apparatus, enabling better visualization of the post-cricoid area.
Conclusion
Currently, there is no standard treatment protocol for multifocal esophageal squamous cell dysplasia. With advancements in the quality of endoscopies, screening protocols, and the recent integration of artificial intelligence, the diagnostic and detection rates of early lesions are expected to increase. It is only with these advancements that we can conduct more impactful research on this important topic. It is crucial for intervention endoscopists and surgeons to cooperate and develop the best personalized treatment approaches for patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.