
Abstract
Introduction
Patients with gastroesophageal reflux disease (GERD) can present with a wide range of symptoms that may be typical, such as regurgitation, dysphagia, heartburn, or atypical, such as cough, pneumonia, chest pressure, epigastric pain, anemia, nausea, and others.
A comprehensive and focused history in patients with GERD should aim to identify the chief complaint and all associated symptoms. Patients with esophageal motility disorders such as achalasia are commonly misdiagnosed and treated for GERD. Likewise, esophageal dysmotility can be misdiagnosed in patients with GERD if symptoms are not carefully assessed by a thorough and detailed history.
This article aims to provide a simple, comprehensive, and focused history in patients with GERD to identify the etiology of patients’ symptoms and to guide diagnosis and treatment.
Number 1 Symptom: The Chief Complaint
Identifying the “number 1 symptom,” the chief complaint, is essential to guide diagnosis and treatment in patients with GERD.
It is important to ask patients simple and short questions that are easy to answer, such as the following:
What bothers you the most?
Is it “food or acid that comes back into your mouth?”
Is it “the sensation that the food gets stuck in your neck or chest?”
Is it “the burning sensation in your throat or chest?”
Or is it anything else?
Most patients can identify their chief complaint.
Timing of the Chief Complaint
Identifying the timing of the chief complaint is essential in guiding diagnosis and treatment in patients with GERD and can be determined by a simple question as follows:
“Do you feel worse during the day, after eating, or when you sleep at night?”
Symptoms that mainly occur during the day and after eating can be related to the presence of a defective lower esophageal sphincter (LES). Symptoms that mainly occur during the night are related to esophageal dysmotility resulting in impaired esophageal clearance in the supine position. Both daily and nocturnal symptoms indicate severe GERD associated with esophageal dysmotility or severe esophageal motility disorders such as achalasia. Nocturnal cough indicates aspiration and requires prompt assessment and treatment to prevent recurrent pneumonia and chronic lung injury.
Response of the Chief Complaint to Proton Pump Inhibitors
The response to Proton Pump Inhibitors (PPIs) is diagnostic and a predictor factor for good outcomes of anti-reflux surgery. 1 Identifying the type, dosage, and degree of response to antiacid medications is essential to diagnose and treat patients with GERD. PPIs commonly relieve symptoms of GERD; however, up to 40% of patients with GERD can develop resistance to standard PPI dose 2 and require escalating dose or another PPI.
A simple question to ask patients to assess their response to PPIs would be: “What medication do you take to relieve your symptoms, and how much that helps you?”
No response to any PPI for the duration of the disease suggests that symptoms may not be related to GERD, and other etiologies should be considered.
Symptoms Caused by Reflux Versus Symptoms Caused by Mechanical Distortion/Mass Effect of a Hiatal Hernia
An important classification of symptoms of GERD should be based on the gastroesophageal junction’s anatomy. Patients with an incompetent LES and type I hiatal hernias can present with symptoms that significantly differ from those with type III and IV hiatal hernias. Therefore, symptoms should be classified into 2 categories.
Incompetent LES and type I hiatal hernia result in symptoms such as heartburn, regurgitation, dysphagia, and cough.
Mechanical distortion and mass effect of large hiatal hernias on mediastinal structure commonly result in symptoms such as chest pain, shortness of breath, and melena, seen in patients with a large type III and type IV hiatal hernia. Most patients with type III and IV hiatal hernias do not complain of heartburn and acid regurgitation.
A thorough history can identify symptoms to distinguish between the 2 groups and guide diagnosis and treatment. Dysphagia is a common symptom in patients with all hiatal hernia types and those with esophageal motility disorders, outflow resistance, and mechanical obstruction.
Typical Versus Atypical Symptoms of GERD
Typical symptoms of GERD
Typical symptoms of GERD include regurgitation, dysphagia, and heartburn.
Regurgitation
Regurgitation, defined as the flow of food or acid in a retrograde fashion, is a common symptom in patients with GERD. Out of 256 patients who underwent primary hiatal hernia repair at our center, regurgitation as the chief complaint was seen in 34/256 (13.3%) and as a presenting symptom in 210/256 (82.0%).
Regurgitation should be classified into regurgitation of undigested food versus regurgitation of acid, as each has diagnostic and therapeutic implications:
Regurgitation of undigested food implies esophageal motility disorders, as seen in patients with achalasia.
Regurgitation of acid implies a defective LES and is commonly seen with a type I hiatal hernia.
It is essential to distinguish regurgitation from vomiting by asking patients specific questions about their symptoms. Regurgitation is not forceful, contains undigested food, and indicates esophageal disease. On the other hand, vomiting is forceful, follows a feeling of nausea, is commonly associated with abdominal pain and cramping, can contain acid or food, and indicates gastric disease.
Dysphagia
Dysphagia, defined as difficulty swallowing, is a common symptom in patients with GERD. Out of 256 patients who underwent primary hiatal hernia repair at our center, dysphagia was the chief complaint in 69/256 (27.0%) and as a presenting symptom in 195/256 (76.2%).
Dysphagia should be classified into dysphagia to solids and liquids, as each has diagnostic and therapeutic implications.
Dysphagia to solids and progressively to liquids indicates outflow resistance or mechanical obstruction at the level of LES, as seen in patients with strictures or malignancy.
Dysphagia to solids and liquids simultaneously indicates esophageal motility disorder, as seen in patients with achalasia.
Dysphagia can be classified based on its location.
Cervical dysphagia indicates diagnoses such as hypertensive upper esophageal sphincter, cricopharyngeal bar, cervical stricture, or malignancy. In addition, patients with hiatal hernia can feel referred dysphagia in the cervical esophagus.
Dysphagia in the lower chest can be caused by outflow resistance at the level of LES, as seen in achalasia, and by the mass effect of a hiatal hernia or outflow obstruction caused by stricture and malignancy.
Heartburn
Heartburn, a burning sensation in the chest, is a common symptom in patients with GERD and is caused by an esophageal injury resulting from reflux disease. Out of 256 patients who underwent primary hiatal hernia repair at our center, heartburn was the chief complaint in 69/256 (27.0%) and a presenting symptom in 184/256 (71.9%).
The presence of heartburn and its positive response to PPIs are pathognomonic of GERD. However, patients with severe GERD and Barrett’s esophagus (BE) may not feel the sensation of heartburn, as the columnar epithelium may have a protective effect against the sensation of heartburn. 3 Patients with BE may think their symptoms are improving but may have worsening GERD. Therefore, the absence of heartburn does not exclude reflux in patients with BE. Healthcare providers should obtain a comprehensive history in patients whose heartburn has progressively improved to evaluate associated symptoms and obtain diagnostic studies to assess for BE.
The burning sensation in the chest can be equally caused by esophageal distension proximal to an outflow resistance in the distal esophagus, as seen in patients with achalasia. Heartburn in these patients is misdiagnosed as reflux disease and is treated with PPI with minimal placebo response or no response.
Atypical Symptoms of GERD
Atypical symptoms of GERD can include a variety of symptoms, ranging from respiratory symptoms such as cough, shortness of breath, pneumonia, and chest pain/chest pressure to epigastric pain, anemia/melena, nausea, vomiting, weight loss, and hiccups.
Respiratory Symptoms
Respiratory symptoms such as cough, shortness of breath, and pneumonia in patients with GERD require careful attention. Cough is a nonspecific symptom and can be the chief complaint in about 4% of patients. 4 Out of 256 patients who underwent primary hiatal hernia at our center, cough was a presenting symptom in 126/256 (49.2%).
Cough associated with reflux disease is primarily dry, can be postprandial and or nocturnal, and improves with PPIs. However, patients with cough as the chief complaint need a more careful and extensive evaluation, with pH study, bronchoscopy, and CT scan of the chest to assess other etiologies, as GERD could be a diagnosis of exclusion.
Antireflux surgery is shown to improve chronic cough by about 60%, 4 but the response can be unpredictable. While reflux worsens the cough, abolishing reflux with an antireflux procedure may not completely resolve it. The absence of response to PPI in patients with cough is a sign that antireflux surgery may not improve symptoms. Furthermore, continuous cough after antireflux surgery puts patients at a higher risk of recurrent hiatal hernia. Therefore, it is essential to set expectations and explain all possibilities and risks to patients before anti-reflux surgery.
Pneumonia is suggestive of aspiration in patients with GERD and esophageal motility disorder, putting them at a higher risk of recurrent pneumonia, sepsis, and death. Recent pneumonia, associated with regurgitation and nocturnal cough, mandates prompt assessment and treatment with antireflux surgery if GERD and hiatal hernia are diagnosed and interventions to relieve the outflow resistance at the level of LES if achalasia is diagnosed.
Chest Pain and Chest Pressure
Chest pain and chest pressure are atypical symptoms of GERD caused by mechanical distortion and the mass effect of a hiatal hernia on mediastinal structures such as the heart and lungs. Chest pain and chest pressure can be equally driven by esophageal distension proximal to outflow resistance at the level of LES, as seen in patients with achalasia. Cardiac etiologies should be ruled out in all patients with chest pain and pressure.
Abdominal Pain
Epigastric pain is common in patients with GERD and hiatal hernia and is caused by the mass effect of a hiatal hernia and possible gastritis or erosions in the fundus of the stomach (Cameron erosions). On the other hand, the right upper quadrant is rare in patients with GERD. In the presence of right upper quadrant pain, an abdominal ultrasound should be obtained to rule out cholelithiasis. If gallbladder disease is the leading cause of the patient’s symptoms, laparoscopic cholecystectomy should be performed first, and the patient’s symptoms should be reassessed after cholecystectomy. If gallbladder disease is a concomitant symptom, cholecystectomy can be planned at the time of antireflux surgery.
Melena/Anemia
Anemia is common in patients with type III and IV hiatal hernias and is caused by mechanical distortion created by organoaxial volvulus and Cameron erosions seen in the fundus of the stomach. In our series of 256 patients who underwent primary hiatal hernia repair, anemia was seen in 56/256 (21.9%) and melena in 7/256 (2.7%). Bleeding in patients with type III and IV hiatal hernias is chronic, slow, and may not manifest as hematemesis. Therefore, patients may not have symptoms until the Hgb level reaches a critical level, and they may present with chronic fatigue and syncopal episode.
Nausea and Vomiting
Nausea and vomiting are atypical symptoms that can be associated symptoms in patients with GERD. The presence of nausea, vomiting and early satiety as chief complaints suggest delayed gastric emptying and gastroparesis that mandates a gastric emptying study before antireflux surgery.
Weight Loss
Weight loss is uncommon in patients with GERD. Out of 256 patients who underwent primary hiatal repair at our center, weight loss was seen in 24/256 (9.4%). Weight loss, as the chief complaint, should alert healthcare givers to suspect other etiologies, such as outflow resistance at the level of LES seen in patients with achalasia, mechanical obstruction caused by malignancy, or other etiologies, such as gastroparesis.
Hiccups
Hiccups are uncommon in patients with GERD and can be associated with a hiatal hernia, mainly if they are worse in the postprandial period. However, they may or may not improve by repairing a hiatal hernia. On the other hand, hiccups can contribute to a recurrent hiatal hernia because of the pressure applied to the diaphragm. Therefore, the risk of recurrent hiatal hernia in patients with hiccups should be discussed with patients who undergo hiatal hernia repair.
Careful attention should be paid to patients who do not have a hiatal hernia and who present with hiccups as the chief complaint unrelated to food intake. Further studies should be conducted in those patients to assess diaphragmatic function, phrenic nerve integrity, or a possible diaphragmatic mass. In patients with hiccups as the chief complaint, maximum medical management should be attempted before any antireflux surgery is considered.
Diarrhea and Constipation
Diarrhea and constipation should be assessed carefully in patients with GERD. In addition, the possibility of diseases such as inflammatory bowel disease should be evaluated. Diarrhea can occur following anti-reflux surgery, which is temporary in most cases and is mostly related to a full liquid diet recommended for about 2 weeks following the procedures. Diarrhea can be exacerbated following antireflux surgery if it is present before surgery. Therefore, the low risk of postoperative diarrhea and the possibility of exacerbation should be discussed with patients before an antireflux procedure.
Constipation should be avoided, as any straining can be associated with an increased risk of a recurrent hiatal hernia which should be discussed and reinforced with patients before antireflux surgery.
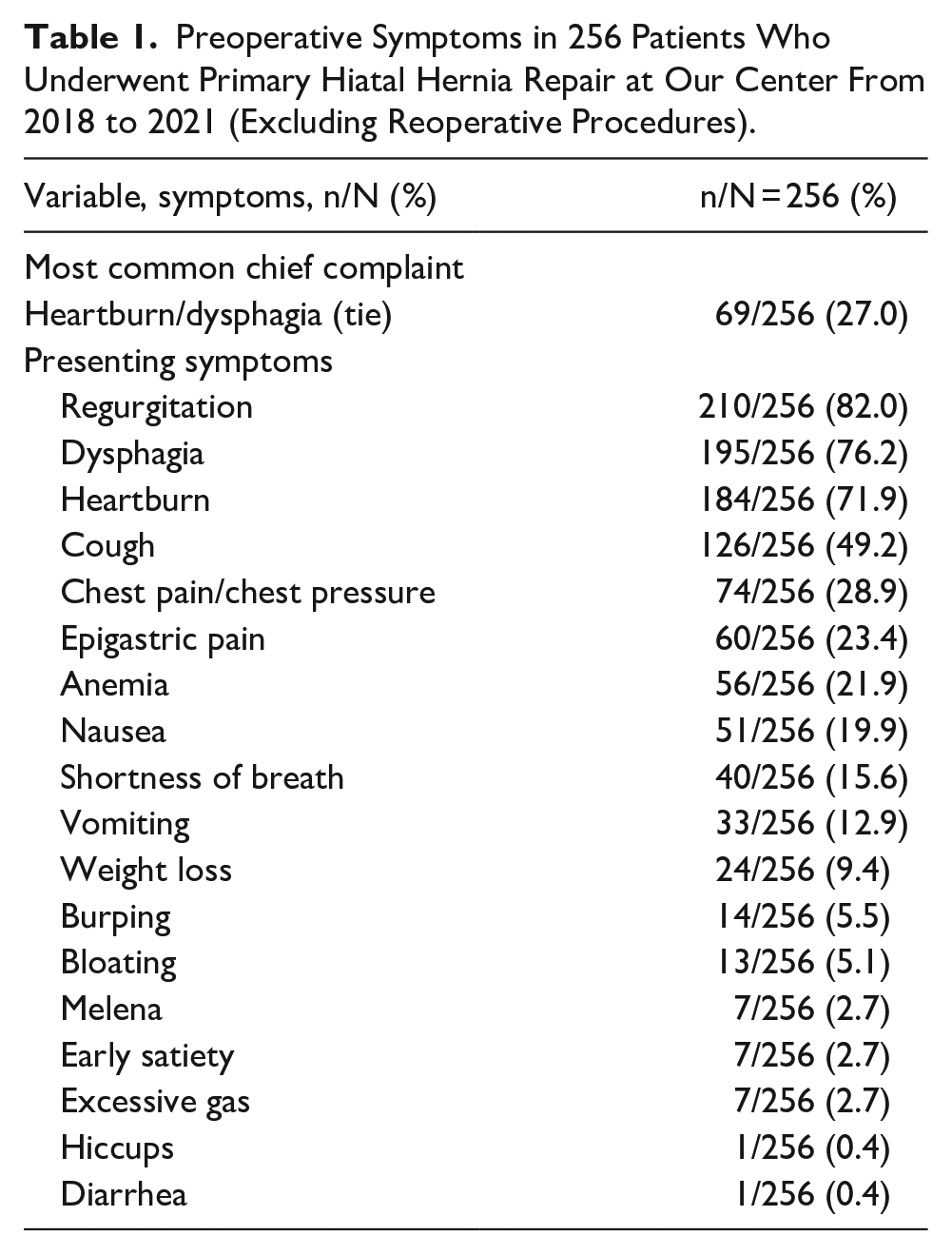
The prevalence of symptoms of GERD in 256 patients who underwent primary hiatal hernia repair at our center from 2018 to 2021 and whose outcomes were previously reported, 5 are shown in the Table 1.
Preoperative Symptoms in 256 Patients Who Underwent Primary Hiatal Hernia Repair at Our Center From 2018 to 2021 (Excluding Reoperative Procedures).
Presentation of Symptoms in the Emergency Setting
The presenting symptoms of patients with GERD and hiatal hernia in an emergency setting can significantly differ from those in the elective setting. Patients do not present to the emergency room because of typical symptoms of GERD, such as heartburn, regurgitation, and dysphagia. Instead, the symptoms in the emergency setting can include acute onset of nausea, non-bilious vomiting, coffee-ground emesis, severe chest and abdominal pain, and melena. These symptoms suggest obstructive organoaxial volvulus, perforation, and bleeding, as seen in patients with type II-IV hiatal hernias. Therefore, it is crucial that when a patient presents to the emergency room, history be directed toward life-threatening symptoms that mandate prompt upper endoscopy and surgical intervention.
It’s equally essential to discuss with patients with type II-IV hiatal hernias who are seen in the elective setting that they are at risk of major complications and life-threatening conditions such as obstructive organoaxial volvulus, perforation, and bleeding. Therefore, if they develop nausea, non-bilious vomiting, coffee-ground emesis, severe chest and abdominal pain, and melena, they should immediately present to the emergency room.
A template for a comprehensive and focused history at the time of the clinic visit is shown in Figure 1.
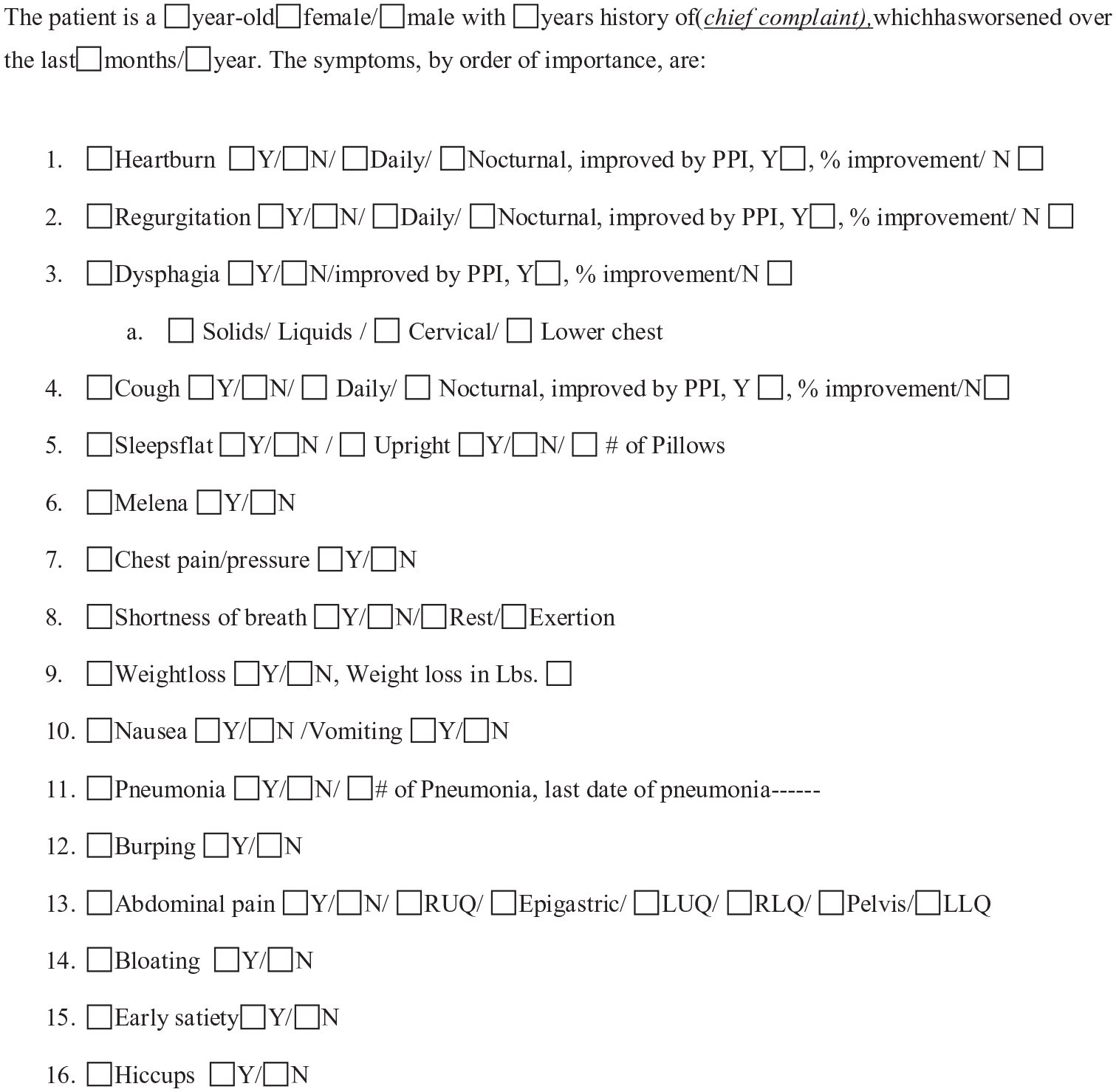
A template for a focused and comprehensive questionnaire to assess GERD symptoms.
Past Medical History
There are elements in the past medical history pertinent to diagnosing and treating patients with GERD. The presence of inflammatory bowel disease can create abdominal pain that is unrelated to GERD and will not improve after antireflux surgery. Right upper quadrant pain suggest gallbladder disease and should be assessed carefully before antireflux surgery.
Multiple Pregnancies
The number of pregnancies is pertinent to the etiology and the risk of recurrent hiatal hernia. The higher risk of recurrence in patients who had multiple pregnancies should be discussed with patients at the time of initial consultation. In addition, it should be emphasized that those patients should pay careful attention to prevent heavy lifting following surgery which is an additional risk for recurrent hiatal hernia. 6
Past Surgical History
Pertinent surgical histories that may alter outcomes of antireflux surgery should be part of a comprehensive history in patients with GERD. Abdominoplasty increases the intra-abdominal pressure and is associated with an increased risk of recurrent hiatal hernia, as we previously reported. 6 In addition, during laparoscopic surgery, the working space is smaller, and a higher insufflation pressure is required to achieve abdominal distention. Therefore, patients may have a higher chance of postoperative shoulder pain, which should be discussed with patients before antireflux surgery.
Umbilical hernia repair with mesh may need lysis adhesion that may increase the length the operation in laparoscopic hiatal hernia repair and may result in bowel injury or bleeding. However, none of the patients who underwent laparoscopic hiatal hernia repair at our center required conversion or had complications related to umbilical hernia repair.
Lastly, it is important to ask patients if they have undergone a prior hiatal hernia repair and examine the abdomen carefully for prior scars.
Diagnostic Studies Based on History
Esophagram and upper endoscopy are complementary studies and should be obtained in all patients with symptoms of GERD. Esophageal manometry, pH study, gastric emptying study, CT scan, or bronchoscopy are obtained selectively based on the patient’s symptoms.
We do not routinely obtain esophageal motility or pH study in patients with type III and IV hiatal hernias. However, esophageal manometry is obtained when severe dysmotility and the delayed passage of contrast through the gastroesophageal junction on esophagram are suspicious for achalasia.
In patients with cough as the chief complaint, we obtain a pH study in all patients. If the cough doesn’t respond to PPI therapy, we suggest a more extensive evaluation, with bronchoscopy and CT scan of the chest, to assess other etiologies, as GERD may not be the etiology or could be the diagnosis of exclusion in these patients.
An algorithm for diagnostic studies based on history is shown in Figure 2.
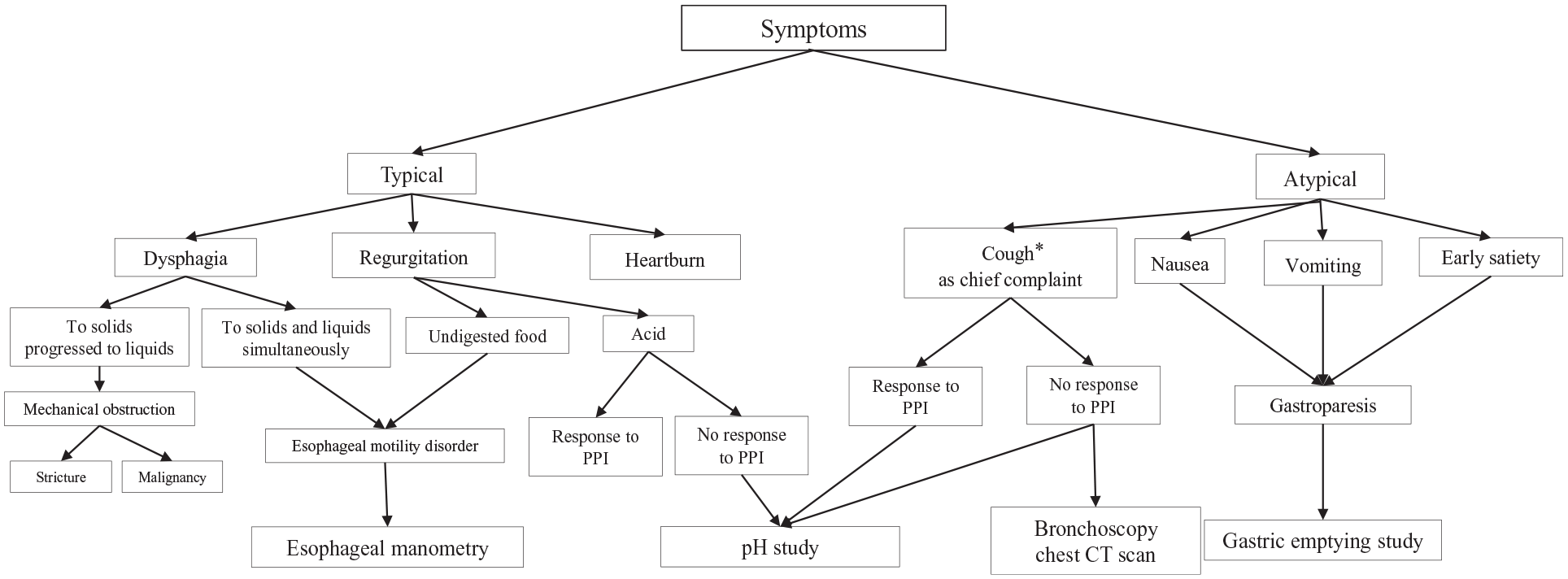
An algorithm to obtain history and guide diagnostic studies in patients with gastroesophageal reflux disease.
Summary
A thorough and focused history can identify the etiology and guide diagnoses and treatment in the majority of patients with gastroesophageal disease. Spending time listening to patients’ complaints and following a systematic template to assess all symptoms, timing, and response to PPIs are crucial. Distinguishing typical versus atypical, GERD symptoms from those associated with esophageal motility disorders, esophageal from gastric symptoms, and reflux symptoms versus those related to mechanical distortion and the mass effect created by a large hiatal hernia are essential to a comprehensive history and will guide diagnosis and treatment.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.