
Abstract
Background:
Esophageal inlet patch (IP) refers to heterotopic gastric mucosa in the cervical esophagus. Secretions from IP may produce symptoms of laryngopharyngeal reflux (LPR) and accelerate progression of lung disease. We aimed to characterize the significance of IP among patients with advanced pulmonary disease, including lung transplant (LTx) recipients, and to assess outcomes following IP ablation.
Methods:
We established and reviewed a prospective database of all patients with advanced pulmonary disease referred for GI motility evaluation for presence of IP over 7 years. Total IP size, results of pH testing, incidence of transplant rejection and mortality, and effects of IP ablation on symptoms were analyzed.
Results:
Twenty-seven (13 LTx recipients) of 440 pulmonary patients referred for upper endoscopy were found to have IPs, and 14 completed IP ablation (mean number of 1.7 sessions to ablate IP). Total IP size correlated with total acid exposure time (P = .01) and symptoms of cough (P < .00001), heartburn (P = .0001), and globus (P < .00001). Symptom severity of heartburn and dysphagia improved following IP ablation (P = .04 and 0.008). Eight of 13 LTx patient with IP developed either acute or chronic rejection, with 3 cases of post-LTx mortality occurring in patients who did not undergo IP ablation.
Conclusions:
IP should be given careful consideration in patients with advanced pulmonary disease and lung transplant recipients, particularly if symptoms of cough, heartburn, or globus are present. Total IP size may be predictive of severity of LPR, and symptom recurrence should prompt re-examination for residual IP.
This is a visual representation of the abstract.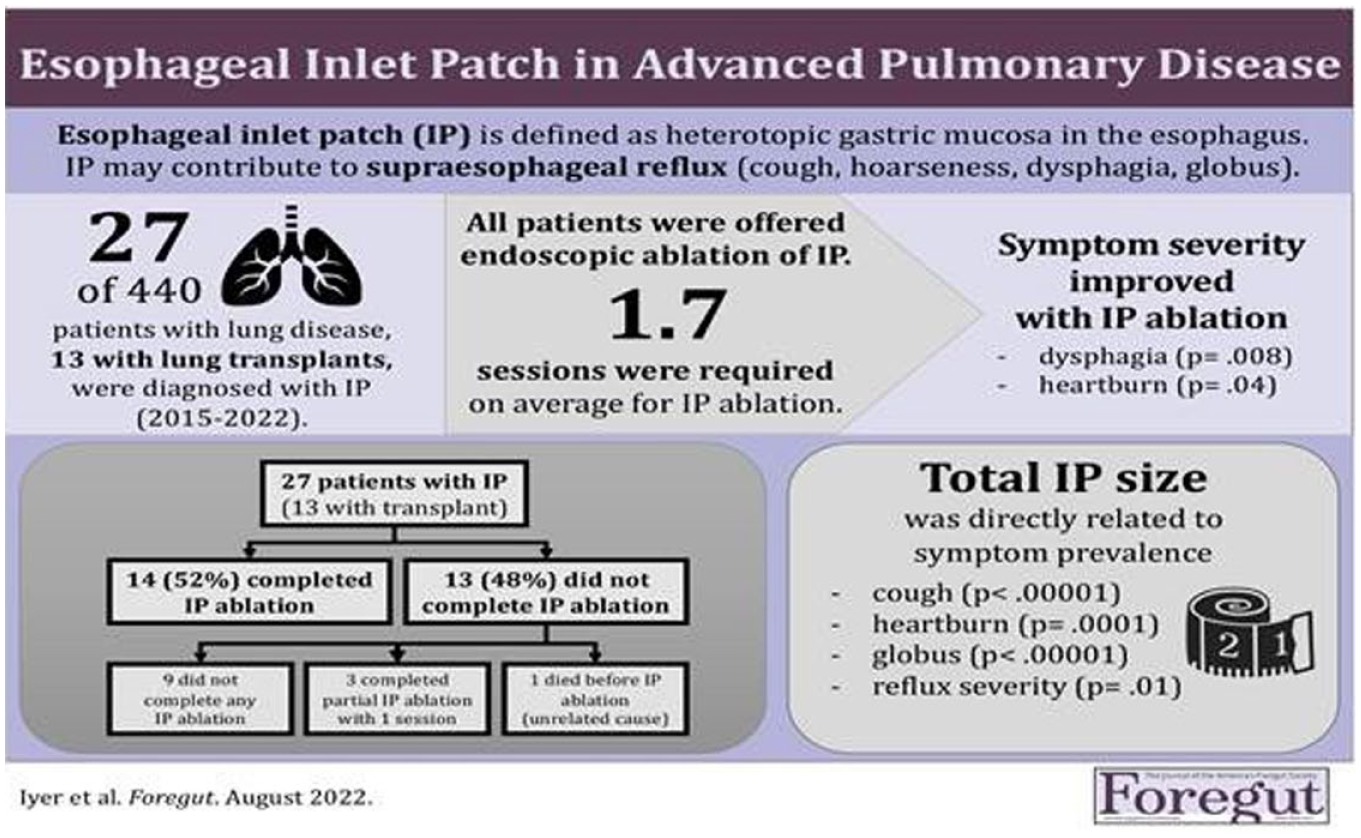
Keywords
Key Learning Points
Esophageal inlet patch was associated with pharyngoesophageal symptoms among patients with advanced lung disease and transplant.
Larger total inlet patch size predicts a higher number of pharyngoesophageal symptoms.
Inlet patch ablation may reduce severity of key symptoms in patients with advanced lung disease and transplant such as heartburn and dysphagia
Background
Esophageal inlet patch (IP) refers to heterotopic gastric mucosa that may be present in the cervical esophagus, near the larynx and airway. The reported prevalence of IP in the general population varies widely from 0.18% to 14%, however IP may be underdiagnosed by routine white light endoscopy. 1 Identification of IP, especially smaller lesions (<5 mm), is enhanced by careful examination of the proximal esophagus with utilization of narrow band imaging. 2
Our understanding of the clinical significance of IP among patients with pharyngoesophageal complaints continues to evolve. Secretions from IP lesions, such as pepsin and hydrochloric acid, may produce symptoms of laryngopharyngeal reflux (LPR) because of the proximal location of the IP. LPR is defined as reflux above the level of the upper esophageal sphincter, resulting in cough, hoarseness, dysphagia, and/or globus sensation. In a prospective cohort study of 65 patients with IP, the majority experienced heartburn or acid regurgitation (51%), followed by dysphagia (17%), cough (14%), and globus sensation (6%). 3
Patients with IP also have significantly increased pathologic gastroesophageal reflux disease (GERD) compared to age-matched controls including significantly increased proximal esophageal acid exposure, consistent with LPR. They are more likely to develop respiratory symptoms including hoarseness, cough, stridor and shortness of breath. 4 Previous studies have shown a strong association between lung disease and GERD with a high incidence of GERD seen in ILD, COPD, asthma and other lung diseases compared to healthy controls.5 -7 GERD is also associated with worse symptoms, higher frequency of respiratory exacerbations, rapid rate of disease progression and mortality. Animal studies have shown that aspiration of gastric contents can cause or accelerate pulmonary fibrosis. 8 Chronic alveolar injury from acidic refluxate may accelerate progression of lung disease and contribute to acute rejection among lung transplant (LTx) patients and progression to bronchiolitis obliterans syndrome (BOS).9,10 Higher bronchoalveolar lavage fluid pepsin concentrations were found in post lung transplant patients with IPF compared to other lung diseases and correlated with high frequency of acute rejection.11,12 The significance of IP has not been previously investigated in this population. The eradication of IP and thereby prevention of chronic micro-aspiration of acidic secretions may play an important role in improving the outcomes of patients with advanced lung disease and lung transplant.
Eradication of IP lesions can be accomplished endoscopically by argon plasma coagulation (APC) or radiofrequency ablation (RFA). A randomized controlled trial of APC versus sham ablation demonstrated improvement in chronic globus in 76% of patients with IP. 13 In a follow up study (mean follow up 27 months), the majority (74%) of patients who underwent APC ablation for globus sensation continued to report symptomatic relief. In addition, those with recurrent IP experienced a significant relapse in symptoms. 14 A smaller study with RFA produced similar results for chronic globus, as well as improvements in sore throat and cough, over a median follow up period of 15 months. Given the strong association of IP and chronic globus, IP is now mentioned in the Rome IV evaluation of globus sensation. 15
In this study, we aim to report on the clinical significance of IP in patients with advanced pulmonary disease and lung transplant and the effects of IP ablation on symptoms and incidence of transplant rejection.
Methods
We conducted a retrospective review of a prospectively maintained database of all patients with advanced pulmonary disease referred for upper endoscopy and ambulatory pH monitoring to the University of California, San Diego GI motility program from 2015 to 2022. Patient recruitment and research interventions were conducted in accordance with the university’s Human Research Protections Program and approved by Institutional Review Board (protocol 200054).
All patients underwent upper endoscopy with careful examination of the proximal esophagus via narrow band imaging to enhance detection of IP lesions. Total net size of IP lesions was determined by the summative diameter of all IP islands (small: ≤5 mm, medium: 6-8 mm, large: ≥9 mm). Ambulatory pH monitoring (96-hour wireless pH recording system) captured the percent acid exposure time off acid suppression. Presence and severity of pathologic GERD was graded by percent total acid exposure time (<4%: physiologic GERD; 4%-6%: borderline; 6%-10% mild-moderate; ≥10%: severe pathologic GERD).
Baseline characteristics of patients with IP, including age, BMI, pulmonary diagnoses, and symptoms (including cough, heartburn, dysphagia, hoarseness, and globus pharyngeus) were recorded. The relationships between IP size and pharyngoesophageal symptoms were analyzed and reported as Pearson’s correlation coefficients. All patients with IP on endoscopy were offered APC ablation. Changes in symptoms (heartburn, cough, hoarseness, globus sensation) were analyzed before and after ablation, if performed, using Fisher-Freeman-Halton exact probability tests. For LTx recipients, mortality and time to allograft rejection, if present, were analyzed and correlated with IP size and percent total acid exposure time on pH testing.
Results
A total of 440 patients with pulmonary comorbidities were referred for upper endoscopy over the study timeframe. Of these, 27 patients (12 women, mean age 58 years [20-78], mean BMI 27.1 kg/m2 [19.0-41.0]) were found to have IP on endoscopy. Based on summative IP diameter, 10 patients had small IPs, 8 had medium IPs, and 9 had large IPs. Thirteen patients had either single (3) or bilateral (10) lung transplants (LTx), including 1 heart-lung transplant. The pulmonary diagnoses of patients with IP are depicted in Figure 1, including 3 with diagnosis of alpha-1 anti-trypsin deficiency.
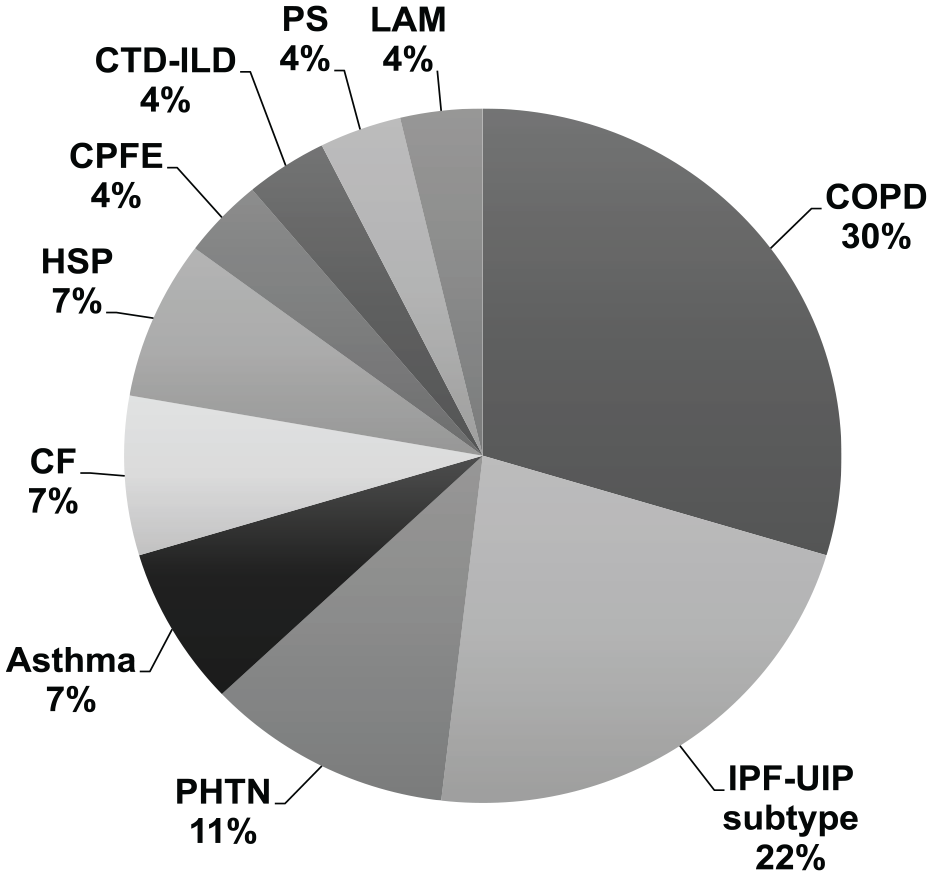
Pulmonary diagnoses of patients with esophageal inlet patch (n = 27). The majority (30%) of pulmonary patients with inlet patch (IP) had a diagnosis of chronic obstructive lung disease (COPD), including 2 with alpha-1 antitrypsin (A1AT) deficiency. Another patient with IP and asthma also was diagnosed with A1AT deficiency. Other advanced lung diseases represented in this study include: usual interstitial pneumonia (UIP) subtype of idiopathic pulmonary fibrosis (IPF); pulmonary hypertension (PHTN, including 2 with pulmonary arterial PAH and 1 with PHTN due to congenital heart disease); cystic fibrosis (CF)-related bronchiectasis; hypersensitivity pneumonitis (HSP); combined pulmonary fibrosis-emphysema (CFPE); connective tissue disease-related interstitial lung disease (CTD-ILD); pulmonary sarcoidosis (PS); and lymphangiomyomatosis (LAM).
The majority of patients had been prescribed pharmacologic acid suppression prior to referral for upper endoscopy (13 on proton pump inhibitors [PPIs], 4 on H2 receptor blockers [H2Bs], 1 on PPI and H2B). Twenty-six of the 27 completed ambulatory pH monitoring off acid suppression. Sixteen were diagnosed with pathologic GERD (4 borderline, 7 mild-moderate, 5 severe), and 10 with physiologic GERD. Reflux severity directly correlated with IP size (r = .49, P = .01). Results of ambulatory pH monitoring and preceding LPR symptoms are presented in Table 1.
Study Interventions and Results of Ambulatory pH Monitoring in Patients With Esophageal Inlet Patch (n = 27).
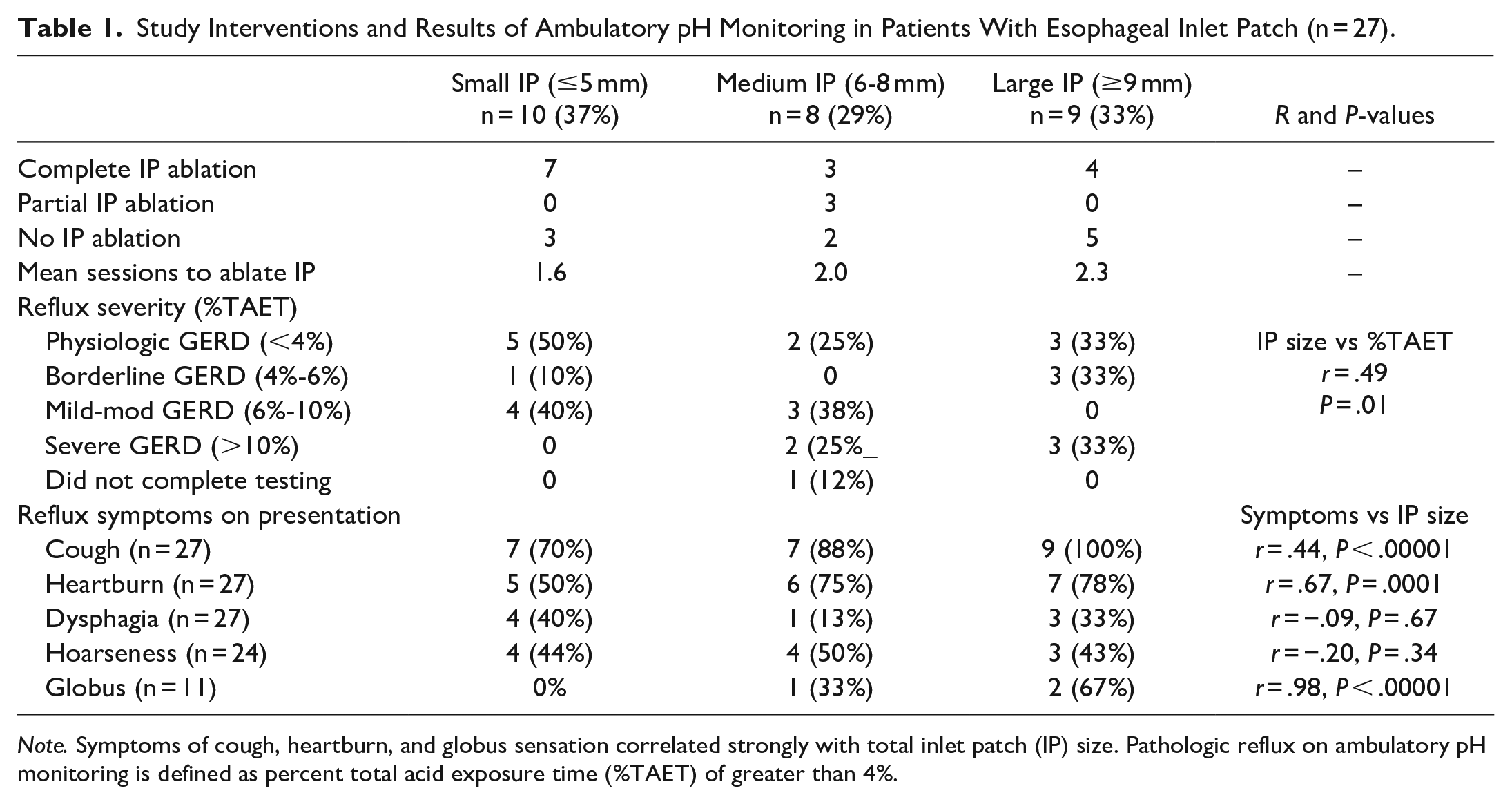
Note. Symptoms of cough, heartburn, and globus sensation correlated strongly with total inlet patch (IP) size. Pathologic reflux on ambulatory pH monitoring is defined as percent total acid exposure time (%TAET) of greater than 4%.
Of the 27 patients with IP, 14 (52%) underwent complete eradication of IP with APC ablation, including 8 LTx recipients. The mean number of sessions required for complete IP ablation overall was 1.7, with more sessions needed for ablation of large IP. Four patients declined IP ablation, while an additional 5 patients deferred ablation while undergoing further pulmonary evaluation. One LTx patient died prior to IP ablation from an unrelated cause (drowning). Three patients underwent only one ablation session but did not follow up for complete eradication of all IP tissue. The study interventions, including IP ablation and acid reflux status of patients, are illustrated in Figure 2.
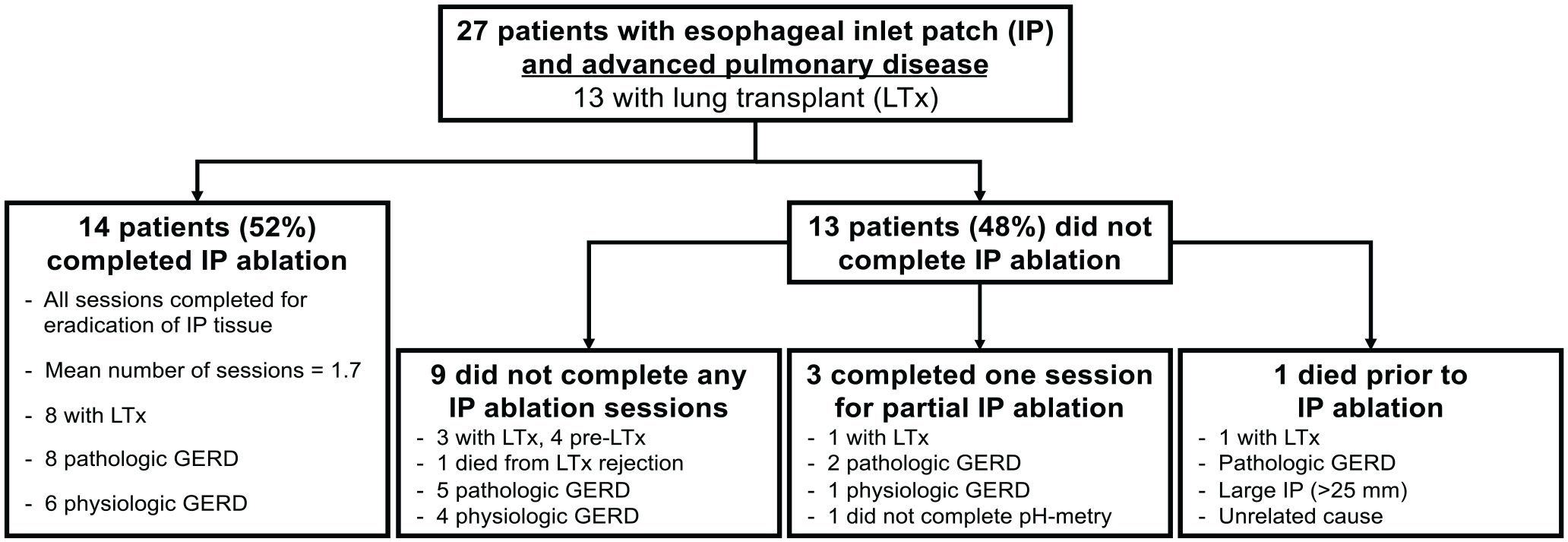
Study interventions and results of ambulatory pH monitoring in patients with esophageal inlet patch (IP). Pathologic reflux on ambulatory pH monitoring is defined as total acid exposure time of greater than 4%.
The most prevalent LPR symptoms prompting GI referral were cough (85%) and heartburn (67%), followed by hoarseness (41%) and dysphagia (30%). Globus sensation was least frequently reported, with only 11% of patients identifying this symptom. Total IP size was directly associated with the symptom of cough (r = .77, P ≤ .00001) and heartburn (r = .67, P = .0001), but not dysphagia (r = −.09, P = .67) or hoarseness (r = −.20, P = .34). Although globus sensation was not commonly reported, this symptom also correlated with large IP size (r = .98, P ≤ .00001).
APC ablation had variable effects on symptoms in patients with IP. Notably, improvement in the symptom of heartburn and dysphagia were observed only among patients who underwent complete IP ablation (P = .008 and 0.04, respectively). Among patients with physiologic GERD, 83% experienced improvement in the symptom of cough with complete IP ablation, compared to 40% among those with pathologic GERD (P = .14). Other pharyngoesophageal symptoms, including cough, hoarseness, and globus, improved with complete IP ablation, although not to a statistically significant degree, as shown in Tables 2 and 3.
Changes in Reflux Symptoms With Complete Ablation Compared to Partial or No Inlet Patch Ablation (n = 27).
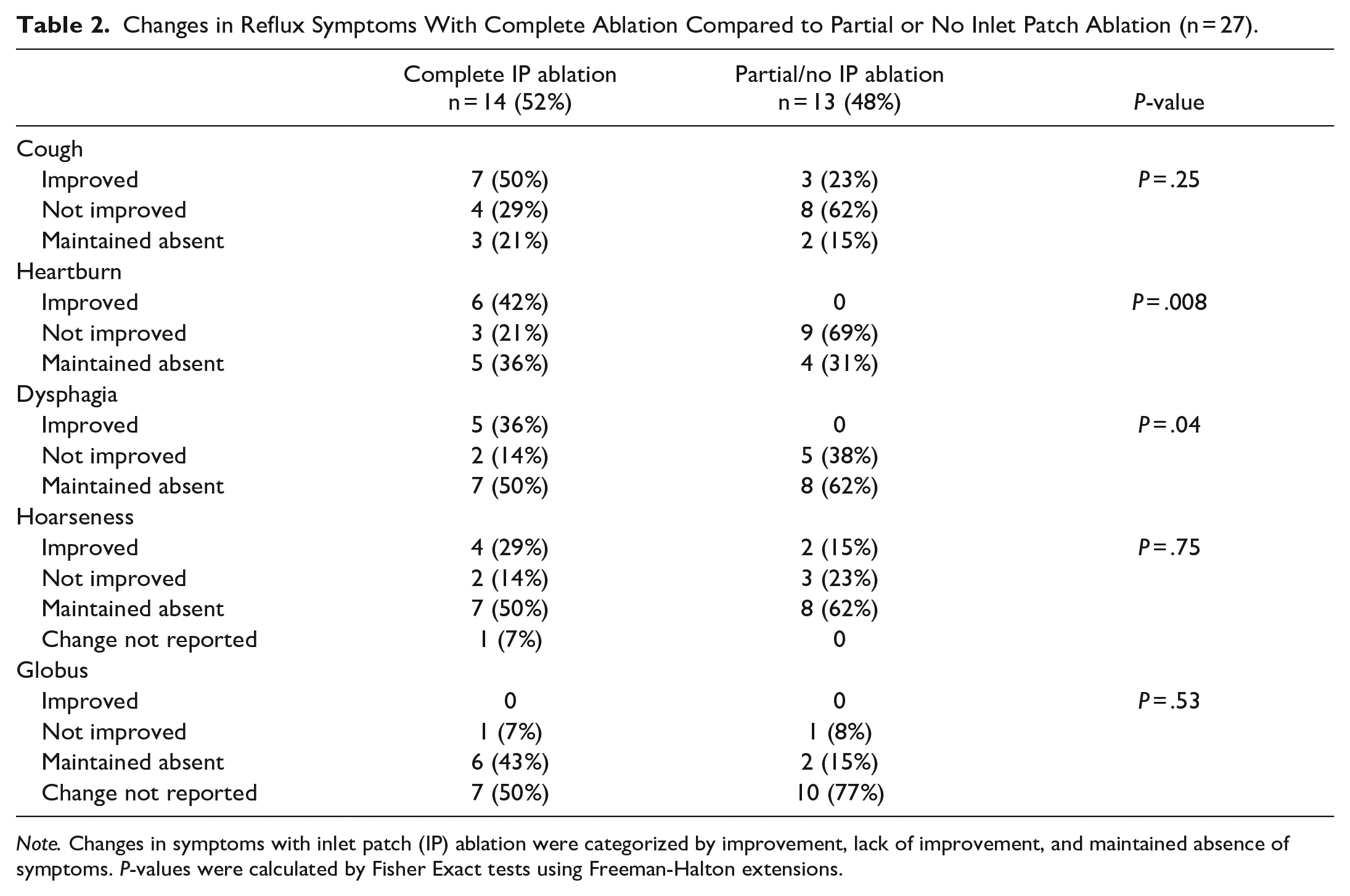
Note. Changes in symptoms with inlet patch (IP) ablation were categorized by improvement, lack of improvement, and maintained absence of symptoms. P-values were calculated by Fisher Exact tests using Freeman-Halton extensions.
Changes in Reflux Symptoms Based on Reflux Status With and Without Inlet Patch Ablation.
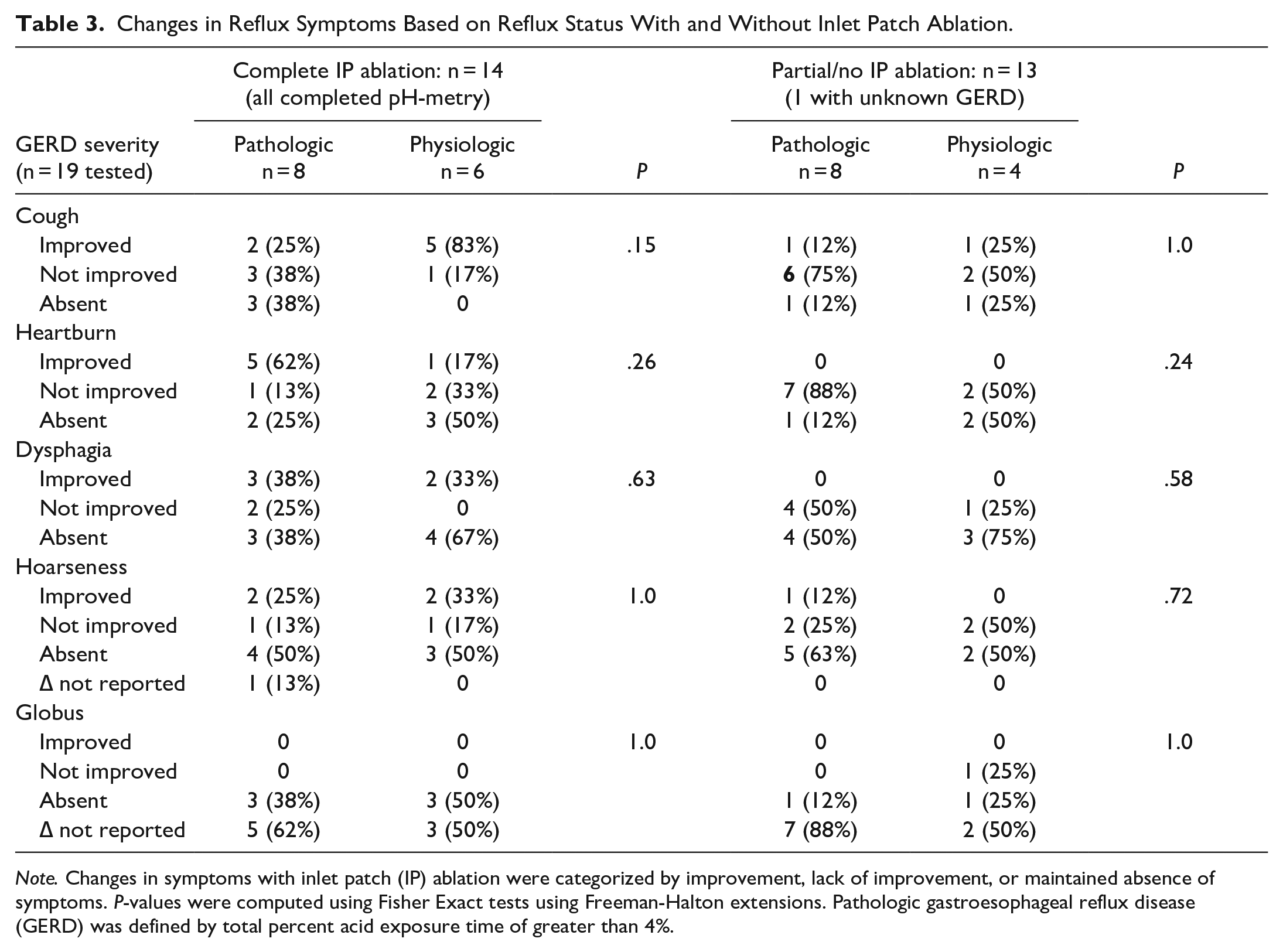
Note. Changes in symptoms with inlet patch (IP) ablation were categorized by improvement, lack of improvement, or maintained absence of symptoms. P-values were computed using Fisher Exact tests using Freeman-Halton extensions. Pathologic gastroesophageal reflux disease (GERD) was defined by total percent acid exposure time of greater than 4%.
The majority of the 13 LTx recipients had small IPs (6), followed by large (5) and medium (2). Seven were diagnosed with pathologic GERD (2 borderline, 3 mild-moderate, 2 severe), 5 with physiologic GERD, and 1 did not complete pH testing. Eight LTx recipients underwent all sessions to complete IP ablation, while one patient only received a single ablation without complete IP eradication. Four did not complete any session for IP ablation. Five patients had chronic lung allograft dysfunction (CLAD) due to bronchiolitis obliterans syndrome (BOS), while one had frequent episodes of acute cellular rejection (ACR). The majority of LTx patients with chronic or recurrent rejection episodes either had medium to large IP or small IP with concomitant pathologic GERD. Two patients had single episodes of acute cellular rejection: one diagnosed on 6-month surveillance lung biopsy, and the other was presumed acute rejection in the setting of acute hypoxic respiratory failure requiring mechanical ventilation. The 3 cases of post-LTx mortality in this cohort occurred exclusively in patients with unablated IP. Five patients did not develop rejection over a mean 5.0 (0.4-14.2) years of follow-up. Time to onset of rejection did not correlate with IP size (r = .33, P = .44) or reflux severity (r = −.27, P = .52; Table 4).
Allograft Rejection and Mortality Among Lung Transplant Recipients With Inlet Patch (n = 13).
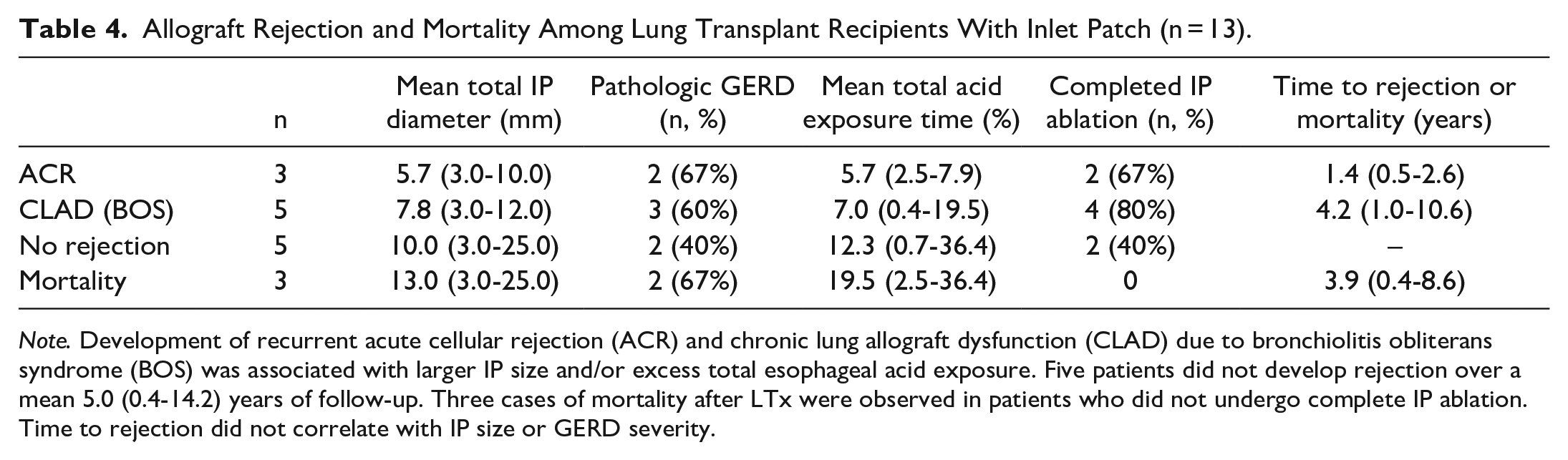
Note. Development of recurrent acute cellular rejection (ACR) and chronic lung allograft dysfunction (CLAD) due to bronchiolitis obliterans syndrome (BOS) was associated with larger IP size and/or excess total esophageal acid exposure. Five patients did not develop rejection over a mean 5.0 (0.4-14.2) years of follow-up. Three cases of mortality after LTx were observed in patients who did not undergo complete IP ablation. Time to rejection did not correlate with IP size or GERD severity.
Conclusions
IP is increasingly recognized as a clinically significant entity driving symptoms of LPR. Given the connection of reflux with lung disease, we investigated the impact of IP ablation among patients with a variety of pulmonary conditions. We identified a prevalence of 6.1% of IP in patients with advanced pulmonary disease, which is comparable to previously published estimates of prevalence in the general population. 1 No single pattern of lung injury was identified, suggesting that IP may be an important finding in a wide variety of pulmonary conditions. Three cases of alpha-1 antitrypsin deficiency were observed, which is notable given its relatively low overall prevalence (1:5000-10 000).
Total IP size may be predictive of severity of reflux symptoms. Baudet et al found that large IP lesions (>20 mm) have been associated with a twelve-fold increased risk of dysphagia. 16 In this study, we found that summative IP size correlated strongly with chronic cough and globus sensation. The association between IP and chronic globus has been previously established with prospective studies of APC ablation.13,14
Chronic cough constitutes a key symptom in patients with advanced pulmonary disease and lung transplant. Seventy-five percent of pulmonary patients with physiologic reflux who completed APC ablation experienced eradication of cough, compared to 29% with pathologic GERD. Given that the symptom of cough may be partly attributable to underlying pulmonary disease, this is a notable improvement. As such, we suggest that persistent cough or globus in patients with advanced pulmonary disease and/or lung transplant should prompt repeat endoscopy with narrow band imaging of the proximal esophagus to evaluate for residual or recurrent IP.
In addition to symptom severity, total IP size strongly correlated with severity of pathologic GERD on ambulatory pH monitoring off acid suppression. The symptom of heartburn was particularly responsive to IP ablation, which improved to a statistically significant degree in comparison to those who underwent incomplete or no ablation. This implies that acidic IP secretions may be an important contributor to esophageal acid exposure in addition to GERD.
CLAD from BOS severely limits long-term survival among lung transplant recipients. 10 IP may be particularly problematic in this population due to their proximity to the pharynx and airway without the barrier protection afforded by the upper and lower esophageal sphincters. These lesions may also secrete hydrochloric acid as well as pepsin, contributing to an inflammatory microenvironment within the transplanted lung. Our data suggest that identification and eradication of IP may also be important for allograft protection. We identified an incidence of BOS among patients with IP that is comparable to transplant recipients overall (60% and 64% within 5 years of transplant, respectively). 17 Time to rejection and/or mortality did not correlate with IP size or GERD severity, however this is not unexpected given the variable progression of BOS. Unablated IP was associated with mortality in this study, indicating that the cumulative injury from IP secretions may be a major risk factor for allograft failure. IP ablation should be considered in these patients for prevention of lung transplant rejection, in addition to timely anti-reflux interventions.
To our knowledge, this is the first study to examine the significance of IP specifically among patients with advanced pulmonary disease, including lung transplant recipients. Although IP is a relatively rare clinical entity, we were able to identify statistically significant associations between total IP size and symptoms of cough and globus, as well as improvement in dysphagia and heartburn following APC ablation of IP. The robustness of the symptom response with APC ablation between those who had physiologic GERD (ie, negative for excess GERD) versus pathologic GERD further strengthens our findings.
This study has several important limitations. A retrospective study cannot determine a causal relationship between IP and development of advanced pulmonary conditions. Because of small sample sizes, a power calculation was not possible as we used all patients that could be included. The lack of formal questionnaire data was limiting, particularly for globus sensation. pH-impedance monitoring has a higher sensitivity for detecting proximal reflux events and was not performed. In addition, the length of time for follow-up evaluation was variable.
Our overall study findings suggest that IP should be given careful consideration in patients with advanced pulmonary disease and lung transplant, particularly if symptoms of chronic cough, dysphagia, or globus sensation are present. Identification and eradication of IP may play an important role in prevention of lung transplant rejection. Given that IP may be easily missed on routine white light endoscopy, GI evaluation of patients with advanced pulmonary disease should include careful narrow band imaging of the cervical esophagus for the presence of these clinically significant lesions.
Footnotes
Acknowledgements
The authors have no acknowledgments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.