
Abstract
Externalisation is a technique from Michael White’s narrative therapy that is commonly used in treating eating disorders. With anorexia, its use presents challenges particularly with a diagnosis where the person is so strongly identified with it. Separating the person from the problem can sometimes lead to a resistance from the patient who feels that the anorexia is part of them. Sartre’s existential approach is a form of psychotherapy that can help resolve this dilemma of accepting that the anorexia is part of who they are but also challenge how they are objectified by it. In addition, because existentialism is always relational (i.e. we are never a separate subject), these objectifications only make sense with a self-other (i.e. the family or the wider system). It helps the patient to engage in a dialogue with the socially constructed narratives that underly the anorexic presentation. The central aim of Sartre’s work is to overcome objectifications of self and other, and this approach offers an innovative method of challenging these objectifications within families. We explore exercises that may be useful in the clinic with a particular emphasis on the future as a way of tackling anorexia and has implications for other clinical presentations and not only anorexia.
Keywords
For us man is characterized above all by going beyond a situation, and by what he succeeds in making of what he has been made even if he never recognizes himself in his objectification JP Sartre- In Search of a Method
Unpacking stuckness
In the therapeutic work with people suffering from anorexia nervosa (AN), frequent is the sense of ‘stuckness’ perceived by both the patients and their families, and the therapist. It is this sense of ‘stuckness’ that led us to examine the contribution that the work of Michael White and Jean Paul Sartre provides in the clinical work with people suffering from AN and their families, deepening Selvini Palazzoli’s insight that anorexia is an existential illness par excellence (Palazzoli, 1985).
In my work (first author) I encountered this ‘stuckness’ when working with young people with a diagnosis of anorexia and using the technique of externalisation, which is common in the field of family therapy for AN. In my own practice, I have used externalization successfully in most presentations, except AN. The most successful externalisation I did was with a young boy of 8 years of age while working in a department of palliative medicine. His father was being treated for cancer and I saw him with his mother because he would have extreme anxiety when she dropped him off to school in the morning. We externalised the separation anxiety, which he called ‘the shark’ and elaborated the influence of the shark when his mum left. It became bigger, circling around him and making him feel upset, crying, and inconsolable. We developed this with a ‘double externalisation’ by finding that dolphins were not afraid of sharks and would bash them on the nose when they came close. With the help of the mum and the school, pictures of dolphins were stuck all around the doorway of the school when mum had to say goodbye. The young boy was able to imagine powerful dolphins warding off any sharks that might be lurking in the doorway. Following this, he was able to say goodbye and the sharks disappeared while his anxiety decreased dramatically.
In my work with people suffering from AN the story was not so simple. In our previous article on Sartre and AN (Ball and Giombini, 2023), we discussed the problem of using externalisation when the person strongly identifies themselves with AN and do not see it as a ‘problem’ but a part of them. They report feeling labelled, therefore objectified, by the diagnosis of AN and they disagree with it. They say that people see AN in everything they do, and they do not feel seen any more for who they are. In this case, our attempt to use the technique of externalisation could potentially reinforce the sense of objectification they have already experienced, leaving them feeling misunderstood. An example of this is a young person I worked with who had attended a community eating disorders (ED) team and I enquired whether she had come across externalisation in her treatment before. She said she had, but ended up not liking it because of the name chosen to externalise the problem (i.e. ‘Ms steps’, as she overexercised pacing up and down the stairs). The name became a source of ridicule when her relatives referred to her as ‘the stairs girl’. In other words, she became objectified again, while the central aim of externalising conversations is to highlight objectifications firstly and to resist them through reauthoring conversations.
For the externalisation to feel helpful and individualised, it is important that the person chooses the name they feel it is more appropriate to describe what they are experiencing, and that the therapeutic work encourages openness, collaboration, and ongoing examination (Freedman and Combs, 1996).
However, parents or relatives often chooses it without involving the young person in identifying a name that feels more representative. They tend to do it because it is what they learnt through books they read and workshops they attended with the hope it will help their children to start fighting against the disorder.
This led us to look more closely White’s work regarding objectification and externalisation, which are the main concepts underpinning narrative therapy and considering how this links with the work of Sartre who presents an analysis of objectifications in Sartre (2018).
White’s use of externalising conversations stands on the assumption that our identities are constructed socially through a series of objectifications occurring within our cultural and political relations, which are shaped by dynamics of power and knowledge (White, 2007). For Sartre, this is called ‘bad faith’. If the person feels that the externalisation depicts them in another fixed identity, we repeat this objectification. This would be a failure to separate the person from the problem, which is the main aim of externalisation.
In this article, we will discuss the helpfulness of the clinical application of some of the main concepts deriving from White’s work on externalisation and Sartre’s concept of the project, expanding on our previous paper. We will consider the stance of the social constructionism approach, from which White’s work derive. Social constructionism makes the basic claim that our identity is not to do with having some internal personality or fixed nature but that we only experience ourselves “as if” our features have some concrete existence in the world. The identity we confer to ourselves is related to our purposes rather than a priori fixed nature (Burr, 2015).
The claim of this paper is that when externalisation as a technique is disconnected from a social constructionist approach that is when it breaks down because it becomes unmoored from a collaborative approach.
The contribution of White’s work on externalisation
Externalising and reauthoring conversations
Often conferring a medical diagnosis has the power to objectify people’s identity into a specific label. The central aim of externalisation is to challenge that objectification (White, 2007). When a person is conferred a label, such as ‘anorexic’, they risk becoming and existing as just this label rather that a person who happens to also have some issues related to eating and body image, and typically a lot of other related distresses and challenges in their life. As one young person said to me: ‘maybe I want to be anorexic because I don’t know who I am’. In essence, their identity is robbed or diminished to a diagnostic label and to a set of cultural discourses, in which they are immersed. Understanding this reconnects the technique of externalisation to the social constructionist tradition of doing therapy.
Externalising and reauthoring conversations have the aim of challenging one’s identity as having a fixed nature. Several well-known techniques in narrative therapy illustrate this. For example, relative influencing questions where the therapist enquires about the history of the problem and rate numerically times when the problem was stronger or weaker enable the therapist to ‘open up other stories about the problem’ so that the problem is ‘less static and fixed’ (Morgan, 2000). Another technique is ‘unique outcomes’ which aims at challenging the dominant narrative of the problem. As Morgan writes: ‘it is assumed that a problem will never be 100% successful in claiming a person’s life’ (Morgan, 2000). White draws on Foucault’s analysis of power to achieve his purpose in showing how our identities are shaped by oppressive cultural and political forces (White, 2007; White and Epston, 1990).
I want to focus on White’s use of the metaphor of ‘maps’ or ‘journey’ in guiding therapeutic conversations as this comes close to Sartre’s notion or metaphor of ‘the project’, which takes up White's invitation when he writes, ‘I welcome efforts to translate the practices described in this book into terms associated with alternative metaphors’ (White, 2007).
White uses the concepts of ‘landscape of action’, and ‘landscape of identity’ as central features of reauthoring conversations. The ‘landscape of action’ in narrative therapy is the material of the client’s story, the sequence of events, the plot, the characters, all charted in time (White, 2007). This is, for the most part, the world of contingency. The ‘landscape of identity’ comprises of the client’s understanding of the above, their reasons, motives, feelings, and reflections. In short, it is their account of what happened and most crucially it includes their plans, intentions, and purposes within this narrative frame. The therapeutic aim is to give the therapist the context to support people in drawing new conclusions and making new choices about their lives rather than repeating these dominant stories. White refers to this process as ‘meaning making activities’ and helping to offer ‘a stronger voice of authorship’. The assumption is that in doing this a sense of a clear theme or plot unites the client’s story, which in Sartre’s terms uncovers a ‘project’.
The limits of externalisation as a technique
When trying to use externalisation with AN, many attempts ended in the interruption of the dialogue. The young person would either say ‘I’ve done this before (i.e. with the community team) and it didn’t help’ or would say that ‘my anorexia is part of me and not separate’. The use of externalisation becomes in fact unhelpful when there is not enough respect for how wedded AN is to one’s very identity to the point where aspects of their lives, other than that related to the problem of food, become marginalised (Dallos, 2006).
We began to see that the young people were so openly identified with the AN that trying to wrestle the person away from it too early didn’t acknowledge how much it was part of their agency. AN was acting for them as an attempt to have power and control over their lives. In fact, it may be the only place where they feel like they can win (Ugazio, 2013). As one young person said to me ‘I was happier when I was controlling my food’ or ‘it is the only thing I am good at’.
The danger of separating the person from the problem is the risk of cutting oneself off from the self and losing one’s agency. This is not to say that the technique of externalisation is not helpful. A typical example is the case of Julia. She chose to call her anorexia ‘the devil’. This was done in the presence of her parents, and it took some effort to allow her to choose the name herself. In exploring its influence on her relationship with her mother and how it made her fight with her mother, it eased the guilt she felt about being so ‘horrible’. It also helped her mother to do the same, that is, ‘the devil’ creates this conflict between them. The externalisation helped to ease the strong sense of blame that each felt and to find a way of talking about their deteriorating relationship that young people often find too difficult to address. The dilemma for this young person was that although initially she found it helpful to do an externalisation and calling her anorexia ‘The Devil’, which helped to take away blame from herself and her parents, she still said in a following session ‘I still feel that the anorexia is part of me’. By accepting this we engaged in a complex conversation about how being anorexic had helped her come to terms with her anxiety and cope with some difficult life events in her family and eventually unravel how her identity had become intertwined with the anorexia. Part of this was creating new narrative about her future projects and plans. In other words, this was a therapeutic process of exploring and imagining parts of her identity that were not yet in existence. It enabled her to take charge of her identity and take responsibility for choices she can make (White, 2007). Therefore, it is crucial to achieve this through a complex collaborative enterprise over time rather than a naming and getting rid of what is externalised and depriving them of this sense of agency however harmful its present form.
The contribution of Sartre’s philosophy: From objectifications towards a sense of agency
Objectifications as the project of bad faith
Sartre’s magnum opus Being and Nothingnessis hardly a book on the reference list of any family therapy course. Despite its complexity, its aim is to create a form of psychotherapy helping people to overcome socially constructed objectifications and recover a sense of personal agency by resisting them. By emphasising that all objectifications occur in interactions with others, it strongly moored the therapeutic work within the family context.
The entire book outlines how these objectifications arise. Sartre called them ‘the project of bad faith’, highlighting how, influenced by our social conditions, we form the false belief (i.e. bad faith) that we have a fixed nature, and we organise all our actions and behaviours, unifying them into a ‘project’. Bad faith is a form of self-deception, but it is not an individual condition rather a contextual phenomenon. The project of bad faith constrains us to see ourselves as having a fixed nature and prevent us from becoming aware of the influence of the social conditioning. This has strong parallels with White’s account. The recovery from the ‘project of bad faith’ towards the ‘project of authenticity’ is achieved by helping the person to see and reflect on their own hidden personal projects, and not feeling determined by them. Like in White, this is a process of reauthoring and revising one’s projects.
Furthermore, Sartre stresses the fact that the objectifications occur in relation with others, as we tend to objectify each other thinking that they have a fixed nature too. In my work with young people, parents find it immensely helpful to see how they participate in these self and other objectifications. An example of this is when a grandfather depicted his granddaughter as ‘strong’. By challenging this identity or objectifications as ‘strong’ the family saw that the young person had to be the strong one and failed to see her vulnerability and therefore her needs.
Therefore, Sartre’s analysis is strongly relational. The formation and foundation of the self for Sartre is not an internal genesis but develops through ‘the look’ of the other. In the same way, the chain of objectifications is embedded in our interpersonal relationships.
The look as the mechanism of objectification
The self is not a separate entity that encounters the other but is co-created in an encounter with the other. Sartre describes this process through the concept of ‘the look’. This concept predates Foucault’s Panopticon. The ‘look’ emphasises the role of others in shaping our sense of self, the Panopticon focuses on surveillance and discipline as a means of control. The look, on the other hand, focuses on interpersonal relations and how this leads to being objectified. When I am seen, I feel this vulnerability and see how fragile myself is. I feel judged. I experience shame and sense myself at the end of their gaze: ‘Shame is the shame of oneself, it is the recognition that I really am this object that is looked at and judged by the Other’ (Sartre, 2018). I feel out of control and realise I am no longer master of myself. I become objectified and I am in danger. In the case of Julia, it is not the anger that makes her feel guilty but that she worries that her parents see her as an angry bad person, that is, this is who she is.
We can see how this mechanism becomes so embedded in a young person’s view of themselves when they are bullied, or spoken about, especially if they are already sensitive to others. Sartre offers two ways people respond to this situation. The first is by negating the other as if they didn’t exist, which he calls the ‘sadistic pole’. The second is by giving up one’s subjectivity altogether and accepting how the other defines me, which he terms the ‘masochistic pole’. In a simple example, if my school friends think I am bad, I withdraw thinking that I am not bad and seeing the other as nothing, I detach from the other isolating myself (i.e. sadistic pole). This is often acted out with parents when the young person reduced contact with them. Or, I believe that I am bad so I will be filled with self-hatred, feeling always subject to their needs and opinions (i.e. masochistic pole). In AN, we commonly see young people taking up one of these two attitudes: either to detach completely or to lose oneself in the needs of others. We also observe how the refusal to eat is often accompanied by a refusal to engage with others whether this be therapy, parents, or friends. This can be interpreted as an attempt to achieve independence of others and of change.
For example, Greta arrived at the hospital seriously underweight and had to be in a wheelchair for several weeks. This created a sense of shame, and she completely disconnected from her family. She refused food and water, and any form of individual or family therapy.
She appeared consumed by AN, as if that was her fixed nature, and was disconnected from her world. Sartre’s analysis explains how objectifications leave the person feeling that have no control over how they are seen, and they are in danger of becoming defined by them. This was also very evident when Greta talked about her body needing to meet severe external standards as dictated by the others.
The project of authenticity: A mystery in broad daylight
The notion of the project is the driving force behind Sartre's philosophy and all other concepts such as freedom and responsibility. Sartre believes that our actions are free because they manifest projects that do not bind us. We become defined by our projects, objectified by them, and we live as if they are truths about ourselves. For example, in AN, we commonly find a young person saying – ‘I am a bad person’ – and experiencing it as a fundamental truth about their identity. They are conflating ‘bad’ with ‘person’.
The aim of any therapy would be to find the fundamental project that drives our lives, gaining a sense of agency towards them. Sartre’s aim is to understand the power of projects in exerting their influence on our behaviour, or to put it more explicitly to track the very reasons why we do what we do.
It is important to consider that our projects aim at preserving something that has positive value for us (Webber, 2018). AN as well can be seen as a project that is deeply entrenched or socially constructed (Hepworth, 2003). In the case of Julia, by acknowledging that anorexia is part of her, we are helping her to see that it is part of her project and by exploring this and other projects she may have in the future she may come to continue the ones she values and hopefully abandon the project of anorexia. Doing this in the presence of parents helps them to empathise with their child and created a richer description of projects that are lacking.
Sartre developed a ‘regressive-progressive’ method of therapy, which emphasised a look back at the past to track one’s project in childhood and social conditioning, but also to look forward to determining the reasons and meanings behind any project that we choose. By analysing the history, the stories and events of your life regressively, the aim is to find a clue to the individual’s project that is futural, that is, their intentions, their meanings. Sartre writes: ‘thus the return to the biography shows us the hiatuses, the fissures, and the accidents, while it confirms the hypothesis (the hypothesis of the original project) by revealing the direction and continuity of the life (Sartre, 1960). Sartre’s claim here is the individual is defined through the ‘ends he pursues’, so this method aims at uncovering this secret of the unified project. For Sartre, all meaning comes from the future, that is, our goals and aspirations. In other words, it is the future in the present and not the past in the present, as psychoanalysis often claims.
The concept of the project is not implying that it is the person’s project and thus blaming them for the choices they made. It is more to do with the idea that we are immersed in projects that we are for the most part unaware of, but we participate as actors.
Through his slogan ‘we are what we are not, and we are not what we are’ (Sartre, 2018), he emphasises that our character consists in freely chosen projects. Sartre’s claim is that although we have character traits, these are not fixed and are not our natures. In a sense, this means I am not what I have been. To affirm that I am what I have been, is to, as Sartre says, ‘deliberately arrests himself at one period in this life’. In AN, this is evident in the common reported experience of not wanting to grow up, which can be related to seeing the self as fixed in nature. He writes: ‘who will decide whether that mystical crisis at the age of fifteen was a pure accident of puberty, or, on the contrary, the first sign of a future conversion?’ (Sartre, 2018).
In Sartre’s account, it is the anticipated future that organises the present and not the past. Therefore, we need to look at the person’s ‘project’. Thinking of this in terms of White’s landscape of action and looking through the events in peoples’ lives I would be interested in finding or uncovering evidence of particular themes or clues to a person’s project. What Sartre stresses is that the person’s project is there, perhaps hidden, and in this is what he means by a ‘mystery in broad daylight’. Thinking of it in this sense creates a therapeutic encounter that is very respectful of the client’s unfolding story. In the case of working with young people with a diagnosis of anorexia, it helps to give them a greater sense of control over their narrative. It promotes a stronger sense of identity. White chooses the term identity to highlight the therapeutic aim that ‘any renegotiation of the stories of people’s lives is also a renegotiation of identity’ (White, 2004).
An example of this is Emilia who, in exploring the aims of her AN, such as pleasing others, being dependant on AN, and saying that she is ‘boring’. We track the influence of being boring on her life. We could say that being boring is her project. Reassuring her that she is not boring is pointless. Instead, if we conceive of being boring as a project or an aim or purpose. This approach creates a new set of questions such as: ‘how is boring helpful in your life, what is its value, what’s its plans, its purpose, who agrees, etc.’ Her project of being fed through nasogastric feeding is a smaller project, of restricting, exercising all encompassed into the project of AN. However, what emerges is the project of being boring.
So, if Emilia’s project is to be boring, we must work out the reason for this, by understanding how the future influences the present. Sartre writes: ‘even observations such as ‘I am ugly’, ‘I am stupid’ (etc…) are in essence anticipations. It is not a matter of purely observing my ugliness, but ‘of grasping the coefficient of adversity presented by women, or society, to my undertakings’ (Webber, 2018). Again, by discussing this in the presence of the family helps to recruit them into projects and purposes outside of the AN narrative.
This requires a more detailed, nuanced analysis of the history of this and how it fits with one’s future directed projects. White strikes a similar tone when he says that we must evaluate and enquire how an externalisation fits into one’s values and life plans. This is the third category of enquiry called ‘mapping the effects of the problem’ (White, 2007). What both share is a strong denial of determinism. Sartre’s notion of freedom can develop White’s externalisation to strengthen the link with agency, responsibility, and freedom to act. It is not a complete separation from the self but a metamorphosis of the self toward other projects that are more constructive. Freedom for Sartre is not some indifferent libertarian abandonment of moral values, but it is a freedom to modify my projects ‘Our actions are free because they are ultimately rooted in our projects, which are themselves freely chosen and maintained’ (Webber, 2018). What Sartre emphasises help the person to explore the part of their identity that has not yet come into being and to find meaning in their future intentions, that is, ‘I am what I am not (yet)’.
Emilia revised her project of being boring, became less concerned with other people on the ward and became more interested in her project of resisting this and showing her strength and value of being independent. This was achieved in exploring her goals of wanting to be a doctor like her uncle and he she valued his determination and independence. She began to work towards leaving the hospital, doing her meal tasks, and finding new and more valued friendships.
The integration of White’s and Sartre’s work: A proposal
White’s externalising conversations and Sartre’s existential therapy share the goal of breaking the objectifications by challenging the fixed identity of a person with how they are defined or objectified by others.
For White the equation is ‘I am not my problem’. His renowned formula for this is that ‘the person is not the problem, the problem is the problem’ (White, 2007). In other words, the sedimented cultural objectifications are the problem and not the subject of these objectifications.
Equally, Sartre’s formula is ‘I am not what I am and I am what I am not’. In other words, I am not the stories that are told about me, but I am the stories that I can co-create which are not yet but are unfolding.
White is developing a new narrative of the self, a new sense of agency that opens up a ‘new range of possibilities become available to revise this relationship’ (White, 2007).
Reauthoring the project
Sartre’s concept of ‘the look’ can be seen as a rich description of the externalisation in the relational self. We can also see Sartre’s notion of the project as an account of reauthoring conversations or in other words how to conduct a therapeutic process to help the young person to overcome externalising objectifications. As described by White by ‘landscape of identity’, our character consists in projects that we can pursue and we can revise, but according to Sartre, we generally prefer to consider them to be fixed natures over which we have no control (Webber, 2018). Why? Because it is easier not to take responsibility for the way we are. Particularly in adolescence this process is frightening and overwhelming.
Our self is linked to our projects that can be brought into the daylight by tracking these projects over time as in the landscape of action and identity. What Sartre emphasises is that our tendency is ‘an ongoing pursuit of a goal-in short, as a project’ (Webber, 2018). In effect, projects structure our experience, whether we are conceptually aware of it or not, into a single goal. Like in White, the goal of therapy is to unpack this project.
In the beginning of therapy, the person’s attitude towards their problem/project is that it is me who is the problem and the aim is to unearth this attitude. As White argues: ‘Many of the people who seek therapy believe that the problems in their lives reflect their own identity or the identity of others.'
Sartre’s aim is to show that it is a belief, an attitude which is built on ‘non-persuasive evidence’. Good faith on the other hand, which is the aim of reauthoring conversations is based on evidence that emerges in the enquiry. For Emilia, the belief that she is boring is a belief that she has a fixed nature and that this is an objective fact rather than on how she sees her world and thus deny our freedom to choose to revise this. But how do we reverse this?
Sartre writes that bad faith ‘dare not speak its name’, and is a ‘buried project’(Webber, 2018).
Most people agree that AN is not just about food. Social constructionism supports this claim and Sartre’s idea that our actions are unified by a project helps to see that any aspect of the patient’s experience linked to the anorexia rather than being independent. In other words, our relations with others, our body image, and our attitude towards ourselves are all linked and working on one area is always connected to another. We don’t have to address the AN directly and most patients find this too hard. This is why externalising conversations work and offer a safer gentler approach. An example of this is when I asked Rebecca if it was ok to talk about her self-harm. She said no. But when I asked if it was ok to talk about ‘anxiety’ that may underly it she said ‘yes’, and we spent a productive session with parents all the various aspects of anxiety and the role it plays in her life. All I needed to keep in mind was that anxiety was not part of her fixed nature and the rest unfolded naturally. Within a week, Rebecca stopped self-harming and was able to separate herself from the anxiety and have some control over it.
Externalising objectifications and reauthoring: An exercise
If we consider objectifications as a core element of both White’s and Sartre’s work, another way of doing externalisation and reauthoring conversations could be to do the following exercise.
Examples of objectification and resistance questions.
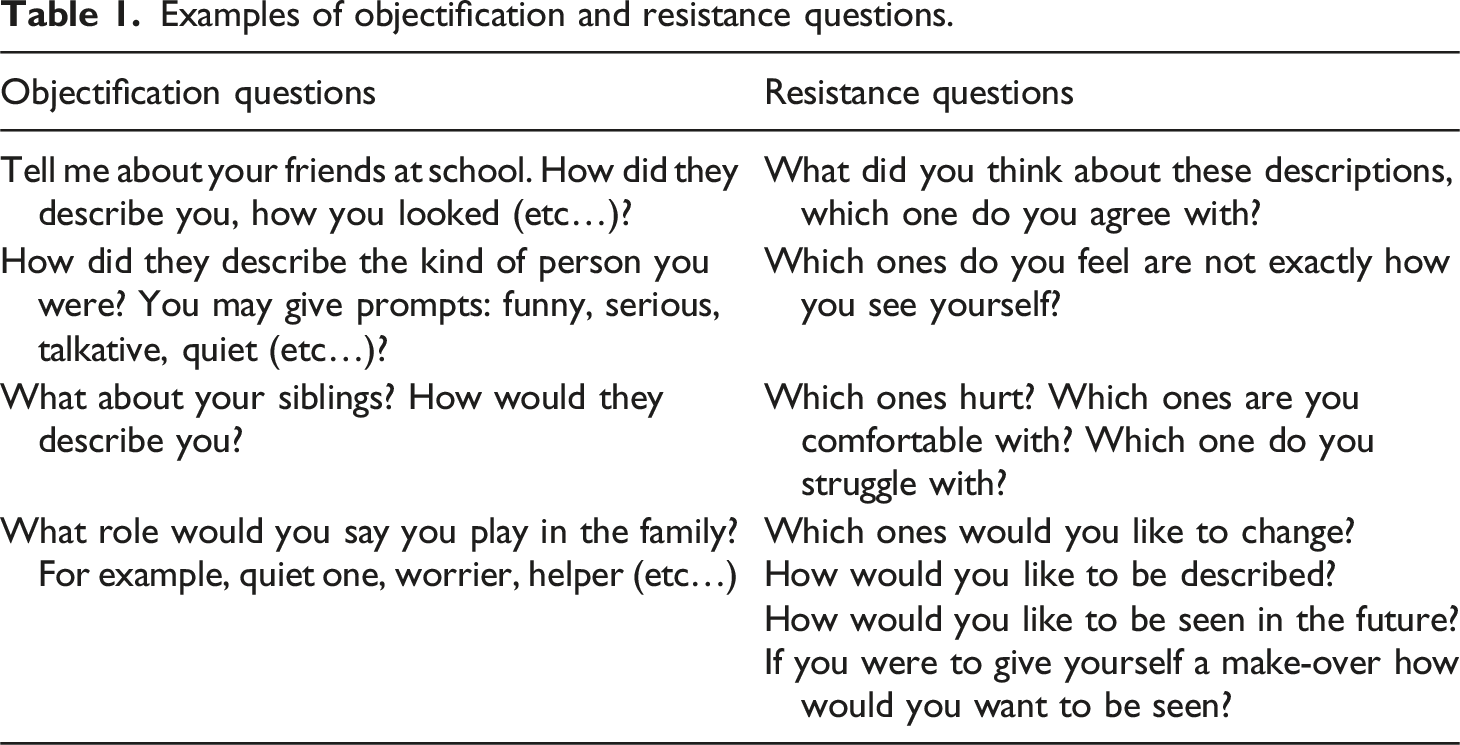
An example is Rebecca, who said that at school she was called ‘a green giant’ and said I didn’t think much of it I assumed it was a ‘little o’, but she said it was a ‘Big O’. This led to further curiosity about how this was so.
I open new questions about the person who said it to them and invite a reflection on this. I also then think about a timeline of Big reauthoring – ‘Big Rs’ and ‘Little rs’, highlighting the resistances to the objectifications. I have done this by asking questions such as ‘how would you like to be defined?’ Rebecca answered ‘as someone who is conscious of environmental issues’. With the parents present, we explored ways of helping Rebecca to develop forms of resistance such as joining environmental groups with Dad’s help. In this simple way, I am engaging in a similar way to White’s movement between externalising questions, that is, ‘Big Os’ and ‘Little os’, and reauthoring questions, that is, ‘Big Rs’ and ‘Little rs’. Following Sartre’s emphasis on the project, which looks to the future or one’s purpose, this timeline of ‘Little rs’ and ‘Big Rs’ can spread out in the future with questions such as ‘what kind of resistances would you like to say or do in the future?’ This can lead to rich descriptions of how they would like to be seen by others in the future. With AN, all young people are very conscious of what to say or do when they are discharged. Within this lens of the project, I can add Big and Little Projects and imagine what project would they like to pursue as an alternative to AN. Keeping this lens in mind, I can get a fuller description of her parents who can support this. It can also be particularly emancipatory for the young person who doesn’t have to remain stuck in the past and looking for causes or why they were anorexic but looking forward to a new future.
I often notice that young people enjoy this line of questioning because it places the burden outside of themselves. Tracing objectifications through the life span achieves a similar result that externalisation does, that is, to separate the person from the problem, and unstick these imaginary constructions from who they are. It promotes agency in their lives and engages them in the authentic project of becoming. This is an endless pursuit and leaves them with a new attitude. The analysis ends with the person’s own illumination or intuition and that is respected as final, not the therapist’s interpretation. This, White argues, is an ethical stance (White, 2007).
Conclusions
This article is about the value of adding Sartre and existentialism as a theory to support family therapy because it highlights that problems arise through concrete relations with others through the mechanism of what Sartre calls the ‘look’. Social constructionism, from which Foucault’s philosophy is widely known as a post phenomenological structuralism that takes its place as a ‘repudiation of the philosophy of the subject’ that focuses on the coercive force of power in the development of the person and this ‘unidirectional’. This is not to say that it is inaccurate but that it doesn’t take enough account of ‘mutual recognition of subjects’ in socialisation and the capacity of the subject to be a strong agent in this process however distorted (Dews, 2007). Similarly, in her discussion of agency in social constructionism, Burr (2015), although not mentioning Sartre explicitly, states that social constructionism shares with phenomenology a rejection of essentialism and takes embodied experience seriously and that phenomenology may be a resource here. Sartre’s claim the body is relational and intersubjective offers a powerful resource for family therapists to theorise AN. Sartre’s work deepens the relational notion of the self and the emancipatory value of resisting objectifications which is the core aim of externalising conversations. He adds another way of tackling rigid sedimented objectifications that can engage parents and young people in a dynamic way where you can generate a systemic generative conversation and where you can start anywhere and not directly addressing AN.
Footnotes
Acknowledgements
The authors would like to thank all the young people, their carers, and staff at Rhodes Wood Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed are those of the authors and not those of Elysium Healthcare or of Royal Holloway University of London.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.