
Abstract
This paper is presented as a response to an invitation from the editor of Human Systems. Systemic theory and therapy have evolved over the last 70 years and each new generation of practitioners encounters the historical and contemporary literature through fresh eyes. Clinical psychology is one discipline which continues to value systemic approaches. Multiple Clinical Psychology (DclinPsy) programmes nationwide facilitate training approved by the Association for Family Therapy and Systemic Practice (AFT). The University of Plymouth is one such example. This paper offers a window into the experience of a trainee clinical psychologist attending a foundation in family therapy course, undertaken as part of their wider training on the DclinPsy. It covers a brief summary of the history of family therapy, the practitioner’s insights into how it is utilised in NHS services and its modern-day application for clinical psychology.
Keywords
Introduction
This paper offers a summary of the development of systemic family therapy (SFT), acknowledging the three distinct phases of its evolution. Following this, a description of how it is implemented in the National Health Service (NHS) is discussed. The evidence base for SFT is covered alongside the barriers to SFT being a ubiquitous intervention across services, with consideration given for its utility in clinical psychology. This will lead to a reflection on how the author, a trainee clinical psychologist, has integrated techniques from two specific SFT models into his practice, namely, Structural and Milan SFT. Reflections are shared about how these two iterations of SFT can be adapted and applied to modern clinical practice.
The development of systemic family therapy
Systemic family therapy (SFT) is a relatively recent intervention with its origins located in the 1950s. General Systems Theory, also known as cybernetics, developed out of the Macy conferences and is grounded in the concept of there being ‘circular causal and feedback mechanisms in biological and social systems’ (Umpleby, 2008: p.28). These ideas informed the work of Gregory Bateson who explored them in the context of the social sciences (Umpleby, 2008). Bateson’s research into psychosis developed the concept of the double bind – describing a situation where whatever an individual does, they cannot win (Bateson et al., 1956). It was pioneering in elucidating the significance of context and relationships in the aetiology of a psychopathology, seeking to reconceptualise psychosis as an understandable phenomenon (Cullin, 2006).
Around this period, Bowlby’s work was also laying down important scaffolding for the future of SFT. Writing one of the first family therapy papers, John Bowlby described supporting a whole family rather than an individual and the impact of working directly with relational dynamics as they unfolded in the room (Bowlby, 1949). Whilst he would not go on to develop this way of working, instead focussing on the development of attachment theory, it did inform the work of others, such as John Bell, one of the first family therapists (Parkes et al., 1993).
Graduating on from these ideas, we see the establishment of ‘first order’ SFT. Structural family therapy was one of the first distinct systemic therapies, focussing on the organisation of the family. Developed by Salvador Minuchin in the 1960s, a key premise was that there is a hierarchy and homeostatic regulation within family systems, with parents being the leaders (Smith, 2011). When significant life events occur, this homeostasis can be perturbed, leading to a dysfunctional organisation of the family system. Specific ideas were generated relating to this, such as, there being distinct subsystems within families that have unique characteristics. Another is called a coalition, where two individuals unite against others in the family (Dallos and Draper, 2024).
Another first order approach is strategic family therapy, which focuses on identifying and formulating the problematic sequence of events a family may be experiencing, seeking to find ways to disrupt these cycles through adopting various strategies (Dallos and Draper, 2024).
The mid-70s to 80s covers a period known as the ‘second order’ for SFT. The Milan group were instrumental in developing new concepts and techniques for family therapy. They drew upon Bateson’s ideas that families are concerned with shared meaning making through multiple layers of communications (Dallos and Draper, 2024). The model was based on identifying these layers of communication through observing family interactions, using specific techniques to intervene. They built on Bateson’s idea that a unit is subject to feedback from the system it resides in, leading to the consideration of feedback loops and the development of circular questioning (Campbell, 1999). The group introduced what would now be considered foundational ideas to family therapy, such as hypothesising, circularities and observing the intervention.
From the late 80s moving into the 21st century, we have seen the development of ‘third order’ approaches which emphasis a strong alignment with social constructionism. Narrative therapy is one such approach which adopts a non-expert stance with an emphasis on facilitating families to tell their stories whilst intervening at appropriate openings to help them tell a new story which aims to decrease blame and increase agency (Minuchin, 1998).
Solution focused brief family therapy takes an approach of building on the family’s resources and focussing attention on exceptions to a problem and doing more of ‘what works’ (Bond et al., 2013). The emphasis is often future focused, identifying clear goals.
In recent decades, there has been a growing development in manualised family therapies, such as the Exeter model. One rationale for doing this is that it creates a clearer process with which to evaluate an intervention; an important point given the ever-increasing weight given to commissioning evidence-based interventions (Pote et al., 2003).
Systemic family therapy in the NHS
Family therapy and systemic practice has also been on a journey in how it has evolved and been utilised within the NHS. Historically this has looked like adopting family therapy skills as a secondary practice within an already established role, such as social work (Webster, 2002). In recent decades, there has been a growth in the number of full-time family therapist roles, coinciding with the formation of the Association for Family Therapy and Systemic Practice (AFT) in 1976 and the UK council of Psychotherapy (UKCP) in 1992 (Stratton and Lask, 2013). During the implementation of the Agenda for Change pay scheme within the NHS in 2004, AFT helped to negotiate a good pay banding for family therapists. Conversely, due to financial pressures, the cost of maintaining these roles at their newly established banding meant that many were lost (Stratton and Lask, 2013).
When considering the accessibility of SFT, three key social graces come to mind; age, geography and culture (Burnham, 2018). Family therapy has an established presence within many Child and Adolescent Mental Health Services (CAMHS) but has struggled to gain a foothold within adult services. The answer to this lies in part due to how adult services are structured around the individual, often at the expense of the wider family system (Stanbridge and Burbach, 2018). This highlights how age can be a dividing line between the potential to receive a family therapy intervention. In a similar way geography is also an underlining factor, with there being a disparity in how family therapy is implemented across the country. For example, Plymouth is the only locality within Devon to have a standalone adult family therapy service.
Culturally, SFT can be a barrier if practitioners consciously or unconsciously subscribe to a western conceptualisation of the family life cycle. The family life cycle refers to the recognition of the different stages a family passes through over time. It is useful as it provides a framework that explains why sometimes, families attempted solutions to navigate significant life cycle transitions, such as children becoming adolescents, can have unintended consequences (Dallos and Draper, 2024). However, ubiquitous application of the western assumptions of the family life cycle in SFT can risk alienating those that reject its heteronormative assumptions and can be oppressive for those who identify with non-western concepts of the family and community (Erickson, 1998). Over time the ideas around what ‘normative’ transitions look like in families have been updated and diversified (Carter and McGoldrick, 1988; Dallos and Vetere, 2021). Caution is still required, however, in the application of the family life cycle given that there are ever increasing variations in life cycle transitions between families (Golijani-Moghaddam, 2014). Taking time to consider how personal social graces and the families social graces may interact can help to mitigate potential pitfalls in assumptions or oversimplifications and ensures that SFT practice is inclusive, meeting the needs of all families and cultures.
With the introduction of improving access to psychological therapies (IAPT) services, there has been concern that this could squeeze family therapy provision, with IAPT having a clear emphasis on providing cognitive behavioural therapy (CBT) interventions delivered by a workforce primarily trained in low intensity CBT (Stratton and Lask, 2013). The breadth of CBT’s evidence base has, in part, informed this decision (David et al., 2018). However, there is also a growing evidence base for the effectiveness of SFT for treating a range of psychological difficulties in both children and adults (Carr, 2019a; Carr, 2019b). Whilst there is not the same depth of research when compared with CBT, which in part can be explained by the fact that many SFT approaches are not manualised, thus make it harder to conduct high quality randomised control trials, there is evidence indicating that SFT is just as effective as CBT for certain psychological difficulties (Hunger et al., 2020). In some cases, such as adolescences with eating disorders, family therapy has the strongest evidence base and is the first line intervention (Wergeland et al., 2024).
Encouragingly for SFT, the Children and Young People’s IAPT programme has seen the development of Systemic Family Practitioner roles which involve integrating the AFT approved foundation and intermediate qualifications into their training (AFT, 2024), creating a financially viable route into systemic family practice. For some trainee clinical psychologists, they are also offered the opportunity to develop SFT skills which they can then integrate into their practice. Several training courses have partnered with AFT to build into their curriculum the approved foundation (and in some case intermediate) qualification, such as the University of Plymouth and Exeter. SFT skills are extremely beneficial to the clinical psychology profession as they often work with families and wider systems, leading teams and services. What follows for the rest of the paper are examples of how the author has embedded certain SFT skills into his practice.
Structural family therapy in practice
I have been working with a family where unhelpful patterns keep repeating, which relate to the youngest daughter engaging in risk taking behaviours. In formulating ideas for this family, I connected with the structural concept that the family problem is located in a dysfunction in the family structure and therefore requires a therapeutic modification of that structure (Colapinto, 2019).
Three distinct sub-systems are present in the family structure (Dallos and Draper, 2024). The parental, the mother daughter, and the sibling subsystem (see Figure 1). Geography has meant that the sibling subsystem has been disrupted, causing sadness for the youngest daughter engaging in risk taking behaviours. The mother daughter sub-system has seen the youngest daughter positioning Mum as a sibling rather than a parent, seeking her out to distract her from her distress. The parental sub-system has lost its sense of parental hierarchy, due to the parent’s close alliance and shared distress of seeing harm come to their youngest daughter. This has led to them inadvertently deferring their parental responsibility of saying ‘no’ to their daughter, in the hope of avoiding escalations. Family genogram denoting subgroups: parental, mother-daughter and sibling.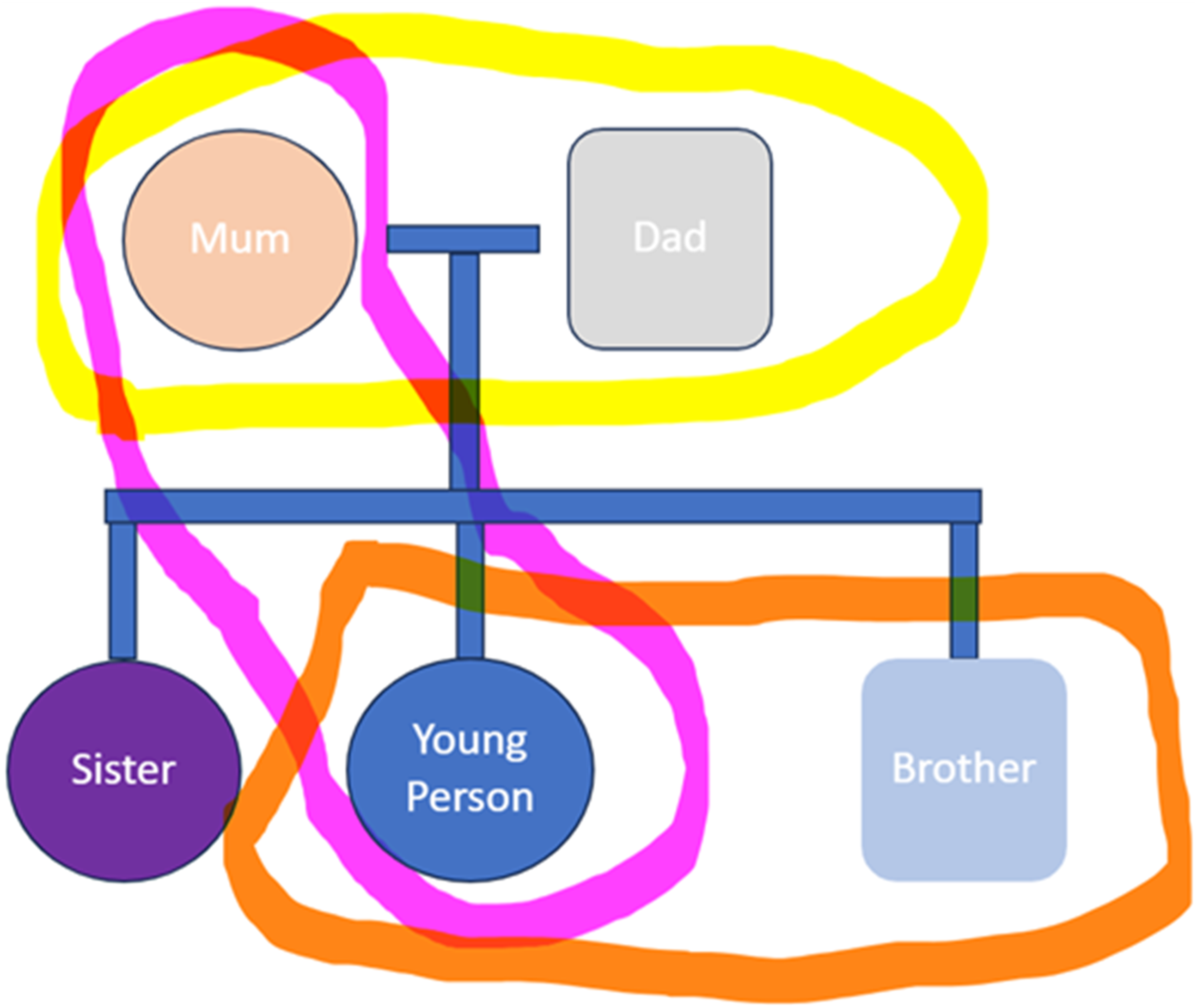
We focused on the parental sub-system, hypothesising that their repeated patterns of interaction with their daughter was a key maintaining factor in her risk-taking behaviour. The parents’ propensity to plicate an unwise request from their daughter. In the hope that this would reduce her risk-taking behaviour, was having the opposite effect, leading to escalation in her risk. A key structural intervention is to seek to reassert the parental hierarchy so that parents can be empowered to make firm but fair decisions, safeguarding their daughter, through clear and concise communication. This is particularly pertinent given that their daughter has autism. The above outlines how the distress in the family system is related to the dynamics of relationships, namely the parental subsystems interaction with their daughter. The parental stress response has led to the re-application of ‘old’ solutions which are having the same negative outcome (Vetere, 2001). Structural theory asserts that the parental subsystem is, ‘vested with the authority for the care and safety of the children’ (Vetere, 2001: p. 134). Restoring this authority is a key aspiration of our intervention. The family clinic I work in has used multiple structural concepts to achieve this, namely, joining, strokes and kicks (a more appropriate rephrasing is encouragement and challenge) and enactment.
Joining is a concept in structural therapy which is very similar to the therapeutic alliance (Dallos and Draper, 2024). It emphasises the importance of building rapport and trust with each family individual and in my opinion creates a therapeutic relationship where you have permission to challenge. We ‘joined’ with the family by connecting with their shared passions, values and memories. Humour was a key component of this. This was necessary in our earlier sessions to facilitate the use of encouraging and challenging (strokes and kicks) (Minuchin et al., 2021). The encouragement strengthened our initial act of joining, whilst the challenging enabled us to highlight parental decisions which were compromising the safety of their daughter because of their fear of causing distress. We then invoked an enactment between the parents and the daughter over a live situation pertaining to an unwise request and concerns from parents that they could not say no. An enactment is where a family is invited to engage in a live and current situation as if they were not in a therapy situation, helping the therapists see the patterns and interaction firsthand, rather than having them described to them (Dallos and Draper, 2024). From this point, we then intervened and supported parents to find safer compromises for their daughter’s requests.
There is good evidence to support the practice of structural family therapy in a modern context (McAdam et al., 2016). This in part explains why we are still using structural techniques in 2024 as evidenced by my clinical examples. However, structural family therapy has been critiqued for its supposed subscription to the maintenance of a westernised concept of the family life cycle. Historically, structural family therapy has sought to rebalance unbalanced family hierarchies and support the transmission of the culture that the family reside in. This leaves it vulnerable to criticism for its assumptions about the family life cycle, alongside the idea that the succession of cultural norms to the next generation are necessary for the health of the family system (James and MacKinnon, 1986). These are important ideas to consider when looking to implement and adapt structural family therapy in a modern context. This critique, however, does not make structural family therapy obsolete to current practice, with a recent study highlighting that it has been shown to be more effective than newer family therapy interventions (Delghandi and Namani, 2024). Importantly this was carried out in a non-western culture, demonstrating its utility in being adapted to other cultures and contexts (Delghandi and Namani, 2024).
Milan family therapy in practice
A key innovation brought into family therapy by Milan was consultation with the observing team (Mitchell et al., 2014). The implementation of someone observing the therapy from a separate location was a groundbreaking concept, whereby they could at the later stages of the session confer ideas, reflections and hypotheses with the lead therapist. However, many have moved away from the behind the screen approach and are adopting post-Milan ideas of being more transparent and less expert led in their use of employing observers, ensuring families can experience the conversations being had with the lead therapist (Mitchell et al., 2014). Tom Andersen was one of the first to do this, promoting the idea of a reflecting team, where the family could witness the conversation between the observers (Andersen, 1987). After families could discuss and share their thoughts with the lead therapist on the reflections discussed, making the overall experience more transparent and inclusive (Andersen, 1987). As family therapy has developed the utility of reflecting teams in the NHS has remained an important component of the intervention.
This has certainly been the approach I have experienced in my current placement, forming a reflecting team in the corner of the room and having open conversations in front of families. As a team we have been discussing the impact that our reflecting teams have been having and have questioned their relevance to certain families. The evidence base indicates that reflecting teams can have impact (Willott et al., 2012), however, it is also important to pitch interventions to meet the needs of families. In my practice I have seen reflecting teams work best when a family engage with a metaphor that conceptualises their difficulties. Currently we are working with neurodiverse families where such reflections appear to have less immediate impact which has led us to re-think how we offer reflections. One idea is that concrete reframing may be more helpful for neurodiverse families who are feeling stuck. Current research supports this idea that certain types of reflecting is more helpful than others for the general population of families seen in family clinics (Hicks et al., 2021). Interestingly this research noted that metaphors were one of the types of reflections that were deemed least helpful. Families reported that, noticing what was talked about, offering expert knowledge, and highlighting something positive were the most useful reflections (Hicks et al., 2021). This is helpful for me to reflect on and integrate into my practice as a reflecting team member. Whilst reflecting teams may not be for every family, they remain a helpful tool for the lead therapist to deploy, helping them to employ reflexivity in the session and to guide their next steps.
Milan’s development of circular questioning has been an area I have been exploring in my practice (Dallos and Draper, 2024). In one session, I used circular questioning to help a mother-daughter relationship process a recent rupture. It helped to take the emotion out of the argument by asking them to share the others perspective. In some regards I have considered circular questioning as a way to encourage individuals to do their own reframing. In this situation, it helped to validate everyone’s position, hearing the other mentalise the others perspective. The following session we drew out a circularity of their rupture-repair cycle (Brown, 2010). Prior to this I used supervision to map out my own circularity of the various stages I had perceived, this meant that I had a blueprint to draw upon if they become stuck. I was amazed at how the mother and daughter engaged in this exercise and how many more steps they identified compared with my own (see Figure 2). From this, we were able to consider how they might perturb the circularity. The mother recognised the negative consequences of placing a demand on her daughter when she is dysregulated and reflected that she should instead step back from such situations to prevent further escalation. These examples illustrate the important contributions Milan has made to the modern-day practice of SFT. Importantly adaptations have been made from the pure implementations of Milan techniques, such as how observing teams have evolved into reflecting teams, parallelled with an evolution of increased transparency for the family. Conceptually, however, Milan’s core ideas remain relevant to supporting families. Demonstration of circularity mapped out with family.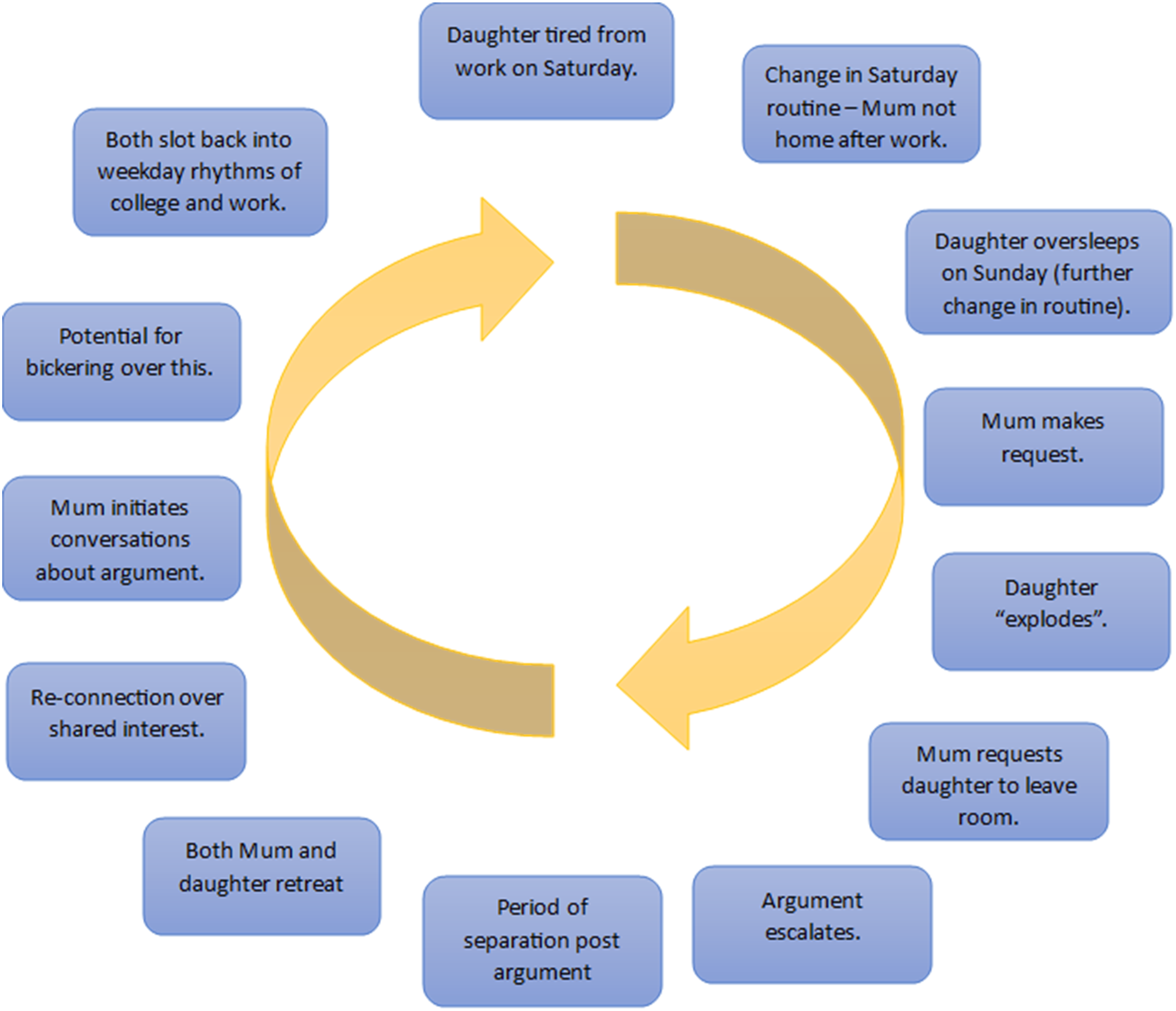
Reflections
I am struck by the skill required to practice SFT and echo the sentiment of Dallos and Draper (2024) who acknowledge ‘the sheer complexity and emotional demand on one practitioner when talking to more than one person at a time’. Conversely, one of the most beneficial aspects of my development has been the fact that you often work in teams when delivering SFT and get to observe different styles and perspectives. I have been fortunate enough to work in a service that regularly uses SFT alongside my academic learning, which has really helped me to put theory into practice.
I think for many of my colleagues studying the foundation in SFT course with me, who had no prior clinical experience of family therapy, the theoretical concepts of SFT were harder to understand and engage with. I wrote the following in my reflective log after listening to my colleague’s views on the first day of the course:
Systemic family therapy sounds wishy washy or indeed pretentious without seeing it in practice. Once you have that frame of reference the language feels more tangible and relevant.
My final thought is that it is a privilege to be permitted to enter the culture and inter-relationships of a family and to begin to understand their shared identity. For me, the process of developing the therapeutic relationship earns the right to offer advice, input ideas and share hypotheses into how the family system can improve.
Conclusion
This paper has provided a concise history of the development of SFT and where it sits within the context of the NHS. There has been a consideration regarding the barriers some families may experience in accessing SFT in the current system. This has been discussed through the lens of the social graces of age, geography and culture. The author has demonstrated how specific models of SFT, namely structural and Milan family therapy have informed their practice in a contemporary NHS context. The relevance that these models have on current practice, which were developed in the 60s and 70s, is striking. Alongside this, it has been necessary to critically reflect on how they need to be adapted to serve the families of 2024. This has looked like questioning the idea that there is normative family life cycle and adapting practices, such as the use of reflecting teams.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.