
Abstract
From the early years of this century, many Western countries adopted the “Dutch Protocol” as a new medical pathway for treating children and adolescents with childhood-onset gender dysphoria. On this approach, gonadotrophin-releasing hormone agonists (GnRHa) were used to suppress puberty, followed by cross-sex hormones (testosterone or oestrogen). This perspective article traces—in each of the countries where we, the authors, live and work—how the Dutch Protocol came to be incorporated into clinical practice or formally adopted into national guidelines. Over time, guidelines across different countries were progressively shaped by a rights-based approach that removed previous safeguards and increased availability of gender-reassignment medical interventions for children and adolescents. From 2010 onward, two developments raised new concerns, generating alternate perspectives and wide-ranging differences in clinical approach. Numerous countries reported an unexpected increase in adolescent-onset presentations, especially among girls. During the same period, an increasing number of individuals who had undergone gender-reassignment medical interventions as minors reported harm and regret. Worldwide, questions were raised about the safety of clinical guidelines for children and adolescents presenting with gender dysphoria. Government bodies in Finland, Sweden, the United Kingdom, and the U.S. state of Florida commissioned systematic reviews pertaining to hormone treatments and issued formal reports. In a parallel process, “conversion therapy” laws, passed in many countries, closed access to exploratory psychotherapy that enables exploration of gender-identity issues from a neutral therapeutic stance. Taken together, these three developments introduced evidence-based and legal considerations into the debate, resulting in tensions that remain unresolved.
Keywords
The emergence of medical interventions for treating gender dysphoria is a modern development. Following a century of scientific and medical developments, clinical guidelines for adult patients were developed in the 1960s by Harry Benjamin, a German-born doctor who worked in the United States (Benjamin, 1966, 1967). In working with adult men with gender dysphoria (then termed transsexualism), Benjamin had determined that psychotherapy was generally unhelpful, thereby justifying the use of endocrine therapy and surgery to “adjust the body to the mind,” or what Benjamin referred to as the patient’s “psychological sex” (p. 115) (Benjamin, 1967). All subsequent guidelines published by the Harry Benjamin International Gender Dysphoria Association (HBIGDA)—founded and officially incorporated in 1979 and renamed as World Professional Association for Transgender Health (WPATH) in 2007—built on Benjamin’s original work.
In the 1990s, in the Netherlands, the guidelines for adults were adapted for treating adolescents (Cohen-Kettenis and van Goozen, 1997). These early guidelines for minors involved comprehensive biopsychosocial assessments (including diagnosis and eligibility for intervention) and, for eligible minors, the use of androgen suppressors for natal males and menstrual suppression with progesterone for natal females. These interventions were to be followed by cross-sex hormones (oestrogen and testosterone) in late adolescence and gender-reassignment surgery in adulthood.
In the late 1990s, clinicians in the Netherlands developed what came to be known as the Dutch Model or Dutch Protocol (Delemarre-van de Waal and Cohen-Kettenis, 2006). The Dutch Protocol—implemented from 1997 onward (van der Loos et al., 2023)—introduced the early use of gonadotropin-releasing hormone agonists (GnRHa), commonly known as puberty blockers, to achieve puberty suppression in children and adolescents (see Text Box 1) (Delemarre-van de Waal and Cohen-Kettenis, 2006). Important aims of the Dutch Protocol were to reduce the distress of children presenting with long-established (from preschool years) gender dysphoria and to improve long-term cosmetic and psychosocial outcomes. Treatment with puberty blockers was also “considered as ‘buying time’ to allow for an open exploration of the SR [sex reassignment] wish” (p. 155) (Cohen-Kettenis and van Goozen, 1998; Delemarre-van de Waal and Cohen-Kettenis, 2006). Brief summary of the Dutch Protocol. The Dutch Protocol was implemented in the Netherlands from 1997 onward. Eligibility criteria included early childhood onset gender dysphoria that was severe and persistent and that met diagnostic criteria (Diagnostic and Statistical Manual of Mental Disorders); psychological stability; and a supportive home environment (Delemarre-van de Waal and Cohen-Kettenis, 2006). The protocol involved the following treatment steps: – diagnostic and psychosocial assessment; – psychological or psychiatric involvement for a minimum period of 6 months before treatment with gonadotropin-releasing hormone agonists (GnRHa) and continuing until surgery; – from age ≥12 years, use of puberty blockers (GnRHa) at onset of puberty (Tanner stage 2 or 3) to halt pubertal development and stop the emergence of unwanted, secondary sex characteristics; – from age 16, use of cross-sex hormones (akin to their use in adults) to produce physical characteristics aligned with the desired gender (testosterone for male gender characteristics and oestrogen for female gender characteristics); – from age 18, gender-reassignment surgeries, to remove unwanted sexual organs and to surgically sculpt organs that align with the desired gender. In following years, the Dutch Protocol for children and adolescents was incorporated into guidelines developed for the Canadian province of British Columbia (de Vries et al., 2006) and by the Endocrine Society (Hembree et al., 2009) and the World Professional Association for Transgender Health (WPATH) (Coleman et al., 2012). Updated guidelines were published by the Endocrine Society in 2017 (Hembree et al., 2017) and WPATH in 2022 (Coleman et al., 2022). Most countries that adopted the Dutch Protocol as national guidelines cited as further authority one or more of these interrelated documents (a practice that has come to be known as circular referencing (Cass, 2024a)).
The majority of countries that adopted the Dutch Protocol did so in the absence of any long-term outcome data. The first early data began to emerge from 2006 onward (de Vries et al., 2014; Delemarre-van de Waal and Cohen-Kettenis, 2006). To mitigate risk and to implement safeguards, most countries initially established multidisciplinary teams that conducted comprehensive assessments—including screening of patients to ensure that they met diagnostic eligibility criteria—and that implemented treatment using a bio-psychosocial (holistic) approach. The overarching idea was that in the absence of an adequate evidence base, biopsychosocial practice—best practice in paediatrics and child and adolescent psychiatry (AAP, American Academy of Pediatrics Committee on Psychosocial Aspects of Child Family Health, 1982, American Academy of Child and Adolescent Psychiatry, 2012; Henderson and Martin, 2014; Wilson and Lawman, 2009)—was the best means of protecting patient safety. Presumably, when outcome data from formal research studies became available, practice guidelines could be adjusted to align with evidence-based standards of care.
Adoption of the Dutch Protocol and the introduction of national Guidelines for the treatment of gender dysphoria in minors; civil rights laws for legal change of sex in the civil registry; and the passing of conversion laws.
aCountries that have instituted national guidelines are listed in the order in which the Dutch Protocol was first adopted in clinical use. Alphabetical order is used (starting with Australia) for the countries that have not developed national guidelines.
Ameli.fr, Internet site for Assurance Maladie (French health insurance); COHERE, Council for Choices in Health Care in Finland; ETENE, National Advisory Board on Social Welfare and Health Care Ethics (Finland); GIDSEEN, Working Group on Identity and Sexual Development of the Spanish Society of Endocrinology and Nutrition; IGAS, Inspection générale des affaires sociales (France); RIZIV/INAMI, National Institute for Health and Disability Insurance (Belgium); UKOM, Norwegian Healthcare Investigation Board; WPATH, World Professional Association for Transgender Health.
Tracking and understanding these developments is timely and important because of the marked changes that have occurred in the field of gender medicine since the introduction of the Dutch Protocol and especially over the last decade or so: the large increase of children and adolescents presenting to gender clinics across Western democracies; a change in demographics, with a shift to a predominance of adolescent natal females with high rates of mental health comorbidities and adverse childhood experiences; the ongoing lack of an adequate evidence base concerning the safety and effectiveness of gender-reassignment medical interventions in this new cohorts of patients; new models of care involving fewer safeguards (such as the optional use biopsychosocial assessment and formal diagnosis); the increasingly common emergence of individuals who underwent gender-reassignment interventions as minors and who are now reporting harm and regret; and the realization (by some detransitioners) that mental health issues or reactions to abuse or past trauma had sometimes been mistaken for gender dysphoria. It is a good time to take a step back and reconsider the present state of the field.
As the reader will see, this perspective article documents the wide variation in guidelines and clinical practice around the world, both between and within countries. In the final, concluding section of the article, we step back and consider the pattern of our findings. Grouped along one end of the spectrum are guidelines informed and strongly shaped by a rights-based approach that emphasizes self-determination, identity and body autonomy, fulfillment of expressed needs, depathologization, and elimination of discrimination. Grouped along the other end of the spectrum, in developments influenced by the rise of evidence-based medicine, are guidelines centring on patient safety and evidence-based standards of care. At present, it remains to be seen how the tension between the two different approaches for children and adolescents will be worked out across time.
Terminology.
DSM, Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1980, American Psychiatric Association, 1994, American Psychiatric Association, 2000, American Psychiatric Association, 2013, American Psychiatric Association, 2022); GID, gender identity disorder; ICD, International Classification of Diseases (World Health Organization, 1992, World Health Organization, 2018).
International adoption of the Dutch Protocol
Spain: Adoption of the Dutch Protocol and related guidelines from 1999
The landscape of gender care in Spain has changed and evolved unevenly across the country’s different autonomous regions. Multidisciplinary, publicly funded assistance for individuals with gender dysphoria was first introduced in Andalusia’s public health care system in 1999 (Esteva de Antonio et al., 2002). A cohort of the first 100 patients included adolescents 15–17 years of age (Esteva de Antonio et al., 2001). Local and national health authorities also started drafting standards of care modelled on the Dutch Protocol in the Netherlands (see Text Box 1) (Bergero Miguel et al., 2004). The health care available developed gradually throughout the country via the creation of new, specialized gender-identity units in 10 of the 17 country’s autonomous regions (Esteva de Antonio et al., 2012; Gómez-Gil et al., 2019).
Initially, gender identity units were multidisciplinary teams of psychologists, psychiatrists, endocrinologists, and surgeons with experience in treating gender dysphoria (Esteva de Antonio et al., 2012). These clinicians later formed the Working Group on Identity and Sexual Development of the Spanish Society of Endocrinology and Nutrition (GIDSEEN, by its Spanish initials) (Gómez-Gil et al., 2019) and published comprehensive national clinical practice guidelines (Moreno-Pérez et al., 2012) and Spain-based research (Gómez-Gil et al., 2020). The guidelines closely resembled those of the WPATH (Coleman et al., 2012) and the Endocrine Society (Hembree et al., 2009), including the use of puberty blockers and cross-sex hormones off-label, when treating minors (see Text Box 1) (Esteva de Antonio et al., 2014). The 2012 guidelines were framed within a biopsychosocial model that stressed the importance of conducting extensive assessments, applying eligibility criteria, and providing psychotherapeutic support throughout the gender transition process.
Starting in 2014, and following a period of intense lobbying and criticism from transgender organizations (Mas Grau, 2022; Missé and Coll-Planas, 2010), laws focusing on depathologization and gender-identity self-determination were approved in some autonomous regions. These laws, drafted largely with input from activist representatives and little advice from medical professionals, resulted in the development of new models of care that decentralized gender care away from gender-identity units, excluded mental health assessments, and created localized endocrinological points of care as the entry gateway to medical treatment, including gender-reassignment surgeries (Gómez-Gil et al., 2019).
At that time, and in response to these changes, GIDSEEN released a position statement that expressed concern and called for caution—most notably, when working with minors (Esteva de Antonio et al., 2015). GIDSEEN subsequently released a review article identifying the risks associated with the emerging configuration of gender care (Gómez-Gil et al., 2020). In line with concerns in other European countries (Kaltiala et al., 2020; Kaltiala-Heino et al., 2015), GIDSEEN noted the importance of psychological assessment, especially in the case of adolescents with rapid-onset gender dysphoria (Gómez-Gil et al., 2020).
More recently, however, some professionals working at gender identity units have shifted their position toward a more permissive approach for minors—what they call “the gender affirmation path” (p. 349) (Moral-Martos et al., 2022). These clinicians advise that support should be individualized and that the process “should not be diagnostic, that is, in no case can the minor be subjected to an evaluation or any other intervention involving the determination of the minor’s identity by a third party” (p. 349) (Moral-Martos et al., 2022).
In February 2023, Spain passed a new national law, Ley 4/2023, endorsing and fostering the principles of depathologization and self-determination (see Table 1). The new law—coupled with the patient autonomy law, Ley 41/2002 (see Table 1)—enables under-18s (or under-16s, depending on the region) to access medical treatment subject to parental consent (subject to family agreement).
At present, no long-term studies have assessed the outcomes of the new models of care implemented in the country. Ley 4/2023 introduced a prohibition of conversion therapies (see Table 1).
Sweden: Adoption of the Dutch Protocol in the early 2000s
Until the turn of the century, children and adolescents with gender dysphoria were not managed within Swedish health care (Frisen et al., 2017). From the early 2000s, however, the Stockholm Child and Adolescent Mental Health Services began to implement a modified version of the Dutch Protocol using a multidisciplinary approach (see Text Box 1). In 2015, Socialstyrelsen, the Swedish National Board of Health and Welfare, issued formal guidelines for minors that institutionalized previous practice (Socialstyrelsen, 2015). The guidelines recommended that assessment and treatment be carried out in multidisciplinary teams, and specified “counselling, including psychotherapy [to explore their gender identity and reduce mental illness] and psychosocial support [as] a prerequisite for quality care of gender dysphoria.” They stated: “Healthcare should offer puberty-blocking hormone treatment to young people to reduce their suffering. Older adolescents should also be offered treatment with gender-affirming hormones to initiate a puberty development that is in accordance with their gender identity.”
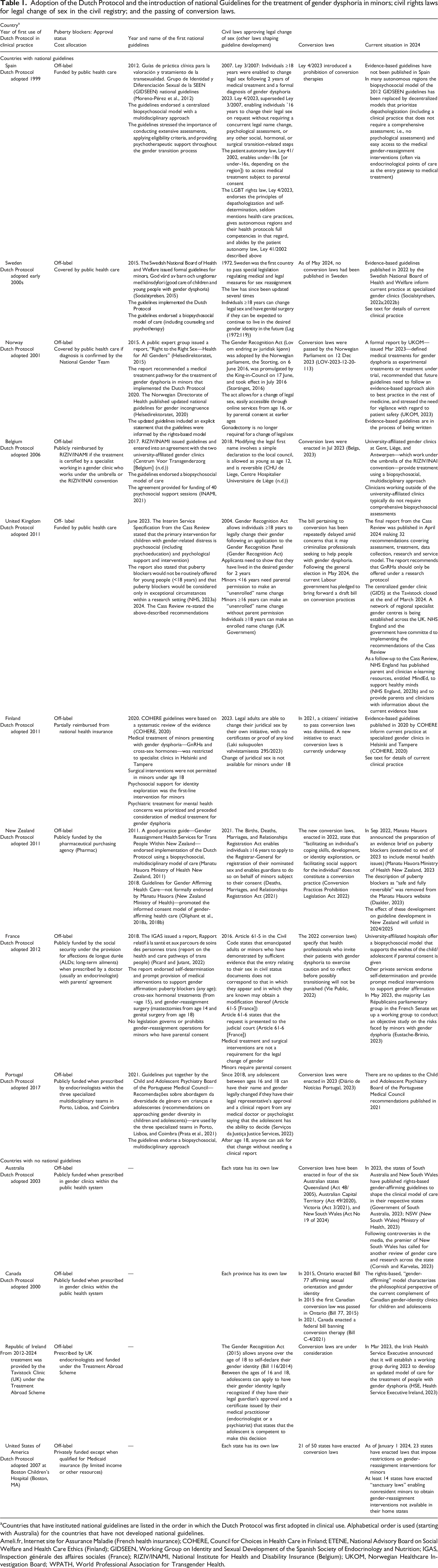
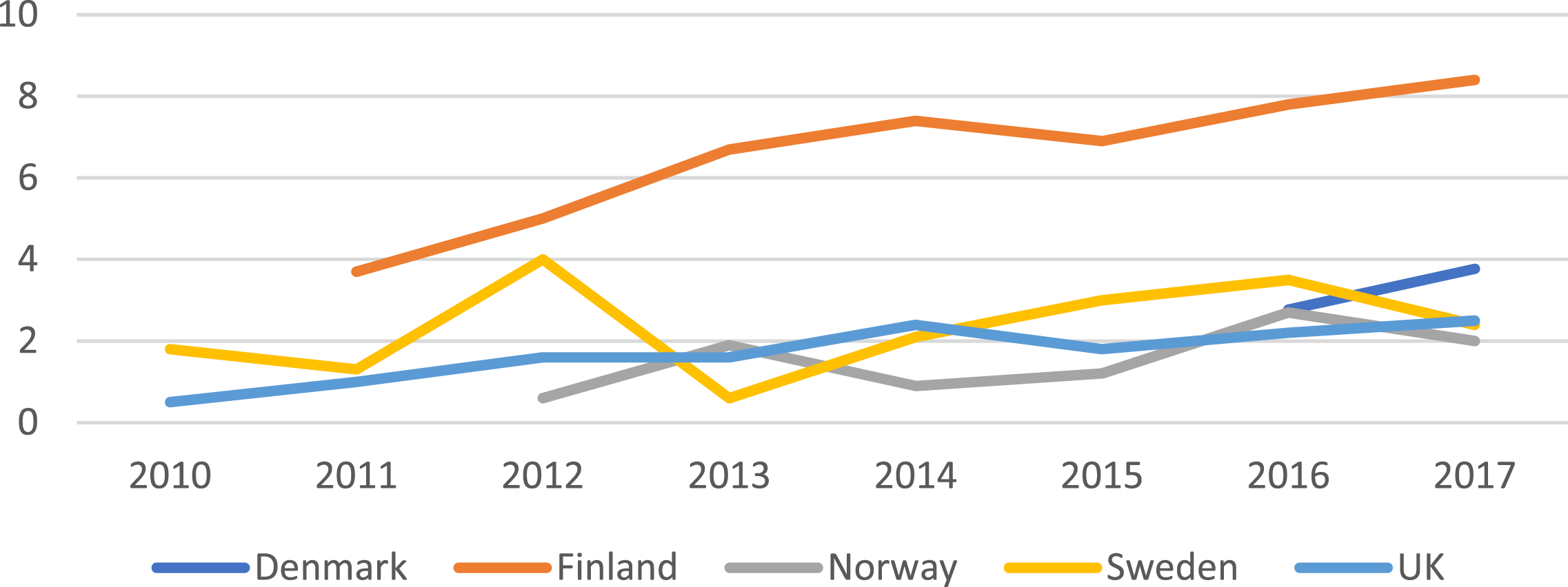
In 2018, in the wake of concerns about the increasing number of young people seeking gender-affirming care (see Figure 1) (Kaltiala et al., 2020; Landén, 2019; Socialstyrelsen, 2017), the government asked the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) to review the evidence for hormone treatments for children (up to age 18 years). This development resulted in a systematic review and the subsequent inclusion of an evidence-based perspective in guideline development in Sweden. The flow-on effects (resultant effect) of these events are discussed in the next main section (“Diverging Pathways”). Referrals to child and adolescent gender identity services 2010–2017 in four Nordic countries. Reproduced from Kaltiala et al., 2020, with permission of Taylor and Francis (Copyright Clearance Center).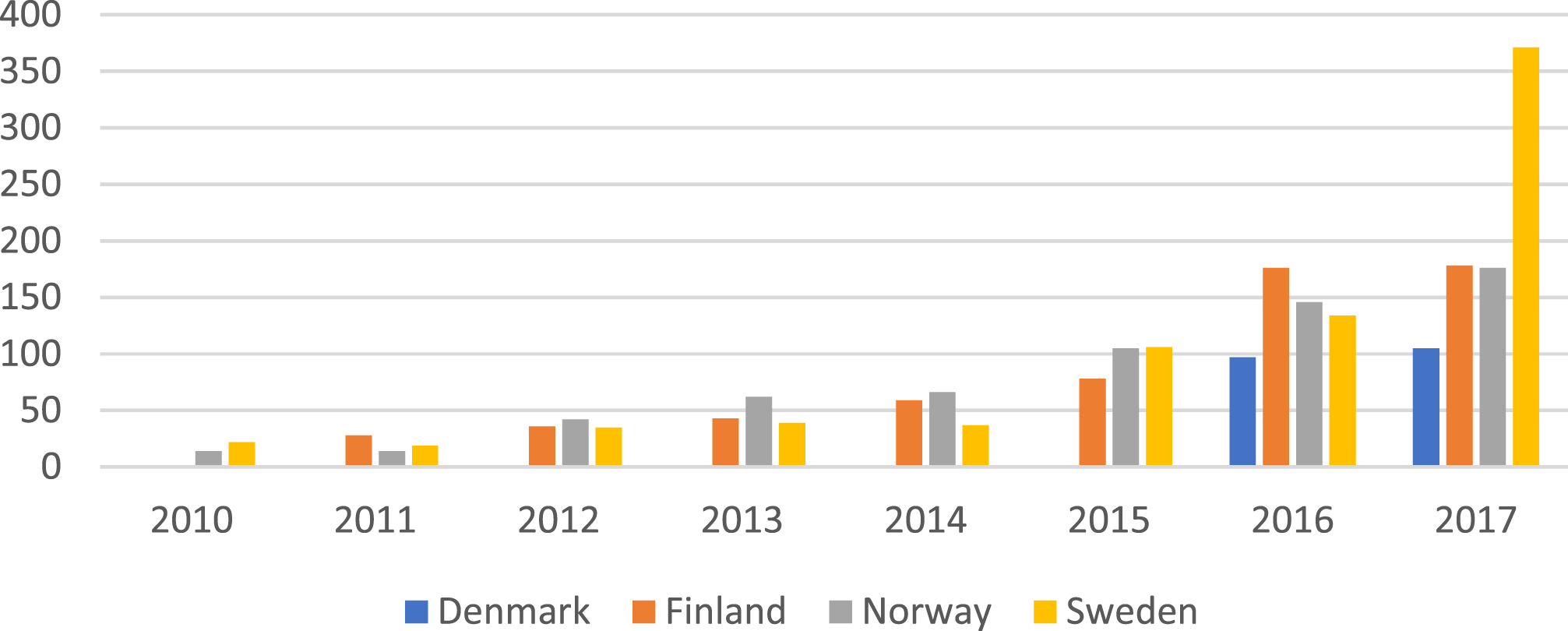
Norway: Adoption of the Dutch Protocol in 2002
In 2001, in response to a directive from Helsedirektoratet, the Norwegian Directorate of Health, Norway established the National Gender Team, at Oslo University Hospital. This multidisciplinary service—made up of psychologists, psychiatrists, endocrinologists, and surgeons—adopted the Dutch Protocol for treating minors (Helsedirektoratet, 2015). It registered its first child patients in 2002.
In 2013, a public expert group was formed to review the health service’s provision of care regarding gender incongruence and gender dysphoria. The group’s report, “Right to the Right Sex—Health for All Genders” (Helsedirektoratet, 2015), recommended the use of puberty blockers from Tanner stage 2 and cross-sex hormones from age 16, in accordance with the Dutch Protocol (see Text Box 1). The report put considerable emphasis on the rights of the child—including the “the right of the child to preserve his or her identity” (p. 77) as per Article 8 in the United Nations Convention on the Rights of the Child (United Nations, 1989).
In 2017, due to the large increase in referrals (see Figure 1), a National Gender Team specifically for children and adolescents was established at Oslo University Hospital (Wæhre and Schorkopf, 2019). Referrals came from local child and adolescent mental health outpatient clinics following completion of a biopsychosocial assessment.
In Oslo, from 2002, a community health care service for youth has made puberty blockers and cross-sex hormones available to minors, though with no financial coverage through the state drug authority (Legemiddelverket, the Norwegian Medicines Agency). This service is not affiliated with the National Gender Team at the university hospital. It is described as being LGBTQIA+ friendly, with “an affirmative approach.” It has no child and adolescent physicians and requires no psychiatric assessment.
In 2020, the Norwegian Directorate of Health published updated national guidelines for gender incongruence (Helsedirektoratet, 2020). The guidelines were formulated as part of the government’s “action plan against discrimination on grounds of sexual orientation, gender identity and gender expression (2017–2020)” (Norwegian Ministry of Children and Equality, 2016). They included an explicit statement that the guidelines were informed by the rights-based approach: the need to address the issue of discrimination and to provide “nondiscriminatory health care and support” (p. 45 translation via Google Translate) (Helsedirektoratet, 2020).
In 2023, in response to “notifications of concern from patients’ family members, clinicians, and others” (p. e1) (Block, 2023b), the 2020 Norwegian guidelines (Helsedirektoratet, 2020) were criticized by the Norwegian Health Care Investigation Board (UKOM) (UKOM, 2023). A key recommendation made by UKOM was that future guidelines needed to follow an evidence-based approach akin to best practice in the rest of medicine. The current situation in Norway, following this development, is discussed in the next main section (“Diverging Pathways”).
Belgium: Adoption of the Dutch Protocol in 2006
The trilingual country of Belgium has three gender clinics. All are affiliated with university hospitals—Universitair Ziekenhuis (in Gent), Centre Hospitalier Universitaire de Liège, and Universitair Antwerpen. The Gent clinic has provided care for minors as of 2006, the Liège clinic as of 2019, and the Antwerp clinic as of 2024. The clinics have all adopted the Dutch Protocol. They currently follow the WPATH 8 guidelines (Coleman et al., 2022). In line with these guidelines, their websites state that it is important and necessary to pay particular attention to psychological difficulties during the assessment process but that these concerns must not be a barrier to access. Data show that the number of children accessing puberty blockers continues to rise, with a predominance of adolescent natal females who have high rates of comorbid mental health conditions (Van Cauwenberg et al., 2020).
Medical care for minors with gender dysphoria is funded by the Belgian health insurance system under an agreement (2017 onward) between the National Institute for Health and Disability Insurance (RIZIV/INAMI) and the three university-affiliated gender clinics. The Convention specifies that clinical care must be provided by multidisciplinary teams. It mandates and funds a total of 40 psychosocial support sessions—individual, family, and group sessions for young people diagnosed with gender dysphoria who decide to undertake the transition process. Due to the increased waiting lists, other clinics, which already provide transgender care, are currently waiting for the approval of RIZIV/INAMI to be part of the Convention, which would provide public funding.
Clinicians working outside the mandated university settings do not require preliminary exploratory interviews or the same level of assessment that is mandated by the RIVIZ/INAMI-approved programs.
At present, no long-term Belgian outcome studies have been conducted. Belgium enacted conversion laws in July 2023 (see Table 1).
United Kingdom: Adoption of the Dutch Protocol in 2011
The Gender Identity Development Service (GIDS), led by Dr Domenico Di Ceglie, opened in 1989 at St George’s Hospital and moved to the Tavistock and Portman NHS Foundation Trust (the Tavistock) in 1994. In the early years, the service provided support to young people from around the United Kingdom presenting with distress around gender identity. In the 1990s, a small minority of patients, aged around 16 years, began to be referred to endocrinologists for treatment with antiandrogens or suppression of menstruation with progesterone. An audit of the first 124 patients (predominantly male, from 1989) showed that the patients, at assessment, demonstrated high rates of depression, family problems (including mental and physical illness in the family), and relationship difficulties with peers (Di Ceglie et al., 2002).
Royal College of Psychiatrists guidelines written at that time emphasized supportive psychotherapy and treatment of comorbid problems, with the aim of reducing distress. If hormonal treatments were initiated, they were be used with caution, ideally delaying any physical interventions “as long as is clinically appropriate” (p. 5) (RCP, 1998). From 1998, GnRHa began to be used with adolescents >16 years “to induce a sex-hormone-neutral environment to provide young people with space to decide whether to progress further with gender reassignment treatment as an adult” (GIDS, 2021).
By 2005, GIDS staff experienced increasing pressure from patients, parents, society, and groups such as Mermaids (a UK charity supporting transgender people) to recommend early prescription of hormonal treatments (as per the Dutch Protocol) (GIDS, 2021; Taylor, 2005). The lack of evidence around the use of puberty suppressants in this patient group was formally noted (Taylor, 2005). Also in 2005, Mermaids and another charity, the Gender Identity Research and Education Society (GIRES), organized a conference to develop guidelines for hormone treatment of children with gender dysphoria in the United Kingdom (GIRES, 2005). The conference was attended by the GIDS leadership. The Dutch group—Henriette Delemarre-van de Waal and Peggy Cohen-Kettenis—presented their approach on the use of puberty suppressants in early puberty as part of the Dutch Protocol (see Text Box 1). The mid-2000s onward saw increased leniency in the clinical community—and position statements put out by key medical societies—regarding the use of puberty blockers (BSPED, 2005, 2009, RCP, 2013) (see Supplemental Text Box 1).
In 2011, GnRHa were made available to children from 12 years of age, under the framework of research, in the Early Intervention Study (Carmichael et al., 2021; GIDS, 2021). By 2014, Polly Carmichael, who succeeded Di Ceglie as clinical director of GIDS, had adopted the Dutch Protocol for all clinical practice and had made the decision to prescribe puberty blockers unrestricted by age limits (Manning and Adams, 2014).
Between 2012 and 2015, there was an uptick in referrals, with a dramatic increase in the number of natal females (see Figures 2 and 3). This increase put considerable strain on the service; long waiting times for initial assessments became the norm; and more patients were referred for hormonal treatments, and with less comprehensive assessment (Barnes, 2023; Cass, 2022). Staff also noted the disproportionate number of children with autism spectrum disorders and other complex mental health issues (Barnes, 2023). For more detail about this difficult period, see Barnes (2023). Referrals to child and adolescent gender identity service 2010–2017 in the UK. Notice that the scaling is different from that in Figure 1. Reproduced from Kaltiala et al., 2020, with permission of Taylor and Francis (Copyright Clearance Center). Development of female:male ratio among children and adolescents referred to gender identity services. Reproduced from Kaltiala et al., 2020, with permission of Taylor and Francis (Copyright Clearance Center).
In 2019, a former GIDS patient, Keira Bell, and a parent of a former patient referred to as Mrs. A, filed a legal action against the Tavistock, arguing that GIDS’s approach was unlawful because children could not give informed consent to treatment with puberty blockers. Akin to previous concerns raised by clinicians (Bannerman, 2020; Barnes, 2023; Taylor, 2005), the Keira Bell case had highlighted concerns pertaining to patient safety, the capacity of minors to consent to irreversible treatment, the risk of clinician error, the lack of long-term outcome data (including rates of desistance and detransition), and the thin nature of the overall evidence base. Against this background, in September 2020, the National Health Service (NHS) announced an independent review of GIDS, which came to be known as the Cass Review (Cass Review, 2020). Two months later, in December 2020, the High Court found in favour of the claimants (Bell v. Tavistock, 2020). In September 2021, however, the High Court decision was overturned by the Court of Appeal, which held that it was for doctors, rather than the courts, to decide whether children had capacity to consent to puberty suppression (Bell v. Tavistock, 2021).
Also in 2021, the Tavistock published data from the Early Intervention Study (Carmichael et al., 2021). This study was an attempt to replicate Dutch findings showing improved mental health outcomes for children and adolescents receiving puberty blockers (de Vries et al., 2011). In contrast to expectations (and information that the charities gave to parents [Barnes, 2023]), the study showed that prescription of GnRHa had no effect—positive or negative—on the children’s mental health. A 2023 reanalysis of the data showed that mental health following GNRHa treatment—measured across self- and parent-report scales—deteriorated in 15% to 34% of children and improved in 9% to 20% of children (McPherson and Freedman, 2023).
The flow-on effects of the Cass Review on guideline development—and the current situation in the United Kingdom—is discussed in the next main section (“Diverging Pathways”).
Finland: Adoption of the Dutch Protocol in 2011
In Finland, gender identity assessments were opened for minors in 2011. This followed a politically driven discussion of whether limiting these assessments to adults was discriminatory. The departments of adolescent psychiatry at Helsinki University Central Hospital and Tampere University Hospital—the two hospitals with adult gender clinics—were given the task of arranging the service for minors, delivered by multidisciplinary teams.
At that time, the most prominent treatment model—the Dutch Protocol (see Text Box 1)—suggested that a gender-identity service for minors would entail working with young people with childhood-onset gender dysphoria that intensified in puberty. A basic theoretical foundation of adolescent psychiatry is that adolescence is the most important developmental phase of identity formation and that identity consolidation is the outcome of successfully completed adolescent development. Against this background it was problematic to assume that one facet of identity development—namely, gender identity—would be sufficiently consolidated in early adolescence to justify interventions on healthy bodies. The Finnish gender-identity services therefore obtained a position statement from ETENE, the National Advisory Board on Social Welfare and Health Care Ethics (ETENE, 2011). In 2011, ETENE acknowledged the risks related to immaturity and suggestibility (particularly of younger minors) and advised cautious assessment and case-by-case treatment decisions. ETENE advised that clinicians at all levels of care (for minors) build competencies in supporting minors who are distressed by gender issues and that specialized gender-identity services be involved when medical gender reassignment needs to be considered. The number of such patients annually was expected to be very small.
What happened in reality was quite different (see Figures 1 and 3). From the very beginning, referrals to the nationally centralized units concerned mainly biological females (>85%) who had first experienced gender distress in middle adolescence (15–17 years of age), well after the onset of puberty (Kaltiala-Heino et al., 2015). Most importantly, 75% presented with severe psychiatric disorders and with psychiatric histories dating far before the onset of gender dysphoria (Kaltiala-Heino et al., 2015). The annual number of referrals also soon vastly exceeded expectations (Kaltiala et al., 2020). The same trends—high rates of referral, with a preponderance of female adolescents—were documented in gender-identity services in Toronto and Amsterdam (Aitken et al., 2015), and in Denmark, Norway, Sweden, and the United Kingdom (Kaltiala et al., 2020). Moreover, the outcome of hormonal gender-reassignment interventions was beginning to appear less favourable than expected (Kaltiala et al., 2020). For example, treatment with cross-sex hormones did not alleviate the overall need for psychiatric treatment, and adolescents who experienced problems in school, peer relationships, and managing everyday matters outside of home continued to experience problems in these areas following treatment with cross-sex hormones.
Observing these developments, the adolescent and adult psychiatrists from the two Finnish centers approached the Council for Choices in Health Care in Finland (COHERE Finland). The council is responsible for issuing recommendations regarding services that should be provided under the umbrella of public health services—including the development of guidelines for treating gender dysphoria.
The COHERE committee for this topic was formed in 2019. It utilized an evidence-based medicine approach to inform its recommendations. We discuss these recommendations and subsequent developments in Finland in the next main section (“Diverging Pathways”).
New Zealand: Adoption of the Dutch Protocol in 2011
In 2010, New Zealand’s Ministry of Health, following a Human Rights Commission report in 2008 (Human Rights Commission, 2008), contracted for a project to help clinicians work with trans people. The resulting “good practice guide,” Gender Reassignment Health Services for Trans People Within New Zealand (Manatu Hauora, 2011). These 2011 guidelines endorsed the Dutch Protocol including: a comprehensive assessment (including a psychosocial assessment); diagnosis by a mental health professional; treatment with GnRHa prior to the age of 16 years (from Tanner stage 2); treatment with cross-sex hormones from “about” age 16 (p. 33); and sex-reassignment surgery “not normally” before age 18 (p. 28). The protocol repeatedly cautioned about the serious side effect of infertility (starting with GnRHa) and the fact that “very few children who express gender variance go on to identify as trans adults” (p. 30). “Although the guidelines highlighted the importance of family involvement and ‘a high level of consent’ (p. 31),” they also stated that “in exceptional circumstances if the young person is under 16 and deemed Gillick competent they alone may be allowed to consent” (p. 31) to initiation of puberty blockers or cross-sex hormones.
In 2018, separate from the Ministry of Health, a group of researchers and clinicians published Guidelines for Gender Affirming Health Care (Oliphant et al., 2018a, 2018b). These guidelines, endorsed by the Australian and New Zealand Professional Association of Transgender Health (ANZPATH) 1 but not by the ministry, were strongly influenced by the rights-based approach, and they dropped previous safeguards. The guidelines follow the informed consent model of gender-affirming health care, which aims to “respect the self-determination of each person as being the expert on their experience” (p. 22) (PATHA, 2018). Compared to the Ministry of Health’s 2011 guidelines, the ANZPATH-endorsed guidelines published in 2018 downplay the likelihood that gender dysphoric children will desist. While noting that cross-sex hormones should, in general, not be available until age 16, the 2018 guidelines state that there may be “compelling reasons” for starting younger (p. 88) (Oliphant et al., 2018b). These guidelines establish no lower age limit for accessing puberty-blocking hormones. Although it includes assessment for gender dysphoria, mental health assessment is not mandatory.
In 2023, a group of researchers and clinicians published the Primary Care Gender Affirming Hormone Therapy Initiation Guidelines for adults (from age 16) (Carroll et al., 2023). These guidelines have been endorsed by the Royal New Zealand College of General Practitioners (PATHA, 2023) but not by the Ministry of Health. These 2023 guidelines take the informed consent model a step further by removing the requirement for a diagnosis of gender dysphoria: “It is not the role of a health professional to make a judgement on whether a patient’s gender (e.g., a non-binary gender) is valid or whether a patient is male or female enough” (p. 1). The guidelines remove the requirement for a mental health assessment. Another new aspect is to acknowledge the phenomenon of detransitioning, while reassuring doctors that it is not their problem if a patient later regrets treatment: “Some providers may feel anxious about ‘getting it wrong’ or worry that their patient may later regret their decision. The informed consent process outlined in this document respects the autonomy of the patient as a competent adult who has the capacity to make their own decisions about their body and health once they have been given the necessary information” (p. 32). If the patient decides to stop hormones, “This is not—and should not—be viewed as a mistake or a failure” (p. 32).
At present, no long-term New Zealand outcome studies have been conducted. Data about GnRHa prescribing for minors—in the years 2006–22—show that New Zealand’s rate of use (110 per 100.000) was 11 times that in the United Kingdom (9 per 100,000) (Paul, 2023), presumably reflecting the permissive nature of the New Zealand guidelines.
In 2022, New Zealand passed the Conversion Practices Prohibition Legislation Act 2022 (see Table 1). The legislation (section 5(2)(e)) states that “facilitating an individual’s coping skills, development, or identity exploration, or facilitating social support for the individual” does not constitute a conversion practice (section 5(2)(e)). An evidence brief of puberty blockers—undertaken by the Ministry of Health—is currently underway (Gower, 2023).
France: Adoption of the Dutch Protocol in 2012
France adopted the Dutch Protocol in 2012. 2 Consultations at university affiliated gender clinics are conducted by multidisciplinary teams involving “somatic doctors” and psychiatrists. Since 2015, these multidisciplinary consultations have included representatives from transgender associations such as Trans Santé France (FPATH Trans santé France). During the multidisciplinary meetings, the medico-surgical indications are considered, and decisions are made collectively. Psychotherapeutic follow-up is not systematic. The aim of the consultation is to promote an intervention based on the young person’s self-determination, words, and feelings. The consultations provide young persons with all the tools they need to support transition. This may include referrals to endocrinologists (e.g., for puberty blockers), surgeons, child psychiatrists, psychotherapists, group therapy, mediation, or fertility consultation, as well as to family therapists or support groups for parents. If the young person is a minor, the consent of the adolescent and both parents is required. As of 2018, 9 hospital-based clinics had opened across 6 of the country’s 13 administrative regions (HAS, 2022).
In 2021, the Ministry of Health contacted the independent scientific authority, the Haute Autorité de Santé (HAS), 3 to update the recommendations for the care pathway for transgender people. The Ministry of Health also commissioned the Inspection générale des affaires sociales (IGAS; General inspection of social affairs) to prepare a report (IGAS Report) 4 assessing, from both a medical and psychosocial perspective, the current situation and prospective needs of transgender people in France.
The IGAS report advocated a care pathway for transgender people based on self-determination and depsychiatrization—elimination of the requirement for psychiatric assessment and diagnosis (Picard and Jutant, 2022). The report recommended puberty blockers (any age, deeming the effects reversible), cross-sex hormonal treatments (prescribed beginning around age 15), and gender-reassignment surgery (mastectomies being permitted from age 14 and genital surgery from age 18).
Among medical authorities, only the Academy of Medicine, in February 2022, has advocated caution (ANM, 2022). Its opinion is advisory. The academy drew attention to the rise in sudden-onset gender dysphoria in natal females and suggested that it is essential to provide, first of all, a medical and psychological support to these children or adolescents, but also to their parents, especially since there is no test to distinguish a “structural” gender dysphoria from transient dysphoria in adolescence. Moreover, the risk of over-diagnosis is real, as shown by the increasing number of transgender young adults wishing to “detransition.” It is therefore advisable to extend as much as possible the psychological support phase (p. 2).
Clinical care can also be sought through a state funded organization, Le Planning Familial. This organization promotes self-determination and gender affirmation, and facilitates quick prescription of cross-sex hormones at the request of adolescents without assessment or psychological support. Hormonal treatments by private medical practitioners can be delivered on demand after one or two consultations.
At present, no long-term French outcome studies are available. Conversion laws were passed on 31 January 2022 (see Table 1). In contrast to other countries, the text of the law specifies that health professionals who invite their patients to exercise caution and to reflect before possibly transitioning will not be subject to prosecution. As of May 2023, a parliamentary review of risks faced by minors with gender dysphoria is underway (Eustache-Brinio, 2023).
Portugal: Adoption of the Dutch Protocol in 2017
In 2017, the Child and Adolescent Psychiatry Board of the Portuguese Medical Council created a workgroup to develop clinical recommendations for working with gender-diverse children and adolescents. The recommendations, along the lines of the Dutch Protocol, were adopted as guidelines in 2021 and implemented thereafter (Prata et al., 2021). The guidelines recommend the creation of three specialized multidisciplinary teams across the country. These were assembled in Porto, Lisboa, and Coimbra. The teams are charged with seeing all minors seeking hormone therapy. Each patient is assessed for persistent gender dysphoria, the ability to give informed consent, and complex comorbid health disorders. The initiation of puberty blockers and cross-sex hormones—prescribed off-label—is a team decision. Surgeries that involve gonadectomy or hysterectomy are recommended only after age 18. Breast surgery prior to age 18 needs to be discussed within a multidisciplinary team, with no defined requirement for a minimum age.
No statistics are available on referrals to, or the current clinical practice of, these specialized teams—or even any statistics on gender-nonconforming children and adolescents attending mental health care. At present, no updates have been made to these recommendations. Portuguese laws prohibiting conversion therapy were approved in 2023 (see Table 1).
Diverging pathways: The progressive emergence of an evidence-based approach to guideline development
In this section we focus on the diverging pathways of Finland, Sweden, the United Kingdom, and Norway, whose guideline development changed direction as the growing evidence base concerning medical interventions for children and adolescents with gender dysphoria began to raise concerns about clinical outcomes and safety of those interventions (see previous sections). Of particular note were the rapid increase in gender dysphoria, especially among natal girls with comorbid mental health conditions (see previous sections); concerns about children’s immaturity or their capacity to provide consent (de Nie et al., 2023; Kozlowska et al., 2021; Latham, 2022; Levine et al., 2022; Nahata and Quinn, 2020); uncertainty about the benefits versus harms of puberty suppression (especially on brain development) (Baxendale, 2024; Chen et al., 2020; Schneider et al., 2017); future sexual function (Bowers, 2022; van de Grift et al., 2020) 5 ; future fertility (de Nie et al., 2023; Johnson, 2023); lack of long-term data on persistence, in addition to detransition and regret in this new group of patients (Boyd et al., 2022; Hall et al., 2021; Roberts et al., 2022; Turban et al., 2021); growing uncertainty as to whether gender-reassignment improved psychiatric morbidity (or not) in this new group of patients (Kaltiala et al., 2020; Ruuska et al., 2024); concerns about treatment models that depart from normal medical norms requiring a diagnosis that follows a comprehensive assessment process (Esteva de Antonio et al., 2015; Jorgensen, 2023a; Littman et al., 2024; Paul, 2023); and feedback from detransitioners—beginning with individual testimonies (Bell, 2020; Helena, 2022)—that their treating clinicians had failed to provide them with “a more robust discussion of risks/benefits of interventions prior to treatment decision-making” (p. 1) (MacKinnon et al., 2023) or that mental health issues or reactions to abuse or past trauma had been mistaken for gender dysphoria (Littman, 2021; Littman et al., 2024). From 2015 onward, Finland, Sweden, the United Kingdom, and Norway commissioned national bodies to consider the need for new guidelines to reflect the framework of evidence-based medicine. In mid-2023, France established a Senate working group to look the same issues and consider potential changes in legislation. And during the writing of this article, the centralized gender clinic in Denmark has also restricted the use of puberty blockers, cross-sex hormones, and gender-reassignment surgery in minors (Hansen et al., 2023). Also during the writing of this article, an updated German systematic review re-examined the current evidence of using puberty blockers and cross-sex hormones in minors with gender dysphoria (Zepf et al., 2024). The review confirmed low certainty using modified GRADE criteria and concluded that “current evidence does not clearly suggest that [gender dysphoria] symptoms and mental health significantly improve when PB [puberty blockers] or CSH [cross-sex hormones] are given to minors” with [gender dysphoria] (English supplement, p. 3).
Finland: Council for Choices in Health Care in Finland report
In Finland, a research study published in 2015 by the gender clinic in Tampere showed a concerning trend in the socio-demographics of clinical presentations: a steep increase in rates of referral with a preponderance of natal girls who had first experienced gender dysphoria well after the onset of puberty (also known as late-onset gender dysphoria) (see Figures 1 and 3) (Kaltiala-Heino et al., 2015). In addition, a subsequent study showed that, contrary to expectations, mental health outcomes did not improve in the cohort of Finnish adolescents treated with cross-sex hormones (Kaltiala et al., 2020). Psychiatrists from the two Finnish centers communicated their concerns to the Council for Choices in Health Care in Finland (COHERE Finland).
The COHERE committee—formed in 2019—obtained a systematic review from an independent expert group: the evidence base for early medical intervention was found to be weak (Pasternack et al., 2019). In June 2020, COHERE issued new recommendations for treating children with gender-related distress (COHERE, 2020). − Psychosocial support for identity exploration—provided in school and primary healthcare settings—is recommended as the first-line intervention for minors. − Before specialized assessment for medical interventions can be considered, any necessary psychiatric treatment and, when indicated, psychotherapy need to be provided by appropriate local services. − Assessment for medical interventions is restricted to the specialized, multidisciplinary, tertiary care units of Helsinki University Central Hospital and Tampere University Hospital. − If indicated, hormonal interventions before legal adulthood may include both GnRHa to halt pubertal development and cross-sex hormones, but surgical interventions are not permitted under age 18.
COHERE also prompted the specialized gender-identity services to begin collecting data and to generate research concerning the following: referral patterns and changes in patient mix (e.g., early- and late-onset gender dysphoria); persistence of the identity experience on long-term follow-up; reasons for withdrawing from assessments or treatments; regrets; and impact of treatments on gender distress, mental health symptoms and disorders, quality of life, and suicidality (COHERE, 2020).
As per the COHERE recommendations, the two specialized gender-identity units for minors now require the following conditions to be met before they start the full diagnostic assessment for possible gender dysphoria and eligibility for medical interventions: − completion of psychosocial intervention to support identity exploration (to be described in the referral); − treatment to remission of any severe mental disorders; − the young person’s entry into at least the early stages of puberty;
With regard to conversion laws, in 2021 a citizens’ initiative was brought to the Finnish Parliament suggesting that “conversion therapies” aiming at changing sexual orientation or gender identity should be made illegal. After hearing experts on jurisprudence, public health, psychiatry, psychology, and spiritual care, the Parliament’s Committee on Health and Social Affairs found that a legal ban on “conversion therapies” was not necessary; the initiative was dismissed (Kansalaisaloite, 2021). Conversion laws were deemed unnecessary because contemporary Finnish health care professionals do not practice conversion therapy, and they consider such historical practices in conflict with their professional responsibilities and neutral therapeutic stance. A new initiative to enact conversion laws is currently underway.
Sweden: Swedish Agency for Health Technology Assessment and Assessment of Social Services report
In 2018, the government commissioned the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) to review the evidence for gender-reassignment interventions for children and adolescents (up to age 18). In a preliminary report (2019), the SBU concluded that the evidence base was weak (SBU, 2019). In 2021, the Department of Paediatric Endocrinology at Karolinska University Hospital in Stockholm discontinued hormone treatment for children with gender dysphoria (Trysell, 2021).
The second SBU report (2022) concluded that the available evidence was insufficient to evaluate the effect of puberty-blocking hormones or cross-sex hormone treatment on psychosocial outcomes, cognitive function, anthropometric measures, or metabolic parameters (Ludvigsson et al., 2023; SBU, 2022).
Based on the second SBU report, the Swedish National Board of Health and Welfare updated the treatment guidelines (published 16 December 2022) (Socialstyrelsen, 2022a, 2022b). The new guidelines conclude that, on the group level, the risks associated with puberty-blocking treatment and cross-sex hormone treatment outweigh the potential benefits. These treatments should therefore not be offered except in exceptional cases or in the context of a clinical research trial. Three main reasons for changing recommendation were stated: first, the incidence of gender dysphoria is continuing to rise, especially among young natal females; second, the frequency of detransitioning is unknown; third, “The experience-based knowledge of participating experts is less uniform than it was in 2015” (p. 4) (Socialstyrelsen, 2022b). 6
Currently, the assessment and treatment process is as follows: − Assessment is multidisciplinary: psychological counselling and identity exploration are always part of the process. − Only carefully selected children—meeting diagnostic criteria for early-onset gender dysphoria, a stable psychosocial situation, and without complicating psychiatric factors (neuropsychiatric or intellectual disability; untreated psychiatric problems, including suicidal risk and trauma; or substance use) are treated with puberty blockers (at Tanner stage 3). − A further comprehensive assessment later in time—which is as thorough and extensive as the first—may result in a decision to treat with cross-sex hormones, from age 16. − Mastectomies are no longer performed before age 18. − Other gender-affirming surgery requires permission from the Swedish National Board of Health and Welfare and is seldom granted before age 23.
At present, conversion laws have not been passed in Sweden.
United Kingdom: Cass Review
The aims of the Cass Review were to examine the evidence pertaining to medical interventions for gender dysphoria in minors using the tools of evidence-based medicine (systematic reviews), quantitative research (data to uncover patterns and to quantify problems), and qualitative research (“the lived experiences of children and young people, their families, and the professionals working to support them”) (Cass, 2022).
Two systematic reviews of puberty blockers and cross-sex hormones, completed in 2020 by the National Institute for Health and Care Excellence (NICE), concluded that the evidence base for both treatments was weak (NICE, 2020a, 2020b).
The interim key findings from the Cass Review, outlined in the February 2022 report (Cass, 2022), are listed in Supplemental Text Box 2. Cass described a poorly functioning service in which clinicians, despite the complex needs of their patients, were “under pressure to adopt an unquestioning affirmative approach” rather than following the “standard process of clinical assessment and diagnosis that they have been trained to undertake in all other clinical encounters” (p. 17). In July 2022, NHS England announced that the Gender Identity Development Service would close in spring 2023 (subsequently pushed back to early 2024).
The interim service specification released in June 2023 highlighted that “the primary intervention for children and young people who are assessed as suitable for The Service is psychosocial (including psychoeducation) and psychological support and intervention. The main objective is to alleviate distress associated with gender incongruence and promote the individual’s global functioning and wellbeing” (p. 2) (NHS, 2023a). The report also stated that puberty blockers would not be routinely offered for young people (<18 years of age) and that puberty blockers would be considered only in exceptional circumstances within a research setting. “Children, young people and their families [were] strongly discouraged from sourcing puberty suppressing or gender affirming hormones from unregulated sources or from on-line providers that are not regulated by UK regulatory bodies” (p. 16).
In the United Kingdom, the bill pertaining to conversion laws—scheduled for consideration late in 2023—has been repeatedly delayed amid concerns that it may criminalize professionals seeking to help people with gender dysphoria. The British Psychological Society, while supporting a ban, has warned: It is important for the legislation or accompanying guidance to make clear that the law will not stop ethical, affirmative forms of therapy (which are non-directive and non-judgmental). It is also important that the legislation does not interfere with psychological and medical professionals who are trained and competent in working with trans and gender questioning youth from engaging in identity exploration or performing clinical assessment of suitability for medical intervention. It should not interfere with regulated professionals working in gender identity clinics under NHS specifications (including any changes to practice made in light of the Cass Review) (BPS, 2022).
In March 2024 NHS England announced that GnRHa would no longer be available for routine use in the treatment of children and adolescents with gender dysphoria due to the lack of evidence (NHS, 2024). The UK government extended this restriction to private prescriptions in May 2024 (Statutory Instrument 2024 No. 727 UK). In April 2024, the final version of the Cass Review, with its formal advice to the NHS, was published (Cass, 2024a). The report confirmed that the patient cohort seen by GIDS since the sharp uptick of referrals from 2012 to 2015 was a “different cohort from that looked at by earlier studies. Among referrals there is a greater complexity of presentation with high levels of neurodiversity and/or co-occurring mental health issues and a higher prevalence than in the general population of adverse childhood experiences and looked after children” (p. 26). The report also emphasized the importance of ongoing research and the evidence-based framework. It noted that, “although some think the clinical approach should be based on a social justice model, the NHS works in an evidence-based way” (p. 20).
The evidence pertaining to the use of puberty blockers and cross-sex hormones in children and adolescents was shown to be weak. The report found “no changes in gender dysphoria or body satisfaction were demonstrated. There was insufficient/inconsistent evidence about the effects of puberty suppression on psychological or psychosocial wellbeing, cognitive development, cardio-metabolic risk or fertility” (p. 32). In this context, the NHS was advised “that because puberty blockers only have clearly defined benefits in quite narrow circumstances, and because of the potential risks to neurocognitive development, psychosexual development, and longer-term bone health, they should only be offered under a research protocol.”
The evidence pertaining to cross-sex hormones was also found to be weak: “no conclusions can be drawn about the effect on gender dysphoria, body satisfaction, psychosocial health, cognitive development, or fertility” (p. 7) (Taylor et al., 2024) (quoted at p. 33 of the Cass Review). Going forward, the report stated that the option to provide masculinising/feminising hormones from the age of 16 is available, but the Review would recommend an extremely cautious clinical approach and a strong clinical rationale for providing hormones before the age of 18. This would keep options open during this important developmental window, allowing time for management of any co-occurring conditions, building of resilience, and fertility preservation, if required (p. 33) (Cass, 2024a).
The report also emphasized the lack of evidence-based guidelines around the world: “most guidelines have not followed the international standards for guideline development, and because of this the research team could only recommend two guidelines for practice—the Finnish guideline published in 2020 and the Swedish guideline published in 2022” (p. 27). The report repeatedly emphasized the importance of “normal clinical approaches to holistic assessment” and treatment, as used with other young people with complex presentations. It emphasizes the importance of psychological and psychosocial interventions to treat and address comorbid mental health issues, to build resilience, to address family difficulties, to provide “more information about gender expressions and the range of possible interventions” (p. 150), and generally to “explore their concerns and experiences and help alleviate their distress, regardless of whether they pursue a medical pathway or not” (p. 150).
Norway: Norwegian Healthcare Investigation Board report
The situation in Norway is currently unfolding. In March 2023, the Norwegian Healthcare Investigation Board (UKOM) issued a formal report (UKOM, 2023) that strongly criticized the previous, 2020 Norwegian guidelines (Helsedirektoratet, 2020) and that articulated concerns pertaining to safety for young people: The report deals with children and young people in general. There has been a large increase in inquiries to the health service from people with gender incongruity in recent years. In particular, the number of children and young people in their teens who apply to, or are referred for assessment and treatment in, the specialist health service has increased significantly. The biggest increase is among teenagers and young adults who are registered as girls at birth but identify as boys. Our attention has therefore been particularly directed at teenagers and young people with gender incongruence and gender dysphoria who seek health care. Children and young people are not fully developed physically, mentally, sexually, or socially. This requires special vigilance with regard to patient safety (pp. 2–3/8, translation by Google Translate).
The UKOM report defined current treatments as experimental treatments or treatments under trial and recommended that the Ministry of Health and Care consider the establishment of a national medical quality register—of persons receiving medical treatment for gender incongruity—to enable the systematic collection of data and promote follow-up research. UKOM’s key recommendation is that future guidelines need to follow an evidence-based approach akin to best practice in the rest of medicine.
On 12 December 2023, a new law banning conversion therapy was passed by the Norwegian parliament (see Table 1).
Countries without national guidelines
In this section, we briefly discuss four countries without national guidelines: Australia, Canada, Republic of Ireland, and the United States. Several of these countries have conversion laws.
Australia
In Australia, the first referrals of children for gender services reportedly occurred in 2003 in Melbourne and 2013 in Sydney, with the first pediatric gender service being established at the Melbourne’s Royal Children’s Hospital (RCH) in 2012 (AusPATH, 2022a). Over the last decade, the number of young people presenting to gender services has substantially increased in all states (Telfer et al., 2018), which all now maintain dedicated gender services. These public services operate with a variety of different models of multidisciplinary care, under the authority of respective state departments of health and Local Health Districts (see further below) (Davey, 2024). Outside the public health system, some young people receive assessment and care through private health practitioners, although data on this group are lacking.
Pharmacological interventions for children and young people with gender dysphoria are generally accessible through gender services funded by state governments. GnRHa for puberty suppression are commonly prescribed in gender clinics, with no age limits, subject to parental agreement and consent and the young person’s assent. Cross-sex hormones are generally not prescribed in gender clinics until the age of 16, by which time young people are considered competent to make that decision (in accordance with the legal concept of Gillick competence) (NSW Health, 2020). No GnRH agonists or preparations of oestrogen or testosterone are registered in Australia for the indication of gender dysphoria; they are used off-label. This means that they have not been assessed for quality, safety, and efficacy for this indication by the federal Therapeutic Goods Administration (TGA, 2023).
The Family Court of Australia, through various judgments, has expressed the view that management decisions for transgender young people should be left to expert clinicians; the Court would usually become involved only if there is parental disagreement. Surgical intervention is generally not considered or allowed until age 18, but some individuals have accessed surgical intervention under 18 after application to the Family Court.
There are no national, government-endorsed guidelines. Gender services around Australia generally follow a rights-based, gender-affirming approach, although not all services have made their guidelines or clinical pathways publicly accessible (ACT Health Directorate, 2023; Hall et al., 2024; RCH Gender Service). Research in Australia is limited (Callander et al., 2019; Elkadi et al., 2023; Hewitt et al., 2012; Hilton et al., 2022; Kozlowska et al., 2020, 2021; Tollit et al., 2023), though existing studies have found significant mental health comorbidities (including autism) (Kozlowska et al., 2020, 2021; Tollit et al., 2023), complex family and psychosocial issues (Kozlowska et al., 2020, 2021), a pattern of adolescent presentations (Callander et al., 2019; Tollit et al., 2023), and an ongoing need for psychiatric treatment over time (Elkadi et al., 2023). There are no studies reporting long-term outcomes.
In 2018, the Medical Journal of Australia published a “position statement” entitled “Australian Standards of Care and Treatment Guidelines for Trans and Gender Diverse Children and Adolescents,” which was predominantly authored by the gender-services team, led by Michelle Telfer, at the Royal Children’s Hospital in Melbourne (RCH) (Telfer et al., 2018). The authors describe the standards, updated in 2020 (Telfer et al., 2020), as being based on clinician consensus, previously published guidelines, and standards of care and research studies in the field, with widespread consultation. Despite the title, the Telfer guidelines do not represent national guidelines or standards.
In New South Wales (NSW), in 2023, the Ministry of Health published a “Framework for the Specialist Trans and Gender Diverse Health Service for People Under 25 Years” (NSW Ministry of Health, 2023). The framework is intended to “guide treatment and care decisions by NSW Health clinicians, private clinicians, General Practitioners (GPs), non-government organizations (NGOs), trans and gender diverse people under 25 years and their families and carers” (p. 3). The NSW framework highlights a rights-based, gender-affirming model of care consistent with the updated Telfer and colleagues guidelines (Telfer et al., 2020), AusPATH guidelines for prescribing cross-sex hormones (AusPATH, 2022b), “Position Statement on the Hormonal Management of Adult Transgender and Gender Diverse Individuals” (Cheung et al., 2019), Endocrine Society Guidelines (Hembree et al., 2017), and WPATH 8 guidelines (Coleman et al., 2022). The framework notes (p. 2) (NSW Ministry of Health, 2023) that it was also informed by a 2020 “evidence check” by the “Sax Institute” (Sax Institute, 2020), an independent research and policy organization. Notably, the institute had actually concluded that the evidence base for puberty blockers and cross-sex hormones was not only small but, overall, of low quality. This conclusion is not mentioned, however, in the NSW framework, nor are the conclusions of recent systematic reviews (Brignardello-Petersen and Wierchioch, 2022; Ludvigsson et al., 2023; NICE, 2020a, 2020b; Pasternack et al., 2019; SBU, 2022).
In South Australia (SA), the state government has published a rights-based, gender-affirming model of care, the “Statewide Gender Diversity Model of Care” (updated July 2023) (Government of South Australia, 2023) to shape the work of clinicians (including those working with minors) in the state. The SA model of care draws from WPATH 8 guidelines (Coleman et al., 2022), AusPATH guidelines for prescribing cross-sex hormones (AusPATH, 2022b), the updated guidelines by Telfer and colleagues (Telfer et al., 2020), the “Position Statement on the Hormonal Management of Adult Transgender and Gender Diverse Individuals” (Cheung et al., 2019), and Endocrine Society Guidelines (Hembree et al., 2017). The SA model of care mentions the interim Cass report (Cass, 2022), the evolving nature of the evidence base, and the changing nature of overseas models of care, but it does not include any evidence-based information from systematic reviews published from around the world (Government of South Australia, 2023).
In responding to the final, 2024 Cass Review, a spokesman for the Federal Health Minister said that “clinical treatment of transgender children and adolescents is a complex and evolving area in which longer-term evidence to inform treatment protocols is still developing” (Davey, 2024). Though the spokesperson asserted that the “clinical care pathways are different in the UK from Australia,” a 2024 worldwide survey of gender services, including five from Australia, suggests that clinical services provided by Australian gender clinics do not differ significantly from the those provided by the now-discontinued Gender Identity Development Service (GIDS) at the Tavistock (Hall et al., 2024) (Clayton et al., 2024).
Laws prohibiting conversion therapy have been enacted in four of six Australian states (Australian Capital Territory, New South Wales, Queensland, and Victoria), with votes pending in South Australia and Western Australia (see Table 1).
Canada
Canada has no formal national guidelines. Its first gender-identity clinic was established for children and adolescents in 1975 at the Clarke Institute of Psychiatry (now the Centre for Addiction and Mental Health) in Toronto (Bradley et al., 1978; Zucker, 2015). In 2000, this clinic adopted the Dutch Protocol, the first clinic in North America to do so (Zucker et al., 2011). From its inception, the clinic integrated research with clinical care and conducted various studies pertaining to diagnosis and assessment, comorbidity, causal mechanisms, and long-term follow-up. Because in its early days many more children than adolescents were referred, the research focused more on children, but this began to change in the early 2000s when there was a notable increase in the number of referred adolescents (Wood et al., 2013; Zucker et al., 2008). Two members of the clinic played substantial roles in subsequent revisions to the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III) regarding the diagnosis of gender dysphoria: DSM-III-R (1987), DSM-IV (1994), DSM-TR (2000), and DSM-5 (2013) (Bradley et al., 1991; Zucker, 2010, 2013). In late 2014, local activists complained about the clinic’s therapeutic approach, particularly for children, and the clinic was closed in 2015 following an external review (Dreger, 2015).
At present, at least ten hospital-affiliated clinics provide gender-identity services to children and adolescents (Singer, 2022). Services are also provided through many community mental health settings, including, for example, Mental Health Services for Gender-Diverse and Sexual Minority Youth (Canadian Mental Health Association, 2023). These clinics currently follow a rights-based, gender-affirming approach. One program was open to starting adolescents on hormonal suppression prior to a formal assessment (Gender Pathways Service, nd), though the clinic’s current referral form is unclear as to whether this policy is still in place (CHEO, 2023). Another clinic informs prospective patients in an introductory letter that “Our clinic takes an affirming approach to gender identity and care. Through ongoing assessment and discussion, we support the young person and family in deciding about options for medical care, with the hopes of decreasing feelings of gender dysphoria and discomfort with their bodies” (SickKids, 2022). This clinic emphasizes that its primary goal is to “provide information on medical options and a treatment plan for puberty blockers and medical transition” (SickKids, 2022, 2023); the clinic does not provide, however, “ongoing mental health care” (SickKids, 2022). For this, families are advised to seek out support in the community.
Because no national therapeutic guidelines are in place to mandate best-practice care, it is unknown how many clinicians who see children and adolescents outside of specialized clinics adopt various therapeutic models apart from gender-affirmation, such as “watchful waiting” or “gender exploratory” therapy.
In Canada, both provincial (in some provinces) and federal legislation state that efforts to “change” the gender identity of a minor are illegal. For example, in the province of Ontario, Bill 77 (Bill 77, 2015), which was adopted in 2015, states: “No person shall, in the course of providing health care services, provide any treatment that seeks to change the . . . gender identity of a patient under 18 years.” However, it also states that “the facilitation of . . . identity exploration or development” is permitted. Unfortunately, no operational definition is provided regarding what constitutes “identity exploration” and how that would be considered different from attempts to “change” the gender identity of a minor.
The Cass Review (Cass, 2024a) has received notable attention in Canada (Kirkey, 2024a, 2024b, 2024c; Zivo, 2024a, 2024b). It appears, for example, to have influenced the Premier of Alberta to create new guidelines for the care of transgender children and adolescents, including a “blanket ban” on hormonal treatment for youth aged 15 and younger (Zivo, 2024a). Notably, however, the Canadian Paediatric Society and the Alberta Medical Association have said that these policies “will lead to significant negative health outcomes, including increased risk of suicide and self-harm” (Kirkey, 2024a).
Republic of Ireland
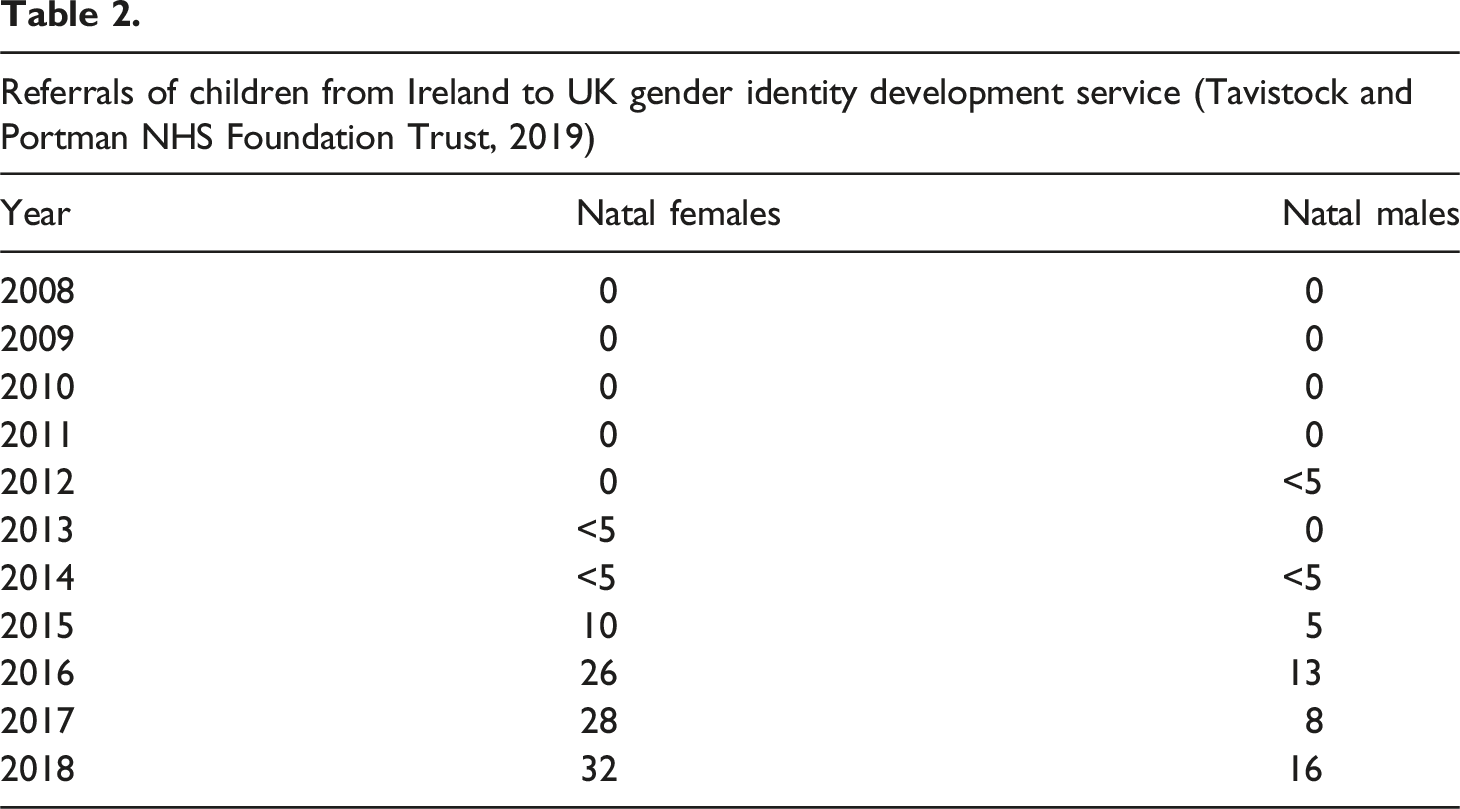
The situation in Ireland is of particular interest because clinicians from the adult National Gender Service have voiced concerns on two fronts. First, WPATH guidelines have been rejected because of their non-biopsychosocial nature: they allow medical treatment to be initiated without a thorough psychiatric assessment (Tighe, 2022). Second, in a 2019 audit, 18 patients—young people transferring into adult services from the paediatric service—were found to have received substandard levels of medical care (Barnes, 2023). Problems included the following: − lack of assessment reports (7/18 cases); − “serious mental health problems (including self-harm, depression, suicidality and eating disorders” (10/18) (p. 237) (Barnes, 2023); − high rate of autism; − young people “taking . . . hormones religiously” while failing to receive holistic treatment to address comorbid psychiatric problems (including being “bed-bound” as a consequence of mental health concerns) (p. 235) (Barnes, 2023); − the presence of “incredibly difficult life circumstances alongside their gender identity issues” (p. 237) (Barnes, 2023).
A psychiatrist from National Gender Service had described the GIDS-Crumlin service as “unsafe” and called for the assessment service provided by GIDS to be “terminated with immediate effect” (p. 237) (Barnes, 2023). These concerns were subsequently borne out by the Cass Review (see UK section) (Cass, 2022).
At present (May 2024), Irish children and young people with gender dysphoria are being referred to the UK’s Children and Young People Gender National Referral Support Service, which will triage these referrals to one of the newly developed services that was opened in the United Kingdom in April 2024 (Bowers, 2024).
On 16 April 2024, following a parliamentary request for a statement regarding the release of the Cass Review, the Minister for Health, Stephen Donnelly, responded that the Irish Health Service Executive “is initiating a new clinical programme for gender healthcare” and that “an updated clinical Model and implementation plan for gender healthcare services will be developed” over the next 2 years. He noted that the program will be based on the best clinical evidence, including the Cass Review and other “emerging and evolving international evidence.” With the aim of providing “a wide range of services for all people with gender incongruence or dysphoria, from care locally in the community to more specialised and complex care,” Donnelly asserted his commitment to “building a service based on experience and clinical evidence, respect, inclusiveness and compassion” available to all “children and adults in the transgender community” (Oireachtas, 2024).
Although conversion laws have not yet been enacted in Ireland, they are actively under consideration.
United States
The exponential growth of gender-reassignment interventions has also occurred in the United States. In 2007, Boston Children’s Hospital opened the country’s first gender clinic for minors (Boston Children’s Hospital, 2023). Currently, at least 79 children’s hospitals provide gender-reassignment interventions. Many more independent mental health clinicians, endocrinologists, adolescent physicians, paediatricians, surgeons, and clinics provide gender transition for youth. The number of youth undergoing gender transition and their outcomes are not being tracked systematically. Insurance data suggest that more than 18,000 youth are currently receiving gender-reassignment interventions in the United States (Block, 2023a; Respaut and Terhune, 2022). Akin to Europe, American gender clinics report an increase in presentations, with a predominance of natal adolescent females having high rates of psychiatric comorbidities (Chen et al., 2016).
The United States is built upon principles of federalism that give each individual state broad authority to independently regulate the medical profession. This leads to a wide divergence among states as to how the medical profession is regulated. The federal government in Washington, DC, can also regulate certain aspects of the medical profession via pharmaceutical regulations, federal insurance programs, and civil rights laws. Federal court rulings add further complexity.
The federal Food and Drug Administration has not approved any drugs for the specific purpose of treating gender dysphoria. The use of puberty blockers and cross-sex hormones is therefore off-label (Florida Board of Medicine, 2022).
The complex relationship between the federal and state governments is plainly seen in the state of Florida: – The Department of Health and Human Services (HHS), a branch of the federal government, has attempted to impose a national mandate that would require doctors and health care entities to provide gender-affirming care. The HHS rule intends to prohibit “gender identity discrimination.” Ostensibly, a physician would violate a child’s civil rights if the physician did not transition a child upon request. Currently, there is no other condition for which HHS requires physicians to prescribe off-label medications. – The state of Florida’s Department of Health commissioned a systematic review that found the evidence for gender-affirming care to be of low quality (Brignardello-Petersen and Wierchioch, 2022). Following that review, Florida’s health department classified gender-affirming care as experimental (Florida Department of Health, 2022). – Medicaid, a jointly managed federal and state health insurance program primarily for the economically disadvantaged, is prohibited by federal and state statutes from paying for experimental care. Consequently, the Florida health department mandated that Medicaid cannot pay for gender-reassignment interventions. This decision is being challenged in court. – The Florida Boards of Medicine are tasked with ensuring the public’s safety by licensing and disciplining physicians and regulating the practice of medicine. There are two boards, one for medical doctors and one for osteopathic doctors. Both boards have barred the use of hormones and surgery under age 18, citing all of the following: the low quality of evidence; emerging reports of regret, harm, and detransitioning; and concerns regarding a minor’s capacity to grant consent. The boards made this decision after weighing systematic evidence reviews from England, Finland, Sweden, and the Florida Department of Health. The boards heard testimony from experts, patients, and the public—both in support of, and opposed to, youth transition. – Rules created by the Florida Boards of Medicine are binding on physicians within the state of Florida. The rule barring transition was challenged in the federal district court, which held that “the benefits of treatment with GnRH agonists, and eventually with cross-sex hormones, will outweigh the risks” (p. 16) (Doe v. Ladapo, 2023). This holding is exactly the opposite of Sweden’s National Board of Health and Welfare, which concluded that “the risks of puberty blockers and gender-affirming treatment are likely to outweigh the expected benefits of these treatments” (p. 3) (Socialstyrelsen, 2022b).
As of January 1, 2024, 23 states have enacted laws that impose restrictions on gender-reassignment interventions for minors, and additional states are considering similar legislation (Equality Federation, nd; FAIR, 2023; Sapir and Wright, 2023).
Some states are moving in the opposite direction. Twenty-one states have passed so-called conversion therapy laws (Equality Maps, 2023). These laws have had a chilling effect on the work of psychotherapists, who aim to create a neutral space for their patients—where children or adolescents can explore their gender-identity and the other psychosocial issues that commonly coexist. These laws have led licensing boards to investigate therapists who have taken an exploratory, holistic approach with their clients (Winn, 2023).
At least 14 states have passed “sanctuary laws” enabling nonresident minors to obtain gender-reassignment interventions not available in their home states (FAIR, 2023). Some states allow nonresident minors who have fled to a “sanctuary state” to undergo gender transition without parental notification and consent (Macuk, 2023; WashingtonLawHelp, 2023).
The courts have increasingly come into play. Challenges to legislation restricting access to gender-reassignment interventions are increasingly common. Lower federal courts have generally prevented these restrictive laws from being enforced, holding that they violate sex-based civil rights and a parents’ right to direct their child’s medical care. On appeal, one higher-level court—the Second Circuit Court of Appeal in Brandt v. Rutledge—held that the Arkansas ban on minor transition could not go into effect (Brandt v. Rutledge, 2022).
Two other circuit courts have held that laws restricting youth transition are permitted, thereby allowing Alabama, Kentucky, and Tennessee to enforce their laws (Eknes-Tucker v. Governor of the State of Alabama, 2023). The courts held that gender transition by a minor is not a civil right enshrined in the U.S. Constitution and that the courts are not the proper place to debate this issue. Since the medical profession is increasingly divided on the safety and effectiveness of minor gender transition, the proper place to decide this question is within the medical profession and the democratic process afforded to the people (Poe v. Drummond, 2023). The Tennessee ruling has been appealed to the US Supreme Court.
On the level of state courts, malpractice cases are being filed by both minor and adult patients claiming that they were harmed physically or psychologically by gender-reassignment interventions 7 (Aldaco v. Perry, 2023; Ayala v. Am. Acad. of Pediatrics, 2023; Brockman v. Kaiser, 2023; Doe v. Lick, 2023; Hein v. UNMC Physicians, 2023; Keifel v. Ruff, 2022; Lovdahl v. Kaiser, 2023; Mosley v. Emerson, 2023; Stewart v. Turco, 2023; Towe v. United States ex rel. Cherokee Health System, 2023; Ulery v. Rafferty, 2023).
The American Academy of Pediatrics and the Endocrine Society have been asked to comment on the Cass Review (Ghorayshi, 2024). The American Academy of Pediatrics released a statement that their clinical guideline is “grounded in evidence and science” (American Academy of Pediatrics, 2024). The Endocrine Society asserted that their guideline “adheres to the highest standards of trustworthiness and transparency” and that the Cass Review “does not contain any new research” (Endocrine Society [US], 2024). Both groups suggest that clinical restrictions implemented in the United States are politically motivated. Neither group addressed the NHS decision to restrict access to puberty blockers, the Cass Review’s conclusion that youth transition is “built on shaky foundations” (Cass, 2024b), or calls for unity to ensure that gender diverse youth receive safe and effective care (Abbasi, 2024).
More broadly, in the United States, discussions concerning the availability of minor gender-reassignment interventions are now dominated by politics. The original questions about the benefits, risks, evidence, and ethics of such care, including the maturity of minors and their capacity to consent, have been relegated to a secondary role or disregarded altogether.
Conclusion
In this perspective our author team—working and living in different Western democracies around the world—has examined from an international viewpoint the development over time of national guidelines for treating children (including adolescents) with gender dysphoria. This historical unfolding across and within different countries has occurred against a background involving diverse social and political forces, along with ongoing scientific developments. Also at work are decades of medical developments, the involvement of powerful pharmaceutical companies, 8 and the rise of gender dysphoria as what Nichter refers to as an idiom of distress (Nichter, 1981, 2010)—“socially and culturally resonant means of experiencing and expressing distress in local worlds” (p. 405) (Nichter, 2010).
The commitment of Western democracies to individual rights (including the rights of the child) (United Nations, 1989), the stigma of mental illness, a shift towards demand-driven health care (Rijckmans et al., 2007), the push for depathologization, the evolving role of the Internet (Haltigan et al., 2023), and the insertion of gender politics/ideology into educational/curricular, social, and political discourse (Dentons Europe LLP, 2019) have worked together to put aside safeguards and to facilitate access to medical interventions for treating gender dysphoria in minors. More recently, in Finland, Sweden, and the United Kingdom, evidence-based guidelines based on the countries’ own systematic reviews have brought into focus questions pertaining to treatment efficacy and patient safety. Notwithstanding this complexity, we can see a clear pattern emerging. Guidelines for treating gender dysphoria in children can increasingly be grouped toward one end of the spectrum or the other.
Grouped along one end are guidelines informed by, and strongly shaped by, a rights-based approach—emphasizing self-determination, elimination of discrimination, identity and body autonomy, fulfillment of expressed needs, and depathologization (see Figure 4). A key idea is that children should be free to make independent decisions that determine their health choices and their own lives (Amnesty International UK, 2020; Coleman et al., 2022). In other words, clinical care is driven by “respect [for] the self-determination of each person as being the expert on their experience” (p. 22) (PATHA, 2018). Our perspective makes apparent that clinical practice in services whose guidelines are shaped by the rights-based approach has shifted away from holistic biopsychosocial practice. In many such services, the role of mental health professionals has moved away from the task of conducting comprehensive diagnostic biopsychosocial assessments to providing optional advice and support. At present, services working from this viewpoint use the terms gender-affirming approach (Hidalgo et al., 2013; Moral-Martos et al., 2022; NHS, 2023a; Oliphant et al., 2018b; Socialstyrelsen, 2017; Telfer et al., 2018) or informed consent model (Carroll et al., 2023; Coleman et al., 2012; PATHA, 2018) to describe their practice (see Text Box 3). The gender-affirming approach and the informed consent model. The gender-affirming approach emphasizes affirmation of the child’s expressed gender. This approach supports gender-reassignment interventions based on what the child/adolescent wants or does not want. The term was coined in the United States in 2003 (Crawford, 2003) to describe the approach that Catherine Tuerk (a registered nurse, psychotherapist, and parent of a gender-variant child) and Edgardo Menvielle (a child psychiatrist) developed for a parent-support group designed to help them accept and affirm their gender-variant children (Menvielle and Tuerk, 2002). The terminology was later adopted by others (Hidalgo et al., 2013). In recent years, it has been used to refer to an “unrestricted” affirmative approach: one where many (or all) safeguards have been removed and where puberty blockers and cross-sex hormones—coupled with early social transition—are seen as first-line treatment for gender dysphoria in children/adolescents (Boston Children’s Hospital, 2023; Carroll et al., 2023; Moral-Martos et al., 2022; NHS, 2023; Oliphant et al., 2018b; Socialstyrelsen, 2017; Telfer et al., 2018). The informed consent model emphasizes the need to obtain informed consent as the threshold for initiating gender-affirming care (Coleman et al., 2012; PATHA, 2018). The child/adolescent (and family) is informed about the risks and benefits of puberty blockers and cross-sex hormones, and if they agree, gender-affirming hormone treatment is provided. A mental health assessment—to meet eligibility criteria and to ensure treatment of mental health concerns—is considered unnecessary unless requested by the child or family (Coleman et al., 2012; PATHA, 2018).
An important point—and a clear finding of this perspective—is that these models shaped by the rights-based approach reflect a wide range of clinical practice across and between different countries. Clinics in university-affiliated hospitals have, in general, tried to work from a multidisciplinary perspective—with multidisciplinary teams involving psychiatrists, psychologists, endocrinologists, surgeons, fertility specialists, and sometimes lawyers—thereby trying to retain a biopsychosocial practice to some degree. By contrast, services provided outside such hospitals—most commonly in the private sector—typically apply the rights-based approach without restrictions (see, e.g., the sections on Spain, Norway, Belgium, France, and Canada, plus some U.S. states). In these services, minors can access medical interventions for gender dysphoria without a comprehensive biopsychosocial assessment, diagnosis of gender dysphoria, psychiatric screening, or ongoing psychological support. Notably, the countries that have applied the rights approach unconstrained by other considerations or restrictions have tended to downplay or dismiss questions concerning potential harms—questions that are now being raised by the increasing number of detransitioners.
Arguably relevant in this context—the application of the rights approach unconstrained by other considerations or restrictions—is the 1989 United Nations Convention on the Rights of the Child (United Nations, 1989). The Convention includes 42 articles, several of which define rights that are potentially opposable to, and that could potentially restrict, any right to gender-affirming medical treatment. Article 24 (children have the right to good-quality medical care) raises concerns about government legislation that funnels children into experimental treatment that lacks a research foundation and long-term follow-up. Article 33 (governments should provide ways of protecting children from dangerous drugs) raises concerns about the widespread use of puberty blockers and cross-sex hormones that are not approved for gender dysphoria by the majority of national drug-regulation agencies and that have likely irreversible consequences for the child’s intellectual (brain) and physical development. Article 36 (children should be protected from any activities that could harm their development) raises the same concerns as Article 33. All these considerations have become even more relevant after information made public through a current U.S. court case has shown that WPATH, in following its rights-based approach, actively suppressed publication of evidence-based information pertaining to medical interventions for gender dysphoria (Exhibit 167) (Boe v. Marshall, 2024; Economist, 2024). After receiving the results of the systematic reviews that WPATH commissioned Johns Hopkins University researchers to conduct, WPATH leadership became “painfully aware that there are many gaps in research to back up our recommendations” (Exhibit 190, page 9) (Boe v. Marshall, 2024) for children and adolescents in WPATH 8 guidelines (Coleman et al., 2022). The Johns Hopkins researchers reached out to U.S. federal authorities, noting that “we have been having issues with the sponsor (WPATH) trying to restrict our ability to publish” and that “we found little to no evidence about children and adolescents” (Exhibit 173, page 23).
Grouped along the other end of the spectrum are guidelines informed and shaped by the evidence-based approach (see Figure 4), which emphasizes a treatment’s effectiveness and the patient’s safety, all under the assumptions that “science is cumulative” and that “scientists need to cumulate [knowledge] scientifically using systematic reviews” (p. 53) (Chalmers, 2007; Lapa et al., 2019). These guidelines highlight the following: the recent change in patient demographics (the increase in adolescent-onset gender dysphoria, predominantly in natal girls, raising questions about the reason for the rise of gender dysphoria); the high rates of mental health comorbidity and psychosocial instability; the capacity of minors (especially those with comorbid mental illness) to provide consent; the lack of evidence that treatment with puberty blockers and cross-sex hormones resolves distress and mental health concerns; and the rising numbers of detransitioners who report that they regret and were harmed by medical interventions for gender dysphoria (Boyd et al., 2022; Cohn, 2023; Expósito-Campos et al., 2023; Gribble et al., 2023; Hakeem, 2023; Jorgensen, 2023b; Littman, 2021; Littman et al., 2024; MacKinnon et al., 2023; Moore and Brunskell-Evans, 2019; Pazos Guerra et al., 2020; Pullen Sansfaçon et al., 2023; Usher, 2023; Valdes and McKinnon, 2023; Vandenbussche, 2022). These evidence-based guidelines also emphasize the following: the importance of the holistic biopsychosocial assessment and treatment, including the provision of a diagnosis of gender dysphoria and the assessment and treatment of comorbid mental health concerns; the importance of exploratory psychotherapy from a neutral therapeutic stance as the first step in treatment; and legislation or national guidelines that delay access to gender-reassignment surgeries until legal adulthood (see the evidence-based guidelines developed by Finland, Sweden, and the United Kingdom).
A final theme emerging from this perspective—which may not be obvious to the reader—is that exploratory psychotherapy from a neutral therapeutic stance is often unavailable in many countries or regions. A core aspect of exploratory psychotherapy is neutrality (see Text Box 2). Clinicians remain open, explore the young person’s experience, and assist the young person (and family) in making informed choices that are based on a full understanding of all of the possible factors contributing to the young person’s distress and all possible outcomes (NHS, National Health Service [UK], 2023, UKCP, UK Council for Psychotherapy, 2023). The overarching aim is to increase autonomy, decrease distress, and improve overall function. The neutral stance of exploratory psychotherapy contrasts with the gender-affirmative approach, where verbal affirmation of the child’s expressed gender is the first active intervention. Of special note in this context is the increasingly widespread adoption of so-called conversion therapy laws. These laws are specifically modelled after earlier laws prohibiting efforts to convert people from a homosexual to a heterosexual orientation. At least in theory, the fundamental purposes of these laws are laudable: to ensure that each individual’s sexual orientation or gender identity is respected, and to bar interventions predicated on the view that a person’s sexual orientation (e.g., homosexual) or gender identity is broken and needs to be fixed (Equality Maps, 2023; Victorian Equal Opportunity and Human Rights Commission, 2021). As a practical matter, however, because of the way in which these laws are likely to be worded or enforced, they work against the interests of gender dysphoric children and their families, who may be unable to access the exploratory psychotherapy from a neutral therapeutic stance that is a vital component of evidence-based interventions for such children. They may also not be able to access psychotherapy for their comorbid mental health concerns—suicidal ideation, anxiety, depression and so on—because evidence-based interventions for mental health concerns are misconstrued as forms of “conversion therapy” (see below).
A common feature of conversion laws is to define what is included and excluded in the range of prohibited practices, although the wording of these laws may nevertheless leave unclear which therapeutic practices are permitted and which are not. Some of these laws, such as the Australian state of Victoria’s recently adopted Change or Suppression (Conversion) Practices Prohibition Act 2021, leave only narrow windows for psychotherapy regarding gender dysphoria. For example, a permitted practice is one that “is supportive of or affirms a person’s gender identity or sexual orientation” (section 5(2)(a)), and the state’s Fact Sheet distributed in advance of the bill’s enactment specifically notes that “psychological counselling for children with gender dysphoria” would be permitted under the new law (Victorian Equal Opportunity and Human Rights Commission, 2020). Nevertheless, the law also explicitly prohibits “providing a psychiatry or psychotherapy consultation, treatment or therapy, or any other similar consultation, treatment or therapy” (section 5(3)(a)). Along the same lines, while the Canadian law in Ontario states that “the facilitation of . . . identity exploration or development” is acceptable, no operational definition is provided regarding what constitutes “identity exploration” and how that would be considered different from a legally prohibited, and criminally punishable, attempt to “change” the gender identity of a minor (Bill 77, 2015). In Canada, Egale, “Canada’s leading organization for 2SLGBTQI people
9
and issues,” (Egale, 2023) has developed information sheets (available on its website) that describe a broad range of practices as forms of “conversion therapy” (see Text Box 4). From the perspective of this organization,
10
almost any evidence-based therapeutic practice can be perceived as a form of conversion therapy. In this context, therapists who work from a neutral therapeutic stance—and even those who specialize in evidenced-based interventions for anxiety and depression (such as cognitive-behavioural therapy [CBT]) (Oud et al., 2019; Pegg et al., 2022) or dialectical behaviour therapy (DBT) (Dimeff and Linehan, 2001) make such therapeutic options available to minors with gender dysphoria at their own risk. Along the same lines, in Australia, the absence of a clear, reliable distinction between conversion therapy and exploratory psychotherapy from a neutral stance is apparent in a statement from the Australian Professional Association for Transgender Health (AusPATH): “The AusPATH Board do not support ‘exploratory therapy’ which is often used as a euphemism for conversion therapy” (AusPATH, 2022c). New Zealand legislation likewise allows identity exploration but fails to provide a definition (Conversion Practices Prohibition Legislation Act, 2022). An exception is France, where the text of the conversion law specifies that health professionals who invite their patients to exercise caution and reflect before possibly transitioning will not be subject to prosecution (Vie Public, 2022). Conflation of psychotherapy with conversion therapy. Conflation of psychotherapy with conversion therapy is common. For example, Egale, a leading Canadian organization for 2SLGBTQI people and issues, has issued a set of five information sheets defining the following therapeutic practices as reflecting forms of conversion therapy (Egale, 2023): ‐ “For example, the lack of treatment or service from a healthcare provider to provide gender-affirming healthcare such as hormone replacement therapy (HRT), is also a form of conversion practice” (information sheet 1). ‐ “Conversion therapy can consist of many different activities including what may look like traditional counselling such as psychotherapy methods like Cognitive Behavioural Therapy (CBT) and Dialectical Behaviour Therapy (DBT)” (information sheet 2). ‐ “Some other names and practices that conversion therapy may be disguised as” include “gender exploratory therapy” (information sheet 3), an alternative term for exploratory psychotherapy from a neutral therapeutic stance that is conducted with a person with gender dysphoria.
Looking at the situation from an international viewpoint, the upshot is that in nations and regions that have enacted conversion laws, many mental health professionals are barred, either in law or in fact, from providing psychological treatment from a neutral therapeutic stance to children with gender dysphoria. Therapists who provide neutral, conventional, exploratory therapy, which is mandated by professional ethics—and by evidence-based guidelines in Finland, Sweden, and the United Kingdom—are consequently unable to address the needs of gender dysphoric youth. The legal and professional risks are simply too great. The ultimate consequence is that children who might well profit from a neutral therapeutic space may find it difficult to find a therapist who will take them on; instead, they will find themselves channelled to seek care from practitioners who take a “gender-affirming” position and who regard hormonal interventions—coupled with early social transition—as the preferred and first-line treatment for gender dysphoria. As noted in the systematic reviews discussed above, however, these medically oriented, gender-affirming hormonal treatments are experimental and not currently supported by evidence-based medicine.
The different forces at work in the arena of gender dysphoria are well apparent in our descriptions of guideline development in the countries where we, the authors, work and live. The interplay—the push and pull—between the rights-based approach and evidence-based approach has created a complex dynamic that will take years to play out, in different countries, and in ways that are hard to predict. Whatever the quality of the medical, cultural, and political processes that come to bear on the situation and its challenges, there is likely to be a serious human cost.
Supplemental Material
Supplemental material - Evolving national guidelines for the treatment of children and adolescents with gender dysphoria: International perspectives
Supplemental material for Evolving national guidelines for the treatment of children and adolescents with gender dysphoria: International perspectives by Kasia Kozlowska, Geoffrey R Ambler, Sophie Dechêne, Maria Cruz Almaraz Almaraz, Caroline Eliacheff, Kirsty Entwistle, Isabel Esteva de Antonio, Esther Gómez Gil, Paul Hofman, Patrick Hunter, Riittakerttu Kaltiala, Beryl Koener, Mikael Land, Alexandre Ledrait, Ann M Maguire, Céline Masson, Stella O’Malley, Melissa Raven, Hannah Ryan, Anne Wæhre, Catherine Williamson, Kenneth J Zucker, and Stephen Scher in Human Systems.
Footnotes
Acknowledgments
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Patrick Hunter is a member of the Florida Board of Medicine and is an expert witness in legal cases related to gender medicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.