
Abstract
There exists a vast amount of research and literature on pregnant women struggling with substance use problems and the challenges they can face in providing adequate and sensitive parenting. The aim of the present study was to explore the thoughts about motherhood and their unborn child of pregnant women in voluntary or involuntary substance use treatment, and to gain insight into their childhood attachment experiences. A total of 16 women in involuntary or voluntary treatment were interviewed about their thoughts about motherhood, their unborn child, and the treatment they were receiving. A phenomenological/hermeneutic analytical approach was used. Four categories emerged from the analysis: Influences of childhood experience, on becoming a mother, relating to the unborn child, and the meaning of treatment. The findings and their implications for treatment planning and support are discussed as a contribution to discussions of issues around compulsory treatment for pregnant woman with an SUD.
Keywords
Introduction
This article explores the thoughts of pregnant women who are in voluntary or involuntary treatment for substance use problems. It sheds light on their thoughts about motherhood, their unborn child, and the treatment they are receiving. There exists a vast amount of research and literature on pregnant women struggling with substance use problems and their potential for providing adequate parenting (see, e.g., Flykt et al., 2021; Weber et al., 2021). Further, research has shown that women who have long-term problematic use of drugs often have limited resources and poor social support; they are also less well educated and their pregnancy is often unplanned (Lund, 2013; Mayes and Truman, 2002; Pajulo et al., 2012; Suchman et al., 2005; Wiig et al., 2017). Furthermore, they show more distrust in relationship settings (Håkansson et al., 2018a), which also might affect their experience of being in treatment. A large body of evidence has found harmful effects on children who were exposed to substances prenatally and the literature documents an accumulation of risk factors because of biological, psychological, social, and environmental vulnerability (Helmbrecht and Thiagarajah, 2008; Moe et al., 2010; Söderström, 2012; Söderström and Skolbekken, 2012; Topley et al., 2008; Vucinovic et al., 2008). There are probably many children with various difficulties due to their mothers’ alcohol consumption during pregnancy who never receive a diagnosis and best practice. The World Health Organization recommends screening of all pregnant women for alcohol use as early as possible (World Health Organization, 2014). An observational study of 4067 pregnant women from the general population in Norway (Finanger et al., 2021) found the blood biomarker of alcohol consumption, phosphatidylethanol, in 1.4% of the women around gestation week 12 and 0.4% around week 24. 0.4% is estimated to correspond to about 200 children in Norway each year.
Many of these women have experienced a childhood of trauma, parental substance use problems, and abusive relationships, which can affect their capacity to reflect on their own childhood relationships and their caregivers’ mental states, which in turn could lead to negative internal working models of parenting (Bowlby, 1988; Dube et al., 2003; Mayes and Truman, 2002; Murphy et al., 2014; Neger and Prinz, 2015). Through the years, a vast amount of research has demonstrated a link between adult attachment and parenting (George and Solomon, 1996; Jones et al., 2015). The Adult Attachment Interview is a semi-structured qualitative interview, originally developed to predict a person’s own attachment strategies, in which the capacity to reflect on childhood relationship experiences and the caregivers’ mental states is assessed (George et al., 1984/1985/1996).
Adverse childhood experiences may also make sensitive parenting difficult, including a negative effect on parenting mentalization (Fonagy et al., 2002; Håkansson et al., 2018b). Parental mentalization has been defined as the parent’s ability to interpret their child’s behavior in terms of envisioned mental states, such as emotions, thoughts, desires, and intentions (Zeegers et al., 2017). Parental mentalization has been shown to be linked to and important for attachment security in offspring (Zeegers et al., 2017). In addition, there is evidence to suggest that the children of mothers who are more inclined to mentalize show higher mentalization ability themselves, display less psychological stress, have higher capacity for physiological regulation, more satisfying relations with peers, display fewer behavioral problems, and have a reduced risk of general psychopathology (Shai and Belsky, 2017). Furthermore, there seems to be a link between the extent to which pregnant women tend to talk about what the unborn child might be like and mentalization 6 months after birth (Arnott and Meins, 2008). Mothers who express more maternal-fetal attachment have shown a higher degree of parental mentalization by using more words related to mental states when they talk about their child up to 19 months after birth (McMahon et al., 2016). It is interesting that Bowlby, the founder of attachment theory, did not himself use the concept of attachment from the parental perspective, since he considered “safety seeking,” not “safety providing,” as a central aspect of the attachment system (Slade and Sadler, 2018). There are different approaches to assess parental mentalization with different focuses, such as parental mind-mindedness, parental insightfulness, and parental reflective functioning (Zeegers et al., 2017). Parental reflective function refers to parents’ skill in interpreting the mind of their infant and the ability to recognize how the child feels and thus act accordingly (Fonagy et al., 2002). Mothers with substance use problems have been shown to have lower parental reflective functioning than parents in the general population (Håkansson et al., 2018a). The Working Model of the Child Interview developed by Zeanah and colleagues (Benoit et al., 1997; Zeanah et al., 1996) was originally developed to study mothers’ representations of their child and has been widely used in research (Slade and Sadler, 2018). However, changes in the wording in the interview have also enabled it to be used prenatally to assess mothers’ representation of their unborn child and their thoughts, feelings, and intentions concerning the child.
There exist various interventions that can support and help pregnant women who struggle with substance use problems, but they are not used in proportion to the need (Weber et al., 2021). In Norway, the use of compulsory treatment for this group of women with substance use disorders (SUD) was legalized in 1996 in Section 10.3 of the Social Services Act (Søvig, 2007). The rationale for compulsory intensive treatment interventions for pregnant women with SUD is primarily to protect the unborn child. Norway is the only country in Europe with such legislation (Leppo, 2009). The core of Section 10.3 is that pregnant women with an SUD can be detained in inpatient treatment without consent if it is reasonably likely that the fetus can be harmed and if voluntary health measures are insufficient (Søvig, 2007). A second legal possibility for compulsory treatment is “voluntary coercion,” defined in Section 10.4, which states that the patient may be retained in inpatient treatment based on her consent for 3 weeks. This agreement can be renewed up to three times. Although the use of § 10.4 is presented as a first choice, it is little used with pregnant woman with an SUD. Part of the explanation may be that these are often women with a long-term heavy substance use problems, with whom voluntary treatment has been tried several times (Søvig, 2007). The legislation is supported by research showing that compulsory treatment plays an important role in successful treatment and rehabilitation of people with substance-related problems (Sullivan et al., 2008), but there has been concern about unintended negative effects (Søvig, 2011). Söderström and Skolebekken (2012) conclude in their study that § 10.3 may be related to unintended effects in the process of preparing for parenthood in a safe environment. Little is known about whether being hospitalized in involuntary treatment adds to the challenges these women experience (Lundeberg and Mjåland, 2009). Söderström and Skolbekken (2012) emphasize the need for further evaluation of the consequences of § 10.3, preferably in comparison with voluntary interventions. Furthermore, there is stigma connected to pregnant women who have substance use problems (Weber et al., 2021), and their substance use is often seen from an individualized and moralizing perspective, detached from contextual factors, by providers of interventions and support as well as in society at large (Benoit et al., 2014). This can create barriers for pregnant women with SUD to seek support and help.
Against this background, we wanted to gain a deeper understanding of how pregnant woman in voluntary and involuntary treatment reflect on their own upbringing, childhood experiences, pregnancy, and motherhood. A deeper understanding of these women’s perspectives might inform the creation, implementation, and use of different interventions for support and treatment.
Aim
The overarching aim of the present study was to explore the thoughts about motherhood and their unborn child of pregnant women in voluntary or involuntary treatment for substance use problems, and to explore the women’s childhood attachment experiences. Our more specific research questions concerned their thoughts about their own childhood, themselves as mothers, and their unborn child. In addition, we wanted to gain a deeper understanding of potential differences in the narratives from women in voluntary and involuntary treatment, which could inform future research.
Methods
The 16 participants in this study came from three of the four facilities in Norway that specialize in inpatient treatment for substance use problems. The head manager and the department manager of each treatment facility were contacted for permission to conduct the study. The leaders of the three facilities were contacted for clearance and initiation of the interviews. All the participants were pregnant women with an SUD. Eight of the women were in compulsory treatment and eight in voluntary treatment.
Participants
The women who were asked to participate in this study all met the inclusion criterion of substance-dependent pregnant women in inpatient treatment in substance abuse facilities on a voluntary or involuntary basis. The average age of the participants was 27 years (range 17–44 years), and the women were at different stages of their pregnancies at the time of the interviews, varying from 9 to 39 weeks. All had been diagnosed with SUDs according to the International Classification of Diseases 10, F10–F19: Mental and behavioral disorders due to psychoactive substance use, usually classified as dependence syndrome (World Health Organization, 2004). All had been using different substances concurrently, such as alcohol, cannabis, and amphetamines. Some had also used additional substances such as prescription drugs, for example, benzodiazepines, and some had been taking opiates. At the time of the interviews, they were not using substances since they were in treatment but were still considered to be substance dependent. All participants reported that their parents had SUD for most of their childhood. One woman reported other family problems and had spent most of her childhood in care. These families were all living on welfare, with little employment, low income, and poor housing. All the women were born and raised in Norway with ethnic Norwegian parents. Five of those in compulsory treatment were first-time mothers. One of them had a child for whom she had retained custody, while two others had lost custody of their children because of problematic substance use. Seven of the women in compulsory treatment reported having a stable relationship with the unborn child’s father, and six of these fathers were substance dependent and actively using various substances. All the couples had a short relationship history.
Four of the women in voluntary treatment were first-time mothers. Two of them had children for whom they had relinquished custody because of substance use problems, one had two children who both lived with their father, and one woman had one child being raised by her aunt. Six of the women were in a relationship with the father of their unborn child, and three of these fathers were staying in the family unit with the women.
In-depth interview guide
A thematic semi-structured interview guide was used to organize the interviews. The interview guide was constructed with the ambition to foreground the women’s narratives and to be as open as possible to their experiences. In the first part of the interview, the women’s experiences of involuntary or voluntary treatment were explored. The second part of the interview was inspired by and based on elements from the Working Model of the Child Interview (WMCI) (Zeanah et al., 1996), in which the focus was on the mother’s representations of the unborn child, and what thoughts, feelings, and intentions she had about the child. The questions in the third part of the interview guide were inspired by the Adult Attachment Interview (AAI) (George et al., 1984/1985/1996; George and Solomon, 1996). In the present study, elements of the original AAI interview guide were used to explore the women’s childhood attachment experiences, including their experiences of how their parents showed care. They were also encouraged to describe how they handled rejection and separation, such as being placed in foster care. Finally, the women were asked to summarize how they thought their childhood experiences had affected their ability to be the kind of mother they wanted to be.
The responses on the questions inspired by the WMCI and AAI were not encoded according to the two coding systems. The primary objective was to obtain descriptions, or discover a lack of descriptions, in the areas mentioned above. By using elements from the AAI and exploring internal working models, we focused on the overall problem and the research questions.
Interview procedure and ethical approval
The research was approved by the Norwegian Ethics Committee (REK number 2011/916C) and followed the guidelines of the Helsinki Declaration. The first author contacted all the participants and provided oral and written information about the study. Participants provided signed consent and were told that they could withdraw from the study at any time. The first author (SMM) conducted the interviews in each facility, audio recorded them, and transcribed them in full. She has intimate knowledge of the client group based on previous lengthy clinical experience. This was helpful in attempting to adopt an approach that showed sensitivity to the informants. The last author (UA) has long experience as a family therapist and psychologist in child and adolescent mental health and social services, but not specifically with the client group in question. All participants were offered follow-up conversations with a resident therapist after the interview, but none took up this offer.
Analytical strategies
We chose a phenomenological/hermeneutic analytical approach based on Giorgi’s (1985) and Malterud’s (2012) principles of phenomenological analysis of qualitative data. The most important objective of a phenomenological thematic analysis is to understand experiential phenomena from the perspectives of the informants and to elicit descriptions of the world as close to the informants’ experiences as possible. A hermeneutic perspective complements the pure phenomenological method. In a hermeneutic interpretation of phenomenology, prior understanding is not viewed as a problem but as a resource in the encounter with the subjective experience to be explored. In the reflexive process of analyzing the data, the researcher’s concepts and theoretical resources are used as tools to enable reflection on the experiences expressed in the interviews (Willig, 2021).
A systematic thematic cross-cutting analysis suitable for analyzing transcribed in-depth interviews was chosen. The analytical process was implemented in four steps. The first step was to provide an overview over the interview data. Different themes emerged from participants’ descriptions of their understandings and experiences in response to the author’s questions. We selected themes that were relevant to the research aims. The next step was to identify meaning units in the selected texts and sort them into different codes across the interviews. All the authors were involved in the analysis, in addition to an external expert in qualitative methods who provided a further perspective. After new readings, the third step was to condense the codes in terms of their significance and meaning. The final process of analysis was to synthesize the significance of the condensates into new concepts and descriptions called categories. The 16 interviews were initially analyzed separately and then subsequently compared in this analysis. The resulting categories are presented in the following section.
Findings
Categories and themes.
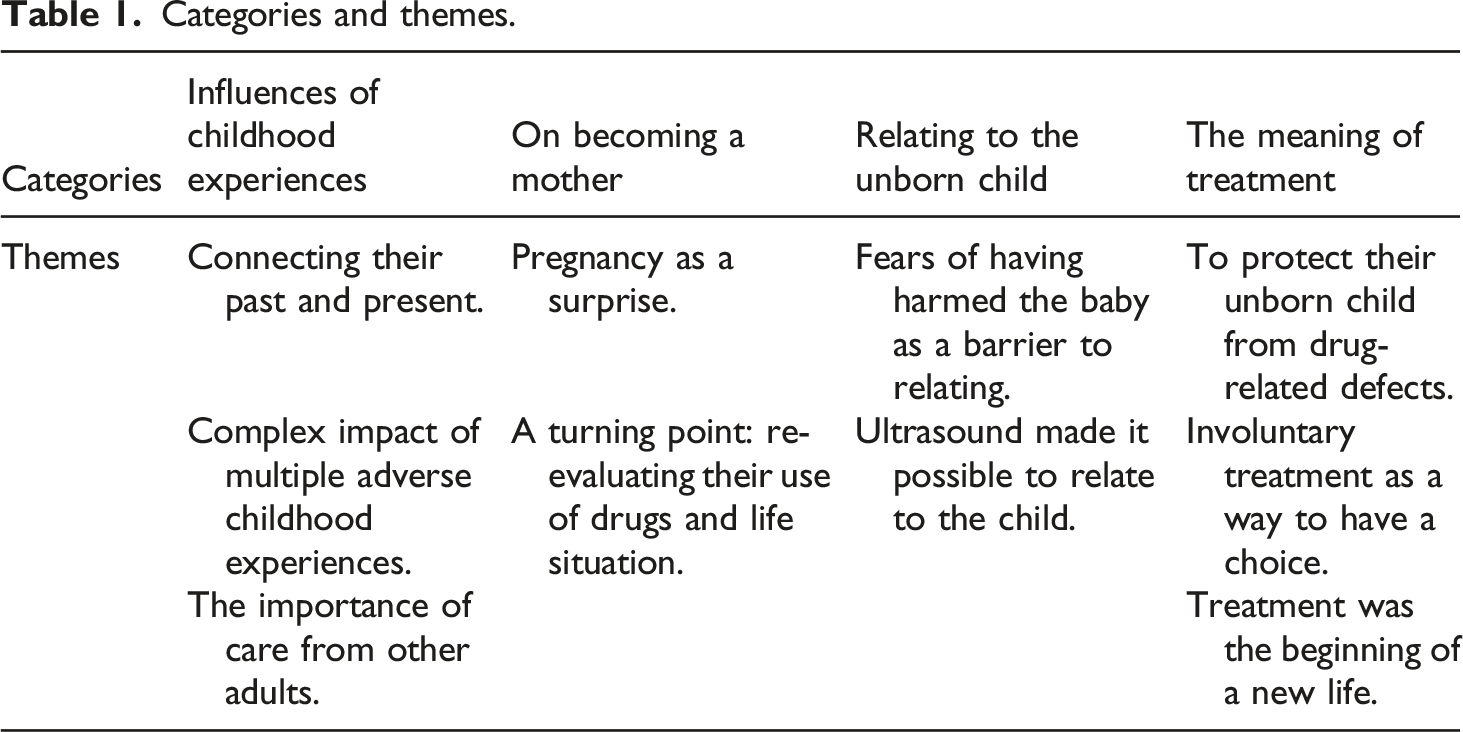
Influences of childhood experiences
For the women in involuntary treatment, it was a new idea to think about themselves in a context that connected their past and present: “No, I don’t know really, it’s completely new to think that way” (Linn). They had reflected little on the possible consequences of their childhood experiences for relating to their unborn child. It’s painful what’s come up now. No, I don’t know really, that I haven’t had family and others around me. It’s so hard to think about that I mustn’t make the same mistakes. I want to be there for my children (Sara).
In contrast, all the participants admitted to voluntary treatment were preoccupied with connections between their own childhood experiences and what they wanted for their unborn child: “I believe my childhood has influenced me a lot in relation to how I am today” (Heidi).
The women described growing up in difficult family settings, including the complex impact of multiple adverse childhood experiences. All the women in involuntary treatment talked about a childhood dominated by dysfunctional family interaction, broken families, and problematic substance use. They talked about painful and traumatic separations, stays in child care facilities, and how they had had few or no reliable caregivers. In an uncertain and partly negligent childhood, the women had been left alone as children with no relational support. Their experiences reflected unsafe and unpredictable relationships. I remember that I felt quite insecure many times. I think I was quite close to mom when I was little. I think probably that I was a bit nervous that she would get sick again. I was afraid of being left alone and tried to please her. I can’t remember exactly but I think my mom loved me (Leah). The only person I felt close to when I was growing up was my sister, and she abused substances. I didn’t have a good relationship with my mother because she kind of gave me up and pushed me away (Sara).
This group of women described how they lacked experiences of belonging. Their narrative style was brief, constricted, and without much imagery. Their narratives reflected difficulty in connecting the past to the present. They had few reflections on how their own adverse childhood experiences could affect them as mothers. However, some of those in voluntary treatment felt that it was important to be aware of these negative experiences in order to mitigate their effect on their present life situation. I will try to take my experiences on board because I think people are very dominated by the childhood they’ve had and it’s easy to transfer it if you’re not very aware of what you want to avoid (Anna).
They also had richer descriptions of what they wanted to pass on to their child and made more connections between their own childhood experiences and the mothers they wanted to be, including what they did not want to pass on to their own child. We’ve talked about what kind of parents we want to be. I’ve worked on events from my own childhood, looked at what I want to take into my role as a mother and what I don’t want to pass on (Susan).
Women admitted voluntarily described some experiences of care from other significant adults, illuminating the importance of care from other adults, not because of, but in spite of, their parents’ problematic use of substances. My neighbour was a sort of grandmother type; I went there when there was trouble at home. I got hot dogs and mashed potatoes, she must have known how things were for me, but we never spoke about it (Anna).
The women who were in compulsory treatment had no such descriptions of supportive relationships outside their family. However, those in voluntary treatment provided varied descriptions of supportive early experiences from different places and people, such as at school, the neighbor’s wife, as well as developing their own resources, such as being good at schoolwork, which is defined as a protective factor. “At school I had normal adult contact in relation to what I did and what I could achieve. That was what saved me because I was good at school, but no one had any idea how things were for me at home” (Hannah).
Some of the women in involuntary treatment also described some school and work experiences, but the most prominent descriptions were related to the lack of such supportive experiences.
However, although the women described receiving external support when things became difficult, they also said that no one helped them to talk about and process traumatic and difficult experiences, because the substance-related interaction in their family was never spoken about. Support of this kind was arbitrary, not in the form of systematic public care provision. Nevertheless, they described some supportive relational experiences that came to form part of their expectations of others, even in adulthood.
On becoming a mother
The second category was the women’s descriptions about becoming a mother. For all the participants, the pregnancy was unplanned and they therefore experienced the pregnancy as a surprise. They had believed that they could not become pregnant, and it had taken a long time to interpret their symptoms as signs of pregnancy. The symptoms were perceived as consequences of a complicated lifestyle with SUD, poor nutrition, and poor general health. It was unreal, I never thought I could get pregnant. But it was a big wish for me. Most women wish for children. I thought I would die of substance abuse because of the life I lived. Then this happened (Kari).
The participants spoke in different ways about how they had experienced reaching “the bottom” and how their pregnancy had become a turning point in which they were re-evaluating their use of drugs and life situation. Getting high was now experienced as a vicious circle they had long tried to break. When I found out I was pregnant, I immediately responded. I called my social worker on a Monday, and on Wednesday I was hospitalized for detoxification. I wanted help, I wanted this child (Kari).
For women in voluntary treatment, awareness of the pregnancy as a turning point was succeeded by an already existing wish and some existing experiences of the possible content of a drug-free life: “I want to be a mom who is clean, who loves herself and feels ok with herself” (Kari).
In contrast, women in compulsory treatment described having had no previous wish to become drug free nor any thoughts about making an issue of their SUD behavior. Their main feeling was that they had been thrown into having to decide whether to keep the baby or not. They realized that for them to give their child a life, they could not continue taking drugs. They described their struggle to get clean and therefore their early ambivalence about motherhood, and several had considered abortion as a solution. In the beginning, it was very difficult because I had strong cravings to get high. I just wanted to get rid of the baby so I could get high again (Linn).
Relating to the unborn child
The third category is the women’s descriptions of how to relate to the unborn child. All the participants described fears of having harmed the baby. When they discovered the pregnancy, this fear appeared to be a barrier to establishing a relationship with their expected child: “I was afraid the baby had been harmed by my abuse. I didn’t dare to think about it” (Anna).
Women admitted involuntarily described the ultrasound as a crucial point which made them realize that they had to choose between continuing using intoxicating substances and their child. The image awakened their emotions and helped them to understand that they would be mothers. The most prominent feeling in their descriptions was their relief at not having harmed the baby. When I knew that everything was OK, and that there wasn’t anything wrong, that my baby hadn’t been damaged by my drug abuse, I could bond with the baby. Because I was getting high while I was pregnant without knowing I was pregnant (Leah).
Several of the women acknowledged the importance of the ultrasound. They described how the ultrasound made it possible to relate to the child. “At the ultrasound examination, I could see quite a large baby with ten fingers and ten toes, wow, and it never passed my mind to have an abortion” (Heidi).
The meaning of treatment
The final category deals with the women’s descriptions of the meaning of treatment. The participants from both groups acknowledged that their treatment context, either compulsory or voluntary, helped them to protect their unborn child from drug-related defects. A striking finding was that all the women in involuntary treatment except one had asked to be admitted on a compulsory basis (§ 10.3) when they discovered they were pregnant. Furthermore, all those in compulsory treatment described the involuntary admission itself as helping them to manage their craving for substances. The women talked in different ways about how their use of intoxicating substances conflicted with their pregnancy and how difficult it was to stop taking drugs on their own. Their main wish was to protect their unborn child from further intoxicating substance-related damage, but their craving for drugs did not give them a realistic choice between drugs and the child. Some participants had lost custody of children previously, even though they had been in voluntary treatment. They did not have an underlying desire to become drug free, and their reactions to the pregnancy must be seen against this background. However, when in treatment this time, the pregnancy became a reason to stop getting high and the only way that they could experience having a choice was through being in involuntary treatment. In a paradoxical way, some said that they regarded involuntary treatment as a way to have a choice. They talked about how they needed the structure of the involuntary setting to help them get clean. “I needed the framework of compulsory treatment; I couldn’t manage on my own” (Nina). They knew from earlier experiences that they would not manage it in voluntary treatment. I don’t care about the coercion, but more about what happens next. When I came here, it woke me up (Anna).
The women talked about feeling fed up with their problematic substance use and how entering treatment saved them from continuing the vicious circle between sober periods and relapses: “I’ve been fed up with getting high for a long time, it’s no fun at all, just a vicious circle that just gets bigger and bigger” (Marianne).
Women receiving voluntary treatment talked about what they understood to be a normal life. To start treatment was the beginning of a new life that was drug free and an “ordinary” life. These participants had already taken the decision to quit taking drugs. They described several motivational factors for giving up their use of intoxicating substances, such as being at rock bottom, and experiencing pregnancy as an important factor in the process of wanting a normal life. Being pregnant represented a turning point in relation to an already existing wish to be drug free, even though “getting clean” was described as a big complex job. They combined their desires to lead a normal life and to protect their unborn child. They described finding work, important relationships, and other professionals as helpful. They had hope for the future and related their hopes to dreams about being “clean and having a normal life” and being a good enough mother. Almost all the women admitted voluntarily had some experience of work and studying. In this way they had a perspective on what they wanted to achieve. They also described the care they had received in relationships outside their families, such as at school, with neighbors, and in foster homes.
Discussion
The aim of the present study was to explore the thoughts about motherhood and their unborn child of pregnant women in voluntary or involuntary substance use treatment, and to gain insight into their childhood attachment experiences. Our more specific research questions concerned their thoughts about their own childhood, themselves as mothers, and their unborn child and to gain a deeper understanding of potential differences in the narratives from women in voluntary and involuntary treatment.
Jääskeläinen et al. (2016) argue that women who have substance-related disorders and are seeking help are motivated to act in the interests of their unborn child, which also applies to the women in this study. The participants were in two treatment contexts, based on voluntary or involuntary admission. There is much in common in their stories, but our analysis also revealed some possible differences. We will therefore not only discuss the different categories and themes that emerged but also discuss some of the possible differences between the narratives of the women in the two treatment contexts.
All the informants in voluntary treatment expressed concern about experiences in their own childhood and how they could affect their current behavior and their relationship with their unborn child. In contrast, the women in involuntary treatment reflected little on how their history would influence their relationship to the child. A previous study found that for this group of women it was a new experience to reflect upon connections between past and present, and their narratives about their past demonstrated a lack of elaborate language and of signs and symbols of reflection (Myra et al., 2016). While all the women in this study experienced the complex impact of multiple adverse childhood events, there were also differences in their descriptions of compensatory relational experiences. Those in voluntary treatment described receiving some care from other adults, but no such descriptions were found among the women in compulsory treatment. This group had few narratives that could link their childhood relational experiences to their current situation and they expressed anxiety and ambivalence about their future role as a parent. The potential difference between the two groups could reflect the impact of protective factors on the women in the voluntary group. Velleman and Templeton (2016) define the concept of resilience as the capacity to overcome adverse experiences and stress. Resilience is defined as an outcome of the dynamic interactions of protective factors, which include biological, psychological, social, cultural, and political issues that affect a child’s life. In this way, the women admitted voluntarily described resources in their relational history that could be used as a bridge to their developing attachment to their unborn baby. These women had experienced difficulties in their families of origin but had caring relationships with significant adults outside their nuclear family. Their narratives connected the past and the present in an expanded storyline in ways that showed the potential to create a reflexive positioning with their unborn child. They also emphasized the importance of help from professionals as crucial to their recovery and to enhancing their attachment to their unborn baby. These women thus had a different basis for establishing a relationship with their child.
Suchman et al. (2018) conclude that “improvement in maternal reflective functioning and caregiving representations could lead to improvement in caregiving sensitivity” (p. 21). Understanding how earlier childhood experiences of being cared for affect the possibilities of good enough mothering is crucial in this process. This seems to be of great importance since it is important to help mothers who have substance use problems to understand their own inner experiences of being a mother and the emotional needs of their child in addition to learning parenting behaviors (Suchman et al., 2018).
For most of the women, the pregnancy was unplanned and came as a surprise, which is in line with previous research (Pajulo et al., 2016). This was especially true for the women in compulsory treatment who all confirmed this. However, all the women in this study pointed out that the pregnancy constituted a turning point which made them re-evaluate their drug use and the state of their lives. Such turning points have been described in terms of existential crises. Experiences or events of this kind serve to stimulate or trigger new decisions, and one such trigger could be pregnancy and the birth of a child (McIntosh and McKeganey, 2000). All the women expressed fears of having harmed the baby and how they wanted to protect their baby from long-term consequences which is in line with findings from Van Scoyoc et al. (2017), who also describe how the women try to engage in different harm reduction behaviors even before receiving treatment. Whereas the women in the voluntary group in the present study gave expressions of already wanted change, and the pregnancy became another important reason to get into treatment, the women in the involuntary group described no underlying desire to become drug free, and their reactions to the pregnancy must be seen against this background. Several of the women described how their fear of having harmed the baby became a barrier to relate to the baby. This is also reported in previous research which has shown how feelings of fear of having harmed the baby, guilt, and stigmatization can increase anxiety and motivation to seek treatment (Pajulo et al., 2016). The women in our study described how the ultrasound was one element that enabled them to relate to their unborn child. This is in line with Boukydis et al. (2006) and Pajulo et al. (2016). Boukydis et al. (2006) found that for mothers who attended a public ultrasound clinic, having an ultrasound consultation improved prenatal attachment and decreased maternal anxiety more effectively than the routine ultrasound screening session available at the clinic. The ultrasound consultation was also found to increase positive maternal feelings toward the fetus and encourage the women to take better care of their own health. Pajulo et al. (2016) described the rationale behind a study with the aim to find tools that would enhance the mothers’ interest and emotional connection with the fetus. This, in turn, was considered to motivate the mothers to reduce their substance abuse and to take better care of their own health. They used interactive ultrasound imaging and a pregnancy diary, which could also be adjusted and used with parents and families in primary health care settings. They argued that the impact of interactive ultrasound and the pregnancy diary in supporting positive attitudes and interest in the child may be significant in preventing early relationship problems. In our study the informants described the ultrasound scan as a turning point, which made them realize that they had to choose between continuing using intoxicating substances and their baby. The scan awakened their emotions and helped them to understand that they were going to be mothers. However, the interviews indicate that it seems as if the women in the voluntary and the involuntary groups needed different treatment frameworks. Those in voluntary treatment were already more motivated to make changes. They showed greater ability to connect their past experiences and relational history to their present situation. They found it easier to see the relevance of their previous experiences, which thus enhanced their efforts to make a clear break with drugs. They wanted changes in their lives. The women in involuntary treatment also had ideas about the kinds of experiences they did not want for their own children but found it difficult to articulate how they could avoid these. This could be related to the lack of caring relationships in their own childhood. Some of them expressed the need for an involuntary context to enable them to adopt a position where they could establish a caring relationship to their unborn child. Compulsory treatment was necessary to enable them to relate to the child. The child’s needs became a specific topic in their minds, which helped them to reflect on their child. Additional support was provided by a therapeutic relationship that could focus on the parts of their own history that influenced the current and future mother–child relationship. These women needed a treatment context which enabled them to recognize, understand, and regulate themselves as caregivers in order to relate to the perspective of the child. From the narratives, it seemed as if the women in involuntary treatment needed such structures to adopt these positions to a larger extent than the women in the voluntary group. Attachment research points out that parental mentalization is a critical factor in the transmission of secure attachment from one generation to the next (Fonagy et al., 1991; Slade et al., 2005). Parental mentalization can be understood as the degree to which a parent develops nuanced mental representations of the caregiving relationship. It is therefore dependent on the ability of the expectant parent to draw on her or his own relational experiences to meet the needs of the child. To have a focus on this seem to be of crucial when working with pregnant woman with an SUD who are in treatment since maternal reflective functioning and mental representations of caregiving are core mechanisms for maternal sensitivity (Suchman et al., 2018). The findings in this study also point in the direction that women in different treatment contexts might need different treatments to break the cycles of insecure attachment, due to differences in their childhood experiences.
Strengths and limitations
A strength in this kind of research was that every in-depth interview given so generously by the participants about such sensitive matters provided valuable and detailed knowledge about their understanding of their experiences due to the different treatment contexts. The study therefore provided vital insights for therapeutic practice and further research.
Another strength of this study is that the participants were recruited from three of the four facilities in Norway providing voluntary and involuntary treatment for pregnant women with an SUD. A limitation is that the findings cannot be generalized to a larger population, since Norway is the only country in Europe where treatment for pregnant woman with an SUD is mandated by law if harm to the fetus is considered probable. A further limitation is the self-selection of women who agreed to participate in the study. However, the study does not aim to present generalizable results, which would require a different design, but to listen to, analyze, and convey the narratives of women in voluntary or involuntary treatment for substance use problems. It is also important to notice that even if one of our research questions was to examine potential differences in the narratives from women in voluntary and involuntary treatment we cannot draw any conclusion from comparing the groups, since that would need another research design with a higher number of participants. Thus, the ambition was to gain a deeper understanding of potential differences that could generate hypothesis that could be tested in future research. We also hope that this study can contribute to nuanced discussions of compulsory treatment for pregnant women with an SUD.
Clinical implications and conclusions
The findings of how the relational history of the pregnant women influenced their capacity to relate to their unborn child provided some crucial descriptions to help address the complexity of the therapeutic context. The study shows that both motivation and relational history need to be taken into account when deciding on the optimal therapeutic context to bring about change. This study reflects themes that have important implications for planning treatment and support. It underlines knowledge about how difficult SUD-related family interactions and previous relationship experiences can lead to complicated, generationally determined problems in later life. The childhood experiences of the women in the present study created ambivalence and lack of faith in their ability to be a “good enough mother” and affected how they positioned motherhood. In that way, parenting style can be replicated from one generation to the next, unless the person manages to achieve a comprehensive break with the past. Contrary to existing research, some of the women in our study underlined the need for compulsory treatment as the only way to provide the necessary structure to address their substance use problems and help them to connect with their unborn child. These women’s experiences and reflections could be essential contributions to the field of treatment, both within and outside institutional contexts. It is sometimes important to combine efforts to process different aspects of life experiences with creating environments that give mothers in need of new attachment experiences a stable and caring life situation.
Footnotes
Acknowledgments
We are especially grateful to Vigdis Wie Torsteinsson who was involved in the beginning and the planning of the study, but who sadly passed away recently. Vigdis was a crucial source of inspiration and knowledge in this work. We would also like to thank all the women who participated in the study for sharing their difficult experiences.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.