
Abstract
The transforming care programme aims to increase care provision in the community for individuals with learning disabilities (LDs) in the United Kingdom resulting in more parents taking on carer responsibilities. Previous research suggests that having a child with LD may be associated with impaired mental health in parents. However, previous reviews have often conflated poor mental health with wellbeing or quality of life and have grouped people with LD together despite the LD severity and/or the underlying cause of LD, both of which may have different types of impact on parents. This review aims to critically appraise and synthesise the literature on the mental health of parents with children with LD of unknown cause to answer the question, ‘Do parents of individuals with LD of unknown cause experience diagnosable mental health difficulties?’ Following PRISMA guidance, this systematic review found seven studies, obtained from four databases, meeting a strict set of inclusion and exclusion criteria. Studies were assessed against the Quality Assessment Tool for Quantitative Studies. A narrative synthesis of the results found that rates and severity of diagnosable mental health difficulties were higher in mothers of children with LD of unknown cause than mothers of typically developing children, Down syndrome and LD of known cause, but lower than mothers of individuals with autism spectrum disorder. LD severity also appears to be a factor impacting parental mental health. Findings suggest that LD services need to provide more psychological support for parents and families.
Introduction
Also referred to as ‘intellectual disability’ and ‘mental retardation’, learning disability (LD) is defined as a significantly below average intellectual ability along with impairments in social and adaptive functioning, present from childhood (National Collaborating Centre for Mental Health UK, 2015; World Health Organisation [WHO], 2019). This paper uses the term LD as it is the widely accepted term in the United Kingdom. A person’s cognitive functioning (which is usually determined via an IQ score) and ability to carry out activities of daily living is used to determine LD severity (mild, moderate, severe or profound) (WHO, 2019). Borderline LD, which is often defined by an IQ of 70–85 (Wieland and Zitman, 2016), is not recognised as a diagnosable disorder; however, individuals who fall within this ‘borderline LD’ category often require intervention (Girimaji and Pradeep, 2018) and thus will be included in the definition of LD in this review.
The estimated prevalence of LD is around 1.5 million in the United Kingdom (National Health Service [NHS], 2018) and 10.4/1000 worldwide (Tomlinson et al., 2014). LD is often associated with or can be caused by a number of different life events and/or comorbid difficulties, for example, traumatic brain injury, meningitis, foetal alcohol syndrome, Angelman’s syndrome, Prader-Willi Syndrome, Down syndrome (DS) and autism spectrum disorder (ASD) (Gillberg and Soderstrom, 2003). A high number of individuals, however (approximately 95 million globally), have LD of an unknown cause (Vos et al., 2015) and appear underrepresented in research.
In the United Kingdom, many individuals with LD are living within settings that may be inappropriate, such as psychiatric hospitals, as a result of their needs not being met within the community. Within these institutions, individuals with LD may be subject to physical and psychological abuse, for example, in the United Kingdom, the well-documented events at Winterbourne View Hospital (Department of Health, n.d). In addition, individuals with LD are often subject to long admissions, are placed far from home and experience high rates of physical intervention and a high number of inappropriate placements (Department of Health, n.d). It is therefore important that we think about how to support these individuals better within the community, to ensure appropriate care. The Transforming Care programme in the United Kingdom aims to increase community care provisions, to do just this (NHS England, 2017) but community care provision both in the United Kingdom and elsewhere could be improved further with a better understanding of mental health impacts in families where a child has LD. Current UK statistics indicate that around 38% of individuals with LD in hospital have been there for over 2 years, 17% are over 50 km from their homes and the majority are on adult mental health wards rather than specialist LD wards (Mencap, 2012). These statistics highlight that despite efforts, services in the United Kingdom are still struggling to support individuals with LD.
One specific area that has not been explored much in the research relates to family systems and the role this may have in the care people with LD receive. This seems relevant given that with the increased demand for community support in addition to the lack of supported living accommodation, a high number of individuals with LD are being placed in the long-term care of their parents (Mencap, 2012). Previous research has demonstrated that the mental health of mothers of an individual with LD is poorer than that of other parents with caring responsibilities (Pinquart and Sorensen, 2003). However, many of these studies consisted of small sample sizes, which along with their lack of comparison to parents of typically developing children, motivated a further review (Rydzewska et al., 2021), which supported previous findings.
Research conducted with parents of typically developing children informs us that if a parent has a mental health difficulty, they may have to rely on their child to take on age-inappropriate responsibilities (Aldridge and Becker, 2003) with their own needs overshadowing the vulnerability of their offspring (Monds-Watson et al., 2010). We know from research in this field that poor parental mental health is associated with child behavioural difficulties (Mowbray et al., 2006) and can impact parent–child attachment (Risi et al., 2021) with insecure attachment contributing to the development of mental health disorders (Mikulincer and Shaver, 2012). With this in mind, it could be hypothesised that having a child with LD, could impact the mental health of parents, which could then overshadow the vulnerability of the individual with LD who may then develop their own mental health difficulties. This may have implications which mean that the individual with LD needs alternative care arrangements; better understanding of this may help prevent inappropriate admissions to psychiatric hospitals and help prevent abuse or neglect occurring in the community.
In their review of mental health among parents of children with LD, Rydzewska et al. (2021) included many of studies which measured wellbeing and quality of life (QOL), labelling this as mental health. Measures of wellbeing and QOL included socioeconomic status, employment and social inclusion, which, although associated with mental health (Kuruvilla and Jacob, 2007; Yu and Williams, 1999), are different concepts. By using these concepts interchangeably, we may over-/under-estimate someone’s mental health by assuming that, for example, all individuals of low socioeconomic status are unwell, and all people with professional jobs are well. These reviews also neglected to include fathers, who within today’s society are increasingly taking on primary caregiver roles. In addition, most of the research did not differentiate between different causes of LD. This is a potential confounding variable, with, for example, parents of children with DS reportedly having better wellbeing than parents of children with other difficulties (Hodapp, 2002). This may be associated with better support for parents of children with DS, variations in behaviours that challenge across the different groups, and many other factors.
This review therefore aims to critically appraise and synthesise the literature on the mental health of parents with children with LD of unknown cause to answer the question, ‘Do parents of individuals with LD of unknown cause, experience diagnosable mental health difficulties?’ It is hoped that this will have implications for services providing support to individuals with LD and their families by highlighting the mental health needs of parents of individuals with LD. The current model in the United Kingdom places an emphasis on supporting the service user (NHS, 2018), with LD services not typically offering psychological support for parents. Parents are instead signposted to parenting classes and support groups, which, although potentially beneficial, often target areas related to wellbeing and QOL, rather than specific mental health difficulties (Law et al., 2002; Lo, 2010). Parents can receive psychological intervention from NHS Talking Therapies or secondary mental health services. However, this could lead to fragmented care and leave parents waiting a significant time for support, when research in other populations has demonstrated that timely intervention may be most effective (O’Donnell et al., 2012).
Methods
In order to fulfil the aim of this review, three concepts were named and defined: ‘LD’, ‘Parents’ and ‘mental health’. ‘LD’ was defined according to the WHO (2019) and included borderline LD. ‘Parents’ referred to the biological or adoptive mother and/or father of the person with LD. For the purposes of the review, ‘mental health’ was defined according to the presence of symptoms related to a diagnosable disorder. This definition was used as it directly relates to how statutory health care services identify and recognise mental health problems, and therefore makes this review clinically relevant. This review also refers to ‘LD of unknown cause’. It should be noted that this refers to an LD whereby the individual has no other known comorbid difficulties which could be impacting their intellectual functioning.
Search strategy
Cochrane (Lefebvre et al., 2021) and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA; Page et al., 2020) were used to guide the search and selection process.
Four databases (CINAHL Complete, APA PsychArticles, APA PsychInfo and Medline with full text) were searched via EBSCOhost in November 2021. Search alerts were set to ensure the inclusion of papers published after this date and found four additional studies. Citation searching was conducted using Web of Science. Search terms used were: (1). ti: m?m OR mother OR maternal OR parent* OR dad OR father OR paternal (2). ab: ‘learning difficult*’ OR ‘intellectual disab*’ OR ID OR ‘cognitive impairment’ OR ‘mental* retard*’ OR ‘low IQ’ or ‘learning disab*’ OR LD OR ‘mental* handicap*’ OR ‘below average IQ’ (3). ‘Mental disorder’ OR ‘mental instability’ OR ‘psychiatric disorder’ OR ‘stress related disorder’ or ‘stress-related disorder’ OR psychopatholog* OR ‘mental ill-health’ OR ‘mental health’ OR ‘mental ill health’ OR ‘psychological distress’ OR ‘mental distress’ OR ‘mental health problem’ OR ‘mental health condition’ (4). #1 AND #2 AND #3
Inclusion and exclusion criteria
For studies to be included in this review, they had to meet the following inclusion criteria: (a) must include parents of children with LD of unknown cause, (b) use of recognised and empirically supported symptom measures of mental health conditions, (c) primary research and (d) published in English. Studies were excluded if: (a) they did not measure symptoms of diagnosable mental health conditions and instead only measured related constructs such as wellbeing or QOL, (b) parents were not the primary caregiver, (c) offspring had comorbid difficulties or known cause of LD and (d) comorbidities or LD cause was not screened.
Study selection and evaluation
The database search identified a total of 402 studies. After removing duplicates and screening titles and abstracts, the full text of 31 studies plus an additional 17 found from extensive citation searching were assessed. Of these papers, seven met criteria to be included in this review (see Figure 1). PRISMA 2020 flow diagram for new systematic reviews (Page et al., 2020).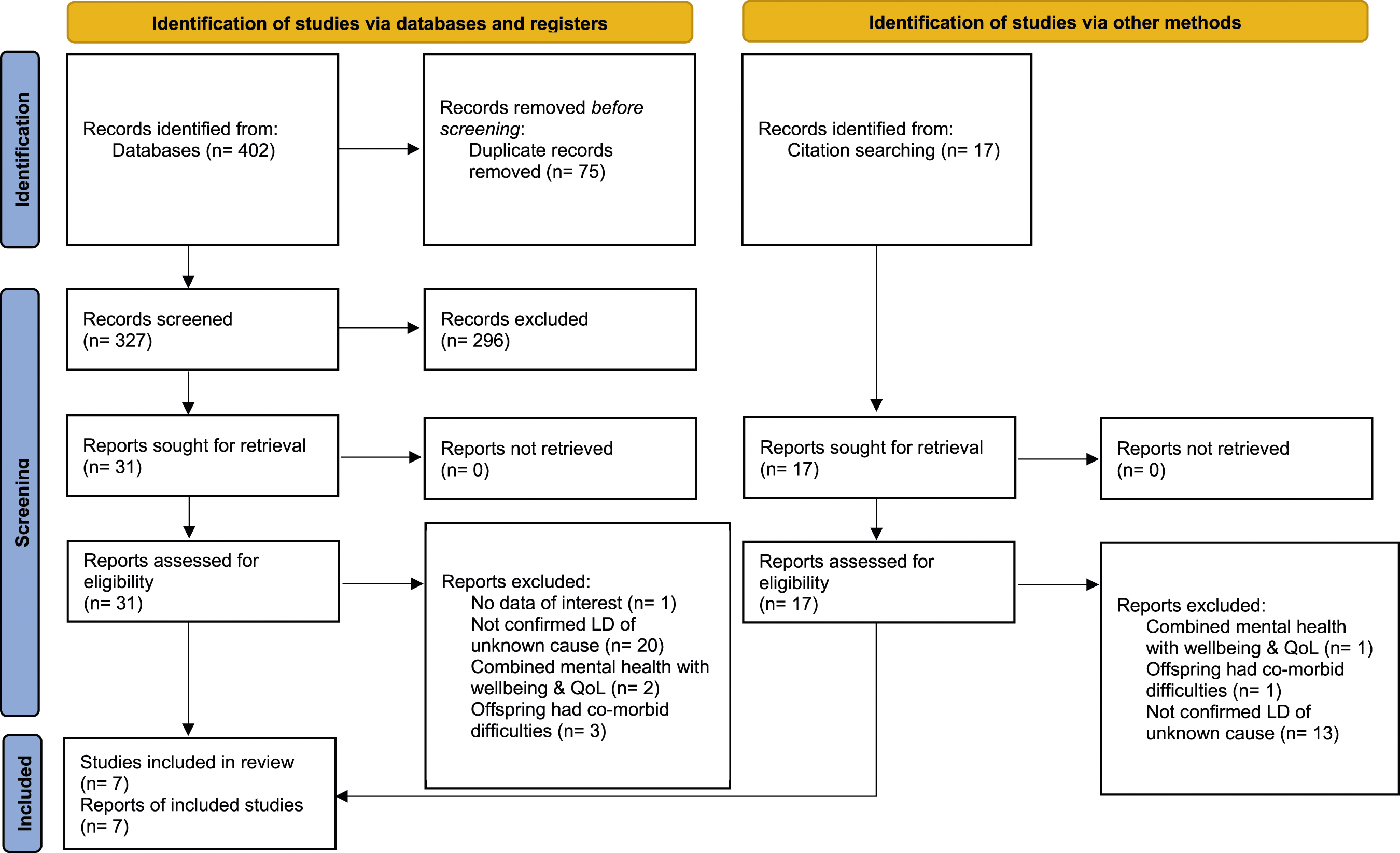
Following PRISMA guidelines, each of the papers underwent critical appraisal, for which the Quality Assessment Tool for Quantitative Studies (QATQS; Ciliska et al., n. d.) was used. This tool, recommended by Deeks et al. (2003), has acceptable content validity, construct validity and inter-rater reliability (Thomas et al., 2004). The QATQS consists of 21 items separated into eight components: selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs, intervention integrity and analysis appropriate to the questions. The ratings for the first six components are used to calculate a global rating. Global ratings include ‘strong’ (no weak component ratings), ‘moderate’ (one weak component rating) and ‘weak’ (two or more weak component ratings).
Statistical methods
Not all of the included studies report the mean and standard deviation for scores on measures of mental health and therefore a meta-analysis was not able to be conducted. Instead, a synthesis without meta-analysis (SWiM; Campbell et al., 2020) guidance was used to conduct a narrative synthesis. All of the available statistics from the included papers have been included within the results. Where available, incidence rate ratios (IRRs) are reported, which provide a statistical estimate of how much more likely parents of individuals with LD of unknown cause were to experience the given symptoms compared to another comparison group of parents. These are presented alongside confidence intervals (CIs) which give a lower and upper estimate of the true IRR value. For studies without IRRs available, percentages are reported, referring to the percentage of parents in the sample that met a given threshold for a particular diagnosis or means (M) along with standard deviation (SD) referring to the mean score on the particular measure chosen. Where a p-value is given, this refers to the significance level of a test comparing difference between two or more groups where a p of .05 or less is normally considered to be statistically significant.
Results
Study characteristics and quality assessment
Study characteristics of included studies.
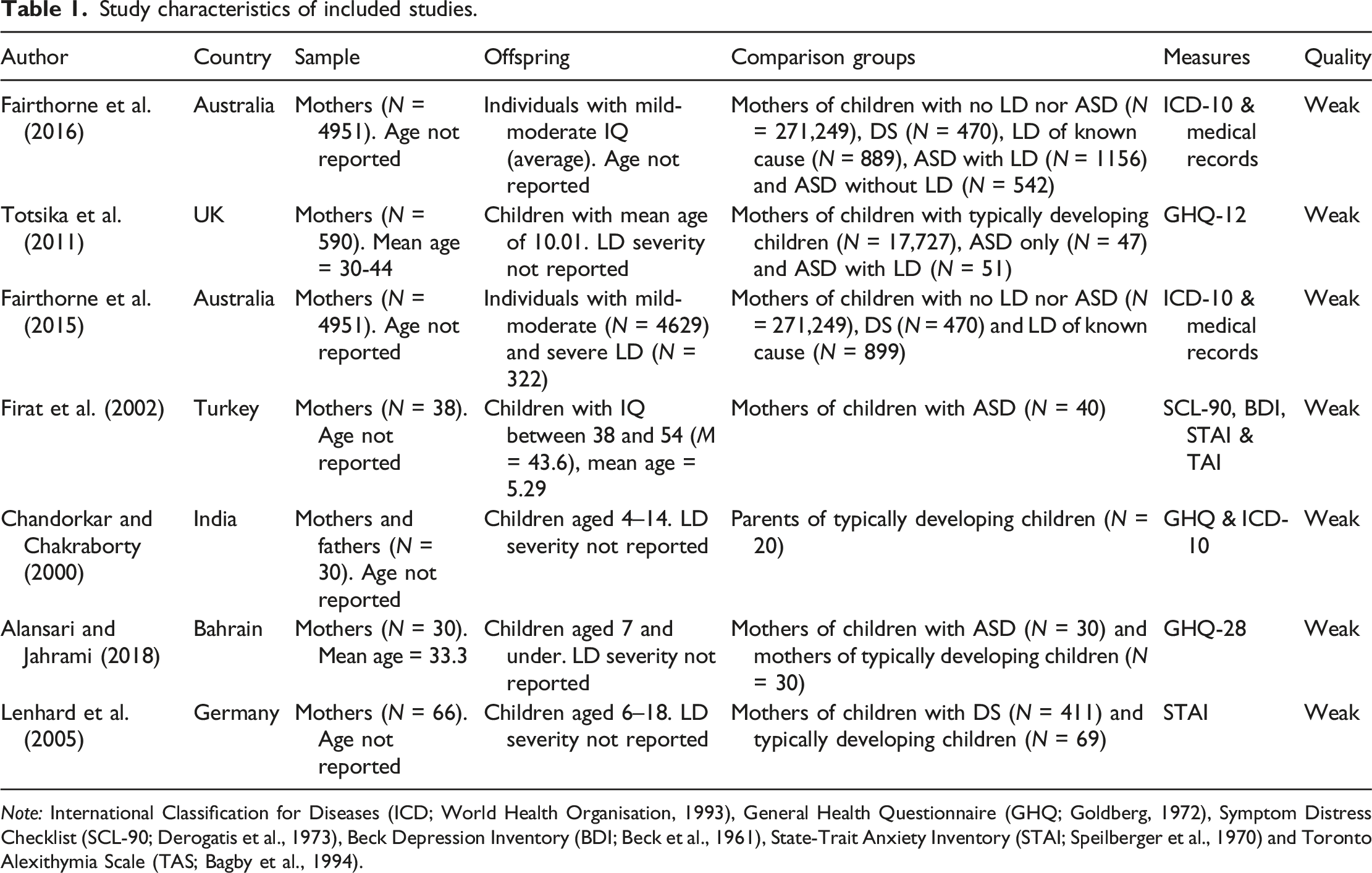
Note: International Classification for Diseases (ICD; World Health Organisation, 1993), General Health Questionnaire (GHQ; Goldberg, 1972), Symptom Distress Checklist (SCL-90; Derogatis et al., 1973), Beck Depression Inventory (BDI; Beck et al., 1961), State-Trait Anxiety Inventory (STAI; Speilberger et al., 1970) and Toronto Alexithymia Scale (TAS; Bagby et al., 1994).
All studies were rated weak in quality, largely due to lack of detailed reporting. The cross-sectional design and lack of blinding also contributed to weak ratings. Despite this, the majority of studies received strong to moderate ratings on selection bias, confounders and data collection method.
Narrative synthesis
Findings are organised thematically according to broad types of diagnosable mental health difficulties. Mood disorders, anxiety- and fear-related disorders, were the most reported and are therefore presented as the two main categories of findings. Obsessive compulsive disorder (OCD) has been categorised as an anxiety and fear related disorder due to it previously being categorised as a ‘neurotic’ disorder in the ICD-10 (WHO, 1993). Studies also measured alcohol and substance misuse, behavioural disorders, personality disorders, schizophrenia, other psychotic disorders and specific difficulties related to mental health diagnoses such as alexithymia, interpersonal sensitivity and paranoid thoughts. Due to little overlap between studies, these were grouped under the heading of ‘other mental health difficulties’. General psychiatric morbidity is the final theme which presents studies where, owing to the type of measure used, it was not possible to place the study into any specific category of mental health difficulty. Totsika et al. (2011) measured ‘emotional disorder’, which was categorised under ‘general psychiatric morbidity’ due to it referring to any mental health disorder characterised by difficulties with emotions and therefore potentially referring to multiple diagnoses (American Psychological Association, n.d).
Mood disorders
Mothers of children with LD of unknown cause experience mood disorders at higher rates than all other comparative mothers, with the exception of mothers of individuals with ASD. Lower levels of depression were associated with mothers having more than one child or a child below the age of three (Firat et al., 2002).
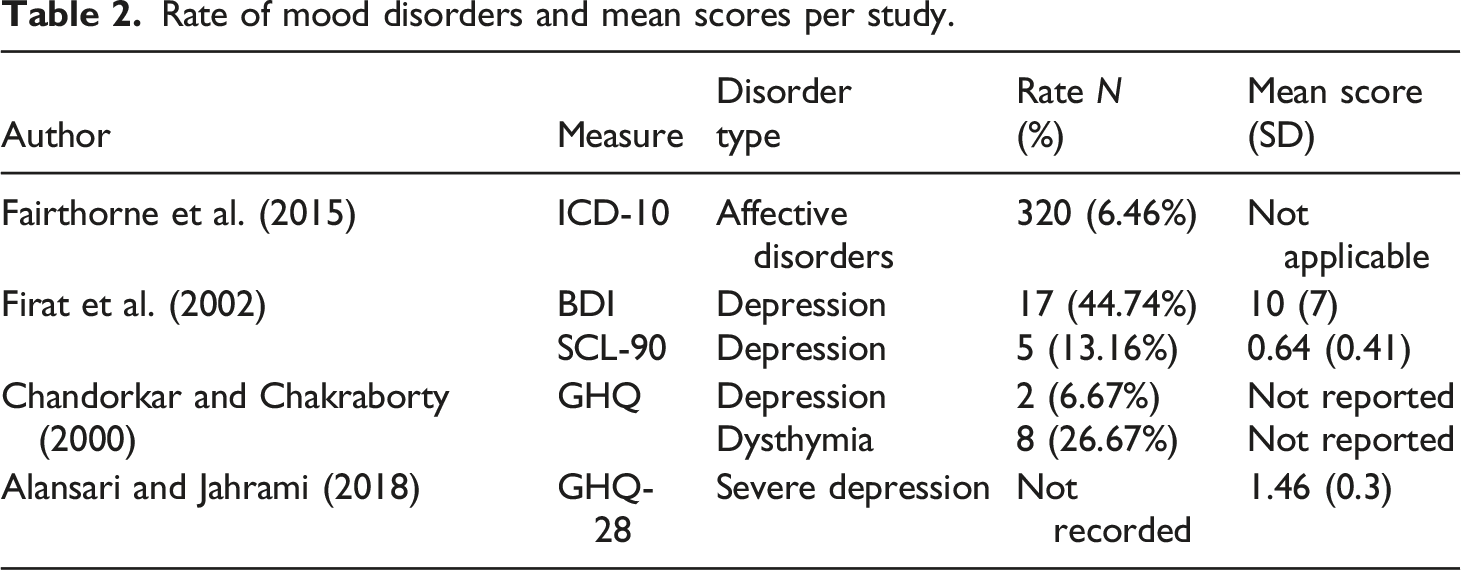
Rate of mood disorders and mean scores per study.
Mothers of individuals with LD of unknown cause were more likely to experience a mood disorder when LD severity was mild-moderate (IRR = 1.98, 95% CI [1.1, 2.8]) and severe (IRR = 5.12, 95% CI [1.4, 18.5]), than mothers of typically developing individuals (Fairthorne et al., 2015). However, when looking at specific diagnoses, this difference only appeared to be present in dysthymia (Chandorkar and Chakraborty, 2000).
Mothers of children with LD of unknown cause had higher rates of mood disorders than mothers of individuals with DS (2.77%), LD of known cause (5.67%) and no LD nor ASD (2.91%) (Fairthorne et al., 2015). When LD severity was taken into account, this remained true for mild-moderate LD but not severe LD of unknown cause, who had lower rates than the LD-of-known-cause group (Fairthorne et al., 2015).
Depression rate and severity were significantly lower than the rate and severity in parents of children with ASD as measured by the BDI (p = .04) and SCL-90 (p = .002) (Firat et al., 2002). AlAnsari and Jahrami (2018), however, found no significant difference in severity scores between mothers of individuals with LD of unknown cause, ASD (M = 1.4, SD = 0.3) and mothers of typically developing children (M = 0.86, SD = 0.19) (p = .27). Mothers had higher rates of both depression and dysthymia, with no fathers meeting criteria for depression and two meeting criteria for dysthymia (Chandorkar and Chakraborty, 2000).
Firat et al. (2002) identified that the majority of mothers who completed the BDI met criteria for mild depression (64.71%). However, the SCL-90 revealed were in the ‘normal’ range. This suggests that whilst depression may be present, symptom intensity may be low, Fairthorne et al. (2015) and AlAnsari and Jahrami (2018) investigated the presence of moderate and severe LD, which may explain difference in rate and severity.
Anxiety and fear-related disorders
Mothers of children with LD of unknown cause had higher rates and severity of anxiety and fear-related disorders than all comparative mothers, with the exception of mothers of individuals with ASD. Despite this, when anxiety was measured via the STAI and SCL-90, mean scores were below the cut off levels for presence of psychopathology.
Rate of anxiety and fear-related disorders and mean scores per study.
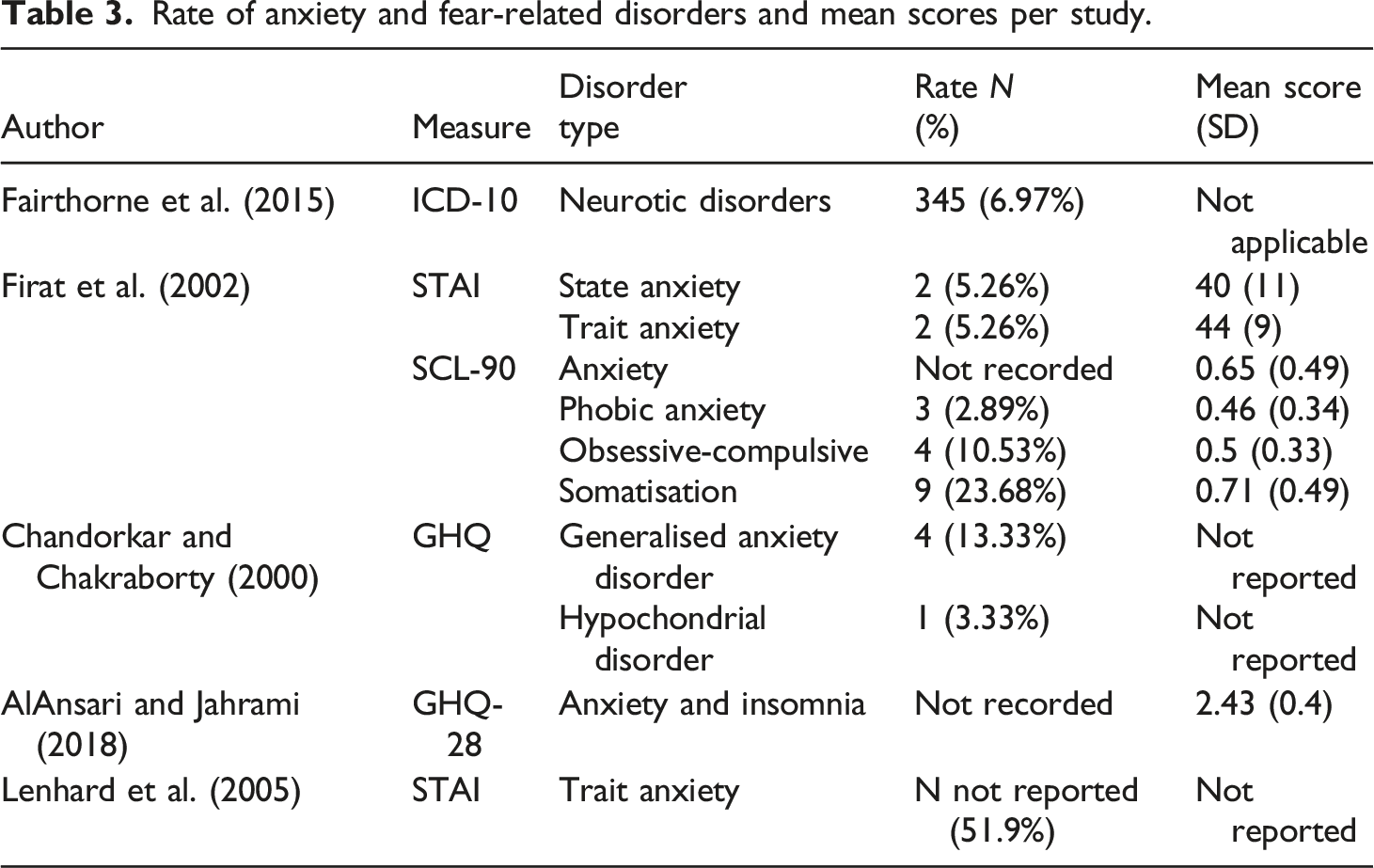
Mothers of children with LD of unknown cause were more likely to experience generalised anxiety disorder and neurotic disorders (mild-moderate: IRR = 1.8, 95% CI [1.3, 2.5]; severe: IRR = 1.98, 95% CI [0.6, 6.4]) and had higher severity of anxiety and insomnia than parents of typically developing children (Alansari and Jahrami, 2018; Chandorkar and Chakraborty, 2000; Fairthorne et al., 2015).
Mothers of children with LD of unknown cause had lower levels of anxiety and insomnia compared with mothers of children with ASD (M = 2.73, SD = 0.44) (AlAnsari and Jahrami, 2018) but higher levels than those with children with DS and LD of known cause (Fairthorne et al., 2015; Lenhard et al., 2005). This difference was present whether LD severity was mild-moderate or severe. Mothers of children with ASD also had higher severity levels of state anxiety (p < .05), trait anxiety, somatisation (p < .05), OCD (p < .01), anxiety (p < .05) and phobic anxiety (p < .001) (Firat et al., 2002).
Mothers appeared to have higher rates of anxiety and hypochondriasis than fathers (Chandorkar and Chakraborty, 2000); these were highest in mothers over 30, with multiple children and with children older than 3 years (Firat et al., 2002).
Other mental health difficulties and related symptoms
Rate of other mental health difficulties and related symptoms and mean scores per study.
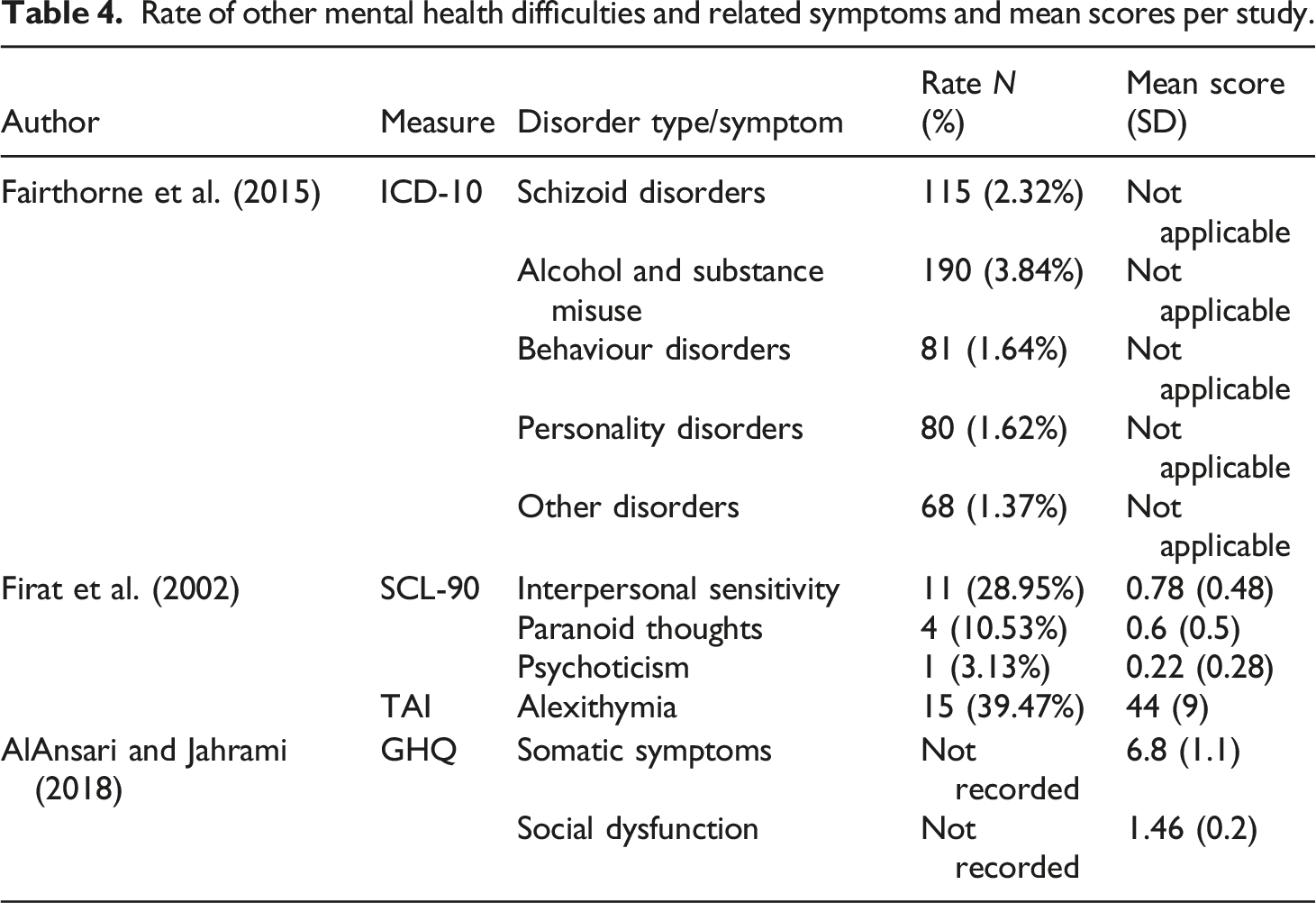
There was no statistically significant difference between mothers of children with LD of unknown cause and mothers of typically developing children (AlAnsari and Jahrami, 2018) or mothers of children with DS and LD of known cause (Fairthorne et al., 2015) on scales of somatic symptoms and social dysfunction, schizoid disorders, alcohol and substance misuse, behaviour disorders, personality disorder and ‘other’ disorders. When LD severity was taken into account, those with children with severe LD of unknown cause had lower levels of behavioural disorders (0.31%) than all other mothers (no LD: 0.7%; mild-moderate LD: 1.7%; DS: 1.3% and LD of known cause [not DS]: 1.1%) and lower levels of alcohol and substance misuse (2.5%) than mothers of children with LD of known cause (not DS) (3.3%) and mothers of children with mild-moderate LD (3.9%) (Fairthorne et al., 2015).
Mothers also had lower rates of interpersonal sensitivity (28.9% compared to 45%), paranoid thoughts (10.5% compared to 35%) and psychoticism (2.6% compared to 17.5%) (Firat et al., 2002) in addition to lower severity of somatic symptoms (mean score = 1.13 compared to 1.76) and social dysfunction (mean score = 1.06 compared to 1.6) (AlAnsari and Jaharami, 2018) than mothers of children with ASD.
General psychiatric morbidity
Rate of general psychiatric morbidity and mean scores per study.
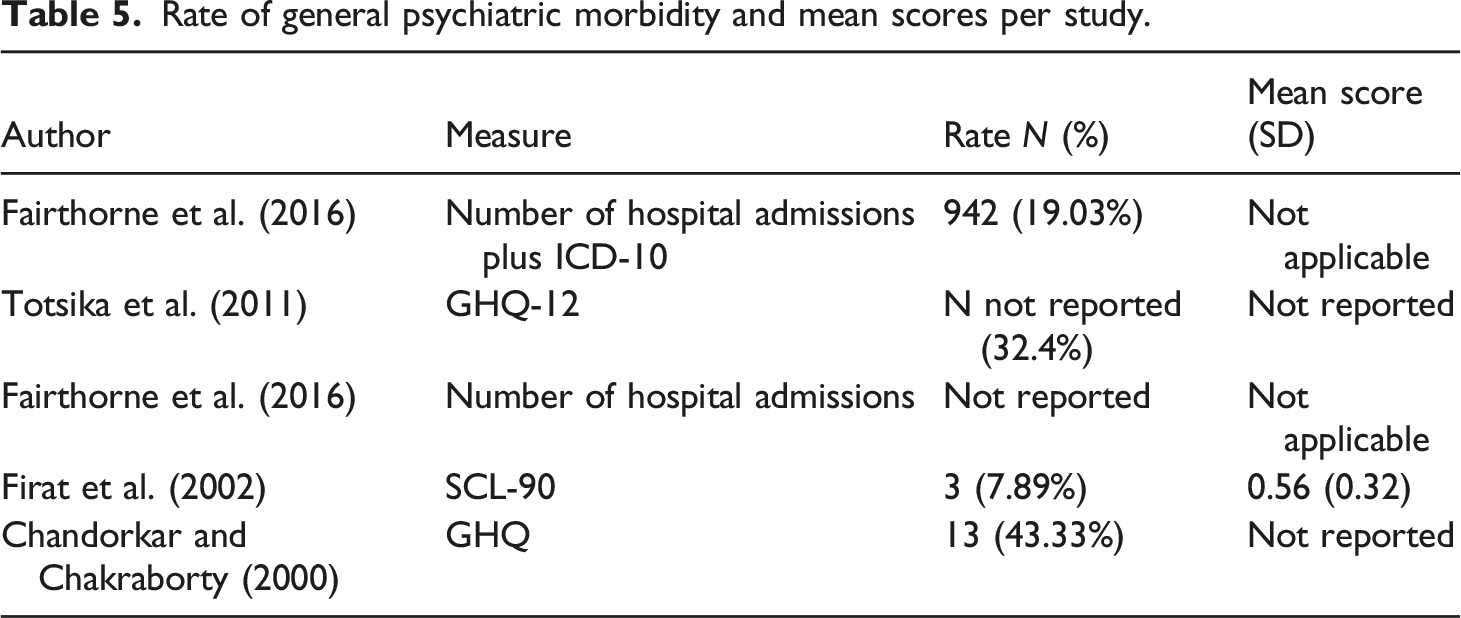
The rate of psychiatric morbidity in mothers of children with LD of unknown cause was lower than morbidity in mothers of children with ASD (p < .01) (Fairthorne et al., 2016; Firat et al., 2002; Totsika et al., 2011), but higher than the psychiatric morbidity of mothers of typically developing children (p < .05, Chandorkar and Chakraborty, 2000; p < .01, Totsika et al., 2011; p < .0005, Fairthorne et al., 2016) and fathers (Chandorkar and Chakraborty, 2000).
Mothers and fathers whose children with LD of unknown cause had no support had higher psychiatric morbidity than those with children in special education (p < .01). However, some parents with children in special education had more than four psychiatric symptoms, 2 years prior to the study. Two-thirds (seven fathers and five mothers) of these parents stated that their mental health improvement was attributed to their child making progress in school (Chandorkar and Chakraborty, 2000).
Mothers of children with LD of unknown cause had slightly more days in hospital than those of typically developing children (IRR = 1.07, 95% (CI) [1.05, 1.10], p < .0005). Hospitalisation rates were also higher than those for mothers of children with DS (IRR = 1.03, 95% CI [0.95, 1.11]) and ASD with (IRR = 0.99, 95% CI [0.94, 1.04]) and without LD (IRR = 1.05, 95% CI [0.97, 1.13]), although in all these cases the CI crosses 1.0 suggesting the true value could be 1 in which case the two groups are equal. Hospitalisation rates were lower than mothers of children with LD of known cause (IRR = 1.25, 95% CI [1.18, 1.32]). Group differences were significant and many of these IRRs are close to 1.0 suggesting limited impact but hospitalisation rates increased when the child’s LD severity was mild-moderate (IRR = 1.80, 95% CI [1.5, 2.2]) and decreased when level of LD was severe (IRR = 0.85, 95% CI [0.4, 1.9]).
In summary, psychiatric morbidity was higher in mothers of children with LD of unknown cause compared with mothers of typically developing children and fathers but lower compared with mothers of children with ASD. Hospitalisation rates are fairly similar to other parents of children with LD but do appear to be increased when also taking into account lower severity of LD.
Discussion
This review provided a necessary insight into the mental health of parents with children with LD. Results demonstrate that mothers of children with LD of unknown cause have higher rates and severity of mental health disorders than mothers of children with DS, LD of known cause and typically developing children, supporting prior research (Pinquart and Sorensen, 2003; Rydzewska et al., 2021).
One finding of note is that mothers of children with mild-moderate LD of unknown cause experience higher rates of admissions than other mothers, demonstrating the vulnerability of this population to severe mental health difficulties. Being unaware of the cause of the child’s LD may cause diagnostic uncertainty which could then lead to greater emotional burden in the parents (Lenhard et al., 2005). However, when the child’s LD was severe, hospitalisation rates of mothers were low. Based on other literature, it could be hypothesised that there is more support for both parents and children where the LD is more severe (Leonard et al., 2004) and these parents may also be more likely to seek support (Lenhard et al., 2005). Attending parenting support groups may increase the mothers’ social interaction and decrease feelings of isolation which could decrease risk of developing a mental health disorder (Kagey et al., 1981), but may not alleviate severe mental health difficulties when already present.
Fathers’ mental health was less negatively affected than mothers’. However, only one study included fathers and the number of fathers within this sample was not reported. Fathers reported a higher presence of symptoms before their child received support and therefore supporting the child may be an effective way to improve the mental health of fathers.
The results of this review could be explained by societal factors whereby mothers of children with LD tend to be less educated, have lower levels of employment (Firat et al., 2002), are more likely to be of low socioeconomic status and more likely to be younger than 20 at the birth of their child (Fairthorne et al., 2016). When adversity of mothers along with the child’s age, gender and behaviour was taken into account, the impact of having a child with LD of unknown cause on mental health was reduced (Totsika et al., 2011).
Strengths and limitations
The use of SWiM (Campbell et al., 2020) as an approach to synthesising research in addition to following PRISMA guidance (Page et al., 2020) led to an extensive and transparent review of the literature which was able to investigate the presence of diagnosable mental health difficulties in parents. This review included papers from a range of countries, accounting for cultural differences in the understanding of mental health. The majority of the included papers were rated moderate to strong in selection bias, confounders and data collection methods suggesting some validity and reliability in the results.
However, only two studies controlled for prior mental health difficulties by excluding mothers who met criteria for a diagnosis prior to the birth of their child. In addition, we cannot guarantee the absence of undiagnosed comorbidities in the offspring and therefore these are both potential confounds. The rates of parents with multiple diagnoses were unreported; therefore, it could be that few parents accounted for the rates of multiple disorders. For example, alcohol and substance misuse is commonly experienced alongside other mental health diagnoses (Weaver et al., 2003) and associated with increased admission (Hunt et al., 2002). It is also important to be mindful that the parents in the included studies were primarily assessed for psychiatric morbidity and were generally not assessed on the basis of other psychologically driven constructs such as attachment, family functioning, couple relationship quality and so on; the findings therefore reflect psychiatric categories and it would be useful for studies in this field (and ensuing reviews) to consider more psychological ways of understanding parenting challenges in this field.
It should also be noted that only one of the included studies included fathers and that more research is needed which includes or focuses on fathers. Within many families, the main carer is not the mother and thus this should be considered when interpreting and using findings which are mostly based on the mental health of mothers.
Implications and recommendations for future research
The findings of this review emphasise the need for mental health support for parents of children with LD, specifically where the child has LD with an unknown cause. In the United Kingdom, services such as Early Intervention in Psychosis, recognise supporting families as one of their core standards. As a result, these services regularly offer family intervention (National Institute for Health and Care Excellence, 2014) along with carers support and recognise a need for individual psycho-social support (Caqueo-Urízar and Gutiérrez-Maldonado, 2006). Review findings would support a call for LD services to adopt a similar model with the aim of improving parental health and thus have positive implications for the care people with LD receive in the community, reducing inappropriate admissions and helping to avoid abuse or neglect in community settings. This would support the Care Act 2014 (UK Government, 2014) within which one of the aims is to assess the carer’s needs for support and offer help if required.
Given the presence of mild depression and anxiety in parents, it may be that the full range of evidence-based psychological therapies could be offered to parents within the context of carers support. In the United Kingdom for new episodes, these could include individual or group Cognitive Behavioural Therapy, Behavioural Activation, Interpersonal Therapy and short-term psychodynamic psychotherapy (National Institute for Health and Care Excellence, 2022). However, given the importance of family dynamics highlighted in this review, family systemic therapy may be a more appropriate intervention. Although not recommended by UK guidelines for depression, McPherson and Oute (2021a, 2021b) argue that a critical gap has emerged between evidence and policy concerning family dynamics in the context of mental health and that several forms of literature ignored by guidelines point toward the importance of offering family-based interventions. Whilst this systematic review did not explicitly explore attachments between parents and their offspring, this may be a confounding factor influencing their mental health. Moreover, whilst this systematic review did not explicitly explore attachments between parents and their offspring, this may be a confounding factor influencing their mental health. Therefore, it may be recommended that parents receive interventions such as video feedback programmes, which support parents in understanding and responding to their child whilst also acknowledging their own emotions (National Institute for Health and Care Excellence, 2016).
Further research is required to explore factors that increase the vulnerability of parents (mothers and fathers) of individuals with LD as a method to identify the most at-risk families, for example, mothers with multiple children (Firat et al., 2002). Longitudinal research is also required to investigate the hypothesis that having a parent with mental health difficulties leads to increased admissions in individuals with LD.
In thinking about how we better support people with LD, it may also be useful for future research to consider wider systems including anyone that might be involved in their care (family or professional).
Conclusion
Parents of children with LD of unknown cause experience higher rates of mental health difficulties than parents of typically developing children and parents of children with other forms of LD, usually with the exception of ASD. Despite this, LD services in the United Kingdom do not currently offer psychological interventions to parents. It is proposed that future research is conducted which explores families most at risk of struggling with mental health difficulties and the type of support that may be beneficial to these families. It is also of relevance to explore whether in providing support to parents of individuals with LD, there are wider implications in relation to reduced number of admissions of people with LD into psychiatric hospitals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.