
Abstract
An outbreak of acute headache, weakness, breathing difficulty and gastrointestinal symptoms occurred among schoolchildren who went near the seashore of a coastal school in North Kerala, India. This article describes a field investigation conducted in response to this outbreak. The overall attack rate was 47% among schoolchildren on the seashore, with a higher rate of 76% among girls. The symptoms subsided uneventfully within 1 day. The investigation team suspected heat stress, mass hysteria or harmful algal blooms. Our team could not identify the cause of the outbreak even after extensive environmental investigations. We recommend training and capacity building for public health specialists in the district’s rapid response team on environmental epidemiological methods to promptly respond to future events.
Introduction
Many disease outbreaks have been reported in schools globally and in India.1–5 Schools may be more susceptible to infectious disease outbreaks, such as influenza and measles, owing to poor hygiene skills, student density, and mass hysteria events due to psychosocial stressors. Although every outbreak is investigated with the principles of controlling the outbreak and preventing similar future outbreaks, many investigations have failed to identify the actual cause of the outbreak. We report an outbreak of an illness among students at a coastal school, where extensive epidemiological investigations failed to identify the cause of the outbreak.
The Outbreak
The district Integrated Disease Surveillance Programme (IDSP) control room was alerted on 18 July 2022, 12 noon as students who went to the seashore were brought to a nearby government hospital with various symptoms. The event occurred in the morning hours of 18 July 2022 when the students were taken to the seashore, approximately 120 m from the school for counselling and playing. The counselling session started at 11.30
Outbreak Investigation
The clustering of cases confirmed the outbreak, and the district rapid response team (RRT) investigated the outbreak on the same day. The district RRT visited and interviewed the affected students and the treating team to identify the symptoms and develop a case definition. A case was defined as the presence of any new symptom that started on 18 July 2022 morning in any student/teacher/staff at that coastal school. The RRT conducted an active case search using a structured questionnaire among students, teachers, and office staff present on that day in the school. The team also interviewed people living near the school on the coastal side to identify any specific symptoms.
Environmental Investigation
The RRT conducted a detailed visual inspection across the seashore area and inquired about any common sources of food or water and chemical or gaseous exposure. The team also visited shops near the school and inquired about the consumption of any common food item by the students. The team also collected food and water samples from the school and nearby shops and handed them to the Food Safety Department for chemical and bacteriological testing. Seawater samples were also collected and sent for testing 3 days later with the help of a local NGO involved in environmental protection activities.
Investigation Findings
The school counsellor took female students of grades 5, 6, and 7 for a “menstrual hygiene” session at approximately 11.15
Location of Students with Symptoms on the Day of the Event.
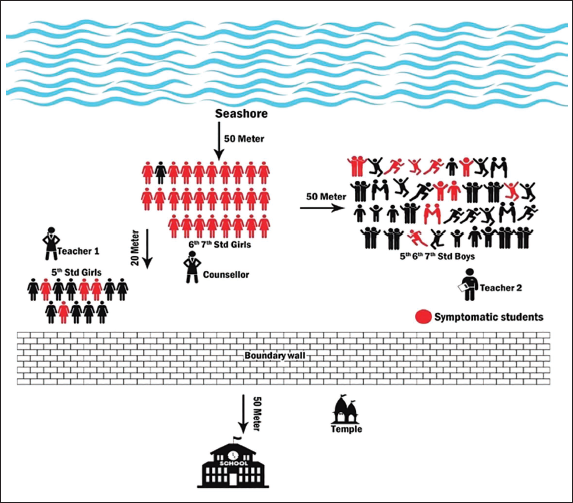
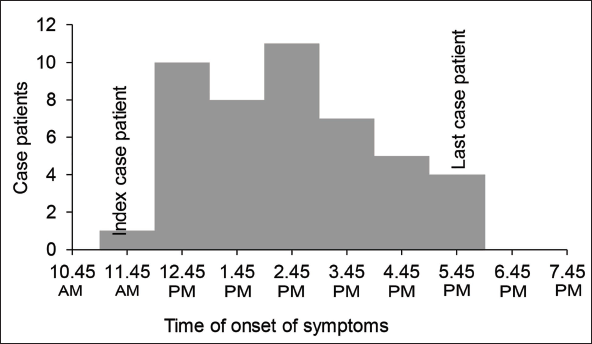
The index case was reported at 11.45
Distribution of Cases by Time of Onset of Symptoms on the Day of Event (18 July 2022; N = 46).
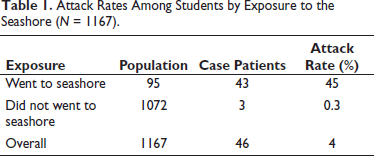
During the day of the event, 1167 persons were present in the school, including students, teachers, and office staff. Forty-three students who went to the seashore and 3 students who did not go to the seashore showed symptoms. Thirty-seven (80%) case patients who visited the seashore reported an uncharacterized sea smell on the day of the event. None of the local residents or teachers interviewed reported any particular new symptoms arising that morning. Table 1 shows the attack rate among school students by exposure to the seashore.
Attack Rates Among Students by Exposure to the Seashore (N = 1167).
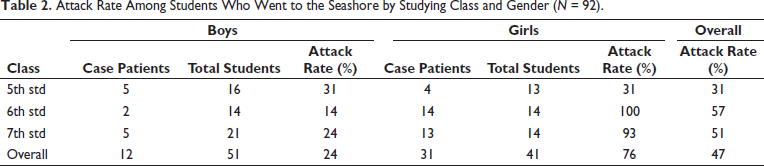
The attack rate was highest among the 6th (100%) and 7th (93%) standard girls. Table 2 shows the attack rate by study grade and gender among students who visited the seashore.
Attack Rate Among Students Who Went to the Seashore by Studying Class and Gender (N = 92).
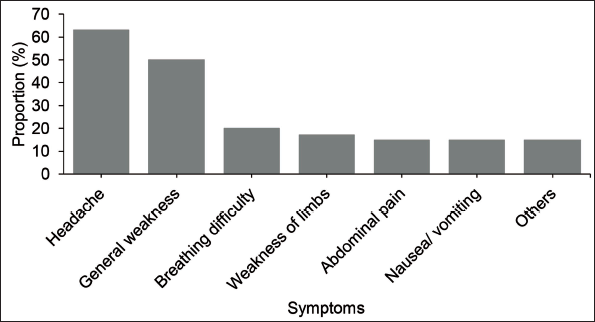
Headache was the most common symptom experienced by the case patients 28 (61%), followed by general weakness 21 (46%). Figure 3 shows the symptoms experienced by the case patients.
Symptoms Experienced by Case Patients on the Day of Event (N = 46).
Among the 46 symptomatic individuals, 42 (91.3%) were admitted to the two hospitals for observation. The mean age (SD) was 11 (1.8) years. 33 (72%) were female. On examination, all the children were clinically stable. None of the patients complained of extreme heat or prostration, and none of them were severely dehydrated. However, due to panic, they were admitted for observation, the treating team gave symptomatic medications, and all the students were discharged the following day uneventfully.
Environmental Investigation Findings
The RRT conducted a thorough environmental search by visual inspection across the seashore area, and found no visible chemicals, pesticides, decaying animal carcasses or insects. On discussing with the teachers, other students, and people living near the school, the team got a mixed response about having and not having an abnormal smell in the preceding 4-5 hours. The team was also informed that the morning was cool, and that no extreme heat was present on the day. The case-patients did not report any insect or crab bite on that day. The teachers and local people informed the team about some smell coming from the sea every year, and the teachers and students were accustomed to that. As per the locals, “the sea smell is due to the sea dumping some waste products out of it every year.” The team inquired with the students and teachers about any common source of food, visited the food preparation area of the school and local shops nearby, and found nothing unusual. As the students had not taken any food from school until the onset of the illness and the previous 2 days were school holidays, the team concluded that no common food or water source was associated with the illness. The food and water samples collected from the school and shops for testing were negative for hazardous chemicals or pathogens. The seawater tested contained dinoflagellates at a normal rate. None of the other visitors to the seashore experienced similar symptoms that day or a week afterwards, and similar symptoms were not reported elsewhere along the coastal margins of the district.
Preventive Measures Undertaken
In collaboration with the school administration, educators, and parents, we organized a meeting to advise them to report any future episodes of similar illnesses to our surveillance unit. During the meeting, we also emphasized the importance of refraining from taking students to the beach for extended periods, particularly during the summer, and cautioned them about any changes in colour or odor in the water. Furthermore, counselling services were arranged to support the students during their illness and thereafter.
Discussion
After ruling out food and water contamination, the investigation team considered extreme heat stress as the cause of the outbreak, which was ruled out by interview findings and clinical symptoms. Then, the team considered the possibility of a mass hysteria outbreak triggered by an unknown event. Several outbreaks of mass hysteria have been reported globally in schoolchildren.3, 6 The sudden clinical improvement in symptoms, preponderance in girls, and failure of an extensive epidemiological investigation to detect an organic cause point to mass hysteria. 5 However, the time duration of six hours between the index case and the last case patient was atypical for mass hysteria. During the discussion, another differential diagnosis of harmful algal blooms (HABs) emerged. Since the symptoms were experienced by students who visited the seashore on that particular day and with the teachers and locals experiencing “some” abnormal smell, environmental causes other than contamination became a primary suspect in this case. A person can be exposed to the algal toxins by eating shellfish or fish containing toxins, swimming or other activities in the water or breathing in tiny droplets in the air that contain toxins. 7 Previously shellfish poisoning due to toxins was reported from many parts of South India including Kumbla region of Kasaragod adjacent to Mangalore. 8 The symptoms of nausea, vomiting, headache, numbness of mouth and extremities can be associated with inhalation of marine aerosols of harmful algal blooms during active bloom of Karenia brevis and Ostreopsis species. 9 In 2004 in South Kerala, over 200 children, mostly under 15 years, complained of nausea, chest pain, and short periods of breathlessness after a strong odor and many were hospitalized and later identified to be due to the bloom of Helladosphaera spp. 10 Similar other episodes have been reported from the coast of Kerala of dinoflagellate proliferations of Karenia mikimotoi, Gonyaulax diegensis and Noctiluca scintillans marked by water discoloration, fish deaths and clinical symptoms among exposed people. 11 Many such events have affected young children who experienced a foul smell followed by nausea, vomiting, breathlessness or weakness.12–14 Although dinoflagellates were identified in the water in this outbreak, no evidence of algal bloom was detected. Unfortunately, no samples from other environmental matrices were collected for analysis.
Although the district IDSP team responded promptly to the outbreak, we were unable to identify its cause. The RRT had no service from an environmental health specialist to investigate any other emerging environmental hazard potential that could cause such outbreaks. Unfortunately, existing epidemiologists are not well trained in environmental health and investigating outbreaks due to emerging environmental hazards other than potential microbiological contamination, which may have led to a delay in sample collection and investigations relating to an ecological etiology.
The eyes do not see what the mind does not know. To deal with emerging environment-related health hazards, we need a trained workforce in environmental health/epidemiology. In addition, standard operating procedures for investigating environment-related acute health emergencies must be developed. With the impending climate crisis, we will face many environment-related health emergencies, and a trained environmental epidemiologist in the district’s RRT is the need of the hour.
Footnotes
Authors’ Contribution
RSV: Conceptualization, methodology, investigation, formal analysis, data curation, writing-original draft preparation.
AEA: Investigation, formal analysis, data curation.
MK: Conceptualization, methodology, writing- reviewing and editing.
MM: Conceptualization, methodology, writing- reviewing and editing, supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The investigation was a public health response to an outbreak, undertaken to identify the source of spread for immediate control of the outbreak, and intended to benefit the community at large hence ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent was obtained from study participants.