
Abstract
Idiopathic intracranial hypertension (IIH) conventionally presents with features like headache, visual obscuration, diplopia and tinnitus. We present a case of a middle-aged male patient with headache and visual complaints and concurrent drug-resistant right focal seizures. Imaging revealed the presence of a left petrous bone defect with temporal lobe encephalocele with other features suggestive of IIH. Resolution of the symptoms was obtained after placement of theco-peritoneal shunt. Focal seizures in IIH are a rare phenomenon, precipitated by parenchymal herniation through eroded bony defects producing encephaloceles leading to tissue traction and ictal focus formation. In evaluation for drug-resistant temporal lobe epilepsy, IIH-induced encephalocele formation should be carefully considered.
Keywords
Introduction
Idiopathic intracranial hypertension (IIH) is characterised by elevated intracranial pressure (ICP) without any identifiable brain pathology and with normal cerebrospinal fluid (CSF) composition. 1 The key features comprise of diffuse headache, transient visual obscuration, diplopia, pulsatile tinnitus and defined by the revised diagnostic criteria of IIH. 2 Seizure as a component and major manifestation of IIH is a rare entity found in around 0.9/100,000. 1 Here we describe a case of IIH with recurrent intractable focal seizures with subsequent improvement with CSF diversion.
Case Presentation
A 35-year-old right-handed non-obese gentleman, a goldsmith by occupation, without any significant drug history, presented with six months history of progressive worsening of holo cranial headache with initial episodes of transient visual obscuration. One month after onset of headache he started having episodes of focal seizures with sudden tonic posturing of right upper and lower limb with tonic-clonic movement and secondary generalisation with impaired awareness, associated with early head turning to left, lasting for one to two minutes followed by post ictal drowsiness for 5–10 minutes. There was no reported aura preceding the events. The episodes recurred discretely around five to six times per day without any residual neurodeficit, requiring titration of upto five antiepileptics (AED) for the seizure control. Initially, he was treated with a levetiracetam loading dose of 2 gm followed by maintenance dose of 1 gm twice daily and oxcarbazepine 450 mg twice daily. Seizures prevailed in spite of treatment and phenytoin 100 mg thrice daily, clobazam 10 mg once daily and perampanel 4 mg twice daily were sequentially added to control the seizures. Magnetic resonance imaging (MRI) and cerebrospinal fluid (CSF) study was normal. Serum autoimmune markers and autoimmune encephalitis panel were negative. Over the next two to three months patient started having tunnelling of vision and during presentation had a residual visual acuity of around 6/36 in both eyes with peripheral field restriction. No other neurological or systemic symptoms were present.
On examination visual acuity was 6/36 that improved transiently up to 6/12 on therapeutic CSF drainage. Fundoscopy revealed grade 4 papilledema with bilateral peripapillary flame-shaped haemorrhages. Automated perimetry showed severe field restrictions in all quadrants and enlargement of blind spots. CSF opening pressure was 70 cm H2O with biochemical parameters and closing pressure was kept at 14 cm H2O after therapeutic drainage. Routine haematological and biochemical parameters were normal. Interictal electroencephalogram (EEG) recording was non contributory.
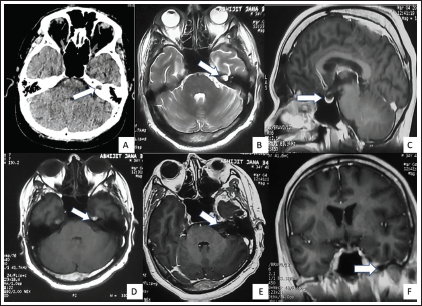
On imaging study, non-contrast computed tomography (NCCT) showed a small left petrous bone defect. Repeat MRI brain showed presence of temporal lobe encephalocele protruding along the eroded defect in the left petrous bone along with mild CSF space dilatation along the left anterior temporal pole. Partially empty sella and absence of any parenchymal or meningeal pathology led to the diagnosis of IIH (Figure 1) MR venogram showed hypoplastic left transverse sinus. Persistent IIH was believed to have caused the bony erosion leading to temporal lobe encephalocele and refractory focal seizures. Patient underwent theco-peritoneal shunt placement at L3 vertebral level followed by resolution of headache, improvement of visual acuity to 6/12 in both eyes with gradual resolution of papilledema and reduced seizure frequency and on one month follow-up required only one AED for maintenance.
(A) Non-contrast computed tomography (NCCT) brain showing bony erosion of the petrous part of left temporal bone (arrow). 3 Tesla Magnetic resonance imaging (MRI) brain (B) T2 weighted axial image showing dilatation of the cerebrospinal fluid (CSF) space in the left petrous apex representing petrous apex encephalocele. (C) Sagittal image showing partially empty sella (D) T1 weighted axial section showing left petrous bone defect with encephalocele intensity similar to CSF and (E) T1 contrast image showing no enhancement of the corresponding part (F) Sagittal T1 contrast image showing dilated CSF space in left anterior temporal region (arrow) with prominence of bilateral Meckel’s cave.
Discussion
Recent literature has shown a propensity for seizure occurrence in IIH. Pulsatile CSF forces are hypothesized to form prominent arachnoid villi, which form minor CSF reservoirs, resulting formation of spontaneous CSF fistulas and encephaloceles. 3 Because of their abnormal location outside the dural venous sinuses, CSF is not properly returned to the venous system, which may facilitate herniation of dura or brain tissue through the path of least resistance.
Temporal lobe meningoencephaloceles are increasingly recognized cause of drug-resistant epilepsy occurring in around 5% of temporal lobe epilepsy population. 4 Tissue traction with neocortical irritation, gliosis and rarely associated dysplasia are possible mechanisms for seizures. 1 In a study by Urbach et al., 22 patients of anterior temporal lobe meningoencephaloceles underwent evaluation for imaging parameters of IIH as well as intracranial CSF volumetric assessment.10 patients had MRI features of IIH and risk factor of obesity and responded to anterior temporal lobectomy. 4 In another study by Martinez-Poles et al., among 29 patients with temporal pole encephaloceles the pituitary gland height was lower and optic nerve sheath diameters were significantly larger than control group of other focal epilepsy patients, but the study group lacked overt clinical signs of IIH. 5 Correia et al. described a patient of Lennox-Gastaut syndrome with raised ICP detected at seven years of age followed by resolution on lumbo-peritoneal shunting. 6 Graece et al., in their study, among 103 patients of temporal encephaloceles IIH like headaches were more common than peri ictal or no headache. 7 Thottiyil et al. reported a case of non-obese young female with temporal lobe encephalocele with features of IIH. 1
Our patient presented with IIH-like headache and drug refractory focal seizures and progressive visual loss with MRI features suggestive of IIH and concurrent presence of temporal pole encephalocele corroborated with the prior literature as the cause of seizures. Improvement of all parameters in terms of headache, visual blurring and seizure episodes reduced with theco-peritoneal shunting.
Conclusion
IIH can present with non-conventional manifestations like seizures that require careful imaging and electroencephalographic evaluation for detection of the focus of encephalocele. Subsequent interventional treatment of IIH usually leads to seizure freedom. Further studies in this regard are required to establish a stronger association between the two entities.
Declaration of conflict of interest: The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Author Contribution
Both authors contributed equally towards the manuscript.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was in accordance with the ethical standards of institutional ethical review committee and with the 1964 Helsinki Declaration and its later amendmentsor comparable ethical standards. As this is a case report with observational study, seperate ethical approval was not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed written consent was obtained from the patient.