
Abstract
This study explores the nature of critical police incidents involving People with Mental Illness (PMI) that result in fatalities. The current study draws from Routine Activity Theory (RAT) to identify key characteristics of the PMI, officer, and place. The study examined all fatal police interactions involving PMIs in Queensland, Australia, over a 13-year period. A total of 32 cases were analysed to examine differences between two main groups: self-directed crises and externally directed crises. The results revealed both commonalities and key differences between the two groups. These findings are discussed within the context of controllers and super controllers, identifying key interventions of Crisis Supporters for PMIs, Response Aides for officers, and Environmental Facilitators for the location, as well as super controllers in terms of Support Frameworks. These findings provide insights for developing practical prevention strategies that can be implemented by police agencies, mental health services, and policymakers to reduce fatal outcomes in police–PMI interactions.
Introduction
Police interactions with People with Mental Illness (PMI) present a complex and often high-risk dynamic that can lead to tragic outcomes such as fatalities. In some cases, officers may simply be the first to arrive on the scene, with the fatality resulting from factors unrelated to any direct or intentional police actions, such as a drug overdose or suicide attempt (Bowler et al., 2022). Understanding the nuanced nature of these encounters is critical for developing strategies that better support both PMI and police to minimise risk and enhance safety for all parties involved.
Responding to PMI comprises a significant portion of police workload, which could be up to 30% of a general duty officer's day (Crissman, 2019; Lorey & Fegert, 2021; Morgan, 2021) and is also rapidly increasing by approximately 10% every year (NSW Government, 2024). PMI are disproportionately involved in fatal outcomes, including police shootings (Australian Institute of Criminology [AIC], 2020; Crissman, 2019; Morgan, 2021). Indeed, 42% of those shot by police in Australia in 2013 were PMI (AIC, 2020). These fatalities have devastating and far-reaching consequences, often leading to strained police–community relations and a lack of trust in police (Velazquez & Hernandez, 2019). The impact on police officers can be profound, with approximately two-thirds of officers involved in these fatalities developing posttraumatic stress disorder symptoms, alongside significant legal and financial burdens on government bodies tasked with investigating these tragedies (Baker & Pillinger, 2019; Velazquez & Hernandez, 2019).
Family members are often present during these situations—indeed, family members are often the ones who initially contacted the police for help (Frankham, 2018). However, they are often not given an opportunity to aid officers in the de-escalation process during police–PMI interactions (Baker & Pillinger, 2019). Given that approximately 35%–75% of those with serious mental illness live with relatives (Chronister et al., 2021), families often serve as primary caregivers, managing psychiatric distress, self-care, access to services, and financial support. However, despite their critical role, families are often left uninformed about their loved one's condition and lack the necessary guidance on how to provide effective support, leading to burnout and a feeling of helplessness (Aass et al., 2021).
Despite this, fatal police encounters involving PMI are a relatively under-researched phenomenon, with most of the body of knowledge established from U.S. populations. Moreover, existing research tends to concentrate on police shootings of PMI, often overlooking the wider spectrum of fatalities outside of shootings. Additionally, many studies lack a comprehensive theoretical framework to fully grasp the complexities of these incidents and to guide the development of effective prevention strategies. The current study expands on previous literature to address these gaps by exploring police interactions with PMI in an Australian context. It takes a holistic approach to examine encounters that not only result in police shootings but also other fatal outcomes that may not be the direct results of intentional police actions. Furthermore, the study uses an environmental criminology framework to understand the nature of these incidents and identify tailored prevention strategies.
Literature review
Police encounter individuals with a wide range of mental health conditions. While psychotic disorders are most common in fatal police interactions (Saleh et al., 2018), mood disorders also account for a significant portion of PMI cases (Crissman, 2019). The presence of comorbid conditions such as substance abuse further complicates these encounters, with nearly half of all PMI also struggling with substance use disorders (AIC, 2020; Crissman, 2019).
PMI in fatal police interactions are most often males, middle-aged, and over half have a criminal record (Crissman, 2019; Saleh et al., 2018). This is particularly concerning given that these are the same demographics of people who are also more likely to avoid professional help. A study by the Australian Institute of Family Studies (2020) found that 75% of adult men would not seek help from a mental health practitioner, even when exhibiting symptoms of mental illness. Moreover, while over 80% of individuals who experienced symptoms of suicidality, depression, or anxiety in the past year consulted a general practitioner, only 40% received specialised mental health care. This lack of timely intervention is problematic, as the longer individuals go without professional support, the greater their likelihood of encountering police and the risk of violent first-attempt suicides (Crissman, 2019; Tang et al., 2021).
Fatal police interactions with PMIs often occur in high-risk environments and involve the presence of weapons. Studies find that over half of these incidents take place within a dwelling, with 52% of fatal interactions occurring inside homes (Crissman, 2019; Saleh et al., 2018; Thomas, 2020). Over two-thirds of these encounters involve the PMI possessing a weapon (Crissman, 2019; Saleh et al., 2018). In the United States, offenders with mental illness used firearms in over half of fatal police encounters (Saleh et al., 2018). Conversely, knives are the most common weapon used by offenders with mental illness in Australia (Crissman, 2019). This difference in weapon use is mostly due to the strict firearm laws in Australia that restrict accessibility (Crissman, 2019). These incidents often involve the PMI threatening or using weapons against officers, others, or themselves, underscoring the high-risk nature of these encounters and the critical need for effective de-escalation strategies (AIC, 2020; Crissman, 2019).
For officers responding to these critical incidents, the situation can be unpredictable and complex, requiring a careful balance between ensuring public safety and appropriately addressing the needs of the individual in crisis. PMI can display behaviours that are erratic and impulsive, often not producing external threat or harm to others. However, for officers who are not adequately trained in mental health crisis, these behaviours may be misconstrued as a threat to safety, needlessly heightening incidents to conflicts (Crissman, 2019; Freeze & Campbell, 2024).
Perhaps not surprising given the male-dominated field, male officers are typically the ones involved in these high-risk situations. Miles-Johnson and Fay (2023) suggest that this overrepresentation of male officers in risky incidents stems from workplace cultures that define such tasks as “men's work”, while their female counterparts are often assigned to lower-risk roles, such as community policing. Male officers also tend to resort to force methods more quickly, while female officers are more likely to use de-escalation techniques (White et al., 2021). Female officers have also been found to be more effective in responding to sensitive crimes involving vulnerable people (Davenport-Klunder & Hine, 2023).
Police versus mental health responses
There has been a recent shift in public sentiment towards moving away from a policing response model and to a mental health-based response model in situations involving PMI, fuelled by growing concerns over problematic police responses (Clifford, 2010; Saligari & Evans, 2016). However, critics argue that these situations are often dangerous and volatile, and alternative services, such as mental health providers, may not be adequately equipped to manage the inherent risks (Illinois Criminal Justice Information Authority, 2022). A key concern is that removing police from these responses could weaken social control and jeopardise public safety. Others suggest that instead of defunding the police, officers should be held to a higher standard, ensuring they are better trained and prepared to handle mental health crises effectively (Ebbinghaus et al., 2024).
Another alternative—interagency collaboration—is often proposed as a solution, but it too presents its own unique challenges due to differing perspectives and competing goals between police and mental health services (Herrington & Pope, 2014). To address these issues, Herrington and Pope (2014) suggest training of police by mental health experts—Critical Incident Teams (CIT)—to improve officers’ understanding of mental health, de-escalation techniques, and communication with mental health practitioners. Studies have shown its effectiveness, with findings showing that CIT-trained officers are more likely to spend additional time with a PMI, using learned de-escalation techniques to produce safer outcomes for both the officer and PMI (Herrington & Pope, 2014; Rohrer, 2021). However, CIT faces barriers, including inconsistent training standards and voluntary participation (Crissman, 2019; Rohrer, 2021). These findings highlight the need for broader intervention strategies to support officers and prevent fatal outcomes, rather than placing the entire responsibility on general duty officers (Clifford, 2010).
Finally, the co-responder team model has emerged as an effective approach to ensuring the safety and care of a PMI during police interactions (Puntis et al., 2018). This model pairs a police officer with a mental health practitioner during patrol and has shown positive results, significantly reducing adverse outcomes for PMIs, with less than 1% of the recorded incidents resulting in arrests or other negative outcomes (Rohrer, 2021). These findings represent substantial benefits when compared to other specialised responses such as CIT, which has struggled to find meaningful results in reducing arrests (Rohrer, 2021).
Building on the success of the co-responder model, it is crucial to consider the roles of other individuals such as family/friends/care providers who may assist in managing mental health crises effectively. For example, Frankham (2018) found that 41% of emergency PMI calls come from family/friends who likely possess extensive knowledge about the individual's mental health condition, care status, and effective approaches for interaction. However, Freeze and Campbell (2024) found that officers often disregard this information, doubting its credibility and relevance. These findings highlight the need for more structured and theory-based approaches such as Routine Activity Theory (RAT) to identify and integrate key individuals who can contribute to better outcomes and minimise fatalities.
Routine Activity Theory
RAT—particularly the crime triangle—can offer valuable insights into understanding fatal police interactions with PMI (Cohen & Felson, 1979; Eck, 2003; Felson & Boba, 2010). Moreover, it can help to identify potential “actors” who can intervene and prevent these situations. The theory purports that crime occurs when three elements converge in space and time (Cohen & Felson, 1979). At the core, the triangle consists of the motivated offender, suitable target, and suitable location (Cohen & Felson, 1979). Surrounding them are controllers: handlers (who influence the offender), guardians (who protect the target), and place managers (who oversee the location) (Eck, 2003). Beyond these direct controllers, Eck (2003) introduced “super controllers” who influence the controllers themselves. Super controllers can be regulatory bodies, community groups, policy makers, or larger societal forces that can shape how “handlers”, “guardians”, and “place managers” perform their roles.
In the context of police–PMI interactions, it is important to recognise both the officer and the PMI can alternate between the role of “offender” and “target” depending on the situation—indeed, in some cases such as an accident, there may not even be an offender or target (Crissman, 2019; Saleh et al., 2018). What is important is that in all encounters both parties—PMI and police—are influenced by actors such as family members, mental health professionals, or police supervisors, who can intervene to de-escalate either the officer's actions or the PMI's behaviour (Crissman, 2019; Frankham, 2018). The crisis triangle depicted in Figure 1 captures these complexities and nuances.
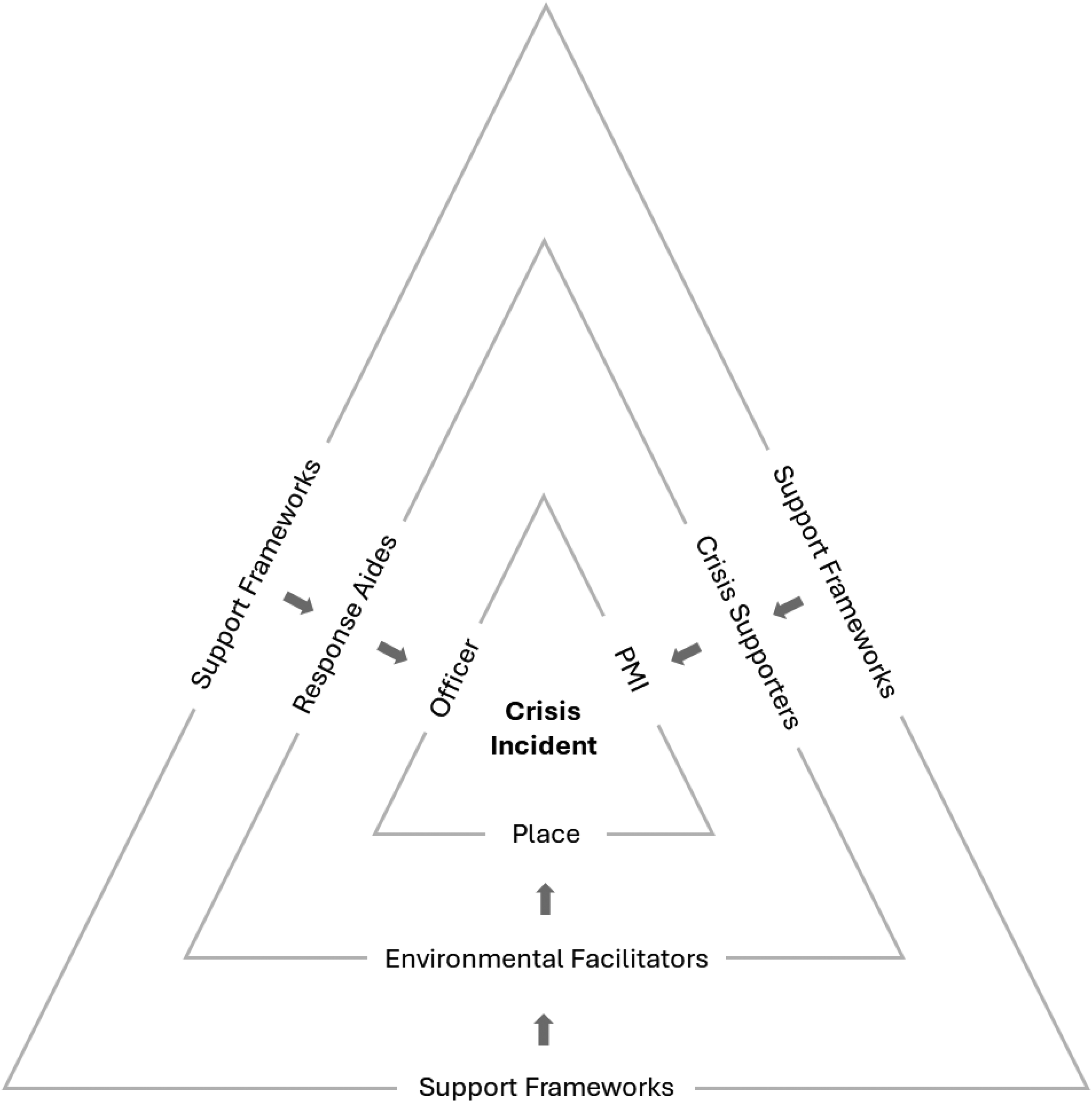
The crisis triangle.
In the crisis triangle, the inner elements consist of the PMI, the officer, and the place where the interaction occurs. Surrounding this core are the actors who can intervene and provide essential support in de-escalating the crisis. This middle triangle introduces the “Crisis Supporters” for the PMI, who are best positioned to influence or manage the person in crisis. For the officer, “Response Aides” can guide and support the officer in responding effectively to the situation. Finally, the “Environmental Facilitators” oversee and manage the place where the crisis occurs. The “Support Frameworks” form the outer triangle to provide oversight, resources, or regulations.
The use of RAT in examining police–PMI interactions provides a clear and accessible framework that not only helps to understand the nature of these encounters but also identifies potential interventions (Eck, 2003). By focusing on the roles of Response Aides, Crisis Supporters, and Environmental Facilitators, this approach enables the identification of practical strategies to prevent escalation and improve safety outcomes (Felson & Boba, 2010). It is relatively quick and easy for policymakers, police, and mental health professionals to apply, avoiding the complexities of psychological factors and instead concentrating on external controls and situational dynamics (Cohen & Felson, 1979). This makes it an effective tool for guiding policy decisions and implementing reforms aimed at reducing fatal outcomes in police–PMI interactions.
Aims
This study aims to understand the nature of critical police incidents with PMI that result in the death of the PMI. Specifically, it aims to understand the officers, PMIs and circumstances involved in such events in order to uncover potential actors and support frameworks that may be available to intervene and help prevent such fatalities from occurring. The findings from this study will help to inform policing authorities and support services to specifically tailor approaches to preventing such incidents.
Methods
To identify the RAT characteristics of police interactions with PMI resulting in the death of the PMI, a quantitative descriptive analysis of coroners reports was conducted. Specifically, the analysis examined the profiles of the police officers, PMI, and locations involved in fatal interactions in Queensland (Australia) that resulted in the death of the PMI.
The Australian context
To contextualise this study, it is important to understand the structure of policing in Australia. There are only eight policing jurisdictions in Australia, reflecting each of the seven main states and territories 1 and the Australian Federal Police (AFP). The AFP enforces Commonwealth laws and manages national security, terrorism, and cross-jurisdictional crime, while the state and territory police services enforce local laws within their respective jurisdictions. While there are some jurisdictional differences, there is considerable consistency across states and territories in terms of police training, performance measurement, and operational policies (Hine et al., 2020; Hine & Carey, 2020; Hine & Davenport-Klunder, 2022).
More specifically, Queensland is one of the three largest policing jurisdictions in Australia, ranked by the number of sworn officers, population size, and geographic area. Queensland has approximately 12,000 police officers (Queensland Audit Office, 2023) who are responsible for policing a population of over 5.6 million people (Queensland Government Statistician's Office, n.d.) spread across an area of more than 1.7 million square kilometres 2 (Geoscience Australia, n.d.), encompassing major cities, regional centres, rural towns, and remote Indigenous communities. Given the size and representativeness, these characteristics make Queensland a suitable setting for examining police interactions with PMI.
To provide context for understanding police-involved fatalities with PMI in Australia, it is useful to consider both national trends and international comparisons. In Australia, such incidents are relatively infrequent when compared to jurisdictions like the United States. Data from the AIC show that between 2010–2011 and 2022–2023, there was an average of 23 deaths per year in police custody or custody-related operations, with annual totals ranging from as low as 16 to as high as 40 (McAlister et al., 2023). These figures include a broad range of fatal incidents ranging from natural causes to shootings. Australian figures are far lower than in the United States, where 1,175 people were fatally shot by police in 2024 alone, including 174 cases involving individuals in a mental health crisis (The Washington Post, n.d.). In contrast, Australia's numbers align more closely with those from England and Wales, where 23 people died in or following police custody in 2022–2023, with 13 of those individuals having identified mental health conditions, including psychosis, depression, anxiety, and posttraumatic stress disorder (Independent Office for Police Conduct, 2023). Earlier research from the AIC focusing specifically on fatal police shootings in Australia found that 42% of the 105 individuals fatally shot by police between 1989–1990 and 2010–2011 had a diagnosed mental illness, most commonly psychotic disorders such as schizophrenia (AIC, 2013). Overall, while fatal police encounters with PMI are relatively rare in Australia compared to countries like the United States, national data still reveal a consistent overrepresentation of individuals with mental illness.
Data source
To provide a comprehensive understanding, data were extracted from all publicly available coroner's reports relating to deaths of PMIs during incidents involving police–PMI interactions within the study period in Queensland, Australia. In Australia, the coronial system is characterised by centralised oversight, legally trained coroners, and accessible reporting. This differs from other countries like the United States, which has more of a decentralised and varied system, which sometimes presents challenges in consistency, oversight, and public accessibility. For example, in Australia, each state and territory operates its own coronial system under specific legislation as a division of the courts (e.g., Coroners Act 2003 in Queensland). Coroners are typically legally trained and qualified magistrates with formal, independent judicial roles who investigate reportable deaths, including those that are unexpected, unnatural, or occur in custody (National Coronial Information System, n.d.). Their role extends beyond determining the cause of death to making recommendations aimed at preventing future fatalities. Oversight is provided through structured judicial systems, ensuring consistency and accountability across jurisdictions (National Coronial Information System, n.d.). Additionally, coronial findings and recommendations are usually published online, promoting transparency and enabling public scrutiny. In comparison, the United States employs a more decentralised system with variations across states that usually focus on the cause and manner of death only. Some jurisdictions may elect officials without medical training, while others employ medical examiners, which leads to inconsistencies in qualifications, procedures, and oversight (Pearsall, 2011).
Coroners in Australia are responsible for collecting all information concerning who the deceased person is, how the person died, when the person died, where the person died and what caused the person to die (Coroners Court of Queensland, 2025). This information is then collected from a range of sources including but not limited to family, friends, police officers and independent bodies such as therapists, counsellors and may include police reports, medical records (including autopsy reports), witness statement, and other relevant documents (Coroners Court of Queensland, 2025). Overall, the reports provide an official and detailed account of events that typically include a wide range of evidence.
Data collection
Using the Coroners Court of Queensland database, reports were collected of cases investigating such incidents that occurred between 2010 and 2023 inclusive. The start of 2010 marked major changes to policing, including the introduction of less lethal weapons nation-wide and a shift from reactive-style policing to community-oriented policing (Hine & Davenport-Klunder, 2022).
Every case for this period was briefly read for relevance. Cases were included only if the fatal incident involved an interaction between a police officer and a PMI that resulted in the death of the PMI. PMIs were identified if the coroner's report specifically stated that the person was diagnosed with mental illness or was likely to be suffering from a mental illness at the time of the incident. Cases were included regardless of whether the fatality was a direct result of intentional police actions (such as a police shooting) or indirectly associated with, though not necessarily caused by, police actions (such as a suicide or accident). The inclusion criteria also included deaths that occurred after the interaction itself but were a direct result of the interaction; for example, cases where the PMI died in transit from the incident or died later in hospital. Reports were excluded if a PMI died before police arrived. All relevant cases were then read in full, and data extracted into an Excel spreadsheet for organisational purposes and to systematically record key variables prior to analysis.
Data coding and analysis
To ensure quality and consistency, a codebook was created. Data were coded by at least two members of the research team to ensure quality and consistency. Any discrepancies were discussed until 100% agreement was reached.
Cases were coded into two main dependent variables: self-directed crises and externally directed crises. Self-directed crises involved incidents where the PMI was mostly a source of risk of harm to themselves. This sample group consisted of PMI who had suicidal intentions. In contrast, externally directed crises were cases that involved incidents where the PMI did not direct their crisis towards themselves, rather they had the propensity to cause harm to others or police. Aligning with RAT, cases were then coded for characteristics of the PMI, principal officer characteristics, and place characteristics. Fatal police–PMI interactions are relatively rare, and despite collecting data over a 13-year period and including all cases for an entire state, the resulting sample size was relatively small, yielding only 32 cases for analysis. Consequently, advanced statistical analyses could not be conducted due to breaches of assumptions, therefore, descriptive statistics were used to identify common patterns in these cases.
Results
The PMI characteristics
Table 1 presents the characteristics of the PMI who died in either self-directed crises or externally directed crises. Of the 32 cases, 12 (37.50%) involved self-directed crises and 20 (62.5%) involved externally directed crises. The data suggest that PMI were likely to have contact with health services prior to the incidents unfolding, including incidents that involved a crisis event or where the PMI committed a crime against a person. Specifically, 84.38% of the PMI were diagnosed with a mental illness prior to police contact. Specifically, 34.38% had been diagnosed with depression and 18.75% diagnosed with schizophrenia. Almost half of the PMI had additional complex needs—43.75% suffering multiple mental illnesses—the most frequent being depression and anxiety (18.75%). However, one (3.13%) PMI had up to six concurrent mental illnesses. For incidents that involved the PMI having a self-directed crisis, all but one PMI had been previously diagnosed with a mental illness. Conversely, 80% of PMI in incidents involving an externally directed crisis had been previously diagnosed with a mental illness.
Descriptive statistics of the subject characteristics.
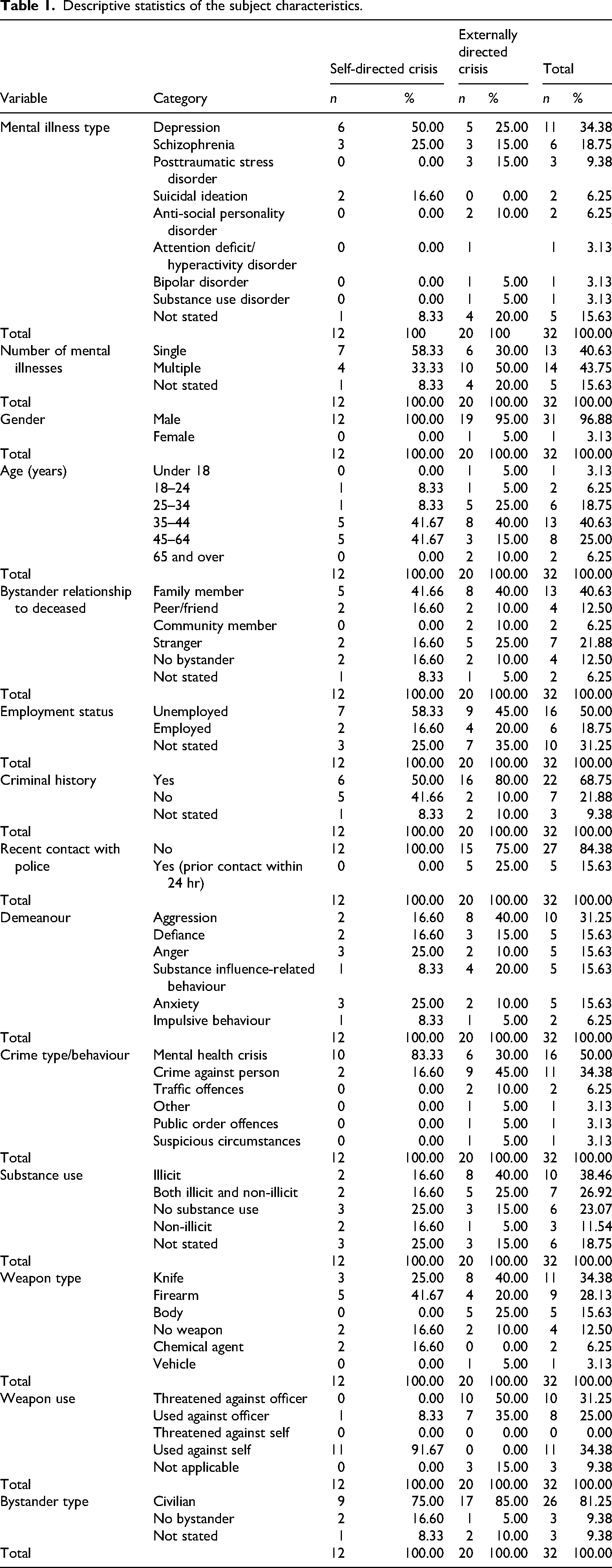
All PMI were male (96.88%) with the exception of one female. PMI were often accompanied by a bystander (81.25%), typically a family member or friend (53.13%). PMI were predominately middle-aged males overall, with the highest proportion (40.63%) falling within the 35–44 age range, followed by those aged 45–64 (25.00%); however, this category spans twice the years of the 35–44 range. 3 Notably, most PMI who experienced a self-directed crisis fell equally within the 35–44 and 45–64 age groups (41.67% each), while those experiencing externally directed crisis were more evenly spread.
Half of all PMIs (50.00%) were unemployed, and 18.75% of all PMIs were employed. PMI experiencing externally directed crisis most often had a criminal history (80.00%), while those who experienced self-directed crises were more equally distributed between those with criminal histories and those without.
The analysis also revealed that the demeanour between the two groups tended to differ. PMI who were experiencing an externally directed crisis were more often aggressive (40.00%) when police were called to the scene compared to those experiencing self-directed crises, who tended to be experiencing anxiety (25.00%) or anger (25.00%) more often. Furthermore, a notable proportion of PMI that were aggressive also had a criminal history (68.75%). Half of all reported incidents involved the PMI having an active mental health crisis (50.00%), with many PMI displaying behaviours of defiance (15.63%), anxiety (15.63%) or anger (15.63%). Examinations of the initial crime type or behaviour of the PMI when police were called revealed that most PMI in the self-directed crisis group were experiencing a mental health crisis (83.33%) compared to those in the externally directed crisis group who were more often committing crimes against a person (45.00%). Additionally, PMI tended to be using drugs and/or alcohol (76.92%).
The data reveal the strong opportunity for violence during these encounters, with most PMI in possession of a lethal weapon during the encounter—34.38% carrying a knife and 28.13% armed with a firearm. However, the usage was notably different between the two groups. Specifically, the externally directed crisis group were found to express their aggression outwardly towards others, either threatening or using the deadly weapons against police (85.00%). In contrast, PMI experiencing self-directed crisis were more inclined to use the deadly weapon on themselves during these incidents (91.67%), expressing an internal struggle. This finding aligns with the understanding that suicidal PMI may be engaging in “suicide-by-cop” scenarios.
Principal officer characteristics
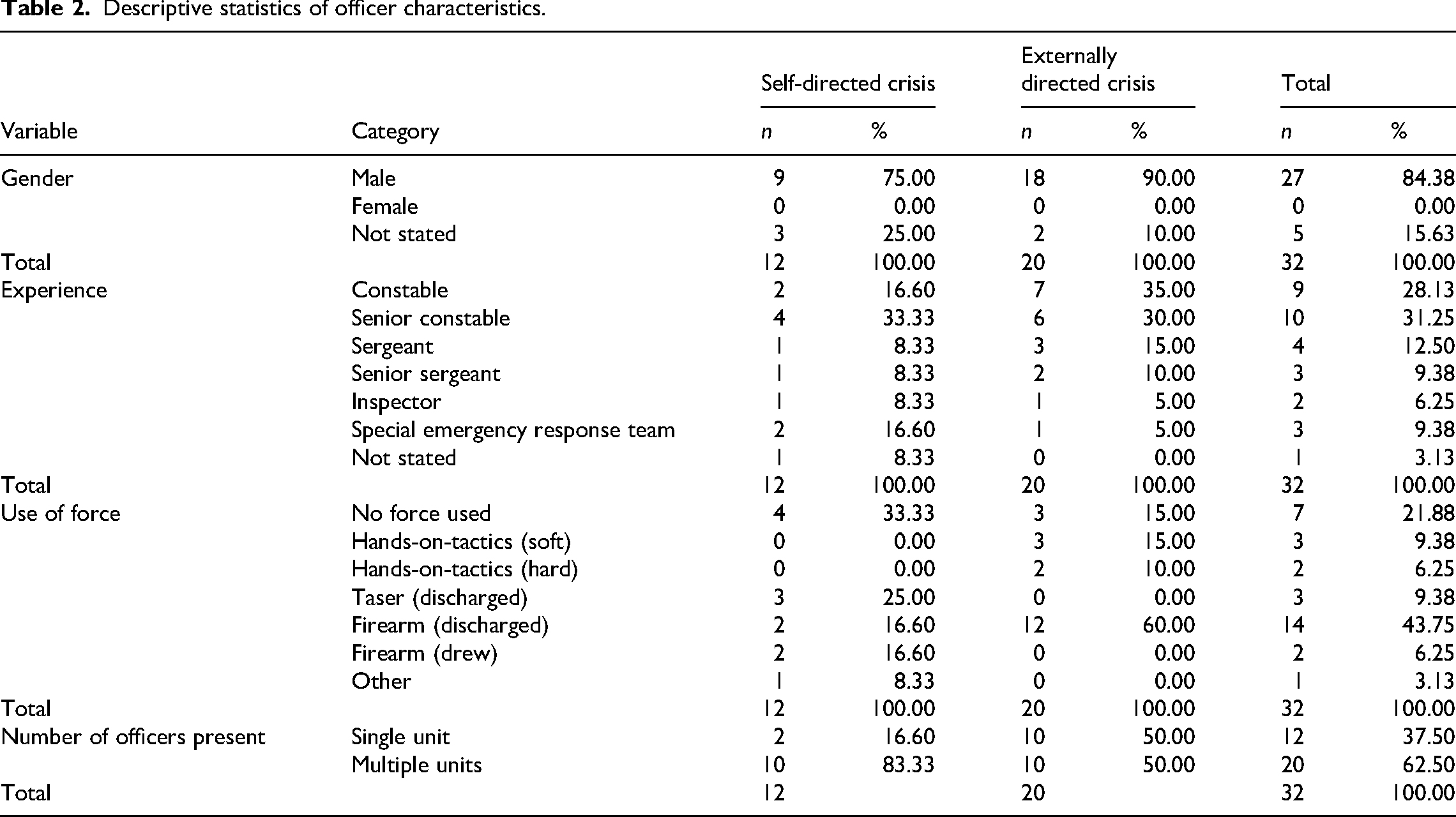
Table 2 reveals that in both types of crises, all the principal officers responding to the situations were male, with no female officers recorded in either group. Notable differences in officer ranks and levels of force used between the two groups were also found. Specifically, lower ranking constables (35.00%) and senior constables (30.00%) more frequently (65.00%) were the primary officers responding to externally directed crisis situations. Conversely, higher ranking officers such as senior sergeants or higher (41.59%) were almost just as likely as lower ranking officers (49.93%) to be the primary responder to self-directed crisis situations. In terms of force used, a notable difference was observed between the two crisis types. In self-directed crises, firearms were drawn or discharged in 33.20% of incidents. However, in externally directed crises, the use of discharged firearms was higher, occurring in 60.00% of cases. Responding units attending externally directed crisis were more evenly spread, as both single units and multiple units responded to these incidents. However, there were mostly multiple units responding to self-directed crisis situations (83.33%).
Descriptive statistics of officer characteristics.
Place characteristics
Table 3 illustrates the characteristics of the place, highlighting the critical role of the situational contexts in these encounters. The findings reveal that a significant majority of incidents occurred in domestic environments, with 65.63% taking place in the home. The majority of PMI that expressed self-directed crisis (75.00%) and externally directed crisis (60.00%) in these incidents were within a dwelling, suggesting that little threat was posed to the community, enhancing officers’ ability for safety management of incidents.
Descriptive statistics of place characteristics.
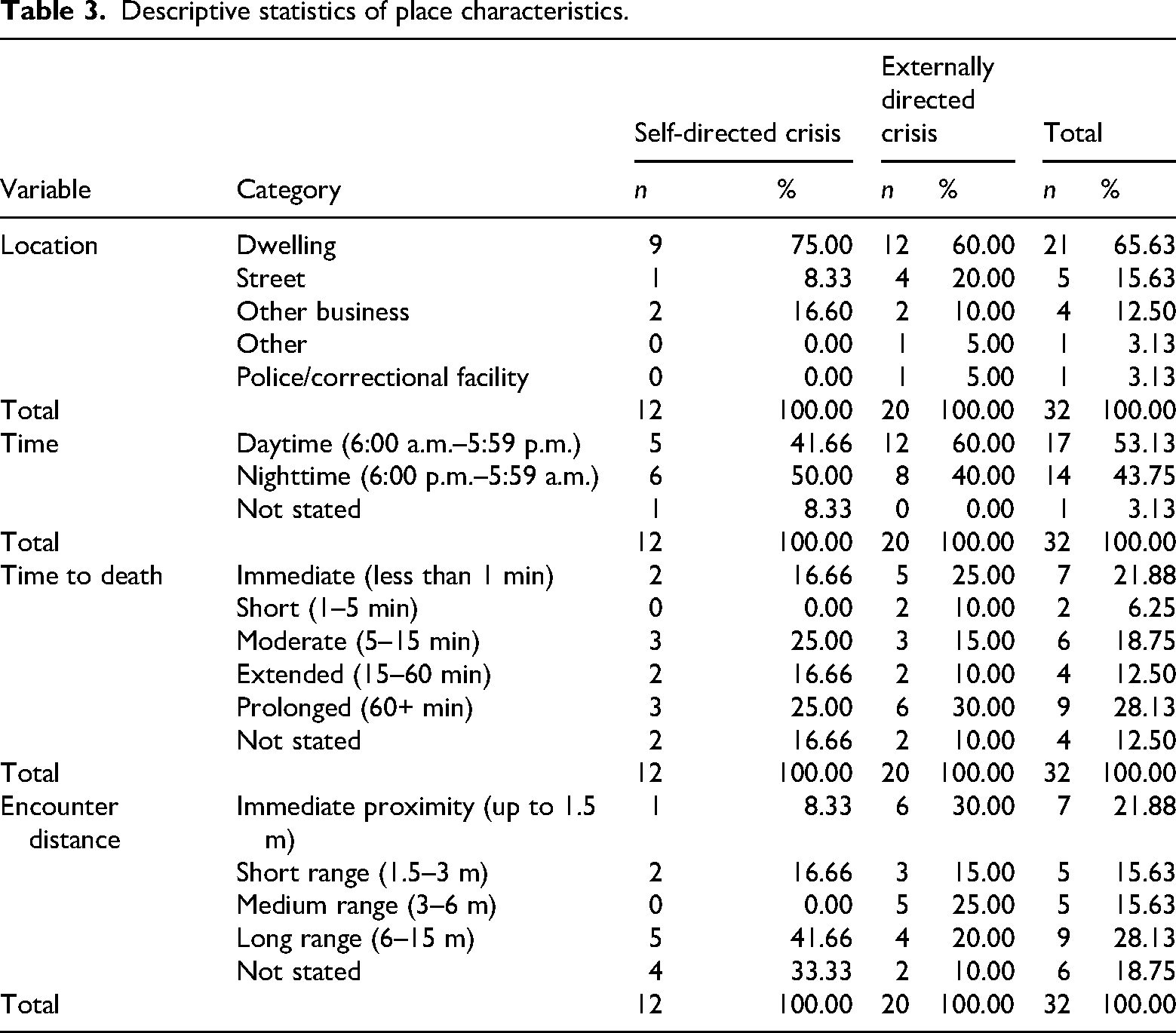
Combined, these incidents were also evenly distributed between night (43.75%) and day (53.13%). However, incidents involving PMI conveying a self-directed crisis were almost just as likely to happen during the day (41.67%) compared to night (50.00%), whilst PMI expressing externally directed crisis were found to mostly be involved in incidents during the daytime (60.00%).
Additionally, the study found the most common outcome for the duration of the incident in terms of the time to death was a prolonged period, with 28.13% of cases extending over an hour. However, this was closely followed by cases where death occurred almost immediately, within less than a minute (21.88%). This was consistent for both groups, highlighting the extreme variability in the duration of these fatal incidents. Where these incidents largely differed was encounter distance between officer and PMI. Those experiencing self-directed crisis were found to consistently be within long ranges of police, accounting for 41.66% of cases. PMI experiencing externally directed crisis were just as likely to be within arm's reach of police during the incident compared to long ranges, suggesting extremely dangerous circumstances for officers to navigate.
Discussion
This study explored cases in Queensland (Australia) where PMI died during or following critical interactions with police. Specifically, it focused on identifying characteristics of the PMI, officer, and place that contribute to fatal outcomes using a RAT framework. The findings from this study indicate notable differences in the nature of police interactions with PMI depending on whether the crisis was self-directed (such as suicide attempts) or posed an external threat (such as threat to officers or others). While fatal police–PMI encounters remain relatively rare, the data showed distinct patterns in the characteristics of the PMI, officers, and situational contexts. These patterns are discussed below in terms of potential opportunities for support actors and frameworks.
The PMI
The study revealed useful insights into the PMI themselves in these situations. For instance, PMI involved in self-directed crises were more likely to exhibit internal struggles, often resulting in suicides, while those involved in externally directed crises were more aggressive and more likely to direct their actions towards others, including police. Notably, in all cases, the PMI was typically male and middle-aged. This is consistent with broader research surrounding mental health in Australia, which also identifies these demographics as being at increased risk for such interactions (Independent Office for Police Conduct, 2024; Saleh et al., 2018) and amongst the least likely to seek care for their mental health issues (Australian Institute of Family Studies, 2020; Crissman, 2019; Tang et al., 2021). The findings also revealed that a large portion of these events also included bystanders such as family members and friends present at the scene (53.13%). Indeed, previous research indicates this to be a common factor in police interactions with PMI (Frankham, 2018).
Given these findings, key potential Crisis Supporters for the PMI can be identified. For instance, since a significant proportion of these encounters involve family members or take place within a household setting—there is an opportunity to utilise family members as effective Crisis Supporters in these situations who often serve as the primary caregivers for PMI—offering critical support in areas such as daily self-care, managing psychiatric distress, accessing services, and handling financial matters (Chronister et al., 2021). Their close relationship and frequent interactions with the PMI position them uniquely to notice early signs of crisis, facilitate de-escalation, and provide vital information to first responders. However, ensuring the safety and appropriateness of engaging family members and friends in the assistance of negotiation with the PMI is paramount. It is also important to note that family members often experience burnout, which can limit their capacity to act effectively as Crisis Supporters (Aass et al., 2021). Additionally, sometimes family members may have mental health or substance abuse issues themselves, which can affect their ability to effectively communicate and help police and, in some circumstances, hinder police operations (Frankham, 2018; Freeze & Campbell, 2024). Beyond these concerns, collaboration between mental health practitioners, general healthcare providers, and community-based mental health outreach programmes is crucial. Integrating mental health services within primary care settings can offer more comprehensive support, ensure early intervention, and provide families with the necessary resources to manage crises more effectively (Kebe et al., 2020). It should be noted that Queensland Health (2016) has attempted to implement these strategies with Connecting Care to Recovery. 4 However, their approach—whilst beneficial in some areas, including the shift towards community-based care—struggled to implement collaboration between primary care and community-based care (Queensland Health, 2016).
To support these efforts, potential support frameworks such as public health authorities, government agencies and policymakers should implement policies and guidelines that promote and ensure mental health awareness and early intervention strategies by ensuring that mental health services are more accessible and integrated into primary care. Additionally, funding and supporting public health campaigns aimed at reducing the stigma around mental health and encouraging men to seek help could further enhance the effectiveness of these Crisis Supporters. For example, Collins et al. (2019) have found that stigma surrounding mental illness has declined since the introduction of campaigns that decreased stigma and increased the probability of PMI to seek and acquire treatment. Whilst Queensland Health (2022) has to some degree already introduced these support frameworks, they intend to improve upon these changes in their Better Care Together 5 initiative that extends into 2027 (Queensland Health, 2022).
A second key finding highlights other vulnerabilities of the PMI aside from their mental illness. These situations often involved PMI affected by drugs and/or alcohol, unemployed, with a criminal history, or displaying aggressive, angry or anxious behaviours. These findings are consistent with previous research (Australian Institute of Health and Welfare, 2024; Crissman, 2019; Thomas, 2020). These overlapping vulnerabilities suggest a complex interplay of factors that contribute to the heightened risk during police interactions. Addressing these issues requires a multifaceted approach, including targeted support services, substance abuse treatment, and employment programmes, which can help stabilise individuals and potentially reduce the frequency and severity of these crises.
Subsequently, potential Crisis Supporters that could intervene and mitigate these factors include substance abuse counsellors and rehabilitation programmes such as anger management. Indeed, research shows the positive impacts of substance use treatment services (Ritter et al., 2024) and anger management programmes (Henwood et al., 2015; Kjærvik & Bushman, 2024).
To provide aid to these programmes, potential support frameworks, including public health authorities, government agencies and policymakers, should implement policies and guidelines that promote awareness and access to these early intervention strategies. Their role as support frameworks can influence the broader system by ensuring substance abuse services and anger management programmes are more accessible and integrated into primary care. Research suggests that, in Australia, only 32% of government budgets for addressing use of illicit substances was used for prevention, treatment and harm reduction programmes (Ritter et al., 2024) despite these programmes having proven benefits. This signifies the need for these budgets to be redistributed to improve the breadth of care and access to these programmes that are currently unable to cope with demand of patients (Ritter et al., 2024). By establishing a framework that prioritises early intervention concerning substance use and anger management programmes, support frameworks can play a critical role in reducing the frequency of police encounters with individuals in mental health crises.
A third key finding of this study is the frequent presence of lethal weapons in these encounters, with a large proportion of PMI found to be armed during their encounter with police. The data revealed that while individuals experiencing self-directed crisis were more often using weapons on themselves, those in externally directed crisis were more often threatening to use these weapons against others, including police. This finding aligns with previous research indicating that weapons are often involved in fatal police–PMI encounters, which can significantly escalate the risk and complexity of these situations (Crissman, 2019; Saleh et al., 2018). The presence of weapons not only heightens the perceived threat for responding officers but also limits their options for de-escalation.
Given these findings, identifying potential Crisis Supporters to de-escalate crises involving PMI in possession of deadly weapons is critical. Police, by necessity, are often the primary responders due to the potential harm PMI can pose to themselves and others. Yet, officers typically have limited training and experience in appropriately handling such incidents, relying mainly on their academy training, which typically focuses on the use of force, subsequently creating adverse environments for both police and PMIs to be harmed during these interactions. This signifies the need for mental health training programmes, such as Crisis Intervention Team (CIT) (Herrington & Pope, 2014; Rohrer, 2021).
Support frameworks such as policymakers and government agencies should re-evaluate and strengthen firearm regulations. Currently, firearm regulation in Australia varies by state, with Queensland having some of the most “lenient” laws (Levy, 2024). By restricting access to firearms for high-risk groups, authorities can create safer conditions for officers to de-escalate crises and reduce the risk of harm.
The principal officer
The findings from this study provide valuable insights into the characteristics and actions of police officers involved in fatal interactions with PMI. Specifically, the findings revealed that all principal officers responding to both self-directed and externally directed crises were always male. This finding may reflect the broader gender distribution within policing, which tends to be male-dominated (Davenport-Klunder & Hine, 2023), but also raises questions about the role gender may play in these high-risk interactions. When examining the experience level of officers involved, the findings show a varied distribution across ranks. Low ranking officers were likely to be involved in externally directed crisis incidents, suggesting that less experienced officers frequently handle these complex situations, possibly impacting the choice of response tactics. The findings are consistent with broader research, which also finds these officer demographics are at the highest risk of being involved in these incidents (Baker & Pillinger, 2019; Rohrer, 2021). The use of force in these encounters varied notably between self-directed and externally directed crises. Police responded by discharging firearms in a notable proportion of the externally directed crisis situations. This finding is perhaps not surprising given the focus of the study on fatalities but does present the opportunity to explore alternative de-escalation tactics for officers, particularly those of lower ranks, to reduce the reliance on lethal force.
Integrating more female officers into the roles of Response Aides could provide a valuable alternative perspective and approach in these high-stress environments. Research suggests that female officers often employ more communication-focused and empathetic strategies, which may help de-escalate tense situations (Davenport-Klunder & Hine, 2023; White et al., 2021). Female officers could serve as Response Aides in crisis teams by bridging skills in communication and empathy, which are critical for de-escalating sensitive situations involving PMIs (White et al., 2021). Furthermore, incorporating higher ranking, more experienced officers into frontline responses could enhance the effectiveness of crisis management and de-escalation strategies.
To offer backing to these crucial Response Aides, potential support frameworks such as police management and policymakers should implement guidelines and recruitment strategies that support and promote female employment in the police force. These support frameworks can influence the systems and guidelines that have been found to contribute to female officer underrepresentation such as stigma, poor complaint resolution systems, promotion obstacles and discrimination (Rabe-Hemp & Venessa, 2019). Higher ranking officers with more experience can create this change through their seniority and expertise in the police organisation. Influencing change at the station level ensures females have the same opportunities as male officers and destigmatises current beliefs of “men's” and “women's” work in the police service (Davis, 2018).
The place
Lastly, this study found critical insights into the situational contexts of fatal police interactions with PMI. The majority of incidents occurred within dwellings, highlighting the private nature of these situations, similar to previous research (Crissman, 2019; Saleh et al., 2018; Thomas, 2020). Since most incidents occurred within the home, they may pose less immediate risk to the general public, as these situations are confined to private spaces, thereby also providing an opportunity for police to create the time and space necessary to involve third parties such as mental health experts to assist in de-escalating the crises more effectively. Indeed, a large portion of these cases involved extended durations and occurred at a longer distance, providing further opportunities for strategic intervention and the involvement of third-party support.
Ultimately, the current study's findings suggest that these incidents provide time and space for third-party intervention. Potential Environmental Facilitators who could intervene and prevent fatal outcomes may include mental health practitioners such as psychologists, counsellors or social support workers that could work alongside officers and use their expertise and experience to de-escalate PMI in crisis with the aid of officers to help minimise threat to safety (Rohrer, 2021). Additionally, remote telecommunication programmes involving forensic psychologist practitioners may also provide officers with relevant management strategies (Queensland Forensic Mental Health Service, 2016).
To ensure these Environmental Facilitators are readily available and collaborate with police agencies, potential support frameworks such as police agencies and mental health services need to improve interagency communication and collaboration. There has been a disconnect between these services (Herrington & Pope, 2014). Support frameworks can address this by establishing clear protocols, joint training programmes, and regular communication channels between mental health services and police. Moreover, they can allocate resources to dismantle structural barriers within mental health services, ensuring more seamless integration with police.
Strengths and limitations
Despite the current study examining all fatal PMI interactions with police over a 13-year period in Queensland, the data provided a relatively small sample size for analysis, which limited opportunity to employ advanced quantitative techniques. However, it is important to note that the sample represents 100% of known fatalities involving PMI during police interactions in Queensland over the timeframe. As such, the data provide a complete account of the most severe PMI encounters—cases that have a significant impact on both the criminal justice system and the broader society.
Coroners reports contain official data ensuring credibility and reliability of the source; however, being secondary data, they have some limitations. Coroners only provide information they deem necessary or a contributing factor to the PMI deaths, constraining the information available for data collection. Future research should consider expanding the data sources to provide additional vital information to help inform best police practices.
Lastly, fatal PMI incidents involving police comprise a highly under-researched area, with extant literature primarily coming from U.S. populations. The need for more international comparisons, especially in the Australian context, is paramount. Future research could include larger populations (e.g., national studies) that provide large samples. This would provide opportunities for better international comparative research and the ability to use more advanced techniques to understand the data.
Conclusion
The study provided a theoretical framework identifying characteristics of PMI, police, and the place involved in PMI–police interactions where the PMI dies, highlighting differences between self-directed and externally directed crises. Self-directed crises often involved middle-aged males experiencing a mental health crisis, sometimes using firearms on themselves, often in the presence of family members. While it is well established that family and friends are frequently involved during these incidents, often as the ones who initiate contact with police, the findings reinforce the critical and under-supported role they play. Recognising their proximity and insight into the PMI's condition, the study highlights the need to better equip and formally integrate family members as Crisis Supporters within response frameworks. Externally directed crises involved PMIs with criminal records who threatened/used weapons against officers. Training officers in CIT could improve negotiation skills and de-escalation outcomes. Both crisis types often occurred in dwellings, with lower ranking male officers typically responding. Strategies like the co-responder model and increasing female police presence as Response Aides could help mitigate risks. Exploring these issues through the crisis triangle offers valuable insights into support actors and frameworks involved in fatal PMI–police interactions, emphasising collaboration to reduce harm and improve outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.