
Abstract
This study aimed to investigate how Anabolic–Androgenic Steroid (AAS) users and healthcare professionals perceive the criminalisation of AAS on users’ ability to seek help and, ultimately, what effect this has on the health outcomes for these consumers. This study triangulated the views (N = 24) of male (n = 8) and female (n = 7) AAS users (Mage = 35.4, SD = 9.1), as well as healthcare providers (n = 9), regarding how the criminalisation of AAS had an impact on consumers’ health behaviours and help-seeking. Data were analysed thematically. An overarching narrative was developed regarding the “politicogenic drug effects” which emerge from the illegality of AAS with three overarching themes. First, participants expressed challenges in seeking help and support due to the stigma and fear associated with the illegal nature of AAS use. This fear stemmed from the criminalisation of AAS and the potential legal consequences. Participants also highlighted the social challenges and the need for secrecy surrounding AAS use, which further hindered open discussions and engagement with healthcare providers. The cohort emphasised the close-knit social networks among AAS users, offering support and shared experiences but also entangled in the criminality associated with AAS use. Moreover, participants acknowledged the difficulties in promoting harm reduction initiatives due to the need for secrecy and the potential social and economic disadvantages. The escalation of AAS criminalisation that has impacted both consumers and healthcare professionals has exacerbated the challenges associated with their interaction, further impeding a relationship already fraught with obstacles. Consequently, users remain entrenched within the illicit market, with few options for harm reduction intervention. The study advocates for a rethinking of AAS policies, considering a potential reclassification aligned with the United Kingdom's Class C framework to destigmatise use and promote harm reduction. This shift would require comprehensive research to assess its impact on public health, user behaviour, and harm reduction outcomes.
Keywords
Introduction
Most Anabolic–Androgenic Steroids (AAS) are illicitly manufactured products, the majority of which have never been developed for the licit medical market (Magnolini et al., 2022). Non-medical consumption is generally facilitated through illegal means, in line with the proliferation of online markets (Cox et al., 2023; Dunn & Piatkowski, 2021; van de Ven et al., 2020). The use of AAS has extended beyond the realms of high-level sport and performance for some time, with most consumers now typically being recreational weight lifters (Goldman et al., 2019; Kanayama & Pope, 2018). Indeed, the “typical” AAS consumer is not normally an elite athlete. Instead, several user typologies capture the increased heterogeneity of the AAS-consuming population, with use revolving around well-being (Christiansen et al., 2017) and body image (Piatkowski et al., 2020; Piatkowski, White, et al., 2021; Underwood, 2017). Research has demonstrated some common practices that contribute to increased harm among contemporary illicit AAS consumers, including polysubstance use, risky sexual practices, and instances of criminal behaviour (Piatkowski, Dunn, et al., 2021; van de Ven et al., 2018). However, a relatively unexplored area in the current literature is the criminalisation of AAS in some nations and the associated harms and harm reduction challenges. This article therefore seeks to address this relative lacuna by examining the experiences of users and practitioners in Australia, where AAS are criminalised.
Griffiths et al. (2016) suggest that the level of social stigma directed towards AAS is comparable to that directed towards potent narcotics like heroin. This significant stigma could potentially create a substantial obstacle to the pursuit of options to reduce harm. Echoing findings from the United Kingdom (Richardson & Antonopoulos, 2019), Australian AAS users have been found to be a “hard-to-reach” group for medical/health professionals (Piatkowski, Hides, et al., 2022). Indeed, Monaghan (2002) points out that individuals who use AAS construct rationalisations for their drug consumption, creating an intricate network of personal interpretations that they deem valid reasons for their actions. As a result, AAS users in the United Kingdom have been shown to simultaneously employ their own resources to access diverted medications to counteract potential adverse effects (Salinas et al., 2019). In line with these findings in UK samples and given the lack of a dedicated harm reduction framework for AAS in Australia, users often turn to each other for sourcing and advice, often disregarding the criminal implications of doing so (Tighe et al., 2017). Notably, even in the United Kingdom where personal possession of AAS is legal, many users remain secretive in response to the stigma fuelled by mainstream media (Kimergard & McVeigh, 2014b; McVeigh & Bates, 2022). Therefore, in the Australian context where use is dealt with punitively (see Table 1), this stigma is compounded by the harsh laws and policies surrounding AAS (Mulrooney et al., 2019). Moreover, a closer examination of the approaches between Australia and the United Kingdom reveals noteworthy distinctions in their strategies towards AAS use. Both countries adopt harm reduction as a guiding principle, which focuses on implementing measures to mitigate the adverse consequences of health-related behaviours, without necessarily eradicating such behaviours entirely or permanently (Hawk et al., 2017). However, the practical implementation and outcomes diverge significantly due to the complex interplay of sociocultural factors, legal frameworks, and healthcare structures (Henning & Andreasson, 2022). Recognising these nuanced differences is pivotal in drawing insightful lessons from the United Kingdom's approach and adapting them to the Australian context. This comparative perspective invites us to contemplate not only the effectiveness of distinct policies, but also the essential role of localised considerations in shaping meaningful interventions for AAS users.
Key aspects of policy approaches towards AAS in the United Kingdom and Australia
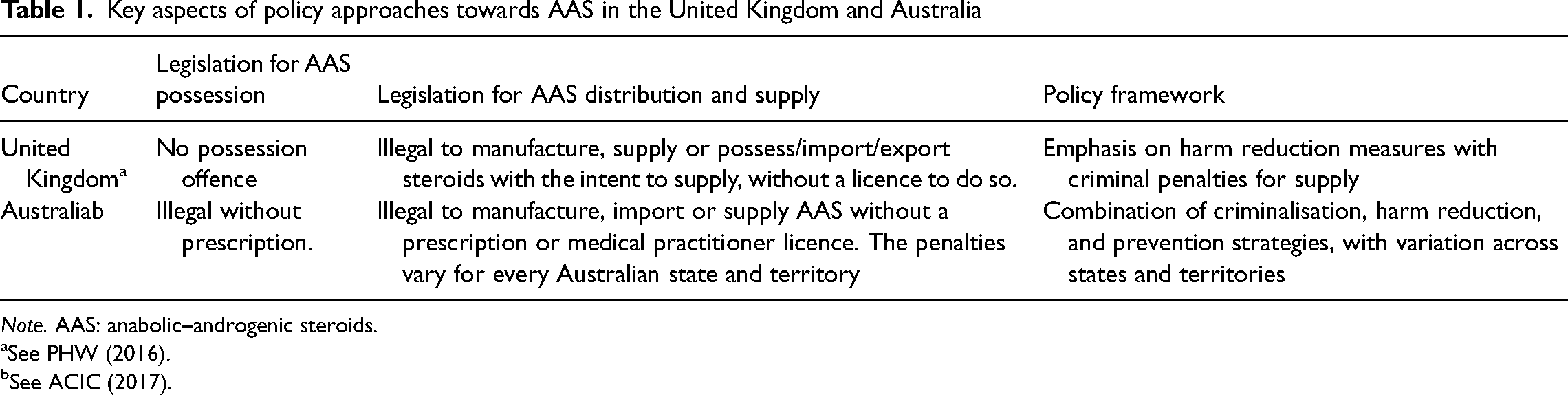
Note. AAS: anabolic–androgenic steroids.
See PHW (2016).
See ACIC (2017).
AAS-related arrests in Australia have increased by 218 percent over the last decade (Crime and Corruption Commission, Queensland [CCC], 2021). However, the legal consequences for the distribution of AAS differ across various jurisdictions within the nation (Australian Crime Intelligence Commission [ACIC], 2017). It is important to note that the utilisation of AAS within Australia has a longstanding history of being prohibited except in instances where they have been duly prescribed by a licensed medical practitioner for legitimate therapeutic purposes (ACIC, 2017). This distinction means that some types of AAS were included in Schedule 4 of the Poisons List (New South Wales Health, 2021) and therefore, possession of these was prosecuted as such in legal settings prior to specified legislative changes in 2014 (ACIC, 2017; James & Wynn, 2022; van de Ven & Zahnow, 2017). Since 2014, Queensland has brought in punitive measures whereby AAS are categorised as a Schedule 1 drug, attracting up to 25 years in prison for possession, and meaning that AAS are aligned with other illicit drugs like heroin, methamphetamine and cocaine in terms of the seriousness of offence and penalty (CCC, 2016) and perceived harms (van de Ven et al., 2018, 2020). This categorisation may have been driven, in part, by perceptions that AAS use is a growing problem with ties to organised crime and international trafficking (Mulrooney & van de Ven, 2015). Similarly stringent penalties are enforced in New South Wales and Victoria, reinforcing the gravity with which these offences are treated (James & Wynn, 2022). However, the number of AAS detections at the Australian border displays a relatively stable trend over the last decade, increasing only 1% from 2010–2011 to 5,614 in 2019–2020 (CCC, 2021). Therefore, it appears that AAS detections in Australia have been unimpacted by legislation, necessitating some research around the perceptions of criminal justice efforts to punish AAS-related offences to critically challenge criminal justice policy. This is, therefore, what this article aims to achieve by seeking the voices of those “on the ground” who are most impacted by this policy decision.
Theoretical framing
It is important to acknowledge that traditional addiction models may not fully capture the complexity of AAS use and its drivers. While these models often portray drug users as passive victims of substances (Hunt & Barker, 2001), such perspectives do not account for the social and cultural factors influencing AAS consumption. Unlike substances that typically lead to addiction, AAS use is driven by a range of motivations beyond chemical dependency. For example, body satisfaction often emerges as a prominent motivator for initiating AAS use (Kimergard & McVeigh, 2014a; Piatkowski et al., 2020). Some users are unaware of the dangers associated with AAS, while others employ various strategies to manage risks, including self-experimentation to assess drug efficacy and adverse effects (Kimergard & McVeigh, 2014a). Thus, framing theoretical discussions regarding AAS should emphasise consideration of social contexts, user agency and the distinct cultural meanings attributed to AAS consumption (Duff, 2007; Rhodes & Treloar, 2008). Viewing AAS through a “politicogenic drug effects” framework (Hupli, 2023) offers an opportunity for critical examination of how these substances and their regulation collaboratively shape social networks, relationships, and practices. By transcending the traditional focus on individual-level chemical effects, this perspective acknowledges the intricate interplay of societal dynamics, regulatory measures and user-driven elements (Müller & Schumann, 2011; Pienaar et al., 2020).
The growing recognition of AAS consumption as a hazardous form of substance use (Goldman et al., 2019; McVeigh et al., 2022; Sagoe et al., 2015) has led to the emergence of discursive frameworks aimed at investigating and addressing this emerging public health concern. Of these frameworks, this study utilises a psycho-criminological framework and its construction of the AAS user as a rational drug consumer. The innovative and self-driven actions of individuals who have taken AAS and reshaped these substances’ usage, from therapeutic use to enhancement, exemplify these consumers’ creativity and agency. Drawing upon De Certeau's notion of “tactics of consumption” (De Certeau, 1984), consumers adeptly utilise AAS to fulfil their individual objectives, encompassing recreational pursuits, sporting endeavours or weight management, among others (Piatkowski et al., 2020). We argue the sociocultural trajectory of AAS exemplifies the fluid transfer of substances across various individuals, contexts and purposes, as elucidated by Appadurai (Appadurai, 1988). It highlights that the significance attributed to these substances is not contingent upon their inherent properties, but rather on subjective evaluations made by individuals (Appadurai, 1988). Indeed, social identity (Piatkowski, Obst, et al., 2022) and group norms (Piatkowski, Neumann, et al., 2023) have been identified as crucial factors influencing the initiation and persistence of AAS use in Australia. Echoing Cohen's (2014) perspective on methamphetamine use, the consumption of AAS in Australia may exhibit certain similarities, as it is not necessarily an act of deviance, but rather a response to growing societal expectations. In this context, AAS consumption can be understood as a means of meeting the heightened demands imposed by society; however, we acknowledge there is a diverse range of factors spanning from individual to societal levels, encompassing various motivations and drivers, which contribute to the multifaceted landscape of AAS usage.
The present study
Similar to the broader context of drug use, individuals who consume AAS can be viewed as rational consumers (Duff, 2004) who consciously opt to utilise AAS to attain desired outcomes. Nonetheless, social and cultural influences play a significant role in the decision-making process concerning drug use (Rhodes et al., 2003). Scholars indicate that the legality of a substance rarely factors into the considerations of potential drug users (Seear, 2019). Elevating penalties associated with the utilisation and possession of AAS has not, thus far, dissuaded uptake or motivated users to discontinue usage. Instead, this approach has failed to effectively deter AAS use but has intensified the seriousness of the AAS consumption experience and associated risks. First, we contend that it has impeded access to essential medical services and information by discouraging both users and healthcare professionals from engaging in discussions about AAS use (Dunn, Piatkowski, et al., 2023; Piatkowski, Hides, et al., 2022). Specifically, the criminalisation of AAS may have contributed to this therapeutic barrier (Piatkowski et al., 2022) by creating an atmosphere of stigma and fear among healthcare professionals. The uncertainty surrounding legal consequences and the broader negative perception of AAS use may discourage healthcare practitioners from engaging in open discussions with users about their AAS consumption, leading to a lack of comprehensive knowledge and understanding of these substances within the medical community. Moreover, stricter penalties have diverted attention from vital harm reduction measures, such as promoting safe injection practices (Dunn et al., 2014; van de Ven et al., 2018). Additional inadvertent negative consequences arising from criminal justice responses to this form of drug use encompass the expansion of a thriving illicit market, geographical displacement of users and suppliers, as well as an augmented risk of substandard drug quality (Turnock & Gibbs, 2023; van de Ven et al., 2020). Specifically, the criminalisation of AAS has been attributed to users’ reliance on personal connections, concerns about counterfeit products and limited access to reliable information (Piatkowski, Puljevic, et al., 2023). Therefore, the current study explored the broader implications of the criminality surrounding AAS. The aim was to investigate how AAS users and healthcare professionals perceive the criminalisation of AAS on users’ ability to seek help and, ultimately, how this affects the health outcomes for these consumers.
Methods
As components of larger research projects (Dunn, Piatkowski, Lamon, et al., 2023; Dunn, Piatkowski, Whiteside, et al., 2023; Piatkowski, Hides, et al., 2022; Piatkowski, Lamon, et al., 2023; Piatkowski, Neumann, et al., 2023), a series of semi-structured interviews were performed with several subsamples of individuals regarding AAS, including users and healthcare providers. The present study draws on a subset (N = 24) of these. Ethical approval was granted from the Griffith University and Deakin University Human Research Ethics Committees.
Several methods were employed to ensure rigour in the analysis. Knowledge is co-constructed between the researcher and the participant and so the theoretical positioning of the investigation may influence data analysis (Poucher et al., 2020). We employed an inductive approach, whereby themes derived from the data were interconnected, consistent with the ontological framework of social constructivism that guided this study. Thematic analysis was utilised to discern and categorise patterns of significance inherent in the dataset, facilitating the identification and organisation of meaningful themes that emerged from the data. The researchers reflected on their experiences as a behavioural scientist, a public health researcher and a criminologist, frequently. The first author actively engages with the AAS consumer community and has a background in the broader realm of strength sports and fitness. His involvement provided a comprehensive understanding of the subcultures that develop among AAS users, and his lived experience constitutes a valuable asset in the research process, enabling profound exploration during interviews and enhancing the depth of inquiry (Anderson, 2021; Zampini et al., 2021). The other authors provided different plausible interpretations of findings and generated novel themes which aided in the construction of the findings and are in line with good practice (Braun & Clarke, 2023).
Sampling and recruitment
The 24 semi-structured interviews were conducted with a mixture of face-to-face and online participants in Australia. The participant sample was purposive and recruited via researcher contacts and through snowball sampling. All interviews were conducted by the lead author. Participants were eligible to be included in this analysis if they had ever used AAS and were over the age of 18, or if they were healthcare providers who frequently interacted with AAS users. The healthcare providers (n = 9) were general practitioners (n = 6) and harm reduction workers (n = 3) who regularly worked with AAS-using patients and clients. The 15 AAS-using participants had a mean age of 34.8 years (SD = 9.2) with relatively even groups of males (n = 8) and females (n = 7). Within this subgroup, all participants were currently using AAS at the time of the study.
The substances employed by the AAS-using cohort included testosterone or its derivatives (e.g., nandrolone, drostanolone, and stanozolol) at various dosages, administered orally and/or intramuscularly. As an overview of the multifaceted substance utilisation within the AAS-using cohort, we also present the intricate nature of their consumption patterns and the array of products employed for enhancing appearance and performance. For instance, many participants were long-term users and had completed multiple “cycles” (AAS combinations and durations of use) and “stacked” (combined) their AAS (injectable and oral) with other Performance- and Image-Enhancing Drugs (PIEDs) such as clenbuterol, insulin, and metformin. Some participants also used other PIEDs for appearance purposes such as Melanotan II (a variant of afamelanotide) (Turnock & Gibbs, 2023). Some participants opted to use prescription medicines such as Angiotensin II Receptor Blockers (ARBs), which could be part of a health maintenance strategy, potentially influenced by online anabolic coaching initiatives (Gibbs et al., 2022).
Materials and data collection
The data for this study are related to excerpts from interviews where participants discussed the legality and criminality related to AAS. This discussion emerged from participants within the broader discourse of use and supply of AAS. The interviews were between 25 and 82 minutes in duration (M = 40.5 minutes). All interviews were digitally recorded and transcribed verbatim. A semi-structured interview guide was used for each cohort with some points of overlap between studies. For example, each semi-structured interview schedule included a list of prompts. The prompts first related to gaining information about the participant, before enquiring about their AAS usage. The remainder of the semi-structured interviews utilised themes identified from previous literature including body image, polysubstance use, social influence, physical and psychological health, and significant life events.
Data analysis
NVivo 12 (QSR) was used to facilitate data organisation, coding and analysis. Inductive analysis was used to identify codes which were synthesised into themes to summarise the key findings from the interviews. The thematic analysis followed Braun and Clarke's six-step guide (Braun & Clarke, 2019), involving data familiarisation; initial code generation; identification of potential themes; review of themes; definition/naming of themes; and the writing up of findings. The lead author generated codes, then further organised and conceptually supported these codes with relevant examples from more than one transcript (Braun & Clarke, 2006). Themes were developed by re-engaging with the transcripts (Braun & Clarke, 2021). As a result of this process, a list of verbatim quotations illustrating each theme was compiled and a list of theme titles and representative extracts was created (Braun & Clarke, 2006). These theme titles and extracts were reviewed and discussed by the researchers in multiple meetings and throughout the analytic process. An overarching narrative was developed regarding the criminality and illegality of AAS with three overarching themes.
Findings
Theme 1: “they’re scared to ask for help”: stigma, help-seeking, and “the law”
Participants acknowledged the broader impacts which the illegality of AAS use had on themselves and their peers. They highlighted the difficulties related to seeking institutional advice and support when using AAS, resulting from criminalisation and the associated perception of deviance. By acknowledging the consumption of these substances, users believed they opened themselves up to the possibility of legal ramifications. Interviewer: What do you think are the biggest obstacles for steroid consumers? P4 [AAS User]: Well, it's not legal what they’re doing, so they get scared to ask anyone. Interviewer: So, you recognise that criminal element brings a lot of fear? P4 [AAS User]: Well, are you gonna go around asking people “What should I do when I use this [AAS]”, and they might say “how do you get that [AAS]” and then they ask some other questions too. So, I guess that's the first thing that will stop someone from going anywhere.
Although some of these concerns stemmed directly from the illegality of AAS, others were related to societal norms more broadly. For example, some participants discussed the social challenges which came from using “illegal” substances like AAS. Although there was discussion of their use among their social circles, discussing the use of AAS for non-medical reasons with those outside the AAS-using group was not condoned. P2 [AAS User]: It's the way that they’re [AAS] viewed by people. Because of that, you have to be careful. We talk about them at [place] because most of us are using. Outside that though, no way.
Expanding on this, participants were extremely reticent to disclose their AAS consumption beyond their drug-using peers, due to the illegality of the substances and a sense of trepidation of being cast as illicit drug users. One participant spoke distinctly to the far-reaching impacts of publicly announcing use. Participants also directly related these impacts to the way the public perceived AAS use, as a result of “the law”. P20 [AAS User]: I don’t publicly acknowledge it [AAS use], because obviously there are legalities involved with what we do. … I don’t want people viewing me differently just because of the way they see [AAS] use. Like, the way that the law portrays it. P6 [GP]: I think stigma and prejudice are the dominant things. And so that link with it … being illegal means that they’re scared to ask for help. P6 [GP]: And I don’t think many people in the fitness community or the gym community or the gay community even know about the reality of their illegal status. So I think it's attractive well, especially for young men, that they might source drugs without prescription and then not realise that they’re breaking the law. And so I think it's a very dangerous one because no one deserves to throw away any of their life in jail because they were seeking to use a substance that probably doesn’t have a big effect on other people other than themselves.
Healthcare providers also acknowledged the difficulty which arose for AAS users due to the substances’ illegality. Harm reduction workers specifically referred to the additional challenges for AAS users wishing to seek help. P8 [NSP Coordinator]: The illegality of steroid use would be a factor in terms of people not getting help. P12 [NSP Coordinator]: They’re doing something that's illegal as well, so that can be a bit of a deterrent for going and asking for extra help. P16 [GP]: Those laws push the supply and the dosing and the control underground, and so they remove it from general medical care. And I know that doctors are scared to engage on the issues of steroid use.
Theme 2: criminality, stereotypes, and social dynamics: the “double-edged” nature of peer networks
Participants emphasised the discrepancy between the moral judgement imposed on them due to their use of AAS and their own self-perception. They drew attention to the negative portrayal of AAS users in popular media, which influenced public perceptions. Contrary to outsider attitudes, participants advocated for AAS consumers, highlighting their collective pursuit of self-improvement across various life domains, with physical appearance being just one aspect. They also underscored the presence of a supportive community among AAS users. P23 [AAS User]: We aren’t doing anything wrong. They just make us [AAS consumers] out to be so bad. It isn’t like that at all. Most of us, the large majority, are just seeking to better themselves. Like, in all aspects of life. Most of us have a community around us … we are a good community. P7 [GP]: Many of the young men who use steroids … many of them know each other and they are very much like a group.
Other providers also mentioned the positive influence of a supportive community on AAS initiatives. They indicated that the presence of a peer network can facilitate rapid learning and provide guidance for individuals navigating the complexities of AAS use. P8 [NSP Worker]: By having a community around them, the ones who have just started [AAS use] will learn quickly. P4 [AAS User]: I guess ‘cause you’re doing something wrong for starters and then you go asking questions and they start asking questions too. So I [think] just that's the biggest reason why. You’re looking at who you actually can trust which is mates [AAS-using peers]. Cause they have just done it before, which is, you know, they aren’t doctors and no one really. They’ve just done a course before and yeah, I guess you should find out yourself when you do it, you learn from your mistakes.
Other participants echoed strong narratives surrounding their own experiences of criminal justice and corrections through AAS networks of use. They believed the networks associated with AAS use came with a number of stressors which were all linked with the punishments which could eventuate from their use. They first mentioned stress arising from sourcing the illegal compounds, often associated with actors involved in these criminal networks. P13 [AAS User]: There is stress that comes with it, because not only it's illegal, for one. So you’ve got to get it … you’ve got to find it … and then that's a stressful process in itself. Usually the guys that you’re getting this stuff off aren’t the most savoury characters. You don’t really want to be hanging around them. P13 [AAS User]: I’ve been caught before. … I was living with a guy, and our house got raided because of him, and they found my stuff. I had to go to court, and I got a fine. That was really stressful in itself. And like, I didn’t feel like I was doing anything wrong – I was just using it for myself, for a performance sport. I know it's illegal, but it's not like I’m selling it or anything like that. But I mean now that was before I was class one, but now it's class [schedule] one … mate, it's illegal. It's like having meth [methamphetamine] or cocaine in your house. You know, it's just … and that again, that comes down to education.
Theme 3: secrecy, legality, and unmet health needs: implications for health engagement and education
Acknowledging that AAS are illegal substances meant that participants recognised that health engagement and public messaging were challenging. Harm reduction initiatives may have difficulty reaching their targeted population due to the need for secrecy directly linked to legality. AAS-using participants expressed that they and their peers were resistant to engage with initiatives due to police surveillance. P11 [AAS User]: At the end of the day, these are illegal substances so that's also tricky as well. To be able to publicly create something for them and then all of a sudden everyone's probably fearful about getting engaged because, like, what if the police are watching me?
For AAS users, engaging in and promoting harm reduction initiatives came with direct costs due to the secrecy and social punishment. For example, disseminating harm reduction resources around AAS could have social and economic disadvantages for participants. These types of social layers of substance use are not uncommon, however, and are directly impacting on users’ ability to engage with and share accurate health information being provisioned by researchers. P5 [AAS User]: It's hard to get it [harm reduction for AAS] out there because it's such a like I think people can’t be open about steroid use a lot of the time. Because it reflects very badly on them. Like for example myself, like I never deny it to anyone who asks me, but I won’t ever promote it either. I wouldn’t for example put it on social media or something like that because you sort of instantly, 4-5 people won’t look at you the same or will never do business with you.
There are also substantial medical and financial costs associated with openness regarding AAS use. Some AAS-using participants spoke of their AAS-using clients and peers who would not disclose their usage to healthcare providers due to the implications of that information being recorded and having legal consequences or contact with law enforcement. They also believed that, in consulting with a GP about their AAS use, they placed themselves at an increased risk of consequences at a later date. Interestingly, the spectre of “roid rage”, the idea that AAS consumption leads to dangerous fits of aggression, was present in this user's concerns. This maps onto research identifying a “narrative of harm” around AAS that some argue has been overstated to the detriment of the consumers themselves (Klötz et al., 2007; Mulrooney et al., 2019; van de Ven, Zahnow, et al., 2020). Interviewer: Is that the legal element? Like is that causing a problem for people to help seek? P3 [AAS User]: That's one thing he [his client] said. I said he [client] needs to go and disclose to a GP and say “hey, I’m looking at doing this [AAS]. What do you think?” Am I safe? He said he doesn’t want [AAS use] on his record because if anything ever comes out like or you lose your s**t then they’re privy to that. That held him back from seeking a lot of things … having it on a record.
This barrier resulted in direct and extreme harm to AAS users. Upon choosing not to discuss their use with a healthcare provider, AAS users are at risk of making poorly informed and, at times, drastic decisions. P3 [AAS User]: Anyway, he upped everything [AAS]. Doubled it for two weeks. Blew his heart out under 30.
As a result of AAS being conceptualised as a legal issue rather than a health concern, users also discussed the perceived consequences that peers believed could occur. For example, some feared disclosing their AAS use to their GP in the event that the healthcare provider informed the police of their criminal activity. P10 [AAS User]: I don’t think they’re aware, like, people aren’t aware of, you can tell your doctor that [AAS use] and the police aren’t going to rock up at your door. … I think somehow their doctor is going to dob them in.
Healthcare providers were also unsure of how to support AAS-using patients. This hesitancy could be directly linked to the criminality surrounding AAS use. GPs discussed the difficulties arising for them supporting and monitoring AAS-using patients from an ethical and legal perspective. P16 [GP]: Yes, as a GP, not knowing where the line is as to, are you supporting this person in doing the illegal activities or not?
Participants emphasised the importance of education and increased opportunities for knowledge about AAS use for consumers. Consumers advocated for open discussions and a more informed approach to understanding AAS use, highlighting the significance of education as a means to dispel misconceptions and promote responsible practices. P18 [AAS User]: There needs to be more education, more opportunity for education. A pathway to break down the taboo of the conversation of it as well. P22: [NSP Worker] I think particularly the steroids, it would just be nice to have some sort of public health response that meets user's needs, keeps them safe.
Discussion
This study investigated how AAS users, and the healthcare professionals in Australia who interact with them, perceive the impact of the criminalisation of AAS on users’ health outcomes and help-seeking behaviours. Our data suggest that the role of criminality in AAS user's decision-making is significant and healthcare providers alike are aware of the barrier which the criminal element represents. The findings indicate the challenge which arises from the perception of punitive measures surrounding AAS use in Australia, leaving users and healthcare providers unsure and fearful to engage. The laws in Australia also seem to have pushed AAS further “underground” and have therefore reduced medical oversight and increased the likelihood of users engaging with actors from criminal networks. Users often resist seeking help due to the potential for legal ramifications and instead engage with peers and those with shared lived experience in illegal activities. AAS consumers and the workforce who encounter them call for public responses centred on health. This underscores the complexity of AAS users’ experiences within the context of legality.
These findings can be situated within the new materialist drug studies framework (Dennis & Farrugia, 2017) and, more specifically, what Hupli (2023) refers to as the politicogenic drug effects of certain substances. Put simply, Hupli employs a critical drug studies perspective to argue that chemical substances (in our case AAS) and how they are regulated (criminalised) co-create certain social networks, relationships, and practices for users and society at large (Müller & Schumann, 2011; Pienaar et al., 2020). As such, following Whyte et al. (2002), substances like AAS are seen as having social lives and “material” consequences as well as their chemical effects. AAS can therefore be understood as “pharmaceutical technologies” (Hupli, 2023) that ought to be examined outside of the good vs. bad/legal vs. illegal dichotomy (Askew & Williams, 2021). Prudent to understanding our data, Hupli employs the term politicogenic drug effects to describe how policy and legal decisions regarding the treatment of pharmaceutical technologies like AAS often result in proportionally more harm for users than the substances themselves. This has been evident throughout this article, as we have argued that the Australian government's politicised decision to criminalise AAS has resulted in a fear to ask for help, pervasive stress regarding potential criminal sanctions, and a subsequent unwillingness to engage with health practitioners. Notably, these outcomes are the result of the “social lives” of AAS rather than the harmful pharmaceutical effects (which we acknowledge are also present) and therefore emanate from the political landscape of AAS regulation, rather than individual's risky health behaviours. Furthermore, the problematic reliance on peers identified above speaks to the politicogenic effects of pushing users into insular, non-cooperating communities. If AAS were not criminalised, we suggest that such practices, though still present, would not hold the significance that we identified under current legislation. Notably, stigma's comprehensive impact on individuals using AAS can hinder their engagement with services, particularly in settings shared with opioid and stimulant injectors (Simmonds & Coomber, 2009). In the United Kingdom, AAS users seek non-judgemental service environments like “steroid clinics” due to their understanding of AAS use, and these clinics, offering more interventions, might better maintain contact with users compared to needle exchange programmes, where AAS users have fewer visits (Kimergard & McVeigh, 2014b). The criminalisation of AAS use significantly magnifies these challenges, even in countries where personal AAS use is legal, stigma and fear remain prominent concerns (McVeigh & Bates, 2022; McVeigh et al., 2022). Our data suggest that if personal AAS possession were legalised, stigma-related barriers might lessen, although the nuances of stigma and other challenges could still persist.
Ultimately, due to the politicogenic drug effects of Australia's regulation of AAS, users are hesitant to engage with harm reduction strategies which target them. This lack of health engagement can have devastating, and wholly avoidable, consequences for AAS users’ health. Furthermore, public health messaging regarding AAS and relevant education initiatives for healthcare providers are somewhat undermined. Without addressing the elements regarding these illegal behaviours or providing clear direction, AAS users are left afraid and unprepared while the workforce who serve them are unequipped to assist. We call for considerations around the revision of drug and criminal justice policies based on these findings. Further research should be mobilised to consider what reclassification of these substances may require, more thoroughly, within the drug policy sector. A feasible recommendation involves aligning Australia's AAS classification with the UK's Class C framework, aiming to destigmatise use and promote harm reduction. This shift could focus on decriminalising personal possession, while maintaining control over distribution and supply, drawing insights from the United Kingdom's approach. This transition would necessitate thorough research to assess its impact on public health, user behaviour, and harm reduction goals. Upon considering these insights, we argue that a revision of AAS classification under state law, exemplified by Queensland's approach, could prove instrumental in fostering harm reduction and promoting help-seeking behaviours within the AAS user community. Considering that New South Wales similarly introduced legislation due to apprehensions about the impact of illicit AAS use on male behaviour and masculinity (James & Wynn, 2022), the revisions tested in Queensland may potentially serve as a precedent for other states (such as NSW) if proven effective.
Given the established and emerging presence of AAS in Australia, particularly Queensland, these data provide insight into a rapidly evolving area. Notably, in 2015–2016 Queensland accounted for the greatest proportion of national steroid arrests (54.4%), followed by Western Australia (19.7%), New South Wales (12.2%) and Victoria (7.4%) (van de Ven, Dunn, et al., 2020). In Australia, on average, 44,904 offenders are detected with a principal offence of any illicit substance use/possession each year and 55% of offenders are diverted by police away from the courts (Hughes et al., 2019). As a result of policy differences in programme design and implementation there are state and territory discrepancies, including the absence of drug diversion for use/possession of drugs other than cannabis in Queensland. However, the Queensland Illicit Drug Court Diversion Program targets illicit drug possession specifically. Given that there are currently no diversion programs available for AAS consumers, the provision of specifically targeted programs may ensure more equitable representation for this unique group of substance consumers. These programs could encompass multifaceted approaches, including educational modules aimed at enhancing awareness and understanding of the legal and health ramifications associated with AAS use. Additionally, harm reduction initiatives could be integrated, providing users with evidence-based strategies to mitigate risks (e.g., safe injecting and post-cycle therapy strategies). Support networks involving healthcare professionals, counsellors, and peer groups could be instrumental in aiding AAS users in making informed decisions and seeking help. The acknowledgement of this unique group is all the more important given Queensland's unofficial moniker as Australia's “Steroid Capital” (CCC, 2016).
The study underscores that changing legislation to reduce stigma around healthcare engagement among AAS users is important, but equally essential is the enhancement of healthcare providers’ knowledge and skills in addressing AAS-related challenges. This multi-pronged approach highlights the need for a comprehensive strategy to address the health needs of AAS users, recognising that legal changes alone will not suffice. For example, among AAS injectors, almost 60% had recently used psychoactive substances and were significantly younger, less educated, and more likely to have experienced redness at an injection site in the previous 12 months (van de Ven et al., 2018). AAS injecting is associated with a range of side effects, such as elevated blood pressure, reproductive issues, and the transmission of blood-borne viruses such as hepatitis C (McVeigh et al., 2021; van de Ven et al., 2018). Recently, an e-module has been implemented for the healthcare provider workforce which provides credible evidence-based resources to support their knowledge around AAS (Atkinson et al., 2021). Reflecting on the study findings, the authors acknowledged that the development of interventions should include the voices of both the workforce and those using AAS, and that careful consideration is given to the various factors that may act as barriers to effective implementation. Notably, numerous healthcare practitioners participate in delivering healthcare to illicit drug users, yet there exists substantiated evidence indicating that certain professionals exhibit stigmatising attitudes (Butler & Sheridan, 2010). In Australian samples, healthcare professionals operating within general healthcare contexts perceive the provision of care to individuals with drug and alcohol-related issues as a challenging and disagreeable endeavour (Happell & Taylor, 2001; Pinikahana et al., 2002), and this attitude extends to those who use AAS (Dunn et al., 2023; Jacka et al., 2020). Upon drawing these data together with existing work, the challenging nature was echoed in the present data, often framed as an element of “fear” expressed by healthcare providers. Further extensions of these types of online modules may consider additional components which encompass elements of criminality and legality for both users and healthcare providers. Expanding on these e-modules could entail incorporating specific content related to the legal aspects and potential criminal implications of AAS use for both individuals and healthcare practitioners. This could involve detailed information on the legal status of AAS, potential consequences of possession or distribution, and guidance on navigating legal boundaries. Additionally, educational modules could address ethical considerations, risk assessment, and proper communication with users about the legal dimensions of AAS use, equipping healthcare providers with comprehensive knowledge to effectively support their clients while adhering to legal parameters.
This research is not without limitations. Most notably, the study did not target the criminality and legality of AAS specifically, rather these components emerged as a discourse from participants. This occurrence is both a strength and limitation. Future studies should consider targeted investigations of AAS users and other service providers to interrogate this issue more specifically. It is noteworthy that the findings predominantly emphasise the broader implications of the illegality of AAS rather than focusing specifically on the associated legal sentencing. While the study does not extensively delve into the legal consequences, it effectively highlights the multifaceted challenges and barriers posed by the illegal status of AAS, encompassing difficulties in seeking help, engaging with healthcare providers, and accessing harm reduction initiatives. Additionally, the study's findings are rooted in a specific sample of AAS users and healthcare providers in Australia, which may impact the generalisability of the results to broader populations or different contexts.
Conclusions
This study represents the first work to explore the broader implications of the criminality which surrounds AAS in an Australian context. These findings, which we have interrogated with reference to the concept of politicogenic drug effects, suggest that the role of AAS criminalisation is significant for users and providers alike. Consequently, this study urges policy reconsideration and emphasises the need for targeted harm reduction interventions. The potential reclassification of AAS aligning with the UK's Class C framework emerges as a promising strategy to mitigate harm. Such a shift, coupled with tailored programs and educational modules, could destigmatise use and empower users to make informed choices. This approach also holds the potential to reshape the healthcare landscape, equipping providers with comprehensive knowledge to offer effective support while navigating legal boundaries. This research's ripple effect extends beyond users to healthcare providers. The integration of legal dimensions into healthcare education is pivotal for fostering a nuanced understanding among practitioners. E-modules addressing criminality and legality can empower providers to navigate these intricate waters, fostering an environment conducive to optimal care and harm reduction. In essence, this study urges a paradigm shift—from punitive measures to health-centred responses—fostering a more compassionate and informed approach to AAS use in Australia.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.