
Abstract


It is estimated that the person with diabetes spends less than 1% of their life with their health care team and therefore, by default, is self-managing their condition during the remaining 99% of the time spent on their own, away from the care team (see Figure 1). 1 According to the American Diabetes Association (ADA), diabetes self-management education and support (DSMES) “addresses the comprehensive blend of clinical, educational, psychosocial, and behavioral aspects of care needed for daily self-management and provides the foundation to help all people with diabetes navigate their daily self-care with confidence and improved outcomes.” 2 The DSMES national standards recommend that DSMES services include activities that support people with diabetes (PWD) to implement and sustain self-management behaviors and strategies to improve diabetes and related cardiometabolic conditions and quality of life on an ongoing basis. 1 This may include the involvement and support of family members, caregivers, and peers. Although the final “S” in DSMES stands for “support,” it can be challenging to incorporate as part of DSMES services in its existing structure. In addition, the support provided is often more medical in nature and does not address the 99% of time spent self-managing away from the clinical care team. We propose the synergistic integration of peer support services in an ongoing manner to complement DSMES services.
Diabetes is largely self-managed (blue) relative to time spent with their health care team (white). Adapted from: https://www.researchgate.net/figure/Fig-1-Symbol-representing-peer-support-offered-by-the-DOC-courtesy-of-the-Diabetes_fig1_275361264.
Not New, but Tried and True: Early Origins of Peer Support and Emergence in Diabetes Care and Structured Programs
Peer support is not a new concept, tracing its roots back to late 18th-century France, when Jean-Baptiste Pussin employed recovered patients to assist with care, promoting the therapeutic value of shared experiences. 3 In 1909, Clifford Beers, based on his personal experiences, founded the National Committee for Mental Hygiene in the United States, advocating for peer-led mental health recovery. 4 In 1918, Dr Elliott P Joslin published A Diabetic Manual for the Mutual Use of Doctor and Patient, emphasizing education and shared management among people with diabetes. 5 In 1934, Dr RD Lawrence, a British physician with diabetes, cofounded the Diabetic Association (now Diabetes UK), promoting peer support and patient advocacy. 6
From informal roots, peer support evolved in the late 20th century into structured programs designed to provide continuous education, psychosocial encouragement, and empowerment. 7 Integration into DSMES services has demonstrated improved health outcomes and enhanced engagement, especially in underserved populations. 8 DSMES services integrating peer support are cost-effective, improve glycemia, encourage self-care, support mental well-being, and reduce hospitalizations, leading to cost savings and thus aligning well with value-based care models. 9
Peer support may be particularly relevant for women because women experience 25% worse health outcomes compared to men. Their symptoms are often dismissed, leading to delayed care and feelings of isolation. 10 Between 2023 and 2024, discussions on women’s health on Reddit increased by 37%, indicating that women are seeking health information from nontraditional sources and seeking peer validation and community. 10 This points to the need for integrating peer support services with formalized DSMES services.
DSMES and Peer Support: Distinct but Complementary
DSMES is structured, evidence-based, and provided according to national standards by credentialed professionals, typically the diabetes care and education specialist (DCES), in person or virtually and/or through digital health platforms. 1 Multiple professional groups representing multifaceted disciplines in a consensus statement identified 4 critical times when DSMES should be provided, including at diagnosis, annually (or more often if needed to achieve goals), when complicating factors occur, and during life and care transitions. 11 DSMES includes education and skill building around the Association of Diabetes Care and Education Specialists’s (ADCES) ADCES7 Self-Care Behaviors: healthy eating, being active, monitoring, taking medications, reducing risks, problem-solving, and healthy coping. 12 However, despite evidence as to its clinical efficacy and cost-effectiveness, 13 DSMES is underutilized, with fewer than 5% of Medicare beneficiaries with diabetes and fewer than 7% of privately insured people with diagnosed diabetes participating in covered DSMES services.14-16 The ADA and the ADCES strongly advocate for all individuals with diabetes having access to this critical service proven to improve health outcomes. 1 DSMES services can and should be incorporated in evolving models of care, including accountable care organizations, patient-centered medical homes, population health management programs and services, and value-based payment models, with a shift toward a continuous, data-informed approach to provision of services.
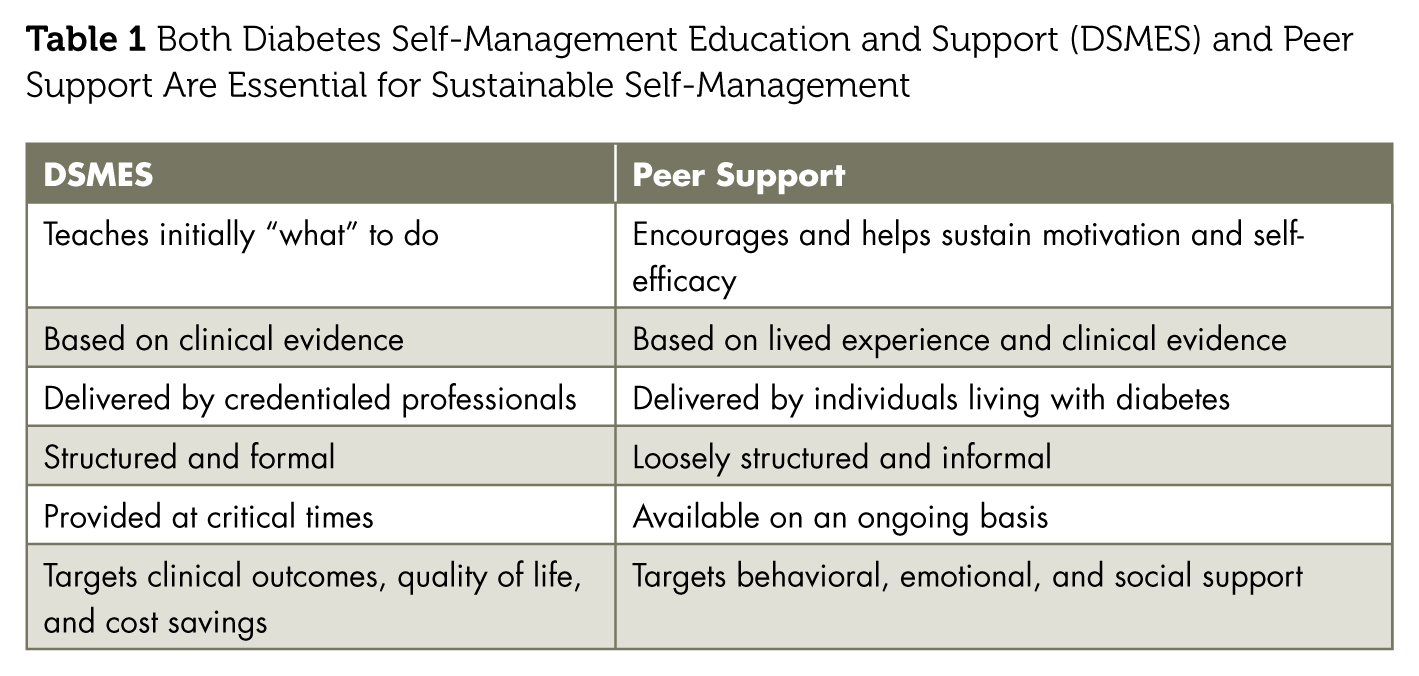
By contrast, peer support is delivered in flexible formats (in person, online, text, phone, apps, etc) and includes evidence-based methods. This offers intentional variety, meaning individuals seek the type and kind of support they need at different times in their journey. Peer support offers emotional and practical support, social connection, and behavior modeling and can help in reducing diabetes distress and burnout and enhancing self-management support.17-19 Table 1 delineates the differences demonstrating the complementary nature of DSMES and peer support. Peer support can help fill in the gaps between clinical encounters and education sessions.
Both Diabetes Self-Management Education and Support (DSMES) and Peer Support Are Essential for Sustainable Self-Management
Combining DSMES and Peer Support Leads to Improved Glycemia, Improved Quality of Life, and Lower Health Care Costs
Although initial DSMES is necessary, it is not sufficient for sustaining a lifetime of diabetes self-management, with initial improvements in outcomes diminishing 6 months after conclusion of the intervention. 1 Peer support enhances DSMES impact, especially at transitions and posteducation drop-off points.17,18 In a systematic review, researchers found DSMES integrated with peer support effectively enhanced glycemia in people with type 2 diabetes, with programs with smaller participant groups, shorter interventions, weekly meetings, and closed group sessions the most effective. 20
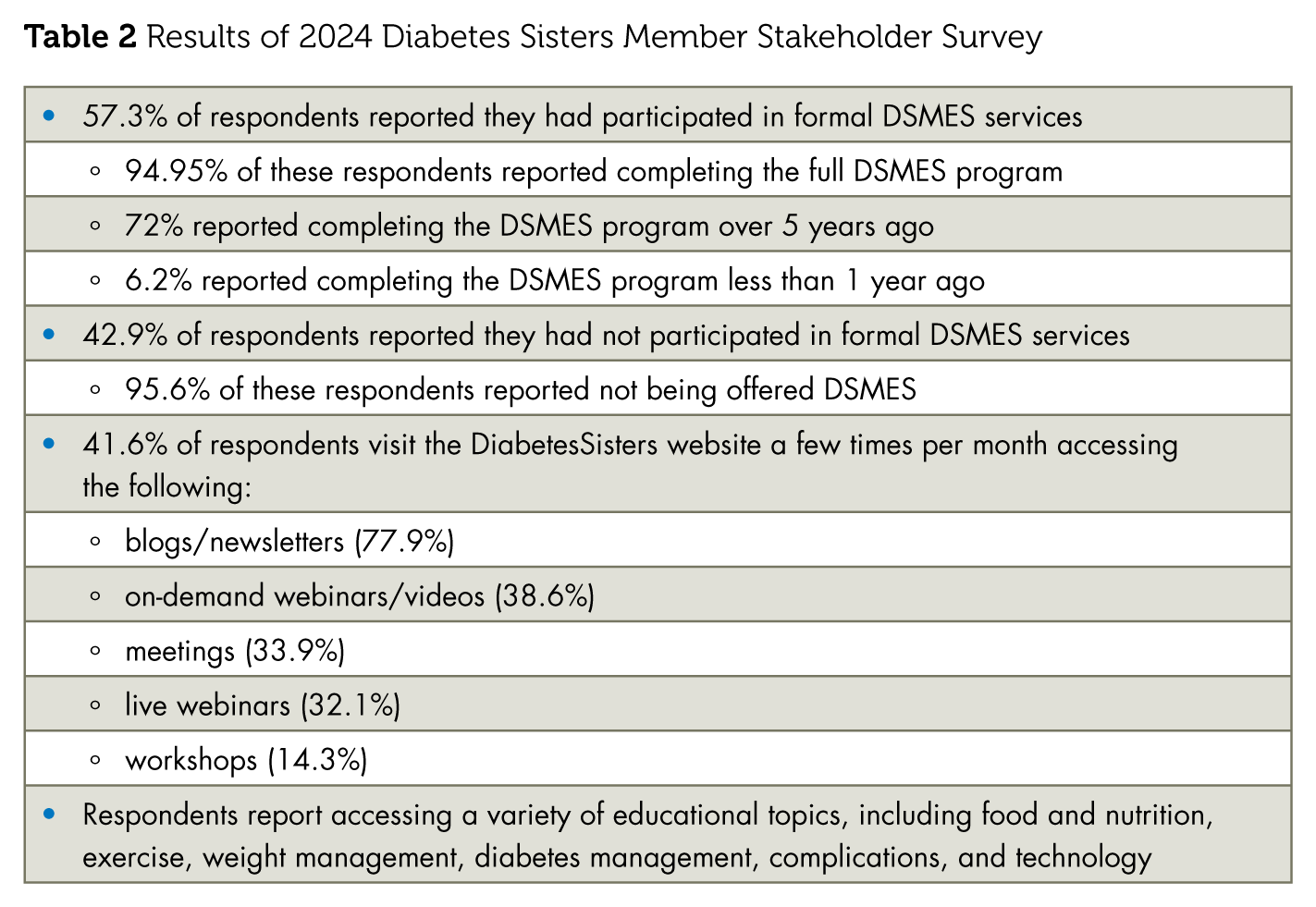
DiabetesSisters is a peer support community for women with or at risk for diabetes offering multiple pathways for engagement for members. DiabetesSisters is a value-based peer support model supported by quantitative and qualitative research. Data generated through this model demonstrates the value of peer support as a complement to DSMES services. An annual survey is conducted among stakeholders and members of the DiabetesSisters Community. Results of the 2024 survey have been reported. Highlights of the survey are reported in Table 2 and suggest possible synergies of linking DSMES services with a peer support community like DiabetesSisters. It is noted that respondents to the survey are likely more engaged in their own health care and thus have a higher reported participation in DSMES services than reported nationally.
Results of 2024 Diabetes Sisters Member Stakeholder Survey
Reimagine DSMES: From Just in Case to Just in Time
DSMES interventions include activities that support people with diabetes to implement and sustain self-management behaviors and strategies to improve diabetes and related cardiometabolic conditions and quality of life on an ongoing basis. Because family members, caregivers, and peers can be an effective resource for ongoing support but often do not know how to help, it can be beneficial to include family members and caregivers in diabetes care, education, and support services. A pilot study investigated incorporating a peer supporter into the DSMES program and reported enhanced self-management capability in following the diabetes treatment plan. 21 Other sources of ongoing support could include referral to local community-based organizations, community health workers, and informal and organized in-person and online peer support.
Connecting individuals with diabetes to technology-enabled solutions, such as connected devices, mobile apps, digital therapeutics, online programs, and peer groups, in the local or online community can encourage practical integration of diabetes self-management and psychosocial support into the existing daily routine. 1 A growing suite of connected technologies enable people to gather data as they live their lives; AI-powered digital health platforms can integrate and analyze the data and provide personalized 24/7 coaching, supporting people as they self-manage their chronic conditions while away from the care team. 22 Clinicians can remotely monitor population-level data to assess the health of their populations, efficiently identifying who needs human intervention from the clinical care team and when, whether the intervention is a brief coaching nudge or reminder or an adjustment in therapy or behavioral, peer, or social support. The clinical team interacts with individuals in a continuous feedback loop,23,24 shifting from providing just-in-case education to providing just-in-time, data-informed education and support on a continuous (on-demand) basis where and when needed, including linking at-risk individuals to local resources and identifying and connecting to available peer support programs and resources.
The Diabetes Care and Education Specialist (DCES) Leads in Integrating Peer Support
The identify-configure-collaborate (ICC) framework is a standardized way to integrate diabetes technology into clinical practice. 25 The framework can be expanded to all aspects of diabetes care, including peer support. The DCES can lead in using the ICC framework to help people with or at risk for diabetes to identify and adopt the support and services that will best meet their needs and enable them to best collaborate and partner with their care team. To incorporate the ICC framework into developing a support plan, the DCES can do the following:
Figure 2 illustrates the potential synergistic integration of peer support services with DSMES. By establishing referral pathways, DSMES providers can direct participants to peer support groups for ongoing motivation and real-world insights, and peer support leaders can refer individuals back to DSMES programs for structured, personalized education when new challenges arise. This bidirectional referral system ensures that people with diabetes receive both clinical guidance and the emotional, social support they need for sustainable self-management. A case study from the perspective of a woman living with diabetes describes the impact of peer support with DSMES.
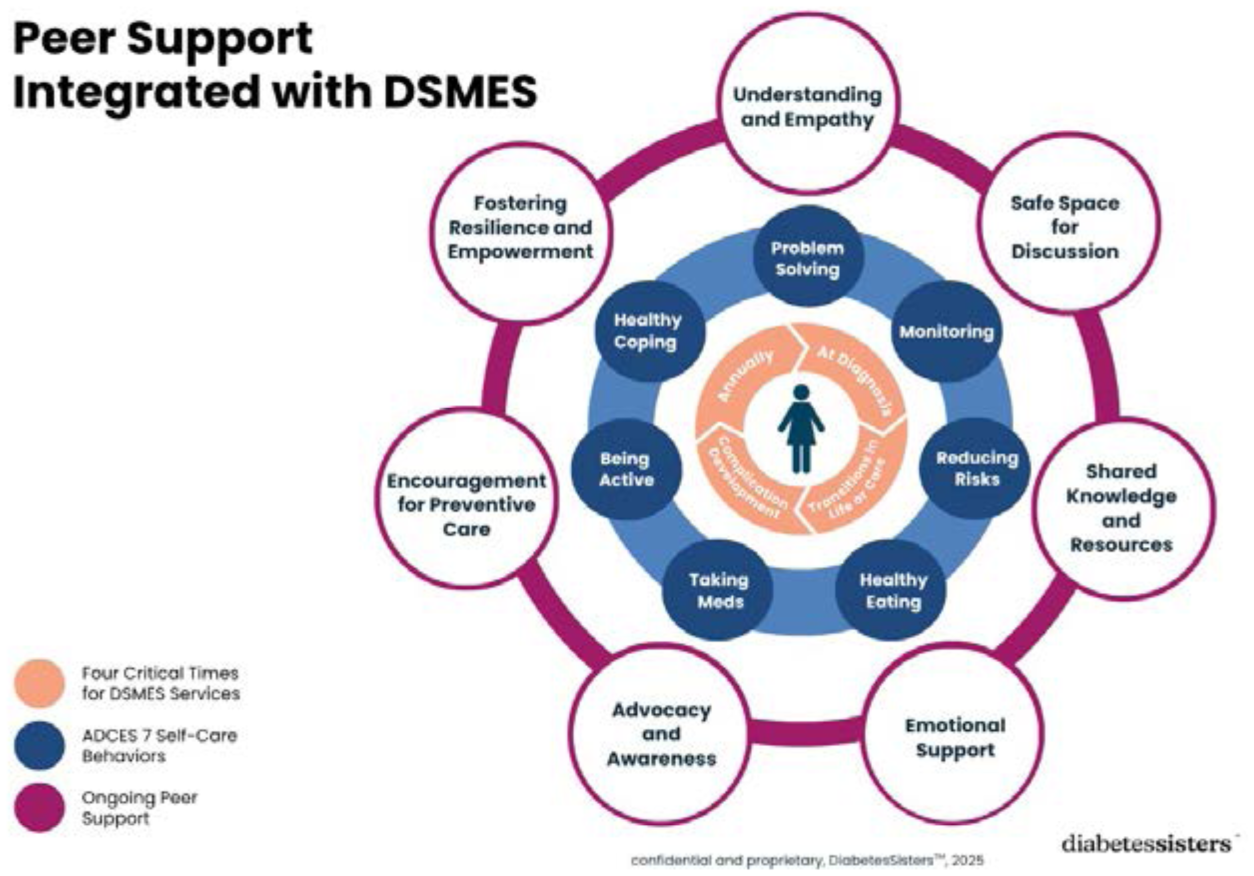
Peer support integrated with diabetes self-management education and support.
Case Study
Introduction
I am a 63-year-old woman who has lived with type 2 diabetes for more than 25 years and have found peer support to be the cornerstone of my self-management success.
History
I was diagnosed with type 2 diabetes at age 37. I regularly saw a certified diabetes care and education specialist (CDCES) for approximately 1 year after my diagnosis. During that time, I managed my diabetes with diet and exercise and did not take any diabetes medications. I lost 35 pounds within the first 9 months of my diagnosis and an additional 10 pounds since then. I attended formal diabetes self-management training (DSMT) at age 48 and attended a monthly diabetes support group run by my local health department for approximately 2 years after that. The support group continually reemphasized the concepts I learned during the DSMT, especially the importance of nutrition, exercise, and goal setting. I moved to a different state and did not have access to peer support again until age 55, when I met the CEO of DiabetesSisters at a diabetes advocacy event. She told me there had been a group in my area, but the leader had recently stepped down, and she offered to train me to run the group. I have been leading peer support meetings regularly ever since, both in person and online.
Medical Treatment and Social Support
Although I began taking metformin approximately 5 years after my diagnosis and a GLP-1 medication approximately 10 years after that, I credit peer support for my continued success managing the chronic disease I have lived with for more than 25 years. I only see my endocrinologist twice a year, but I have to manage my diabetes every hour of every day. Peer support has provided me with practical tips for managing my diabetes and emotional support that I do not get from my health care professionals (especially those who do not live with diabetes themselves).
When I started on the GLP-1, I had a lot of problems with morning nausea. My doctor said, “Yes, that can be a side effect.” But someone in my peer support group said, “You might want to try eating very small meals and drinking plenty of water.” The doctor didn’t really offer any advice that helped alleviate my nausea, but the suggestion from my peer worked.
The food tips and recipes I get at our meetings are the best. For example, protein pancakes made with rolled oats, cottage cheese, and eggs are now one of my go-to breakfasts. I make extras and freeze them for a quick morning meal when I am rushed. A dollop of plain yogurt and some fresh berries are all I need to add.
Because of peer support, I now understand the impact that stress and sleep have on my blood glucose numbers. Previously, I blamed my food choices and beat myself up about it even when it did not make sense. Now I know several stress management techniques and have developed a bedtime routine that helps me consistently sleep better. And I probably would not be using a continuous glucose monitor, which is the most positive thing I have ever done for my diabetes management, if I had not heard others in my peer support group talk about its benefits. Even though I lead the group, I leave each meeting feeling motivated and confident that I can continue to improve my diabetes self-management. I learn something new each time we get together.
Value of Peer Support
Having access to health care providers, accurate medical information, medications, and tools is important for understanding diabetes, but peer support is critical for successful day-to-day management of the condition.
Conclusion: A Call to Action
Diabetes is a disease managed overwhelmingly outside the walls of clinical settings, with individuals self-navigating the daily complexities of their health nearly 99% of the time. 1 Although DSMES offers a structured, evidence-based foundation for self-management during 4 critical times, 11 this traditional model often falls short of sustaining behavior change and motivation over the long term. Peer support, by contrast, provides an accessible, flexible, and ongoing source of encouragement, validation, and shared experience. From the earliest diabetes education manuals to present-day community-based programs, peer support has consistently demonstrated the power to improve glycemia, reduce distress, and lower health care costs, particularly when integrated thoughtfully alongside professional care. 9
To truly reimagine DSMES for the realities of daily life, we propose a model that moves from “just-in-case” education, delivered episodically, to “just-in-time,” data-informed education and support woven into daily life. Combining credentialed DSMES services with structured peer engagement leverages the strengths of both approaches: the clinical rigor and individualized goal setting of DSMES with the lived wisdom, social connection, and sustained motivation that peer communities uniquely provide. This continuous feedback loop—enabled by technology, facilitated by DCESs and enriched by community partnerships—has the potential to redefine self-management support as an accessible, empowering experience that meets people where they are whenever they need it most.
Now is the time for a call to action:
Explore and make a list of available peer support communities and services that are accessible to the populations your clinical practice serves, such as DiabetesSisters (DiabetesSisters: Diabetes Non-Profit Organization for Women). Remember to include online services, too.
Incorporate the ICC framework into your DSMES services to ensure a systematic approach to offering support opportunities.
Provide information to the identified peer support communities/services regarding the DSMES and medical nutrition therapy (MNT) services your clinical practice provides, including how and when members of the community can be referred to your services.
Create a 2-way feedback loop between your DSMES/MNT services and peer support resources to maximize access to the benefits of both services with the goal of improving the health and well-being of people with or at risk for diabetes.
Let’s reimagine DSMES by systematically integrating peer support to ensure those with or at risk for diabetes are set up for success! ■
Footnotes
Author Contributions
JM and DS conceptualized and outlined the manuscript. JM wrote and edited the manuscript. DS and DG reviewed and edited the manuscript.
Declaration of Conflicting Interests
JM, DR, and DG serve on the DiabetesSisters Research Committee; DR is Chief Operating Officer of Diabetes Sisters; DG is an employee of Dexcom and Chair of the Board of Directors of DiabetesSisters.
Guarantor Statement
All coauthors have made a substantial contribution to the design and drafting of the manuscript and have reviewed and accepted the contents of the manuscript prior to its submission.