
Abstract
Lack of access to health care in rural communities is a multifaceted challenge that often leads to unfavorable patient outcomes and impacts people with diabetes, providers, payers, and the health care system as a whole. 1 In the United States, from 1999 to 2018, approximately 20% more adults with diabetes lived in rural than in urban areas, likely contributing to increased diabetes-related complications and mortality rates in rural areas when compared to metropolitan areas. 2 Factors that led to an escalated mortality rate are a shortage of health care providers, a lack of specialty resources, and the absence of preventive screenings. 3 In recent years, access to health care in rural areas has notably declined. As of 2022, approximately 65% of all primary care shortage areas were in rural locations.
Presentation of the Significance of the Problem
An estimated 38 million Americans have diabetes, and an additional 98 million adults have prediabetes, reflecting that diabetes care is in high demand nationally. 4 When analyzing the trend between adults diagnosed with diabetes and ethnicities, American Indians and Native Alaskans led, with 13.6% of their population having been diagnosed, 5 followed by African American adults at 12.1%, Hispanic adults at 11.7%, Asian adults at 9.1%, and White adults at 6.9%. The prevalence of diabetes is slowly rising each year, with a more rapid increase found in low- and middle-income areas. Diabetes disproportionately affects low-income populations due to their inability to afford preventive health screenings and limited healthy food availability. 6 Seeing that 1.5 million deaths globally are attributed to diabetes, access to diabetes maintenance, comorbidity management, and diabetes self-management education and support are a necessity. 7
In people with diabetes, the absence of health care is just one of many contributing factors to glycemic management not within target, increased comorbidities, and hospital visits. In addition, potential complications, such as stroke, myocardial infarction, kidney disease, and atherosclerosis, are often a result of unmanaged diabetes. 8 Therefore, it is significant to have regular diabetes care and education to ensure quality of life and decrease the risk of complications. With the declining number of rural providers, diabetes has become a common admitting diagnosis in hospitals. With over 78 million diabetes-associated hospitalizations in the United States from 2010 to 2019, diabetes is a leading component in the oversaturation of hospital emergency rooms. 9
Recommendations for Telehealth Practice
Two recommendations to ensure high-quality telehealth visits are for the patient to have a continuous glucose monitor (CGM) device and video monitoring available for telehealth calls. These additional accessories help eliminate the geographical barrier between the physician and patient, promoting patient engagement and rapport. 10 Although these recommendations are proven to improve the quality of care for the patient, they are costly, making them difficult to obtain.
Technological advancements have allowed for additional opportunities to obtain medical care. Telemedicine has created a pivotal role in health care that offers a multitude of services via video or audio-only calls. 11 Utilizing video has many advantages, such as permitting the physician to evaluate the patient’s understanding of medication administration through the teach-back method, which has proven to improve patient medication management. 12 Remarkably, 86% of physicians prefer video during telehealth so they can accurately examine patient skin, range of motion, gait, and so on. 13 Although providers prefer telehealth, it is not always feasible for the rural population due to the lack of broadband internet and insurance restrictions. In 2021, the Federal Communications Commission (FCC) estimated that a minimum of 9.3 million rural residents have inadequate broadband internet service. 14 Telemedicine utilization differs based on geographical area due to the significant difference in internet availability. It is found that metropolitan areas use telemedicine 40.2% of the time for medical visits, whereas rural areas only use telemedicine 29.7% of the time. 15 Another barrier to the use of telehealth is the lack of reimbursement and licensing/malpractice coverage and the lack of health care coverage for telehealth encounters. 16 Although these barriers exist, there is ample evidence that telehealth encounters improve glycemic management. For example, it is conferred through a metaanalysis that A1C levels improved 0.6% in patients with type 2 diabetes. Additional nonglycemic outcomes include improved blood pressure management, body weight maintenance, and improved health literacy through education. 17 A 12-month nonrandomized trial of patients with a A1C >9% was referred to the Telemedicine for Reach, Education, Access, Treatment, and Ongoing Support program, where a diabetes care and education specialist provided services through videoconferencing. 18 Through this telehealth program, 64% of participants in rural areas achieved their self-management goal, including an average A1C decrease of 0.21% every 3 months. In addition to telehealth programs, CGMs have proven to have positive outcomes for people with diabetes. A recent systematic review found that CGMs are more effective at reducing A1C than standard insulin or on-insulin therapies, with a weighted mean difference of −0.43%. 19 Additionally, CGMs also reduce hypoglycemia in older adults with diabetes. 20 This in-real-time glucose reading allows the provider to have accurate trends of the patient’s blood glucose with time stamps, permitting improved glycemic management. These statistics highlight the importance of telehealth availability within rural communities to improve the outcomes in patients with diabetes.
Increasing Telehealth in Rural Areas
Although it is now established that telehealth can benefit the lives of patients with diabetes in rural areas, how do we implement telehealth in these areas of health care inequity?
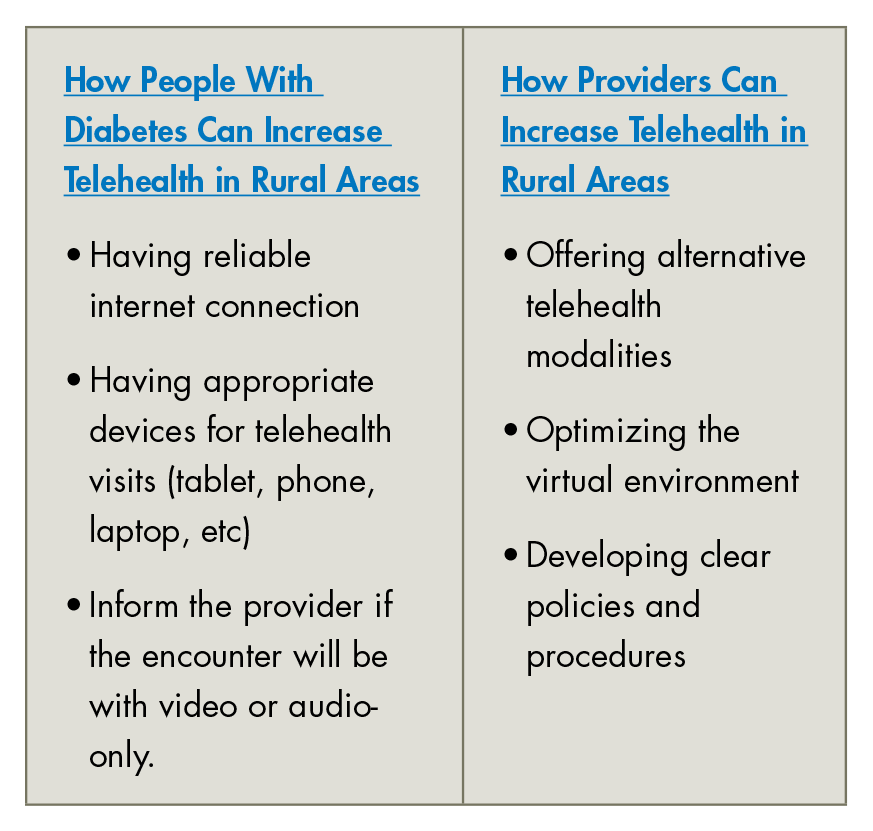
For the patient, increasing telehealth in rural communities focuses on ensuring reliable internet infrastructure and having appropriate devices for telehealth visits. To begin, the patient must have reliable internet. Reliable internet enhances the patient experience by clear and uninterrupted communication. Additionally, appropriate bandwidth speed ensures accurate and timely data transmission. How does one find affordable and reliable internet? In rural areas, finding an affordable high-speed internet provider is a challenge. The Lifeline Program, an FCC program, was created with the intent of extending digital services to low-income consumers, which includes those in rural areas. 21 Through this program, the consumer is given a discount on qualifying monthly phone, internet, or bundle of services when purchased from a participating provider. Eligibility for the Lifeline program is based on the consumer’s household income, which must be at or less than 135% of the federal poverty guidelines, or if they participate in federally funded assistance programs, such as the Supplemental Nutrition Assistance Program. Through this program, the digital divide can be minimized, and health care can expand. Find if you are eligible for the Lifeline program through: https://www.lifelinesupport.org/do-i-qualify/.
It is necessary to address technology difficulties by offering alternative telehealth modalities, optimizing the virtual environment, and developing clear policies and procedures. Offering different alternatives to video calls, such as audio-only calls, or messaging through an information-secure platform, such as a patient's portal, can create more opportunities to utilize telehealth by having different modalities. Audio-only telehealth visits or messaging are significant for patients who lack appropriate devices, internet availability, or technological competence. 22 Optimizing the virtual environment can be comparable to standards for in-person visits. This can consist of minimizing background noise and having optimal lighting. Additionally, testing telehealth equipment before the virtual appointment and having telehealth support on standby can be beneficial for a seamless encounter. 23 Lastly, policies and procedures for telehealth can consist of obtaining informed consent and establishing criteria for appropriate telehealth patients. Informed consent for telehealth should include limitations, advantages, disadvantages, and the possibility of internet disconnections. 24 Appropriate telehealth patient visits can include but are not limited to wellness visits, follow-ups on new medication or postprocedure, and medication refills. 25
Conclusion
The number of primary care shortage areas is expected to grow due to an estimated shortage of more than 100 000 physicians by the year 2030, which will have devastating effects especially on rural populations. 26 People with diabetes in rural areas are markedly underserved, which leads to higher mortality rates and complications than their urban counterparts. 27 The trend for telehealth gives those residing in rural areas an opportunity for diabetes self-management education and support and specialty care consultations. Increasing the recommendations for CGM use and video availability for telehealth visits create a substantial improvement, as evidenced by improved blood pressure management, weight maintenance, and improved health literacy through ongoing education. Although the benefits are notable, we must consider the barriers to these recommendations. These barriers consist mostly of financial concerns but also a lack of broadband internet availability and difficulty of reimbursement and licensing/malpractice coverage. Overall, telehealth has generated a remarkable improvement in patients with diabetes quality of life and patient awareness through modifying their diet, physical activity, stress management, and medication compliance. Over time, patient and provider efforts will coincide to improve diabetes management and the availability of care. 28 ■
Key Points
Rural populations are medically underserved, which has resulted in unmet glycemic targets in diabetes equating to 1.5 million annual deaths globally attributed to diabetes.
Health care disparities in rural areas are due to the lack of providers, unreliable transportation, decreased health literacy, limited healthy food availability, and financial barriers.
Telehealth in rural locations can have a pivotal role in health care that offers a multitude of services via video or audio-only call.
Two recommendations for high-quality telehealth visits are a continuous remote blood glucose monitoring device and video monitoring available for telehealth calls.
Footnotes
Acknowledgements
Troy and Janet Antley, Rascal Yates, and Della Connor for their unwavering support.
Author Contributions
The author researched data, wrote the manuscript, and reviewed/edited the manuscript.
Declaration of Conflicting Interests
None.
Funding
None.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request