
Abstract


As a person with type 1 diabetes and a CDCES, I have both personal and professional motivation for supporting person-centered language.
Nails on a chalkboard. That's how it sounds to me when people use words like "diabetic" and "noncompliant."
In 2017, the Association of Diabetes Care and Education Specialists (ADCES) and the American Diabetes Association (ADA) published a joint paper (https://journals.sagepub.com/stoken/default+domain/SYRQNKSEWGKXARZUSCIJ/full) calling for a shift from negative, judgmental language to supportive, person-centered language in diabetes care and education. In the years since that publication, many of us who specialize in diabetes care have become skilled in the use of person-centered language, but people with diabetes don't just speak with diabetes specialists. Those living with diabetes often interact with licensed professionals in other health care specialties when managing their diabetes, in addition to schedulers, receptionists, billing specialists, and many others in health care.
Professionals and support staff who do not specialize in diabetes may have never been exposed to the concept of person-centered language in diabetes care or to the literature supporting it. As a result, negative diabetes language is still present in health care, and therefore, the message about person-centered language must reach beyond just diabetes specialists. It needs to reach everyone in health care. But how do you change people's minds regarding something that has been part of the culture for decades?
As Certified Diabetes Care and Education Specialists (CDCESs), we need to use engaging teaching methods that speak to both clinical and nonclinical health care workers if we're to truly transform the language of diabetes care.
Through My Eyes
As a person with type 1 diabetes and a CDCES, I have both personal and professional motivation for supporting person-centered language. I know the impact of negative language on diabetes self-care because I've experienced it personally and I've heard it used with patients. I've also read clinical documentation, listened to continuing education courses, and sat in meetings with stigma-laden language.
Perhaps people use negative language because they're unaware of the problem, they don't fully understand the impact of negative language, or they simply haven't embraced the need for change. This further supports the need for education to promote and drive culture change and for teaching methods that go beyond sharing the research.
Teaching Through Storytelling
Storytelling has been used as an educational tool across cultures for centuries. It can be used to reach learners of all backgrounds and education levels, a big benefit considering the pervasiveness of negative language in diabetes care.
In a 2016 meta-narrative review, Rose and colleagues pointed to the value of storytelling in health care and found that it had the power to facilitate meaning-making, promote compassion and empathy in listeners, and support culture change. The same year, Lawrence and Paige described storytelling as a method for helping learners make connections between new concepts and past experiences, highlighting the relationship between storytelling and experiential learning. The connection to experiential learning was further detailed by Landrum and colleagues in a 2019 theory review. The authors described storytelling as a valuable pedagogical tool through which listeners can learn by relating the narrative to their own experiences.
Many of us already use storytelling in diabetes care and education. In group classes and support groups, we often facilitate the sharing of stories among participants. When promoting our services to health care providers, we may use deidentified case studies to illustrate the impact of diabetes care and education.
Often, the most effective stories come from the personal experiences of the storyteller, and many CDCESs either live with diabetes or have a family member with diabetes. This puts us in a position where our personal stories can be used as the impetus to help people in health care make sense of the need for supportive language, feel empathy and compassion for people with diabetes, and be active participants in this necessary culture shift.
Telling My Story
Driven by my own experience and my desire to help others embrace culture change, I chose to use storytelling as a teaching strategy for person-centered language. Having decided to tell my own story, I began by setting goals and learning objectives. My overarching aim was to change the way people in health care thought about the use of language in diabetes care. I hoped that listeners would be able to distinguish between positive and negative diabetes language and to demonstrate positive language in subsequent communication. It was also important for me to identify the learners and the context.
I mapped out the plot of my story and created a presentation. The story I shared was of myself growing up as a teenager with diabetes, the words I heard during those years, the feelings I experienced upon hearing those words, and the impact they had on my diabetes self-management. I used slides showing actual pictures of myself during my teenage years and the language that impacted me (Figure 1).

Juxtaposing the words with an image of myself as a teen highlights the impact of negative language.
Driven by my own experience and my desire to help others embrace culture change, I chose to use storytelling as a teaching strategy for person-centered language.
I spoke of my experience as a newly diagnosed teen and how it felt to be suddenly labeled as a "diabetic" and "noncompliant." I talked about hearing that my glucose numbers were "bad," my internalization of that word, and how it drove me to simply stop checking my glucose because I didn't want anyone to think I was a bad person if I had numbers in the 200s.
The conclusion of my story was the recounting of an interaction I had several years later with a CDCES who used positive and person-centered language and the beneficial impact her words had on me as a patient (Figure 2). I told the story of how she asked me about my challenges, acknowledged my self-care barriers, and explained that high numbers did not mean I was a bad person. She taught me about tools that could help me overcome the barriers I was facing and ultimately inspired me to become a CDCES.
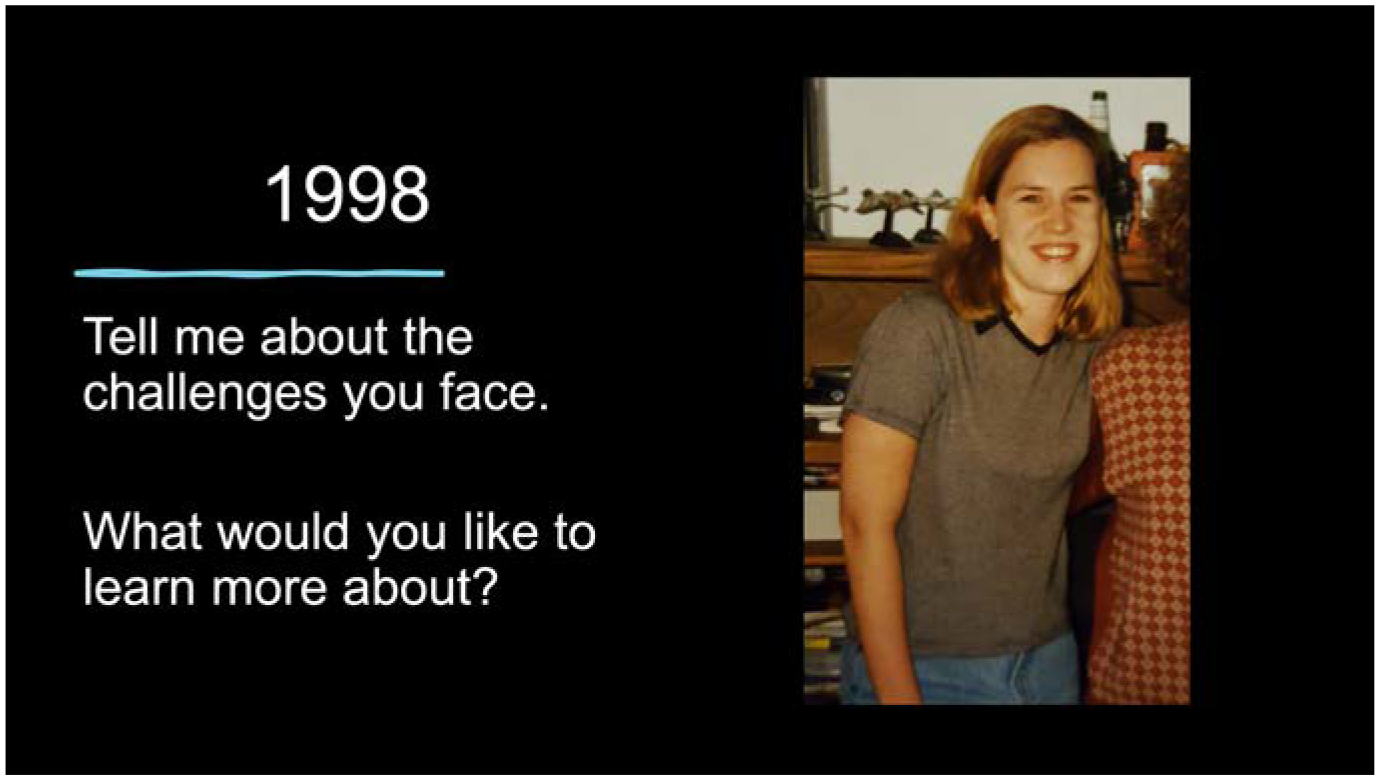
A positive ending can help inspire listeners and empower them to apply what they've learned.
I intentionally ended the story on a positive note for several reasons. First, by concluding with an example of person-centered language, I was able to demonstrate its power and impact. Second, my hope was that listeners would walk away feeling empowered to make a difference. An optimistic conclusion served as the stimulus. Finally, the positive ending was a transition to a call to action, where I asked listeners to consider how they speak to and about people with diabetes and to work toward improvements where needed.
Delivery Methods
When designing the delivery of the story, I chose to use a lecture format, primarily because of the expectations of each group leader and the limited time that was allotted for speaking to various groups—typically 30 minutes or less. I've shared my story in a variety of settings, including departmental staff meetings, shared governance meetings, and grand rounds. The lecture format was an accepted and standard teaching method in all these learning environments.
My preference was to deliver the presentation in person, but it was easy to transition to a virtual option when needed. Although not interactive until learner questioning was opened at the end, delivering the story as a lecture allowed me to tell it uninterrupted from start to finish, thereby maintaining the emotional impact.
Lessons Learned
I've told my story to diabetes specialists as well as clerical teams, clinical and administrative leaders, primary care providers, inpatient and outpatient nurses, clinical support staff, care coordinators, and even external payers. This has helped me understand how each of them interacts with people with diabetes and has allowed me to align my story with what I hoped learners will think, feel, and do after hearing it.
After several years, I've been able to fine-tune my use of storytelling as a teaching method. The following are key things I have learned that may help others who are interested in sharing their own stories.
Ensure sufficient storytelling time. It'll be more difficult to convey the emotion if you're rushing through it.
Allow discussion time. Whether discussions are in a small group or large group format and whether they are incorporated throughout the story or at the end, including time for questions and discussion can help presenter and listeners to process the information and learn from the perspectives of others.
Be prepared for emotion. I've seen listeners cry during my story many times, sometimes because they've experienced the same things. The storyteller's own emotions should also be considered. If the story is difficult to tell, practice is important.
Choose how transparent you want to be. Honesty was a critical component of telling my story, but honesty can increase vulnerability and decrease privacy. The storyteller must be comfortable with the amount of information they're sharing.
Get approval from others if necessary. Although HIPAA rules apply to patients, they don't apply in our personal lives. However, common courtesy dictates that it's best to check with those closest to us before telling a story publicly about them.
Have a structure to the story. It's easy to ramble when it's your own narrative, so plan it like any other story with a beginning, middle, and end.
Know your audience and adapt as needed. When I'm telling my story to licensed health care professionals, I often preface the story with a detailed discussion of the research pertaining to the impact of stigma in diabetes care. When I'm telling it to unlicensed professionals, I give a more basic overview of the evidence before proceeding with the story. If I'm speaking to people who don't have a clinical knowledge of diabetes, I may change how I describe some of the details in the story. For example, physicians will know what an A1C is, but when speaking with nonclinical people, I often just refer to "diabetes lab results."
It's Worth It
Telling my personal story about the impact of words on my diabetes self-management has become one of my favorite teaching experiences.
The emotion I see on the faces of the listeners while I'm telling the story is why I share it so freely. It's apparent that it means something to them, and I can see the beginning of the transformation. Almost every time I tell my story, I'm approached by at least one listener who asks me to tell it to another group. This has helped spread the message about person-centered language within my own organization, a necessary component of culture change.
I've told my story to diabetes specialists as well as clerical teams, clinical and administrative leaders, primary care providers, inpatient and outpatient nurses, clinical support staff, care coordinators, and even external payers.
By sharing my story, I can be a small part of a larger effort to change the mindset of people in health care. However, I know I'm not the only one. If you have a personal story to tell about the importance of person-centered language in diabetes care and education, consider sharing it. Together, we can work to transform the language used in diabetes care.
No more nails on the chalkboard. ■
Footnotes
Duality of Interest
The author declares having no professional or financial association or interest in an entity, product, or service related to the content or development of this article.
Funding
The authors declare having received no specific grant from a funding agency in the public, commercial, or not-for-profit sectors related to the content or development of this article.
Shannon M. Knapp, BSN, RN, CDCES, is with the Cleveland Clinic Foundation in Cleveland, OH.