
Abstract
Background
Inflammatory bowel disease (IBD) may be burdened by other comorbid conditions. We herein sought to assess comorbidity in hospitalized and non-hospitalized IBD patients.
Methods
This was part of the San MAtteo Complexity (SMAC) study (2017–2019). Data of hospitalized IBD patients were compared to gender- and age-matched IBD outpatients in a 2:1 fashion. The association of comorbidity in relation to hospitalization and clinical and socioeconomic factors was assessed.
Results
We included 104 patients, 27 hospitalized (median age 49 years, IQR 32-70) and 77 outpatients (median age 54 years, IQR 37-68). Comorbidity was reported in 63/104 patients (60.6%), of whom 45 (58.5%) non-hospitalized and 18 (66.6%) hospitalized. Patients with comorbidity were older (median 60 years, IQR 44-61 vs median 40 years, IQR 28-50 vs; p<0.001), had a higher Cumulative Illness Rating Scale severity index (median 1.85, IQR 1.5-2.5 vs median 1.31, IQR 1.2-2.5; p=0.002), were more commonly female (37, 60.7% vs 14, 35.0%; p=0.01), frailer (14, 22.2% vs 1, 2.4%; p=0.004), and had a lower educational level (13, 20.6% vs 2, 4.9%; p=0.04). In a bivariable analysis, factors associated to comorbidity were age >65 years (OR 5.30, 95% CI 1.81-15.55; p=0.002), female sex (OR 2.92, 95% CI 1-27-6.71; p=0.012), income <1000€ (OR 3.04, 95% CI 1.09-8.44; p=0.033), schooling <8 years (OR 5.09, 95% CI 1.08-23.96; p=0.039), frailty (OR 12.56, 95% CI 1.48-106.45; p=0.020), and polypharmacy (OR 10.41, 95% CI 1.85-59.38; p=0.008).
Conclusion
A high prevalence of comorbidity was found in IBD, possibly related to low socioeconomic status and poor educational level.
Introduction
Inflammatory bowel disease (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic immune‐mediated disorder of the gastrointestinal tract with relapsing-remitting course and heterogeneous clinical manifestations. 1 At present, IBD cannot be cured and represents a lifelong disease burden 2 and even patients with long periods of remission may experience a disease flare or a complication requiring surgery. 3 IBD complications are several and they may potentially be ascribed in a comorbidity framework,4,5 where IBD represents the index disease, and all its complications and extra-intestinal manifestations represent the comorbid conditions. 6 Despite the impact of comorbid conditions on IBD clinical outcomes, there are few studies looking at this issue both in outpatient and hospitalized settings.
Available evidence reporting on hospitalization trends in IBD patients.

Abbreviations: Inflammatory Bowel Disease (IBD); Crohn’s Disease (CD); Ulcerative Colitis; (UC); Anti-tumor necrosis factor alpha (anti-TNFα); Patient-Reported Outcome Measures (PROMs).
In this regard, the aim of this study was to evaluate the prevalence of comorbidity and its demographic, social, and clinical characteristics in a prospectively enrolled cohort of IBD patients in both a hospital and an outpatient setting.
Methods
In this single-center study, data from the San MAtteo Complexity (SMAC) study, a large ongoing prospective research project on clinical complexity (NCT03439410) were analyzed. In the SMAC study, adult patients admitted to our internal medicine unit have been included, regardless of the cause of admission. This academic unit also comprises a tertiary referral center for the diagnosis and treatment of IBD. The details of the enrolment have already been described elsewhere. 28 Denial of informed consent and a prognosis <24 hours were the only exclusion criteria.
For the purposes of the present study, we only included patients with either a new diagnosis or a history of IBD (both CD and UC), regardless of the cause of hospitalization (that was either related to IBD activity or not). These patients were selected through the ICD9 codes pertaining to IBD (i.e., 555.0, 555.1, 555.2, 556.0, 556.5, 556.2, 556.3, and 556.6). Non-inflammatory bowel diseases were excluded. In all cases, the diagnosis was confirmed by reviewing the discharge letter. By applying these criteria, 27 consecutive hospitalized IBD patients were included. The second sample consisted of patients affected by IBD but managed as outpatients. The diagnosis was based on clinical, radiological, and endoscopic/histological criteria, according to internationally agreed guidelines. 29 Disease location and extent were confirmed by endoscopy in UC, and by endoscopy plus imaging in CD. In order to avoid a statistical unbalance and potential biases, due to the small sample size of hospitalized patients, we prospectively enrolled 77 IBD outpatients, hence in a 2:1, age- and sex-matched, fashion, who had been diagnosed at least three months prior to study enrollment. Outpatients were consecutively enrolled in the dedicated IBD outpatient clinic of the same Internal Medicine Unit, hence randomly including both recently diagnosed patients, and those with a longer disease history, over a 1-month time span, following the age and sex matching rules. By doing so, we have enrolled a sample representative of the general IBD outpatient population.
As a primary aim, we assessed the prevalence of comorbidity in both hospitalized and non-hospitalized IBD patients, along with relevant sociodemographic and clinical characteristics, namely age, gender, age of IBD onset, therapy (steroid, immunosuppressive, biological), Harvey-Bradshaw Index (HBI) and Mayo score for CD and UC, respectively (dividing patients into active IBD or inactive IBD), Cumulative Illness Rating Scale (CIRS) severity and comorbidity indexes, Barthel index, Edmonton Frail Scale, 25-item Connor-Davidson Resilience Scale, and the Short Blessed test. An expert physician classified all patients, both from the hospital and outpatient settings, as having comorbidity according to current definitions (i.e., any condition in addition to the index disease under study, that is IBD in our population).30–32 Under the variable “number of chronic conditions”, we simply enumerated the total number of conditions, also including IBD and their complications or extra-intestinal manifestations, if any. As a secondary aim, we assessed potential sociodemographic and clinical factors associated to comorbidity in the whole cohort of IBD patients, in relation to the hospitalization status.
Statistical analysis
Continuous data were described with the median and interquartile range (IQR) and compared between groups according to the type of cohort (outpatients vs hospitalized) and the presence of comorbidity vs no comorbidity with the Mann Whitney U test. Categorical data were reported as counts and percentages and compared with the Fisher exact test. Logistic regression was used to measure the association of the type of cohort with the presence of comorbidity. Odds ratios (OR) and 95% confidence intervals were computed. Though no multivariable analysis could be performed due to the sample size, this association was adjusted in turn in a bivariable analysis, for a series of candidate confounders, which were considered the most relevant patient clinical characteristics in relation to the hospitalization status. The modifying effect of the confounders was assessed by including an interaction term with cohort in the model. The software Stata 17 (StataCorp, College Station, TX, USA) was used for all computations. A 2-sided p-value <0.05 was considered statistically significant. The study was approved by the local Ethics Committee, as an extension of the SMAC study (Protocol number NCT03439410). The study follows the STROBE recommendations for quality assurance. No patients, nor members of the public were involved in the design or interpretation of the study. All data relevant to this study have been here reported; additional raw data can be shared upon reasonable request to the corresponding author.
Results
Overall, we included 104 patients, of whom 27 were hospitalized (median age 49 years, IQR 32-70) and 77 outpatients (median age 54 years, IQR 37-68) in a 2:1, age- and sex-matched, fashion.
Sociodemographic and main clinical features of the non-hospitalized vs hospitalized patients.

Abbreviations: 25-item Connor Davidson Resilience Scale (CD-RISC25); Body Mass Index (BMI); Cumulative Illness Rating Scale (CIRS); Short Blessed Test (SBT); Edmonton Frail Scale (EFS); Short Blessed Test (SBT).
Clinical characteristics of IBD in non-hospitalized vs hospitalized patients.
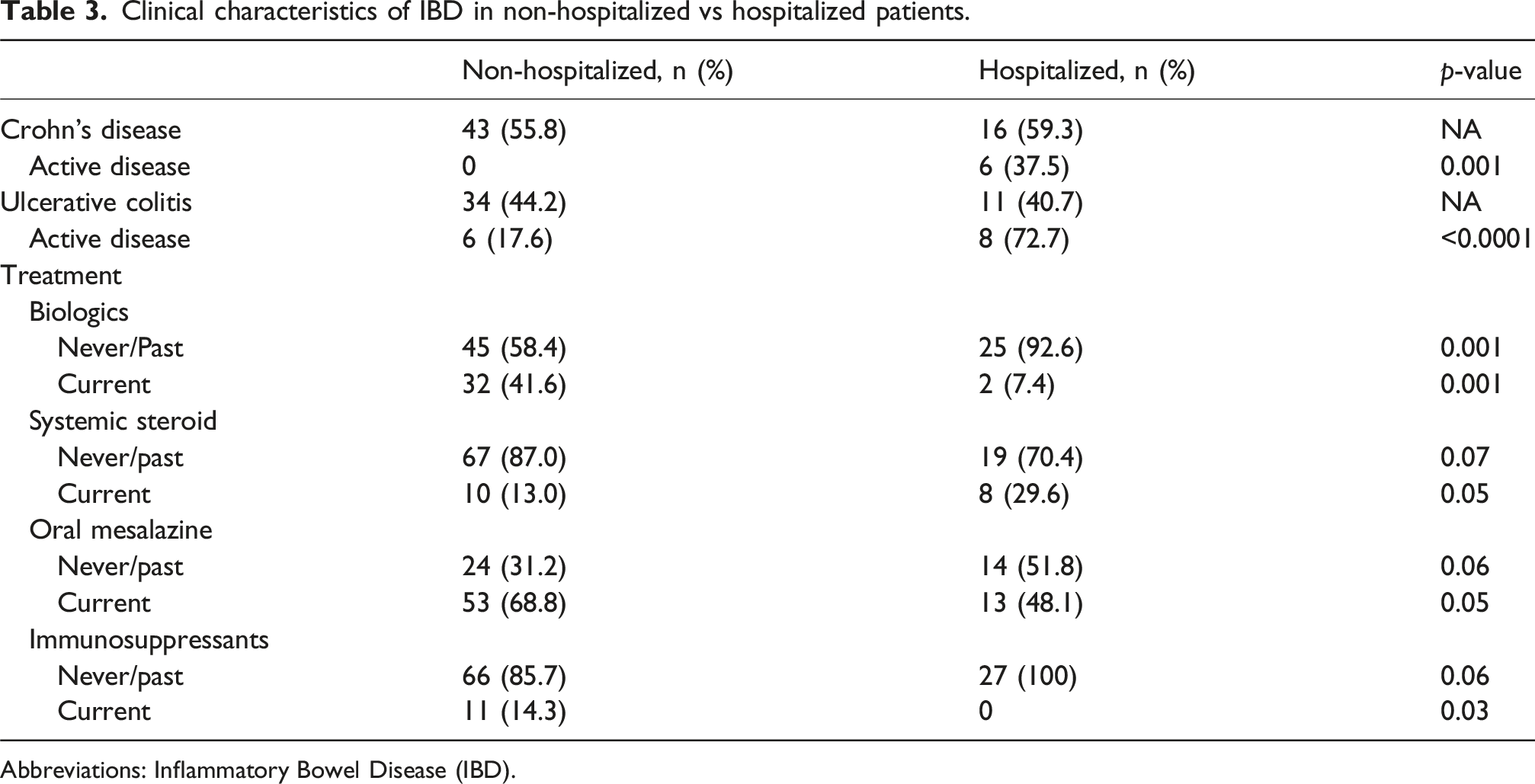
Abbreviations: Inflammatory Bowel Disease (IBD).
Sociodemographic and main clinical features of patients with no comorbidity vs comorbidity.

Abbreviations: Multiple Chronic Conditions (MCC); Connor Davidson Resilience Scale (CD-RISC25); Body Mass Index (BMI); Cumulative Illness Rating Scale (CIRS), Edmonton Frail Scale (EFS); Short Blessed Test (SBT).
Bivariable analyses assessing potential factors associated to comorbidity in the whole cohort of inflammatory bowel disease patients in relation to the hospitalization status.

Abbreviations: Standard Error (SE); Confidence Interval (CI); Body Mass Index (BMI); Crohn’s disease (CD); Ulcerative Colitis (UC); Edmonton Frail Scale (EFS); Short Blessed Test (SBT).
Discussion
We have herein focused on an overlooked topic in the field of IBD, namely the relevance of comorbidity in both outpatients and hospitalized patients. To corroborate common knowledge, hospitalized IBD patients had a more clinically active disease and needed systemic steroid therapy. Instead, among the novel findings, although our study should be considered as a preliminary observation, we showed that older age, female sex, low income, low educational level, frailty, and polypharmacotherapy were all more likely associated with comorbidity in IBD patients, regardless of hospitalization. Hence, IBD plays a key role in shaping the health profile of patients with multiple conditions, and even outside of severe cases requiring hospitalization, IBD contributes significantly to the occurrence of other health issues. Consistently, in our hospitalized patients IBD was active in many cases, with a greater severity in CD than UC, thus justifying the reason for hospitalization. The significance of these data is even stronger when considering that we prospectively collected a large amount of information per individual patient, including both clinical data and performance status indices, without the use of administrative databases. Indeed, a study including a larger cohort of IBD patients is needed to confirm our results.
As it appears clear from Table 1, there are little data about the impact of socioeconomic factors in determining hospitalization in IBD patients. In addition to the predictable associations between comorbidity and age, CIRS severity index, polypharmacotherapy, EFS >5, an association was also observed with female sex, income <1000€/month, and low educational level (<8 years). Although some of these factors may be associated with comorbidity per se, regardless of the underlying specific disorders, studies addressing these factors in IBD are largely lacking. In general, the increased prevalence of multimorbidity in females has been attributed to a higher prevalence of autoimmune diseases, mental disorders (e.g., depression, anxiety), and functional disorders (e.g., irritable bowel syndrome) compared to males. 32 In addition, women under 60 years old are more likely to have a contact with their general practitioner than men of the same age, thus making it easier to be diagnosed. 33
Overall, our data showed that individuals with IBD frequently experience a heavy burden of comorbidity, potentially associated with lower socioeconomic status and limited education levels. A low income (<1000€/month) is not only associated with a comorbidity status 34 but also increases the risk of it by about three times. Being low-income made people more likely to fall into a group of increased rates of mortality and illnesses and, at the same time, adult chronic illness may increase the likelihood of poverty. Indeed, a risk factor for every pattern of multimorbidity was material deprivation 34 and a possible explanation may be the association between low income and eating an unhealthy and low-cost diet.35,36 Although we did not specifically look at this issue in our study, an inappropriate diet has been found to be associated to malnutrition with all its complications, and it plays an even more fundamental role in gastrointestinal diseases, particularly in IBD. 37 Additionally, low income and malnutrition are also strictly tied to the level of education which is per se a risk factor for developing comorbidities.27,29,38,39 In this regard, it has already been shown that fewer patients with IBD achieved post-secondary education as compared to a control population. 40 There are few inconclusive studies looking at the significance of socioeconomic deprivation in IBD. According to a review, it appears that socioeconomic, racial, and ethnic disparities in IBD are increasingly being identified, where both upstream (e.g., poverty, racism, underinsurance) and midstream (e.g., lack of social support, food insecurity, lack of access to IBD healthcare, psychosocial stressor) socioeconomic determinants cause downstream health outcomes (e.g., delayed IBD diagnosis, increased IBD severity, more hospitalizations, more disability and mortality). 41
Some differences also emerged between hospitalized and non-hospitalized patients. Regarding the prevalence of comorbidity, this was roughly 58% in non-hospitalized patients and 66% in hospitalized patients. The low difference in the two settings stresses the role of IBD in being associated with several complications and other comorbid conditions, where the hospitalization status has no influence. While this figure denotes a high prevalence, we might have expected an even higher prevalence in hospitalized patients, since our setting is that of internal medicine, where more than 90% of patients usually have this feature. However, the median age of hospitalized IBD patients was markedly lower (roughly 50 years old) compared to that of other patients admitted to our internal medicine ward (roughly 75 years old) 38 ; age is indeed one of the most important factors associated to multiple chronic conditions.
As far as the clinical pattern of our outpatients compared to inpatients is concerned, it may appear paradoxical that more outpatients were on biologics. However, a large meta-analysis of 27 studies 13 highlighted that infliximab reduced the risk of hospitalization and surgery in IBD patients, so we can deduce that all new biologics and small molecules will reduce it even more significantly and hospitalization could be not strictly related to disease activity, but to other factors.
Among our results, frailty was also found to be rather common in hospitalized patients as previously shown in a retrospective and administrative database study. 14 Indeed, patients with IBD may be particularly exposed to both biological and social frailty, due to the impact of their disease on need for treatments (e.g., immunosuppressants, biologics), surgery, extra-intestinal manifestations, social stigmatization and low resilience.42–46 This finding is of particular importance when considering the relatively young median age of our inpatients. IBD and related factors may therefore enhance frailty even in younger patients.
The present study has indeed some limitations that must be stressed. First, due to the small size of the sample, that did not allow us to differentiate between UC and CD, the inferential analysis must be generalized with caution. For this reason, this should be considered as a preliminary study that needs to be confirmed by further evidence. In addition, the low heterogeneity of the sample did not allow a deeper statistical analysis. Further, we could not make a distinction between comorbidity and multimorbidity,6,30,31 not only due to the small size, but also because IBD certainly represents a prototype of index disease mostly affecting young adults and not older adults where multimorbidity is instead a common feature. On the other hand, our study has some strengths, such as the large amount of information collected per individual patient, including both clinical data and performance status indexes, and all data were collected prospectively and without the use of administrative databases. Finally, since we have particularly focused on socioeconomic factors, we believe that studying IBD as a whole, without splitting into UC and CD, is appropriate, because those factors are certainly shared between diseases. In fact, it is expected that social determinants, including financial strain, health literacy, and access to education, impact disease management and outcomes in a similar way in UC and CD. 41
To conclude, patients with IBD displayed a high prevalence of comorbidity, not only because of disease severity and its complications, but also possibly related to low socioeconomic status and poor educational level, in both the hospital and outpatient settings. Future studies addressing these issues to confirm our preliminary results are warranted.
Footnotes
Consent to participate
All patients provided a written informed consent to participate in the study.
Consent for publication
Obtained from all patients.
Author contributions
All authors participated in the drafting of the manuscript or critical revision of the manuscript for important intellectual content and provided approval of the final submitted version. Individual contributions are as follow: GRC designed and coordinated the study; MVL and ASB drafted the manuscript; all authors organized data collection conducted the study and/or enrolled patients; CK designed and performed statistical analysis, interpreted data, and revised the manuscript; GRC made the final critical revision for important intellectual content. All authors approved the final version of the paper.
Funding
This research is part of a project for the study of clinical complexity (SMAC study) funded by San Matteo Hospital Foundation - Italian Ministry of Health (Progetto di Ricerca Corrente 2017), and part of a project focusing on immune-mediated diseases of the gastrointestinal tract (Progetto di Ricerca Corrente 2022, same funder). The funding source had no role in the design, execution, analyses, and interpretation of the data.
Declaration of conflicting interests
The authors report no conflict of interest.
Data Availability Statement
All data relevant to this study have been here reported; additional raw data can be shared upon reasonable request to the corresponding author.