
Abstract
Objectives
Many older adults with multiple chronic conditions (MCC) frequently experience hospitalizations, functional limitations, and poor quality of life. Outcomes may be improved by promoting self-regulation, which may individuals respond to health threats and manage their health conditions. The aim of this study was to describe self-regulatory coping among older adults with MCC.
Methods
A qualitative descriptive study using semi-structured interviews and content analysis and guided by the Common-Sense Self-Regulation Model. Seventeen community-dwelling older adults with two or more chronic conditions participated in our study.
Results
Three themes were developed from the analysis: (1) “I don’t think about it unless something happens": coping in the absence of a health event, (2) "doing what I am supposed to do”: coping during a health event, and (3) “How do I know if what I did works?”: appraisal of coping success.
Discussion
Self-regulatory coping was influenced by individual beliefs and experiences (illness representations), context, self-efficacy and availability of support and resources to cope with MCC. These findings suggest implications for clinical practice and future self-regulation interventions for older adults with MCC.
Introduction
Over 80% of individuals 65 years and older in the United States live with multiple chronic conditions (MCC). 1 MCCs are co-occurring health conditions that last for at least a year and require continuous medical management. 2 Older adults with MCC frequently experience poor health outcomes (e.g., hospital readmissions, functional limitations, poor quality of life) and those who identify as Black or Hispanic are disproportionately affected by these poor health outcomes.3-5 Community dwelling older adults with MCC are also at greater risk for nursing home placement than their counterparts without MCC. 6 Self-management of MCC is complicated by polypharmacy, treatment burden, and the need to coordinate care among multiple providers.7-10
Self-regulation, defined as the process of regulating behavior and emotions to cope with and adapt to a situation, is an essential strategy for self-management of MCC.
11
One approach to describing self-regulation is the widely used Common-Sense Self-Regulation Model (CSM).
11
The CSM describes a set of illness representations and coping procedures and appraisals that influence an individual’s response to and adjustment to an illness. Illness representations are individual cognitive perceptions of a health condition, such as the cause or treatment of illness, and emotional responses to a health condition, such as anxiety, fear, or sadness. Prior research operationalizes coping procedures as problem-focused or emotion-focused coping.11-14 Problem-focused coping is a strategy to attenuate the consequences of a perceived health threat such as seeking/receiving instrumental support; in contrast, emotion-focused coping refers to strategies to attenuate emotional responses, such as cognitive reappraisal, acceptance, and avoidant coping.12-14 Finally, as individuals cope with a health threat, they also appraise the effectiveness of coping with illness representations.
11
Adaptation of the Common-Sense Regulation Model.
11

Earlier studies indicate that CSM-informed interventions targeting illness representation and coping are associated with positive outcomes such as treatment adherence in individuals with hypertension and end-stage renal disease, A1C reduction in diabetic participants, and faster return to work following a myocardial infarction event.15-17 These earlier studies describe the success of intervention focused on treatment of individual diseases. However, a significant gap in earlier research is the development of CSM-informed interventions focused on the needs of individuals with MCC.15-18 Thus, limited data exists to inform capacity-building interventions designed to improve self-regulation among of individuals when illness representations and coping may be severely challenged by multiple symptoms and compounded emotional burden related to the experience of illness.19-25 Qualitative research based on the lived experiences of individuals with MCC is necessary as a first step toward designing intervention models to improve care. Therefore, the purpose of this study was to use the CSM as a guiding model to describe self-regulatory coping among older adults with MCC.
Methods
Design
Qualitative descriptive design methods are useful for researchers seeking understanding of attributes of a phenomenon being studied. 26 Ethics approval for this study was granted by the Institutional Review Board at the University of Texas Health Science Center, San Antonio (#HSC20160103H). We used the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 27 to guide reporting of study methods and results (Appendix).
Sample
We recruited older adults with MCC living in South Texas and Northern Virginia. Inclusion criteria were: (1) being 65 years and older, (2) self-reported diagnosis with at least two chronic illness with at least one condition of hypertension, hyperlipidemia, coronary artery disease, diabetes, or arthritis. The chronic conditions were purposively chosen because they are the five most common chronic conditions in older adults in the United States. 28 Besides, prior CSM-based studies involving older adults with MCC have also utilized this approach.23,57 Because the study is focused on MCC self-management of community dwelling older adults, we excluded individuals who resided in nursing homes. Participants who met the inclusion criteria were invited to participate in the study and given information sheet about the study objectives, plan, risks and contact information about the study P.I. Participants were given adequate time to ask questions about the study. To recruit participants, fliers were placed in public areas of seven geriatric clinics and senior community centers in Texas and Virginia. We also advertised at minority serving and low-income senior centers and senior apartment buildings. Potential participants contacted the study team via phone and/or email. Screening questions included age, residence, chronic disease diagnosis (including both physical and mental diagnosis). All participants provided verbal consent using IRB-approved procedures before enrollment in the study and ongoing consent was sought throughout their participation in the study.
Data collection
One investigator [AB; trained in qualitative methods] conducted one-on-one interviews with participants, in private and in the participant’s homes or private and quiet areas of Senior Apartment buildings/centers. Participants were asked to self- report their diagnosed chronic conditions (physical or mental health conditions) and recent hospitalizations within a year of the interview. Previous research indicates that hospitalizations are especially taxing for older adults, and some may require up to a year to return to their pre-hospitalization health baseline, potentially influencing their coping strategies.29-32 An interview guide was developed based on the literature on CSM. The topic list of the interview guide included: illness representation, such as cause, timeline, consequences, treatment for each condition; coping strategies for illness representations; daily managing of MCC and the effectiveness of coping with MCC [Appendix]. Interviews were conducted in English and participants were financially compensated for their time. Our interviews began by first, eliciting participants’ perspectives about their illness representation of identify, cause, timeline, consequences, treatment for each of their conditions (tell-me about your conditions). We asked probing questions such as “how does it impact your life?” “how do you feel about it” to elicit emotional responses. After that, we asked how they coped with each illness representation and their emotions about MCC. Second, we asked them to describe a day or daily managing their MCC and/or coping with their MCC. We further probed the participants on how they prepare for disease exacerbation, how they have managed disease exacerbation in the past. We also asked them to describe circumstances around their disease exacerbation. Third, we asked the participants to identify other methods (besides their treatment regimen) that was used to manage their MCC. We also probed the participant on each method reported use how useful they were Finally, we asked participants about what they found useful to manage the MCC and what not useful. We probed participants further to describe their experience with each strategy reported and how they determined that it was useful or not useful. Participants were also asked to rate their health as poor, fair, good, or very good. The data collection period was continued until additional interviews yielded no new information pertaining to coping with MCC. 33 Interviews were audio-recorded and professionally transcribed.
Data analysis
Interviews were analyzed using content analysis. 34 We used the CSM to guide our content analysis. The analysis started by reviewing interview transcripts line by line for sentences or phrases that represented illness representation, coping and appraisal. Coding was conducted manually by AB, discussed with SG and was presented to the research team. When all data were coded, the principal investigator and research team used content analysis and data condensation to identify patterns in illness representation and coping with MCC across the full set of interview transcripts. Finally, data were organized for reporting in data tables and a narrative report on the themes. Individual bias was managed by audio-recording and verbatim transcription of interviews, creating an audit trail with records of interactions and decisions of the principal investigator and the full research team, and member checking of study findings with three study. Member-checking 35 was conducted by reviewing the pre-liminary themes with three participants to ensure that participants’ thoughts, knowledge, and feelings were congruent and captured in the analysis. Insights gained from member-checking were also integrated into the data analysis.
Results
Participant clinical and nonclinical characteristics N = 17.

Rounded up to the nearest percentage point.
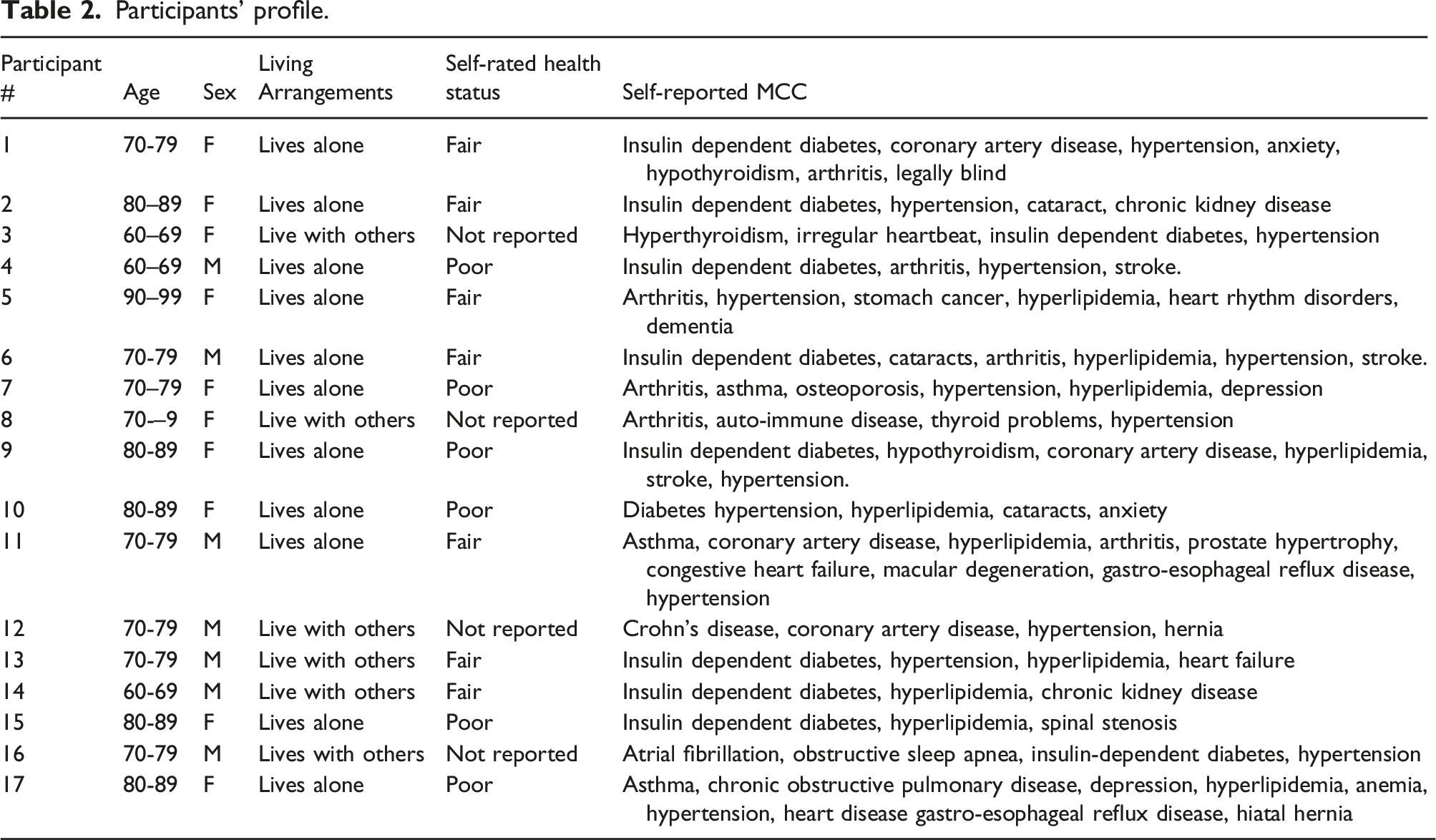
Participants’ profile.
Qualitative findings
Throughout the interviews, participants detailed how their coping strategies were shaped by context- specifically whether they were experiencing a serious health event or not. Participants described serious health events as situations requiring attention such as: symptom exacerbations, abnormal health values (e.g., blood pressure, blood sugar values) and perceived deviations in function or baseline health status. Three themes were identified: (1) coping in the absence of a health event, (2) coping during a health event, and (3) appraisal of coping success. The themes are described in detail below.
Theme 1: “I don’t think about it unless something happens”: Coping in the absence of a serious health event.
Overall, all participants recognized that MCC posed a long-term threat to their health, well-being, and survival. While the most participants expressed acceptance of their MCC, some conveyed sadness regarding their MCC. Nevertheless, every participant believed that their MCCs were controllable with their existing treatment regimen. They employed problem-focused coping strategies to manage their treatment regimen and functional issues and emotion-focused coping strategies to address their emotions about MCC.
Problem-focused coping
In the absence of a serious health event, participants coped with their MCC by following their treatment regimen and incorporating them into their daily lives. For example, participant #11 describes how he routinizes his daily treatment regimen: “You just get a routine going. You take your medications….When I’m watching TV… I exercise… you do the same thing all the time, the same way, the same time, same day…
Other participants sought support from others to manage and follow their treatment regimen. For example, participant #5 who is describes how her children help her with managing her medications and how she integrated exercise as a shared activity with her friend. They [children help me with fill] my pillbox… so, whatever’s in that little box [pillbox] is what I take….. I try to walk, and my friend likes to walk, too, so we walk [together].”
Due to their confidence in managing their MCC, belief in the treatment's effectiveness, and commitment to their regimen, the participants chose not to 'think' about MCC because they believed they were doing all they could to manage their MCCs. For example, Participant #2 states: “I don’t think about it, unless something happens…I take care of myself…I take my medicine. I try to sleep I try to eat correctly. Exercise and walking and doing things…
On further probing, on why she chose “not to think about” her MCC, she states: “I guess [my] self-confidence comes with experience [managing MCC]...I’ve had it for so long,”
Emotion-focused coping
Overall, most study participants reported acceptance of their MCC. They believed MCCs were a normal part of aging and reported accepting MCC as part of living and aging. For example, Participant #5 credited experience of MCC to normal aging. “I mean, I’m 90 years old. I’ve gotta have something to show for those lives that I’ve lived. Something’s gotta be wrong somewhere. Hearts gotta be wearing out somehow. And I realize that I’m not as young as I used to be…. I’ve accepted it…I don’t think about it’s part of life.”
However, some participants experienced negative emotions about their MCC. While they believed that their treatment regimen was effective in controlling their physical symptoms (and followed their treatment regimen), they expressed sadness and dissatisfaction with their health status and/or loss of independence. For example, Participant #10 explained that she chose not to “think” about MCC because those thoughts made her experience feelings of loss and chooses to “block it out of her mind.” “And that’s another thing that bothers me, I’m not independent like I used to be…I try to block out of my mind my conditions. I just try not to think that they’re there. I want to be normal.”
One participant coped with their emotions about functional impairments by swapping activities that they previously enjoyed (and could no longer perform) for equally satisfying activities. For example, one Participant #15 reported: “you have to switch what you’re doing... I used to love running…I [can’t] run anymore…[but]…I quilt.. for my family now and I love it”
While another preferred to distract themselves by doing things that brought them joy. For example, Participant #7 expressed the desire to be busy, doing things that she likes to do, instead of focusing on her MCC. “Because I wanna do others – if I thought about them then I wouldn’t think about doing good things, you know? I’m busy with the Senior Center. I’m busy...I’m helping on a campaign for a town district congressperson...I keep busy. I try not to think about myself. I try to think about other things…. The more you dwell on stuff, the worse you’re gonna feel.”
Theme 2: “Doing what I am supposed to do”: Coping during a serious health event.
Overall, most participants perceived health events such as new symptoms, symptom exacerbations, abnormal health values abnormal health values (e.g., blood pressure, blood sugar values) as serious health events requiring attention. Problem-focused coping were prioritized during these serious health events.
Problem-focused coping
Participants coped during serious health events by following guidance of their health care team; Participant #1 stated, by “doing what I’m supposed to do.” This entailed following a specified action plan and/or seeking support from others. Action plans were specific to the nature of the health events. Participant #1 attributed her symptoms of weakness, dizziness, and nausea to accidentally skipping a dose of medication. She reported her prior knowledge and understanding of symptoms that informed her action plan to manage symptoms. “If I forget to take my blood pressure medicine…And that’s when you’re going to get a headache…. Yeah, I can feel it when I get real hot, and your face gets real red. It feels like a hot flash. And then, when I do get, if I go lay down in the dark someplace and just kind of relax for a few minutes, sometimes, it will go away. But I take my pills, and sometimes, if I forget to take it on time – oh, that’s telling me to take a pill.”
Participant #1 also described an action plan, developed with her health providers, for emergency situations. You start getting anxiety and palpitations, and then, you start getting these little pains (chest pain). But I have that Nitrostat. So, if I take one of those, and then, wait five minutes and take another one, and if it doesn’t go away, then, I go to the Emergency Room or call the doctor if it’s office hours. And they’ll either tell you to wait or not go.
Participants reported that carrying out action plans during health events was contingent on the being able to identify the nature of health events. However, some health events were undetectable by the person with MCC. For example, Participant #10 expressed confidence in identifying symptomatic health events, but she was shocked when she learned risks that were not apparent to her. “One time, I went to my primary doctor, and when I walked out of his office, I wasn’t sure I was going to live long enough to get home. Because he found my cholesterol was up, my glycerides were up, my heart was beating too fast, sugar was up, blah, blah, blah, blah, blah, blah. And I thought, dear God, what in the world’s wrong with me....I didn’t know. I felt okay. I felt fine.”
In contrast, two participants chose not to seek help for health events. Both participants withheld information about abnormal health events from healthcare providers. They participants believed that took too many medications and attributed their symptoms to aging. Participant #7, who was taking 5 medications daily, reported withholding information about arthritis pain because she feared reporting the pain would result in an increase in medications. “I don’t really go to a doctor for…. arthritis in my hands or knees because I don’t wanna take any more medicine than I do. I was taking six. I’m down to five. And that’s a lot of medicines to take a day.”
In addition to preparing medical action plans, some participants also described action plans for their health and plans to support their family and friends around them during times of health events. They had action plans for situations when a health event could be highly consequential to their social role and burden or potentially harm loved ones or those in their care. For example, Participant #9 described an action plan for exacerbation of her depression symptoms which could diminish her ability to care for her grandchildren. “I just don’t want to talk to anybody or do anything [when she experiences exacerbation of her depressive symptoms]. I just want to be by myself. And I get those days. I don’t know how I’m gonna deal with it with babysitting right now because I can’t take those days. My daughter...got a backup babysitter.”
Similarly, two participants reported financial action plans for health events. Both were women who lived alone and had post-graduate education. For example, Participant #5 made financial plans to protect her family. “And then I have long-term care [insurance], too. I took that insurance out when I was very young. Take it out. Okay, well, if I get pneumonia – well, if I get something that I’m not going to survive, and I’m gonna be in a hospital for a long time – in and out, in and out, in and out – it would take care of that.”
In addition to planning for serious events, participants also described how they coped after serious hospitalization. Four participants reported being hospitalized within a year of the interview and relied on instrumental support from their family, friends, home-based clinicians (health nurse and/or rehabilitation therapist) after hospital discharge. Of the four participants, two (Participants 9 and 17) experienced a hospitalization within a month of their interview. Although medically stable, both participants were actively experiencing symptoms and relied on their family and/or home-based clinicians. For example, after a recent stroke experience, Participant #9 discussed feeling overwhelmed with her treatment regimen and how her daughters helped provided support to her. She states: “ Just right now, it’s a little bit overwhelming...I have two daughters who are nurses….they take care of me..[they take me]..to my appointments…and I have a [rehabilitation] therapist that comes, [to the house].”
Emotion-focused coping
Emotion-focused coping were frequently reported in the aftermath of a serious health event; particularly among those who were experiencing difficulty adjusting to new symptoms and treatment regimen. Participants coped with their feelings of sadness” by seeking emotional support from others and expressing gratitude. For example, one participant who lived alone and experienced a recent hospitalization described how daily phone calls with her friend helps her with feelings of sadness. Participant #9 states: “my friend calls me every night….[it] has been helping me a lot.”
Another participant #17, who was hospitalized expressed gratitude that they were still alive after their hospitalization. The participant stated: “I was in the hospital four days..it was really bad”..I’m happy that I’m still [alive]”
Theme 3: “How do I know if what I did works?”: Appraisal of coping success.
Participants evaluated the effectiveness of coping by monitoring for improvement in symptoms and health lab values. For example, Participant #4 described how he appraised the effectiveness of his coping approach during a health event. “How do I know if what I did works? I mean, I’m not dizzy; I’m not falling like I had done, my sugar is good, so something’s working.”
Similarly, Participant #5 expressed the belief that her regimen was effective when the doctor says, “I’ll see you in six months.” This was particularly important to some participants who had frequent healthcare provider visits for serious illness. For example, participant stated: “When they say, ‘Come back in six months,’ what does that mean? It means you’re okay. Just keep doing what you’re doing.” Well, there for a while, I was going back every two weeks when I was dealing with the cancer and trying to get that under control and everything.
To this participant, her physician’s comment meant that her lab work was normal, to continue her regimen without any changes.
Alternatively, some participants did not focus on lab results and numbers because they were confident about self-management practices. To these participants, their health goal was not just getting their “numbers” lower. Rather, their overall goal was to “get better,” have fewer or no medications, and being able to engage in meaningful activities (without disruptions from MCC). For these participants, their approach to coping with MCC was beyond the numbers. For example, Participant #2 explained her health goal was not only beyond getting her lab work normalized. As she coped with illness, she wanted to be off the medications she was taking: “No. I don’t worry about the numbers because I know I’m eating as correctly as I can. I’m getting certainly enough fluids, I’m walking around, I’m interacting with things, trying to stay interested in life. All of those are aids to getting better. Now, it’s not my goal to stay on medicines and to stay in a situation where I’m getting worse. It’s my goal to get better…I want to be able to play with my grandkids.”
One participant reported “feeling better” and having “a good feeling” as an indicator that their coping strategy was effective. Participant #1 states: “you just have a good feeling about yourself….Have you ever been out in the cold and you’re so cold, you, brrr….And then somebody walks up to the fire and puts a nice warm blanket around you, like, ahh. You know that feeling? You just have a good feeling about yourself; it’s a comfort.”
Overall, participants believed that their coping strategies were effective if it yielded outcomes that aligned with their personal health goals. For many, these goals were to take fewer medications, feel better psychologically and to participate in meaningful activities.
Discussion
Overall, participants employed problem and emotion-focused strategies to cope with their MCC. In the absence of a serious event, they implemented their treatment regimen with support from others (problem-focused coping) and coped with their emotions about MCC by re-appraising their MCC as a part of aging, and distraction (emotion-focused coping). In the presence of a serious health events, the participants prioritized problem-focused coping (implemented pre-established self-management action plans and/or sought instrumental support from others). Overall, they appraised the effectiveness of their coping by seeking insights from healthcare providers and monitoring for improvements in symptoms, polypharmacy, social role function, and wellbeing. Findings from our study suggest: participant’s selection of coping strategy was not only guided by their beliefs and emotions about MCC (illness representation) and, health goals but may also be influenced by the context (presence or absence of a serious event), confidence in their ability to manage their MCC (self-efficacy) and the availability of support and resources to manage their MCC.
In the absence of a health event, the phrase “I don’t think about it” was commonly mentioned by participants. The participants chose “not to think” about their MCC because they followed their treatment regimen (problem-focused coping) and/or to avoid feelings of sadness about their MCC on their (emotion-focused coping). Our findings are consistent with literature on coping in individuals with chronic illness such as diabetes and HIV.36-38 For example, in a 2021 qualitative study 36 examining coping and diabetes distress among women in Latin America, “not thinking about” diabetes was reported as both a problem focused and emotion-focused coping strategy. Adding to prior research, our findings highlight this coping strategy in the context of self-regulation and MCC self-management.
In our study, we found that participant’s confidence in the effectiveness of their treatment regimen as well as the confidence in their ability to implement their treatment regimen (self-efficacy) were driving factors in their decision to adhere to their treatment regimen and “not think” about their MCC; suggesting that a relationship between perceptions of controllability, self-efficacy and problem-focused coping may exist among older adults with MCC. This finding aligns with prior CSM-based studies. For example, meta-analysis of CSM-based studies have proposed a positive relationship between perceptions of controllability and problem-focused coping.12,39 Findings from a prior CSM-based study texamining illness representation among older adults with MCC suggest that individual factors such as self-efficacy may also influence illness representations (and potentially coping) among individuals with MCC.40,41 Moreover, previous studies also indicates that health literacy plays an important role in shaping both illness representation and developing self-efficacy to cope with chronic illness. 42 Future quantitative studies are needed to clarify the relationships between illness perception, self-efficacy, health literacy and coping strategies among older adults with MCC.
In our study, we also found that, many participants relied on support and resources from family/friends and/or their healthcare team. Prior research suggest older adults with complex illness such as MCC often require supported by from caregivers which may influence coping, especially during serious health events (e.g hospitalization).43- 45 Prior studies also indicate patients and caregivers report differing perceptions of their illness which may influence how they cope and respond to health events. For example, a study examined illness perceptions among individuals living with mild cognitive impairment and their family members (n=60 dyads). 46 In their study, individuals living with mild cognitive impairment perceived their illness to be less serious than their family members. Future CSM-based interventions involving older adults, researchers may consider dyadic interventions targeting illness representation and coping among older adults with MCC and their caregivers. Moreover, researchers developing CSM-based interventions may also consider addressing social determinants of health factors that impact successful self-regulatory coping and ensuring that the patients and caregivers have the necessary tools and resources to promote successful MCC self-management.
Despite their coping efforts, most of participants reported their “fair” or “poor.” While we did not utilize the validated Medical Outcomes Study SF-36 scale, 47 our findings provides some insights within the scope of this qualitative study. In our study, participants had an average of five chronic conditions. Previous research indicates that older adults with multiple chronic conditions are likely to report suboptimal health status.48-51 For instance, a study using data c from the 2008 and 2010 United States Health and Retirement Study (n=13,232), suggest that older adults with three or more conditions were 23 times more likely to report fair or poor self-rated health than those no chronic condition. 51 However, self-rated health is a multi-dimensional construct influenced by various factors beyond the individual level.52- 54 Further research, utilizing quantitative methods and validated measures of self-rated health, is necessary to understand the relationship between coping strategies and self-rated health among older adults with MCC.
Implication for clinical practice
In our study, the participants expressed confidence in identifying symptomatic events and events that they had experienced beforehand; however, they expressed less confidence identifying health events when they were asymptomatic. Earlier studies suggest that individuals with MCC also have trouble attributing symptoms to specific health conditions.9,10 Our findings suggest that identifying the nature of a health event was essential to coping. Clinicians must renew efforts to equip older adults with MCC and their families with (1) individualized decision-making strategies to identify health events and (2) individualized action plans to manage potentially serious health events.
In addition, two participants withheld arthritis-pain symptoms from their healthcare providers to prevent an increase in their medication count and ascribed their arthritis symptoms to normal wear and tear of aging. This finding aligns with current literature on arthritis and chronic disease self-management and indicates an important challenge for individuals with MCC;10,53 It may be essential to discuss treatment preferences with patients (such as concerns about polypharmacy), so they feel safe to disclose information pertinent to their care. 54 Research initiatives are needed to explore patients’ priorities and how they decide what to disclose to their healthcare providers. For example, de-prescribing practices have emerged as a valuable resource to reduce medication count and adverse side-effects and align healthcare with the older adults’ health goals and values.55,56
Strengths and limitation
While this study has its strengths, there are some limitations to consider. In this qualitative study, we conveniently sampled participants from only two regions within the United States. S. While, the participants came from different backgrounds, over half were college educated and/or had advanced degrees. We are also not able to gather a full picture of their socio-economic status as many of the study participants chose not to report their income. This may have influenced findings of understanding of MCC and access of participants to self-management resources. Moreover, we did not assess participants’ cognitive status and health literacy which may contribute to their experiences managing MCC.
Conclusion
Self-regulatory coping was influenced by individual beliefs and experiences (illness representation), context, self-efficacy and availability of support and resources to cope with MCC. Additional studies are to further characterize self-regulatory coping and develop capacity-building interventions to improve self-regulation and health outcomes among older adults with MCC.
Footnotes
Acknowledgements
We would like to thank Dr. Mark Toles and Dr. Jennifer Leeman for reviewing and providing feedback on this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The funding for this work was supported by the Sigma Theta Tau International. Portions of Ayomide Okanlawon Bankole’s contribution to this work were supported by National Institute of Health/National Institute for Nursing Research Postdoctoral Training funding (T32NR007091-28).
Appendix
ISSM COREQ (Consolidated criteria for Reporting Qualitative research) Checklist
Topic
Item No.
Guide Questions/Description
Reported on Page No.
Domain 1: Research team and reflexivity
Personal characteristics
Interviewer/facilitator
1
Which author/s conducted the interview or focus group?
4
Credentials
2
What were the researcher’s credentials? e.g., PhD, MD
4
Occupation
3
What was their occupation at the time of the study?
4
Gender
4
Was the researcher male or female?
4
Experience and training
5
What experience or training did the researcher have?
4
Relationship with participants
Relationship established
6
Was a relationship established prior to study commencement?
4
Participant knowledge of the interviewer
7
What did the participants know about the researcher? e.g., personal goals, reasons for doing the research
4
Interviewer characteristics
8
What characteristics were reported about the inter viewer/facilitator? e.g., bias, assumptions, reasons, and interests in the research topic
4
Domain 2: Study design
Theoretical framework
Methodological orientation and Theory
9
What methodological orientation was stated to underpin the study? e.g., grounded theory, discourse analysis, ethnography, phenomenology, content analysis
3, 5
Participant selection
Sampling
10
How were participants selected? e.g., purposive, convenience, consecutive, snowball
3,4
Method of approach
11
How were participants approached? e.g., face-to-face, telephone, mail, email
3,4
Sample size
12
How many participants were in the study?
6
Non-participation
13
How many people refused to participate or dropped out? Reasons?
6
Setting
Setting of data collection
14
Where was the data collected? e.g., home, clinic, workplace
4
Presence of nonparticipants
15
Was anyone else present besides the participants and researchers?
4
Description of sample
16
What are the important characteristics of the sample? e.g., demographic data, date
6,
Data collection
Interview guide
17
Were questions, prompts, guides provided by the authors? Was it pilot tested?
4,5
Repeat interviews
18
Were repeat inter views carried out? If yes, how many?
4,5
Audio/visual recording
19
Did the research use audio or visual recording to collect the data?
5
Field notes
20
Were field notes made during and/or after the interview or focus group?
6
Duration
21
What was the duration of the inter views or focus group?
6
Data saturation
22
Was data saturation discussed?
5
Transcripts returned
23
Were transcripts returned to participants for comment and/or
6
Domain 3: Analysis and findings
Data analysis
Number of data coders
24
How many data coders coded the data?
5
Description of the coding tree
25
Did authors provide a description of the coding tree?
5-6
Derivation of themes
26
Were themes identified in advance or derived from the data?
5-6
Software
27
What software, if applicable, was used to manage the data?
5
Participant checking
28
Did participants provide feedback on the findings?
6
Reporting
Quotations presented
29
Were participant quotations presented to illustrate the themes/findings?
Was each quotation identified? e.g., participant number7-14
Data and findings consistent
30
Was there consistency between the data presented and the findings?
7-14
Clarity of major themes
31
Were major themes clearly presented in the findings?
7-14