
Abstract
Introduction
Multimorbidity, in its simplest form, can be described as the coexistence of multiple health conditions in an individual. 1 Living with multimorbidity negatively impacts on the individual’s ability to work, 2 increases their healthcare costs3,4 reduces their quality of life5–8 and intensifies the need for regular contact with healthcare services. 9 Multimorbidity cuts across different spheres and introduces many negative consequences for the healthcare system, which is traditionally, orientated around single disease conditions 10 (i.e., non-communicable diseases (NCDs), chronic infectious diseases and mental health conditions). It could also alter the resources required for staffing, financing 11 and technological development. 12 The vertical nature of health service delivery, along with a lack of training by healthcare workers could further hinder patient-centred care and delivery. 11
Levels of multimorbidity are expected to increase globally as populations age, people adopt unhealthy lifestyles, and the incidence of chronic diseases increases. 13 Low- and middle-income countries (LMICs) face additional challenges when dealing with multimorbidity, including fragmented healthcare systems with limited capacity, inequities in healthcare utilisation and a lack of data on the subject. 14 In South Africa, an upper middle-income country, 15 despite limitations, a growing body of literature has sought to characterise the epidemiology and consequences of multimorbidity in the country.16–20 Our project consisted of a systematic review of prevalence studies on multimorbidity, 21 which informed, and was followed up by the systematic analyses of the three most recent national health surveys.22–24 The systematic review found a paucity of local studies and a lack of standardization of studies reporting multimorbidity estimates. 21 It was argued that the lack of funding and reporting mechanisms are impeding research on multimorbidity. 25 The systematic analyses 26 of multimorbidity in three nationally representative surveys in South Africa,22–24 highlight the high levels of multimorbidity among three key groups, namely, older adults, women, and the wealthy. 26 Our results indicate eleven common disease clusters affecting the multimorbid population. 26 This article aims to synthesize the main findings from a project that described the epidemiology of multimorbidity in South Africa 27 and highlight the importance of implementing multimorbidity focused health policies and service delivery in the country.
Discussion
Multimorbidity among older adults
Prevalence of multimorbidity by survey and age group (weighted).

dPeople aged 15 years and older are commonly included in national health surveys.
The increased odds of multimorbidity in older age are consistent with what has been observed internationally.31–33 The prevalence of multimorbidity among older individuals is concerning, because the proportion of older people are increasing dramatically in LMICs. 34 Population ageing is being driven by falling fertility rates, improved survival at younger ages, fewer adults dying of infectious diseases, and socioeconomic development in the past 50 years.34,35
Statistics South Africa estimated that the proportion of older persons (60+ years) increased from 3.5 million people in 2002 to 5.4 million people in 2020 (i.e., from 7.6% to 9.1%). 36 It is further predicted that the population over 60 years will double between 2012 and 2050. 37 A 2020 report on ageing in Africa highlighted that older adults experience a disproportionate burden of disease - NCDs dominate the disease burden, but infectious (e.g. HIV, Tuberculosis, lower respiratory infections) and nutrition-related disease still account for a sizeable proportion of the disease burden, compared to other regions. 38 Older people also struggle to access healthcare due to financial constraints, as shown by a study in Cape Town, which found income-related disparities in accessing quality care. 39 Mobility issues, the physical effort of spending hours waiting in lines, and dealing with rude and ageist healthcare staff were noted challenges faced by participants. 39 Poor and dismissive communication contributed to confusion in participants trying to navigate the health system. 39
The rights of older people have been recognised internationally by several legal and policy frameworks. Since 2002, two major international policy instruments have guided action on ageing – the Political declaration and Madrid international plan of action on ageing 40 and the World Health Organization’s Active ageing: a policy framework.34,41 Both documents detail the importance of health in older age but there has been a lack of prioritisation of the issue and a consequent lack of progress in implementing these instruments in South Africa. 34 The South African government has endorsed these policies on ageing, and subsequently developed the South African Policy for Older Persons 42 in 2005. 43 The policy promotes a life-course approach, focused on the prevention of disease, and integrated treatment and management of disease in older persons. 43 However, the policy has not been followed up with implementation guidelines, regulations or evaluation plans. Of further significance is The Protocol to the African Union Charter on Human and Peoples Rights on the Rights of Older Persons in Africa which was adopted by the African Union in 2016. 44 Article 15 of this charter guarantees the rights of older people to access health services that meet their needs, facilitate reasonable access to health services and medical insurance, and ensure the inclusion of geriatrics and gerontology in the training of healthcare workers. 44 To ensure appropriate services are available to older people, multimorbidity needs to be considered a vital aspect of these services, given the high prevalence among older adults.
Ensuring a healthy life for all remains a key commitment of the South African government. In 2010, the government adopted the Negotiated Service Delivery Agreement 2010-2014 and among the key outputs were: increasing life expectancy; combatting HIV and AIDS and Tuberculosis; and, strengthening the effectiveness of the health system. 45 More recently, in the National Development Plan (NDP) 2030, the South African government stated that they aim to increase the average life expectancy at birth for men and women to 70 years. 46 The NDP noted that a change in the demographic profile will affect government spending in terms of healthcare and pension provisions, and that high levels of unemployment in the working-age population may make it difficult to absorb these costs. 46 However, no clear strategies exist on how to meet these needs. 43 A notable omission (or oversight) is the lack of acknowledgement of the implications of rising multimorbidity.
In the authors’ view, multimorbidity could be indirectly managed through the implementation of Goal 4 (reduce the prevalence of NCDs) and Goal 6 (complete health-system reform) of the NDP 2030. 46 Another plan that could also indirectly impact multimorbidity is ‘The Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2013 – 17' which was a result of the South African Summit on the Prevention and Control of Non-communicable Diseases held in September 2011. 47 It set ten clear targets to be reached by 2020 - the first, to reduce premature mortality in people under 60 years of age due to NCDs by 25%; 48 which effectively excludes older people. There was no focus on population ageing, although achieving these targets would yield healthier older people 43 and reduce multimorbidity. More recently, the ‘National Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2022 – 2027’ was launched. 49 This document explicitly mentions multimorbidity in Goal 3 (people living with NCDs must receive people-centred health services to prevent and control NCDs). 49 As part of Goal 3, the document states the need to ‘promote and strengthen care within a context of managing co- and multimorbidities’. 49 However, the plan does not mention targeting at-risk groups of people with multimorbidity.
Some provincial health authorities such as the Western Cape Department of Health recognize co-morbidity as an issue. As part of their 2013 plan, Healthcare 2030: A Future Health Service for the Western Cape 50 they set out a strategic framework and focus on four pillars to address the burden of disease in the province. 51 The pillars include having a person-centred approach, integrated provision of care, continued support for the patient and a life-course approach to treating patients. 51 They acknowledge the increased risk of co-morbidities in adulthood, hence the strong focus on mental health integration into primary healthcare services, HIV and chronic disease health services. 50 However, older adults and their needs are not specifically mentioned.
While nationally the policy environment is supportive of the needs of older people, few documents mention co-morbidity or multimorbidity in older people. In South Africa, much attention has been given to increasing life expectancy. However, no clear strategies have been suggested to enable South Africa to meet these challenge and many of the policies appear not to be implemented or evaluated. 43 It may be essential to further prioritise the needs of older people – in the same way the needs of under 5s have been prioritised. 43
Multimorbidity in women
In the three analysed South African national surveys,22–24 it was noted that women had a higher prevalence of multimorbidity compared to men, and this was true across most age groups (Figure 1). Multimorbidity prevalence by survey, age group and gender(weighted).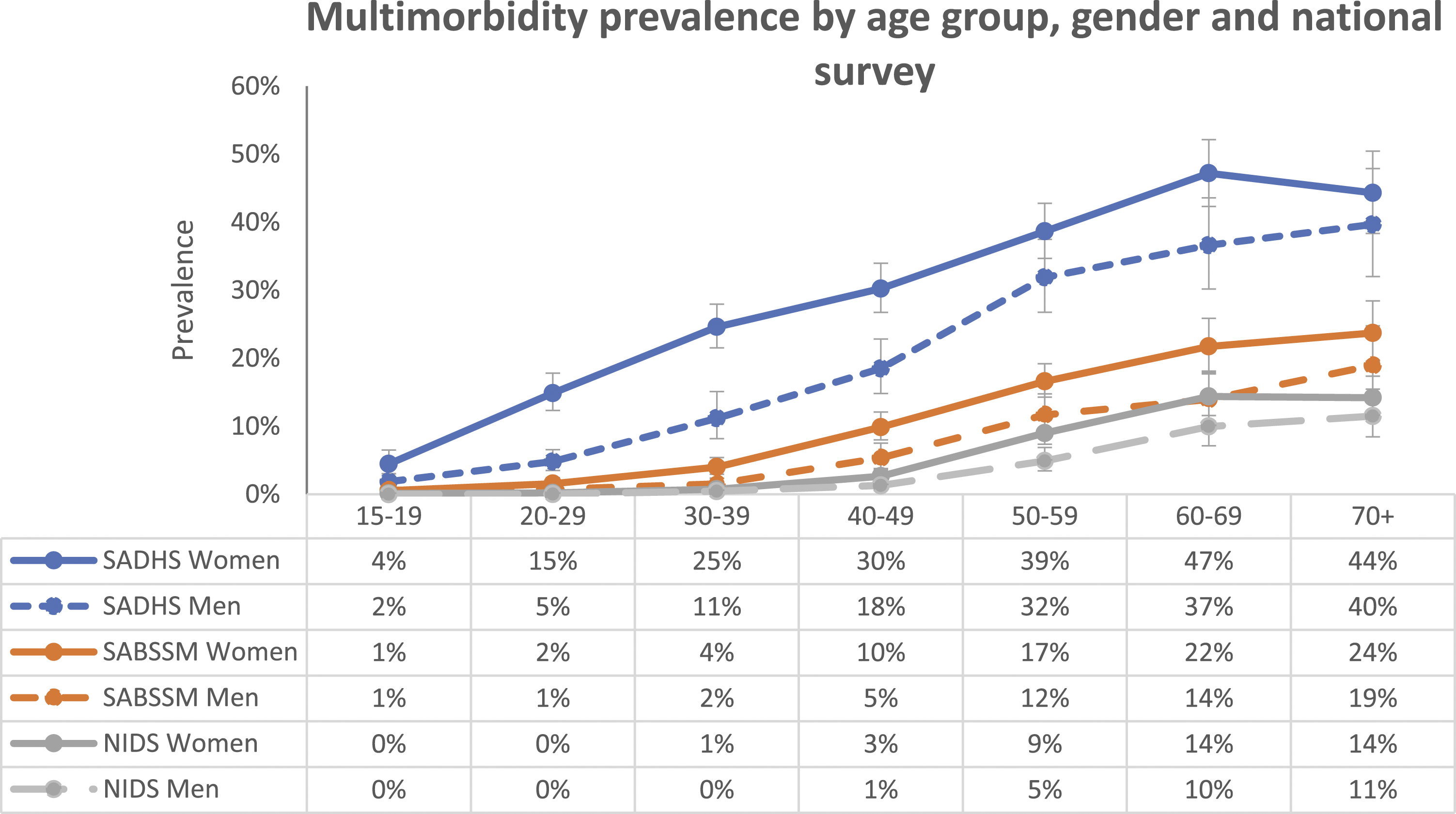
The gender differential has been found in other local17,18,52,53 and international studies.54,55 While fairly well established, it is unclear why these differences exist. There are various possible explanations. First, there is a gender gap in self-reported health status. 56 Second, women are more likely to know their health status as they tend to have higher healthcare utilisation compared to men. 57 Third, the gender differential reflects disease burdens that are more prevalent in women, such as HIV 58 and obesity. 59 This high prevalence of HIV among women has been attributed to multiple related factors, including biological, behavioural, socioeconomic, cultural and structural risks. 60 Similarly, women have high and increasing rates of obesity,61–63 which is associated with increased odds of multimorbidity. 64 In addition, gender norms may exacerbate the consequences of multimorbidity. For example, multimorbidity can impact women’s lives by affecting their ability to earn an income due to women having less secure forms of income with little to no social protection.
Since women live longer than men, and have higher levels of multimorbidity than men,54,55 the compounded effects of age and gender could result in older women being the group worst affected by multimorbidity. However, no policy documents speak directly to multimorbidity in women. Although the Negotiated Service Delivery Agreement 2010-2014 mentions reducing the adult mortality rate, decreasing maternal mortality and reducing mother-to-child HIV transmission, 45 multimorbidity is not mentioned. The NDP 2030 notes that diet-related NCDs may rise, especially among ‘poor African women’ but does not mention multimorbidity, nor does it target specific groups for NCD interventions. 46 The National Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2022 – 2027 mentions the need to strengthen care in the context of multimorbidity 49 but does not focus on high-risk groups. In comparison, other national strategic plans (the plan for HIV, TB and Sexually Transmitted Infections) explicitly mentions reaching vulnerable populations (such as young women), addressing social and structural drivers of HIV 65 and have incorporated gender inequality, gender norms and gender-related vulnerability into their agenda. 66 Gender mainstreaming should be adopted into policies related to multimorbidity.
Multimorbidity and inequality
In high-income countries, multimorbidity is associated with poverty. 67 However, our analysis of the National Income Dynamics (NIDS) 2017 survey revealed higher odds of multimorbidity among wealthier people in South Africa. 23 Other studies on the African continent (Burkina Faso 68 and Ghana 69 ) have confirmed this pattern. This could be linked to lifestyle risk factors among the wealthy, where disposable income could facilitate access to fast foods 70 and increase the odds of being obese. 71 Obesity has also been linked to being wealthy (prosperous) in South Africa72,73 a factor also associated with multimorbidity. Obesity risk in African population groups may also be influenced by cultural norms that associate fatness with beauty. 74
The association between wealth and multimorbidity may also point to a different disparity altogether – which is access to healthcare. South Africa has a two-tiered health system comprising private and public health sectors. 75 Wealthier people may be more aware of their disease conditions as they tend to have better access to healthcare due to being able to afford the cost of private health insurance or medical aid. 76 Many private medical aid schemes in the country offer - or require - annual health screening (blood pressure, body mass index (BMI), glucose and cholesterol), 77 which could possibly increase awareness of health conditions among employed people. They may also have access to work programmes that do health and wellness screenings.77–79 If the cause for higher observed levels of multimorbidity among wealthy people is greater access to healthcare, it points to a gross level of unmet need among average South Africans. One local study found disparities in healthcare utilisation by socioeconomic level – with the disadvantaged far more likely to postpone care seeking due to monetary reasons. 76
The movement toward universal health coverage (UHC) has gained momentum globally. 80 UHC recognises that all people should have the access they need to health services without incurring financial hardship. 80 Achieving UHC is a target of the SDGs explicitly stated in SDG 3.8. 80 In 2019, a United Nations High-Level Meeting on UHC was held and a political declaration affirming high-level political commitment to UHC was adopted by member states. 80 South Africa has taken up the cause of UHC, in the form of a National Health Insurance (NHI) scheme. 81 NHI is a health-financing system designed to pool funds to provide quality, affordable healthcare services to South Africans, based on need, regardless of socioeconomic status. 82 The implementation of the NHI is being done using a phased approach. 82 In 2019, President Ramaphosa launched the ‘Presidential Health Summit Compact’ which lays out a five-year roadmap for accelerating UHC in South Africa. 81 Although the transition to the NHI was meant to be functioning by 2026, public health experts agree it will take much longer. 83
The implementation of the NHI and achievement of UHC will undoubtedly benefit South Africans in general, and those with multimorbidity. Assessments of progress toward UHC in South Africa found that there has been some progress in terms of service coverage. 84 However, there has been a lack of support from the public for the NHI. 85 These concerns are echoed by civil society groups which believe that the current health system is not ready for the NHI, and first needs to be improved. 85 These concerns are not unfounded and transparency and clarity have not been well managed. 85 If the NHI is successfully implemented, hopefully more screening will take place. This will allow people, regardless of socioeconomic status, to be aware of the diseases they have and enable access to quality treatment that does not negatively impact them financially.
Disease clusters
In examining the different disease clusters (classes) in the multimorbid population, hypertension was prominent in the majority of clusters. 26 The combination of diabetes and hypertension was common across three surveys;22–24 while heart disease and hypertension were common in two surveys.23,24 Hypertension co-occurred with other NCDs and with an infectious disease such as HIV – thus a mix of concordant and discordant multimorbidity classes exist in the population. Concordant multimorbidity tends to be similar in its origin or aetiology, whereas discordant multimorbidity is when the co-existing disease conditions tend to be unrelated. 10 An important caveat when interpreting this data is that the surveys analysed22–24 only collected information about selected disease conditions, hence these may not be the only prevalent disease clusters present in the population. For example, few national surveys collect information on mental health conditions and there are indications that the mental health burden is large in South Africa. 86
The disease clusters highlight the need for integrated care and a ‘one-stop-shop approach’ where treatment is available, no matter the underlying cause. The need for integrated care has been acknowledged by the Department of Health i.e. integrating HIV, TB and NCD services with maternal and child health services for efficient service delivery. 87 This was exemplified in the release of the 2016 South African National Department of Health Adherence Guidelines for HIV, TB and NCDs. 88 This policy and the service-delivery guidelines seek to address issues in non-adherence to long-term therapies amidst the expansion of ART programmes and the rising burden of NCDs. 88 Certain aspects of the programme implementation related to this policy have been positively evaluated.89,90 Another part of the strategy focused on linkage to care and implementing screening activities to identify diseases early for intervention. While the Adherence Guidelines do not cover every disease combination possible, these are steps in the right direction.
The Adherence Guidelines complement other South African guidelines and strategies that have been put in place to reduce disease burdens, such as the Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2013 -2017, 48 the Strategy for the Prevention and Control of Obesity in South Africa 2015 -2020 91 and, legislation to decrease sodium levels in the food industry. 92 Although South Africa has policies for the major NCD risk factors (tobacco smoking, unhealthy diets, harmful use of alcohol and physical inactivity), the implementation of these policies is stuttering. 93 Much more work is still needed to tackle the drivers of multimorbidity such as hypertension. The number of people with hypertension continues to increase, yet treatment rates remain extremely low (control rates are below 13% in sub-Saharan Africa). 94
A robust health information system in South Africa is needed to monitor changes in multimorbidity and disease patterns over time. With plans to implement the NHI scheme, an electronic health record (EHR) system would be essential for registering and tracking patients. 95 However, current sources of patient-level data are fragmented and poorly coordinated.96,97 Problems with the routine health-information system should be addressed to enhance the monitoring of the disease burden in South Africa.
Conclusion
Multimorbidity has been largely overlooked in South Africa due to limitations related to routine health information systems as well as the current focus on single diseases. Based on what we know currently as well as trends identified in other countries, multimorbidity is likely to be a significant contributor to ill health in South Africa. Comprehensive information on multimorbidity is needed for health-service delivery planning. While there is increasing focus on epidemiology,20,21 and the experience of multimorbidity in South Africa98,99 a better understanding of the epidemiology and patient experience of multimorbidity could also allow for interventions to be developed which allow for more effective and efficient treatment of patients.10,100
Multimorbidity is a growing concern in South Africa and therefore requires action. In this paper, we highlight pertinent issues that drive multimorbidity such as ageing, gender and access to healthcare. Multimorbidity poses a threat to the ailing health system in South Africa. Activists, researchers, and the public need to pressure decision-makers in government to act and provide responsive healthcare to the population.
Footnotes
Author contributions
All authors contributed to the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported herein was made possible through funding by the Burden of Disease Research Unit at the South African Medical Research Council. RAR conducted this research under the South African Medical Research Council through its Division of Research Capacity Development under the Internship Scholarship Programme from funding received from the South African National Treasury. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the South African Medical Research Council or the funders.
Ethical approval
This analysis was approved as part of the lead author’s doctoral studies and received additional ethics clearance by the Biomedical Research Ethics Committee of the University of the Western Cape (BM20/5/8).
Consent to participate
Participants gave informed written consent to take part in all three surveys.
Data availability statement
The data provided in this article were from three sources, including the anonymised 2016 SADHS dataset obtained from the DHS programme
101
https://dhsprogram.com/data/dataset/South-Africa_Standard-DHS_2016.cfm?flag=0 anonymised NIDS Wave 5 data (available for public distribution) from the research data service, DataFirst
102
https://doi.org/10.25828/fw3h-v708https://www.datafirst.uct.ac.za/dataportal/index.php/catalog/712 and anonymized SABSSM 2017 data from the Data Curation Services at the Human Sciences Research Council
103
http://dx.doi.org/doi:10.14749/1585345902![]() .
.