
Abstract
The primary objective was to quantify the influences of care delivery teams on the outcomes of patients with multimorbidity. Electronic medical record data on 68,883 patient care encounters (i.e., 54,664 patients) were extracted from the Arkansas Clinical Data Repository. Social network analysis assessed the minimum care team size associated with improved care outcomes (i.e., hospitalizations, days between hospitalizations, and cost) of patients with multimorbidity. Binomial logistic regression further assessed the influence of the presence of seven specific clinical roles. When compared to patients without multimorbidity, patients with multimorbidity had a higher mean age (i.e., 47.49 v. 40.61), a higher mean dollar amount of cost per encounter (i.e., $3,068 v. $2,449), a higher number of hospitalizations (i.e., 25 v. 4), and a higher number of clinicians engaged in their care (i.e., 139,391 v. 7,514). Greater network density in care teams (i.e., any combination of two or more Physicians, Residents, Nurse Practitioners, Registered Nurses, or Care Managers) was associated with a 46–98% decreased odds of having a high number of hospitalizations. Greater network density (i.e., any combination of two or more Residents or Registered Nurses) was associated with 11–13% increased odds of having a high cost encounter. Greater network density was not significantly associated with having a high number of days between hospitalizations. Analyzing the social networks of care teams may fuel computational tools that better monitor and visualize real-time hospitalization risk and care cost that are germane to care delivery.
Background
Eighty-one percent of Americans ages 65 years and older are living with multimorbidity (i.e., two or more chronic conditions). 1 Over the past decade, the prevalence of individuals living with multimorbidity has expanded beyond aging populations, such that now 50% of Americans ages 45 to 65 and 18% of Americans ages 18 to 44 have multimorbidity.1,2 Furthermore, the sickest top five percent of patients make up 50% of the total annual healthcare costs. 3 Multimorbidity has been associated with functional decline and diminished quality of life, relative to individuals with one or no chronic conditions.4,5 Additionally, previous studies have shown that multimorbidity has significant power for predicting death, leading much of the literature to target clinical and lifestyle interventions for multimorbidity.6,7 Clinical interventions (e.g., medication burden of complex therapies for each single chronic condition), financial burden, patient education, and diet have been most consistently explored. 8 These attempts have had limited success and have been met with difficulties related to nationwide replication, indicating that a more comprehensive approach is needed, which now expands the focus to factors related to a patient’s care delivery team that have been identified as influencing care outcomes.9,10
More specifically, a patient’s care team and their interactions was defined [and operationally referred to] as a patient’s “social network” during care delivery. 11 Of particular interest to healthcare delivery, social networks are composed of two components: the people (i.e., known as “nodes”) and the relationships between the people (i.e., also known as “ties” or “edges”). 11 The ties within these social networks (e.g., communication, coordination, and information exchange) have shown great potential for improving care in individual chronic conditions, including cardiovascular disease, substance use, and diabetes.11–13 Yet, there is a gap in knowledge regarding the ways in which the presence of specific clinical roles influence the outcomes of patients with multimorbidity in care delivery.11–13 To address the knowledge gap, this study examined the influence of care teams on the care outcomes (i.e., hospitalizations, days between hospitalizations, and cost) of patients with multimorbidity. More specifically, this study 1) examined the differences between the care teams of multimorbidity and non-multimorbidity patients and 2) evaluated the impact of social network structures associated with the care outcomes of patients with multimorbidity.
Quantifying influences of care teams in chronic diseases using medical records
Within informatics, electronic medical record (EMR) systems fuel social network analysis and facilitate information exchange among patient care teams. Information contained within the EMR includes patient demographic data, progress notes, health assessments, medications, medical history, and other contextual information. 14 The EMR has produced relatively salient improvements in care outcomes as a result of its ability to map and analyze the social networks of care teams in various settings. For example, in ambulatory care setting (i.e., 74,618 patients, 466 related clinicians), care teams with larger social networks, compared to care teams with smaller social networks, were associated with significantly better care outcomes in hemoglobin A1c testing of patients with diabetes (90.1% v. 84.2%), breast cancer screenings (78.6% v. 74.2%), chlamydia screenings (65.8% v. 53.0%), and colorectal cancer screenings (51.3% v. 48.0%). 15 A similar study of 169,711 patients with diabetes showed that EMR information exchange within the social networks of care teams was associated with improved rates of follow-up monitoring by the care team and improved rates of glycemic indicators [measured by HbA1c levels] and lipid control. 16 Other studies have shown that increases in care team presence and engagement were associated with care outcomes beyond physiological parameters, including reductions in emergency department (ED) and urgent care visits related to post-care. For example, a follow up study of EMR information exchange among care teams in 169,711 patients with diabetes, reflecting 100,510 hospitalizations, 211,623 ED visits, and 2,574,472 office visits prior to EMR implementation, found that, after EMR care team implementation, there were 13.10 fewer hospitalizations and 519.12 fewer ED visits per 1,000 patients annually. 17 An EMR study of 7,457 patients with cardiovascular disease and 41 related clinicians found that large interaction among care teams were associated with 38% fewer hospitalization days and $556 lower total medical costs per encounter. 11 For patients with alcohol use disorder, EMR information exchange among care teams was related to 10% fewer alcohol-related hospitalization days. 13 In contrast, a sample of 2,242 patients with diabetes and 83 related clinicians demonstrated that EMR information exchange among care teams did not, on its own, produce improvements in care outcomes. 12 More specifically, patient hospitalizations increased by 13% and total medical costs increased by $223 for every 1% increase in the social network of the care teams. 12 Results of these studies, while impactful, were limited by the lens of patients with single chronic conditions. Additional inquiry is needed to understand how care teams influence the care outcomes of patients with multiple chronic conditions.
Materials and methods
Study design and data source
Study procedures (Protocol# 262593) were approved by the Institutional Review Board (IRB) at the University of Arkansas for Medical Sciences (UAMS). This UAMS IRB is a research ethics committee that has been fully accredited by the Association for the Accreditation of Human Research Protection Programs since 2005. The UAMS IRB waived informed consent because the study posed only minimal risk through the secondary use of EMR data (i.e., deidentified patient data). EMR data collected from patient care encounters between January 1, 2015, and July 1, 2021, were extracted from the Arkansas Clinical Data Repository (AR-CDR). 18 Eligibility criteria limited all subjects to those ages 18 years and older. Data included information on two patient groups (i.e., multimorbidity and non-multimorbidity) and on the clinicians related to each of their care encounters. Multimorbidity was defined as two or more chronic conditions for an individual patient. Non-multimorbidity was defined as one or no chronic conditions for an individual patient. These two patient groups were mutually exclusive, but shared the same pool of clinicians who provided there care. All data were initially captured through routine healthcare delivery systems at UAMS, Arkansas’s only academic medical and adult Level I Trauma Center. UAMS includes family medical centers at 6 regional campuses throughout the state. However, data only reflected patient encounters from the primary UAMS campus, a hospital capacity of 535 beds (i.e., 431 adult beds, 64 newborn bassinets, 40 psychiatry beds).
Measures of chronic conditions and multimorbidity
Data extracted from the AR-CDR included information on chronic conditions and outcomes of patients with multimorbidity. Chronic condition data were categorized with International Classification of Diseases Rv.10 codes that were selected according to formal recognition of 21 chronic conditions by the Centers for Medicare and Medicaid Services. 19 These criteria identified a total study sample of 54,664 patients: 30,030 patients with multimorbidity and 24,634 patients without multimorbidity (i.e., non-multimorbidity).
Variables
Patient care teams were operationally defined as the groups of clinicians who provided patients with care during each care encounter. The AR-CDR dataset contained pseudonym identification (ID) numbers for all clinicians and patients. Through these IDs, patients were linked to specific clinicians in the dataset before being received by the study team, forming care teams. These care teams were initially documented within the EMR during normal clinical workflows of care encounters as patients were assigned to specific clinicians for care. Through these care encounters, patients in both groups were provided with care by various combinations of 60 types of care team roles (i.e., specific clinicians). However, this study focused on seven specific roles: “physician”, “resident”, “nurse practitioner”, “registered nurse”, “patient care technician”, “care manager”, and “physical therapist”. These roles were selected because they 1) had a high number of patient interactions (i.e., at least 1,000 ties with patients), 2) were significantly associated with at least one of the outcomes in the model,
Social network analysis (i.e., network density) was performed on the care teams to contextualize the impact of care team size on care outcomes. More specifically, we assessed the influence of the median network density structure (i.e., minimum care team size of 2) on each of the three care outcomes with binomial logistic regression. 13 During the analysis, both patients and clinicians were treated as nodes. A network tie was defined as a connection between a patient and a clinician, forming undirected social networks. Network density was defined as a measure of the overall connectedness between the multimorbidity patients and the clinicians who provided their care during each encounter. 13 Network density was calculated by dividing the number of patient-to-clinician ties in each care team by the total number of ties in the overall network of the patients in each group (i.e., multimorbidity v. non-multimorbidity).13,21 Network density values range from 0 to 1, with higher values reflecting a higher number of the network’s clinicians engaged in a care encounter (i.e., high density networks/large care teams).21,22 Social network analysis was important to use because it formally quantified the influence of care teams on patients by evaluating individual care encounters in relation to all of the potential network’s clinicians who could have engaged in a care delivery encounter within an ecosystem of care. Simply using counts of clinical roles as a substitute would have only allowed for the evaluation of individual care encounters, excluding the potential impact of the ecosystem of care in which the individual care encounters were provided.21–23
Patient care outcome variables
Three binary patient outcome variables (i.e., “a high number of hospitalizations”, “a high number of days between hospitalizations”, and “a high cost encounter”) were constructed by dichotomizing the continuous variables initially provided in the AR-CDR dataset (i.e., “the number of hospitalizations”, “the number of days between each patient’s hospitalizations”, and “the dollar amount of each cost encounter”) at their medians (see “statistical analysis” section for details). The number of hospitalizations was calculated by counting the number of hospital admission dates listed within the AR-CDR file. A hospitalization was operationally defined as an official decision by a licensed physician to admit a patient for observation and/or treatment and assign a hospital bed to the patient. For days between hospitalization, the number of days between each patient’s hospitalizations were counted, chronologically, from the hospital admission dates provided in the AR-CDR dataset. For care encounter cost, the total dollar amount (i.e., in USD) for each care encounter was provided directly by the AR-CDR in the dataset. The total dollar amount reflected the dollar amount charged for each care encounter and paid by patients, their insurance companies, or other stakeholders on behalf of the patients. The charges reflected the dollar amounts of services provided that were germane to the delivery of care (e.g., X-rays, specific procedures, medications, etc.), excluding non-care related charges such as (e.g., parking, elective food costs during stay). A full list of over 60,000 itemized charges that were included in the study is publicly available. 24 These three outcomes were selected because they have historically been established as standard indicators of health in patients with chronic conditions.3,12,25 For example, healthy patients generally have a lower number of hospitalizations, spend more time at home between hospitalizations (i.e., a high number of days between hospitalizations), and have a lower dollar amount of cost associated with each care encounter.
Statistical analysis
All analysis was performed in IBM SPSS v.27 software. Descriptive statistics were calculated for each group. The dataset primarily contained binary variables which met the statistical assumptions of the binomial logistic regression. 26 The purpose of using the binomial logistic regression was to model influences of care teams on the care outcomes (i.e., a high number of hospitalizations, a high number of days between hospitalization, and a high cost care encounter) of patients with multimorbidity.11–13,27 This form of regression was required because of the dichotomous outcomes that were being predicted. More specifically, there was a need to understand the odds that an observation fell into one of two categories of a dichotomous dependent variable (e.g., a high number of hospitalizations v. a low number of hospitalizations, dichotomized at the median) based on independent variables (e.g., race, gender, clinical diagnoses, specific care team roles, and the cumulative presence of care team). 26 Within the regressions, adjusted odds ratios were used to represent associations between these dependent and independent variables.11–13,27 All continuous variables including patient outcome variables were dichotomized at the median to create binary variables, as required in binomial logistic regression analysis. 27 For example, to create the dichotomous variable for “high cost”, costs above the median cost for a care encounter in our multimorbidity sample (i.e., $1,813) were coded as “1,” representing “yes” (i.e., a high cost encounter) and cost below this amount were coded as “0”, representing “no” (i.e., a low cost encounter).
Results
This study included a sample of 4,166 clinicians and 54,664 patients segmented into two groups: multimorbidity (i.e., 30,030) and non-multimorbidity (i.e., 24,634). Patients in the multimorbidity group had an average of 5.17 chronic conditions and those in the non-multimorbidity group had 0.35 (i.e, less than 1 chronic condition). Collectively, the 54,664 patients generated 68,883 care encounters: 41,642 and 27,241 within multimorbidity and non-multimorbidity groups, respectively.
Patient-level and patient encounter-level demographics stratified by group.

aNumbers and percentages for individuals of Hispanic, Latin, and Spanish ethnicity were not mutually exclusive to racial categories.
Care team roles and outcome variables encounters stratified by group.
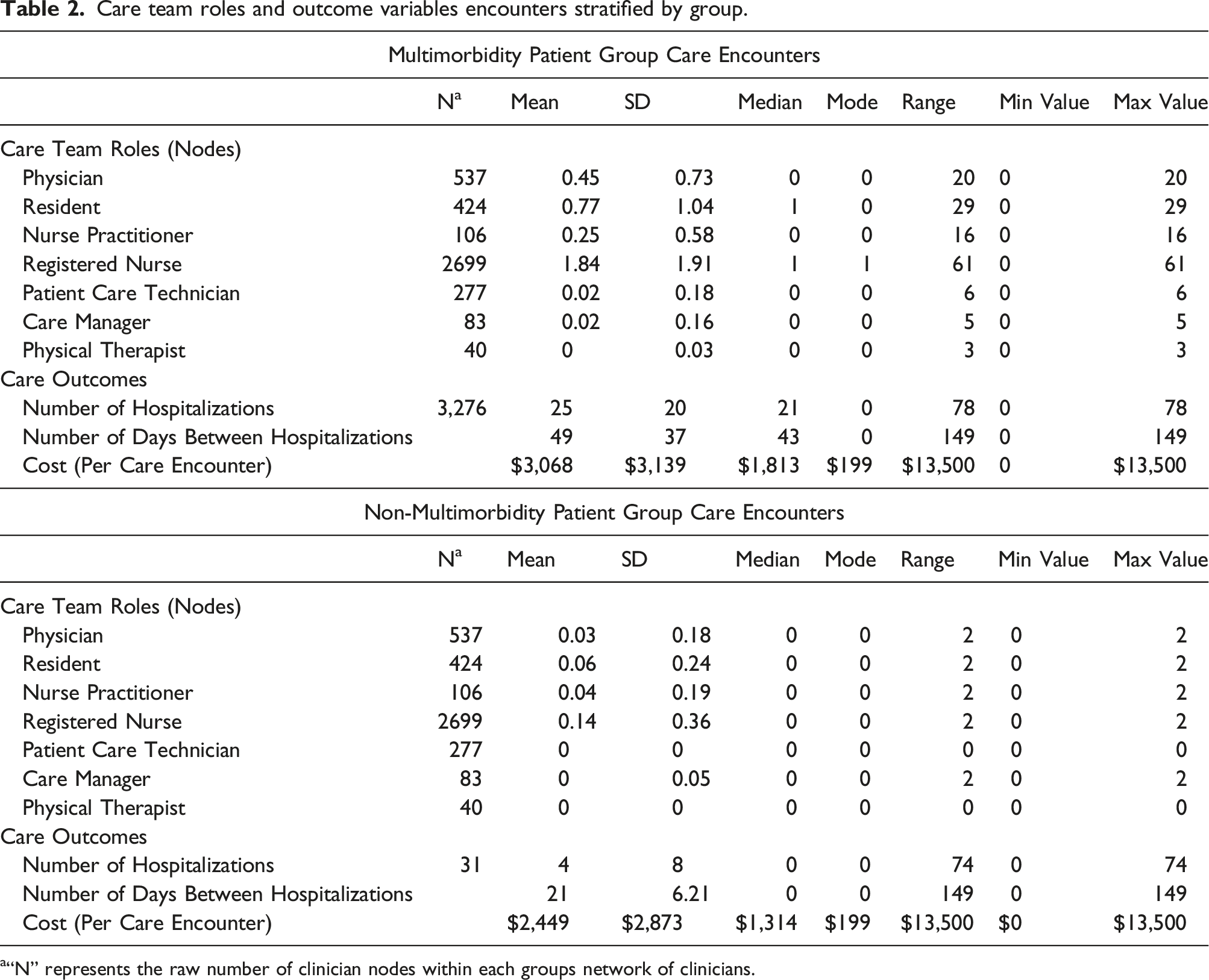
a“N” represents the raw number of clinician nodes within each groups network of clinicians.
The median cost per care encounter was $1,813 for patients with multimorbidity, which is greater than the median cost of $1,314 for patients with non-multimorbidity. The median number of hospitalizations during the study period per patient with multimorbidity was 21. However, patients with non-multimorbidity had a median of 0 hospitalizations which indicated that approximately 50% of non-multimorbidity patients had less than 1 or no hospitalizations at all during the study period. For patients with non-multimorbidity, the median number of days between hospitalizations was also 0, the result of these patients having less than 1 to no hospitalizations during the study period. Conversely, for patients with multimorbidity, the median number of days between hospitalizations were 43.
Figure 1 illustrates the number of times each of the seven care team roles provided care to patients (i.e., network ties), by group and role. The 68,883 care encounters generated 146,905 patient-to-clinician ties with the seven clinical roles. This included 139,391 and 7,514 for the multimorbidity and non-multimorbidity groups, respectively. Within these ties, registered nurses were the most highly engaged care team role in care encounters, as represented by 1) the 76,514 instances (i.e., 55% of total instances) in which they provided care to the 30,030 multimorbidity patients and 2) the 3,887 instances (i.e., 52% of total instances) in which they provided care to the 24,634 non-multimorbidity patients. Physical Therapists were the least engaged clinical role in care encounters in both groups. Total patient-clinician ties stratified by clinical role.
Associations between care teams and outcomes of patients with multimorbidity
Binomial logistic regression of care team and outcomes of patients with multimorbidity.
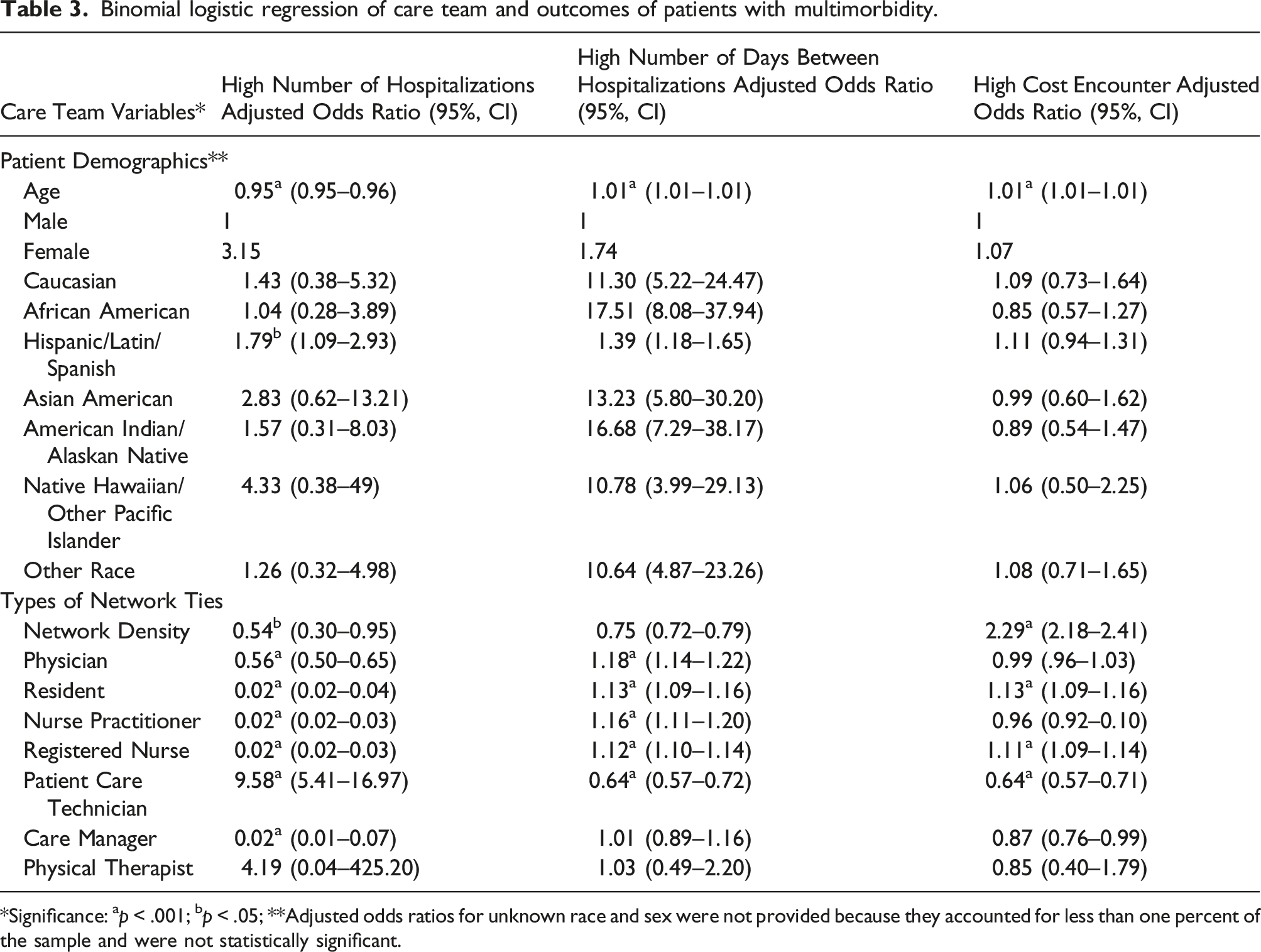
*Significance: ap < .001; bp < .05; **Adjusted odds ratios for unknown race and sex were not provided because they accounted for less than one percent of the sample and were not statistically significant.
Individual presence of care team roles
The presence of a physician within a care team was associated with a 54% decrease in odds of a multimorbidity patient having a high number of hospitalizations (i.e., above the median of 21) and an 18% increase in odds of having a high number of days between hospitalizations (i.e., above the median of 43). The odds of having a high number of hospitalizations was also decreased by 98% when a resident, nurse practitioner, registered nurse, or care manager was present on a multimorbidity patient’s care team. Additionally, the presence of a resident, nurse practitioner, or registered nurse on a patient’s care team increased the odds of having a high number of days between hospitalizations by 12% to 18%. The presence of a patient care technician within a patient’s care team was associated with 9.58 times the odds of a patient with multimorbidity having a high number of hospitalizations and with a 46% decrease in the odds of having a high number of days between hospitalizations. Moreover, for patients with multimorbidity, the presence of a resident and a registered nurse within the care team was associated with 13% and 11% increased odds of having a high cost encounter, respectively.
Cumulative presence of the care team
In terms of the cumulative presence of the care team, Table 3 shows that greater network density (i.e., two or more of the care team members providing care during an encounter which was reflected by any value above the network density median of 0.000000002620) was associated with a 46% decrease in odds of a patient with multimorbidity having a high number of hospitalizations (Figure 2(a)). Please see Table 3 and Figure 2 for which two or more specific care team roles were associated with the outcomes. There was no significant network density (i.e., care team size) associated with a high number of days between hospitalizations, only the significance found in specific care team roles (Figure 2(b)). Greater network density in patient care teams also was associated with 2.29 times the odds of having a high cost encounter (Figure 2(c)). Significant network density structures associated with multimorbidity care outcomes.
Associations between chronic condition type and outcomes of patients with multimorbidity
Binomial logistic regression of chronic condition types and outcomes of patients with multimorbidity.

*Significance: ap < .001; bp < .05 **AIDS= acquired immunodeficiency syndrome; ARTH=rheumatoid arthritis/collagen vascular diseases.
In terms of a high number of days between hospitalizations, patients whose multimorbidity included the following conditions were at an increased odds (i.e., 13%-2.45 times) of having a high number of days between hospitalizations: acquired immunodeficiency syndrome, chronic pulmonary disease, depression, complicated diabetes, drug abuse, complicated hypertension, and hypothyroidism. Patients whose multimorbidity included congestive heart failure had a 19% decrease in odds of having a high number of days between hospitalizations.
In terms of a high cost encounter, patients were at an increased odds (i.e., 8-36%) of having a high cost encounter if their multimorbidity included congestive heart failure complicated hypertension, hypothyroidism, liver disease, fluid and electrolyte disorders, and solid tumor without metastasis. Conversely, patients had decreased odds (i.e., 5-12%) of having a high cost encounter if their multimorbidity included depression, drug abuse, and psychoses.
Sensitivity and Specificity Analysis
All six regression models in Tables 3 and 4 had a statistically significant chi-squared omnibus test coefficients (i.e., p-values < 0.001), indicating our models were stronger than (i.e., outperformed) the null models with no predictors. Sensitivity and specificity analyses tested the assumptions that the three models in Table 3 had fully controlled for patient characteristics (e.g., age, race, and sex) and did not confound the relationship between care teams and care outcomes. Sensitivity and specificity did not change when age, race, and sex were added to the models in Table 3, indicating the models accurately predicted the outcomes.
Discussion
Overall, the study 1) examined the differences between the care teams of multimorbidity and non-multimorbidity patients and 2) evaluated the impact of social network structures associated with the care outcomes of patients with multimorbidity. Notably, multimorbidity patients had larger care teams than non-multimorbidity patients as noted by the minimum and maximum values. For example, some multimorbidity patients were provided care by up to 61 registered nurses during their care encounter (i.e., likely a large length of stay) while non-multimorbidity patients had up to only two registered nurses who provided care during their care encounter. Registered nurses were also the only care team role with a mean greater than or equal to “1”, indicating that multimorbidity patients were heavy utilizers of registered nurses as a care resource. Notably, non-multimorbidity patients generally did not have physical therapist not patient care technicians providing care during their care encounters, as indicated by their means, medians, modes, ranges, and maximum values of “0”. Broadly, a large number of clinicians providing care during an encounter (i.e., high network density; 2 or more of clinicians) was associated with decreased odds of patients with multimorbidity having high numbers of hospitalizations and increased odds of having a high cost encounter. These findings were consistent with prior findings for patients with single chronic conditions including substance use and diabetes.12,13 However, only individual clinicians were associated with a multimorbidity patient having a high number of days between hospitalizations. The results indicated that care teams and individual clinicians can be used as predictors to surveil and monitor the outcomes of patients with multimorbidity.
Implications for use of informatics in care coordination
As the number of conditions within each individual increase, so does the complexity of care coordination.28,29 When care teams work cohesively and with informatics tools, care coordination drives improvements in care outcomes (i.e., hospitalizations, cost).11–13,30–34 Interestingly, for decreased odds of having a high number of hospitalizations, care managers were identified as being just as highly associated with odds as residents, nurse practitioners, and registered nurses. This finding emphasizes the value of the care manager’s role of coordinating patient care, deliberately organizing care activities through the exchange of information among clinicians who were responsible for different aspects of care.28,29,31 The primary aim of coordinating care is delivering the right healthcare services at the right time, in the right order, and in the right setting. 32
With the EMR at the core, informatics interventions and tools for multimorbidity are currently focused on patient management of their chronic conditions, developing algorithms to support clinical decision-making, and care coordination.34,35 Our results, in conjunction with previous studies, confirm that EMR data can serve as the backbone of social network analysis in patients with single chronic conditions as well as patients with multiple chronic conditions.11–13,27 EMR data can fuel additional informatics approaches to care coordination that support clinics and hospitals in managing and monitoring care team engagement with patients in real time and simultaneously assessing them potential impact of clinician engagement on the care outcomes of patients. For example, as evident in our results, network ties between patients and their physicians within patient care teams were associated with better outcomes for multimorbidity patients (i.e., decreased odds of having a high number of hospitalizations and increased odds of having a high number of days between hospitalizations). The presence of residents, nurse practitioners, and registered nurses on a patient’s care team increased the odds of having a high number of days between hospitalizations by 12% to 18%. The individual presence of residents, nurse practitioners, registered nurses, and care managers [and cumulative presence of 2 or more] resulted in a 98% decrease in the odds of a multimorbidity patient of having a high number of hospitalizations. This may also indicate that diversity of the professional roles in care coordination leads to decreased utilization of healthcare services. This finding was particularly meaningful because multimorbidity patients were heavy utilizers of healthcare, the top five percent of medically complex patients (i.e., the sickest) make up 50% of the total annual healthcare costs. 3 More specifically, managing care costs may be supported by monitoring care team engagement, not only the number of members within a patient’s care team but also in the types of clinical roles that make up the care team. This is critical to improving care, which is consistent with the large body of evidence on interprofessional education and professional team dynamics. 36 Notably, the range of the hospital costs in this study (i.e., $0-$13,500) were still below the national average of $14,101. 37
Implications for clinical decision-making
EMR data can be directly integrated with support tools for clinical decision-making to receive automated updates, fueling risk identification and management. 38 When predicting risk is targeted toward improving care outcomes, it is particularly impactful on the allocation of healthcare system resources. 39 Examining the ways in which care teams influence care outcomes is more fully realized as a result of the development of operational tools that support clinical decision-making. As the backbone of support tools for clinical decision-making, algorithms have been used to identify and manage risks (i.e., hospitalizations, length of stay) for patients with chronic conditions.35,40 Interestingly, greater network density in care teams was associated with 46% decreased odds of a patient with multimorbidity having a high number of hospitalizations. This indicates that a larger number of ties between patients and 2 or more specific clinicians in the network resulted in fewer hospitalizations. This finding is consistent with prior evidence from academic health centers and ambulatory settings which have suggested that the monitoring of social networks by EMR-based clinical decision-making tools can lead to fewer hospitalizations, relative to control groups that do not use these tools.35,41 Therefore, the influences of care teams should be embedded into EMR systems to actively measure, monitor, and stratify risks of poor outcomes in patients with multimorbidity, as clinicians are their primary conduit of healthcare delivery. More broadly, advancing the capacity of the EMR to apply social network analysis would allow healthcare systems to visualize live, real-time risks associated with hospitalization and cost care. This form of real-time risk stratification will complement the independent clinical assessments performed by care teams, comprehensively improving care outcomes.35,42
Limitations
Study data was generated from Arkansas’s only academic medical center, whose status and rurality may offer a group of clinicians and patients that are more diverse than in many other settings. While the study data was sufficient for the analysis methods, the lack of national databases with patient-to-clinician matching limited even larger-scale assessment. However, as individuals interact more with healthcare systems, data collection within EMR systems will increase, increasing opportunities for accurate prediction of risks and evolving data interoperability. Therefore, all findings may not be generalizable to the larger population of patients with multimorbidity in the United States (US), but may reflect the large populations of clinicians and patients in rural academic health centers throughout the US. Second, adjusted odds ratios were provided in lieu of regression coefficients (i.e., “R2”) for the binomial logistic regressions (i.e., Tables 3 and 4) because of the dichotomous nature of the variables and the study’s specific focus on examining the odds of a patient having any of the three outcomes. This is consistent with all known studies which use similar methods, many of which were cited within this publication. Consequently, the study did not estimate specific increases in the outcome variables (i.e., high number of hospitalizations, high number of days between hospitalizations, high cost encounter) based on raw unit increases or decreases in the predictor variables (e.g., adding 2 additional registered nurses to a care team).
Notably, there are an infinite number of potential confounders within the multimorbidity and non-multimorbidity groups. These potential confounders included but was not limited to the severity of each of a patient’s single chronic conditions that compose their multimorbidity (e.g., functional and or cognitive impairment status, frailty, and oxygen support needs), length of hospital stay and any hospital acquired infections, medications use, health behaviors (e.g., smoking, alcohol use), and other social determinants of health. There were also a significant number of potential confounders related to the clinicians who provided care. Furthermore, we recognize that geriatricians and other specialty physicians have a vital role in caring for patients with multimorbidity because its traditionally associated with aging populations. However, the AR-CDR aggregated all types of physicians into the general role of “physician”. Therefore, our results did not distinguish between generalist and specialty physicians (i.e., geriatricians). Other clinician-related limitations included but was not limited to clinician training and experience, an itemization of care-related tasks performed by each clinical role, clinician staffing and availability to provide care, how clinicians interacted with other clinicians within the teams, and the influence of the presence of clinicians that were excluded by this study criteria for the seven clinical roles that were selected. Future studies should address these confounders in each of the specific combinations and permutations of multimorbidity that were found within the 21 chronic diseases and their influence on the care outcomes.
Conclusions
Care teams may be used to improve care outcomes for patients with multimorbidity. Informatics interventions and tools focused on developing algorithms to support clinical decision-making and care coordination will be particularly impactful in improving outcomes of individuals with multimorbidity.
Supplemental Material
Supplemental Material - Quantifying care delivery team influences on the hospitalization outcomes of patients with multimorbidity: Implications for clinical informatics
Supplemental Material for Quantifying care delivery team influences on the hospitalization outcomes of patients with multimorbidity: Implications for clinical informatics by Tremaine B Williams, Taiquitha Robins, Jennifer L Vincenzo, Riley Lipchitz, Ahmad Baghal and Kevin Wayne Sexton in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We would like to acknowledge the guidance and support of Dr. Amy Franks and the CCOP Writer’s Block Group that was provided during the drafting of this manuscript offered through the UAMS Center for Childhood Obesity Prevention funded by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number P20GM109096 (Arkansas Children’s Research Institute, PI: Weber). The manuscript was edited by the Science Communication Group at the University of Arkansas for Medical Sciences.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KWS has equity in HoopCare, Inc; hDrop Technologies, Inc; Decisio Healthcare, Inc; and Datafy, LLC. KWS has licensed intellectual property owned by Vanderbilt University and the University of Arkansas for Medical Sciences.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the project described was supported by the Translational Research Institute (TRI), grant TR003107 and KL2 TR003108 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Data availability statement
The data that support the findings of this study is available upon email request to the UAMS IRB (
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.