
Abstract
Purpose
Early identification of colorectal cancer (CRC) is an international priority. Multimorbidity (presence of ≥2 long-term conditions (LTCs)) is increasing and the relationship between CRC and LTCs is little-understood. This study explores the relationship between individual LTCs, multimorbidity and CRC incidence and mortality.
Methods
Longitudinal analysis of the UK Biobank cohort, participants recruited 2006–2010; N = 500,195; excluding previous CRC at baseline. Baseline data was linked with cancer/mortality registers. Demographic characteristics, lifestyle factors, 43 LTCs, CRC family history, non-CRC cancers, and multimorbidity count were recorded. Variable selection models identified candidate LTCs potentially predictive of CRC outcomes and Cox regression models tested for significance of associations between selected LTCs and outcomes.
Results
Participants’ age range: 37–73 (mean age 56.5; 54.5% female). CRC was diagnosed in 3669 (0.73%) participants, and 916 (0.18%) died from CRC during follow-up (median follow-up 7 years). CRC incidence was higher in the presence of heart failure (Hazard Ratio (HR) 1.96, 95% Confidence Interval (CI) 1.13–3.40), diabetes (HR 1.15, CI 1.01–1.32), glaucoma (HR 1.36, CI 1.06–1.74), male cancers (HR 1.44, CI 1.01–2.08). CRC mortality was higher in presence of epilepsy (HR 1.83, CI 1.03–3.26), diabetes (HR 1.32, CI 1.02–1.72), osteoporosis (HR 1.67, CI 1.12–2.58). No significant association was found between multimorbidity (≥2 LTCs) and CRC outcomes.
Conclusions
The associations of certain LTCs with CRC incidence and mortality has implications for clinical practice: presence of certain LTCs in patients presenting with CRC symptoms could trigger early investigation and diagnosis. Future research should explore causative mechanisms and patient perspectives.
Background
Colorectal cancer (CRC) is the second most common cause of cancer death globally1–3 with an estimated 54% of cases being preventable. 2 Early identification of cancer, and specifically CRC, is a major international primary care focus.4–7 CRC survival is improving, and early diagnosis has major prognostic benefits. 8 Chronic disease burden, including multimorbidity, (the presence of ≥2 long-term conditions (LTCs)), is also a growing international problem 9 and is strongly associated with increasing age, frailty and adverse health outcomes. 10
CRC incidence is increasing3,11 and global patterns of CRC incidence track closely with socioeconomic development. In public health terms, CRC is considered a major disease marker of transition to more ‘westernised’ lifestyles, 12 reflecting the powerful influence that lifestyle factors play in CRC aetiology.13,14 Multiple factors interact to contribute to an individual’s CRC risk, including non-modifiable (age, male sex, ethnic background, history of colonic polyps, inflammatory bowel disease (IBD), CRC family history, hereditary conditions, for example, familial adenomatous polyposis (FAP) and hereditary non-polyposis colorectal cancer (HNPCC)) 15 and modifiable (overweight and obesity, physical inactivity, diet, smoking, alcohol intake) risk factors.16,17
Validated population-specific patient risk-stratification tools, for example, the Colorectal Cancer Risk Assessment Tool (CCRAT) 18 and QCancer tool19,20 have been developed to facilitate early CRC detection. These tools utilise various data to calculate individual risk: CCRAT encompasses demographic and lifestyle factors, over-the-counter medication use, history of colonic polyps and CRC family history, whereas QCancer makes a briefer lifestyle assessment alongside information on medical history and LTCs, for example, specific cancers in women (breast, uterine, ovarian, cervical) and in men (oral, lung, haematological), diabetes, ulcerative colitis and colonic polyps. The development of these evidence-based tools has established the instrumental role of comorbidity assessment in primary care evaluation of CRC risk.
A Spanish cohort study of LTCs and multimorbidity in CRC patients 21 highlighted highly prevalent late and advanced-stage CRC presentation in patients with multiple LTCs; particularly dementia. The impact of multimorbidity on an individual’s identification, perception of and presentation with CRC symptoms matters because late diagnosis impacts significantly on CRC survival. 8
An inverse association between presence of LTCs and CRC survival rates was demonstrated in a Dutch population. 22 Suggested explanations for this included less aggressive treatment being offered to multimorbid patients due to risk of complications and limited evidence of treatment efficacy in frailer patients with LTCs, memory impairment considerations, and multimorbid patients themselves being more likely to decline treatment. A Danish cohort study on CRC mortality using population health data 23 found a significant association between presence of LTCs 24 and CRC mortality.
Presence of LTCs is associated with delayed CRC diagnosis 25 and with increased CRC mortality.26,27 Prior research examining the relationships between LTCs and CRC has considered a limited number of LTCs, including inflammatory bowel disease, 28 colonic polyps, FAP and HNPCC 29 and diabetes.30,31 As CRC survival improves, coexistence of CRC and LTCs increases, therefore enhancing understanding of the relationships between these different conditions may aid CRC risk-stratification, diagnosis and screening, and inform public health efforts addressing modifiable (e.g., lifestyle) CRC risk factors, many of which are shared in common with multimorbidity. 32
The nature of any association between these conditions is complex and remains obscure. Research investigating the interactions between CRC outcomes and a comprehensive list of LTCs is urgently needed. The objective of this study is to explore the relationship between CRC and a range of 43 distinct LTCs, and multimorbidity, by firstly describing prevalence of LTCs in participants with and without CRC in the UK Biobank (UKB) dataset, then exploring associations between LTCs and multimorbidity, and CRC outcomes of interest, namely CRC incidence and mortality.
Methods
This study is a prospective population based study, and was designed according to the STROBE guidelines for reporting of epidemiological studies. 33
Population
The UKB is a large ongoing prospective UK-based health resource with over 500,000 participants from across England, Scotland and Wales, providing anonymised health and demographic data to support health research. 502,655 participants were recruited between March 2006 and October 2010, with a response rate of 5.5%. 34
Data collection
Access to the UKB dataset for this analysis was granted through generic ethics approval for UKB studies from the North West Multi-Centre Research Ethics Committee (original approval 2011 REC ref 11/NW/0382; renewed in 2016 REC ref 16/NW/0274). 35 During UKB baseline registration assessments participants completed two questionnaires, one nurse-led and one touch screen, providing self-reported demographic, lifestyle, and health-related information. 36 Participants provided informed consent for prospective data linkage of their self-reported information with national data registries, including those on cancer incidence and mortality37,38 which were utilised for this study.
We included information on 500,195 UKB participants (excluding 2345 noted at baseline to have a previous CRC diagnosis). We examined demographics, socioeconomic status, lifestyle factors, CRC family history and presence of LTCs from a previously published list39,40 in the dataset (see Supplementary Material 1, Supplementary Table S1 for full list of conditions). Participants were followed up for a median of 7 years; we obtained data on CRC incidence and CRC mortality in participants over this follow-up period through the established data linkages to cancer and mortality registries, respectively.
Variables
Demographic variables including age, sex and socioeconomic status were examined at baseline. Age was categorised into three groups, with upper and lower limits defined by the age range of the study population: age groups 37–49, 50–59 and 60–73. Socioeconomic status was measured by Townsend Score, 41 a UK-specific measure of material deprivation incorporating census-derived data on unemployment, non-car ownership, non-home ownership and household overcrowding where a higher score correlates to greater socioeconomic deprivation and scores are grouped into ordinal quintiles for purposes of analysis. Health-related and lifestyle factors included were smoking status (current smoker, ex-smoker, never-smoker), alcohol intake (never/occasionally, one to three times per month, one to four times per week, daily/most days), body mass index (BMI) category 42 (underweight (<18.5kg.m2), normal weight (18.5–25 kg.m2), overweight (25–30 kg.m2), obese (>30 kg.m2)) and level of physical activity (in the past 4 weeks: none, low (e.g., light DIY activity), medium (e.g., heavy DIY activity, walking for pleasure or other exercises), high (e.g., strenuous sport). 43
Presence of 43 pre-defined LTCs, based on previously published multimorbidity research39,44 (please see Supplementary Material 1, Supplementary Table S1), were included as predictor variables. Multimorbidity status was defined according to methods previously used in other large health dataset analyses,39,44 using the provided LTC data to create a composite multimorbidity variable describing a count of LTCs, ranging from zero LTCs, one LTC, two LTCs, three LTCs to four or more co-existing LTCs in an individual participant.
Additional variables previously shown to be important in the development of CRC, namely: use of certain medications, for example, aspirin, 18 presence or absence of relevant cancers, for example, oral, lung and haematological cancers for men, and breast, uterine, ovarian or cervical cancers for women, 19 and family history of CRC 19 were also included in our variable selection models.
Outcomes
Data was obtained on the outcomes CRC incidence and CRC-specific mortality obtained from registers using ICD-10 codes C18 – C21, 45 encompassing all cancers of the colon and rectum.
Analysis
Statistical analysis was performed using R programming environment software. First, demographic and lifestyle features of the study population were described. We then sought to design a practical and interpretable analysis by removing redundant predictors from the analysis using variable selection. 46 The large number of variables included in the UKB dataset introduces potential for unmanageably large data output, with accompanying noise in the statistical modelling caused by inclusion of irrelevant variables. 47 To mitigate this, the range of variables included for analysis were refined based on existing UKB work 39 and previously published CRC risk assessment tools.18,20,48 Least absolute shrinkage and selection operator (Lasso) variable selection models 49 were performed to identify candidate LTC variables that may be potential predictors of the CRC outcomes of interest – incidence and mortality. These models also tested multimorbidity status for association with CRC outcomes.
Those LTCs identified as candidate predictor variables in the Lasso models were tested for significant association with CRC outcomes using fully-adjusted Cox regression models (Supplementary Material 2, Supplementary Tables S2 and S3). Models were adjusted for age, sex, Townsend quintile, smoking status, alcohol intake, physical activity and BMI. Separate models were used for CRC incidence and mortality. The Cox regression model used for CRC mortality incorporated the Fine and Gray subdistribution method to estimate true CRC mortality over time in the presence of competing risks of death due to other causes.50,51
Results
Characteristics of participants, with and without colorectal cancer.

CRC = colorectal cancer.
Lasso variable selection identified 24 LTCs (from 43) for possibility of having significant association with CRC incidence: dementia, chronic kidney disease (CKD), heart failure, chronic obstructive pulmonary disease (COPD), peripheral vascular disease, stroke or transient ischaemic attack (TIA), epilepsy, diabetes, rheumatoid arthritis (RA), depression, hypertension, multiple sclerosis, asthma, anxiety, thyroid conditions, painful conditions, diverticular disease, glaucoma, prostate disease, dyspepsia, female cancers (ovarian, endometrial), male cancers (testicular, prostate), ulcerative colitis and colonic polyps.
Long-term conditions associated with colorectal cancer incidence.
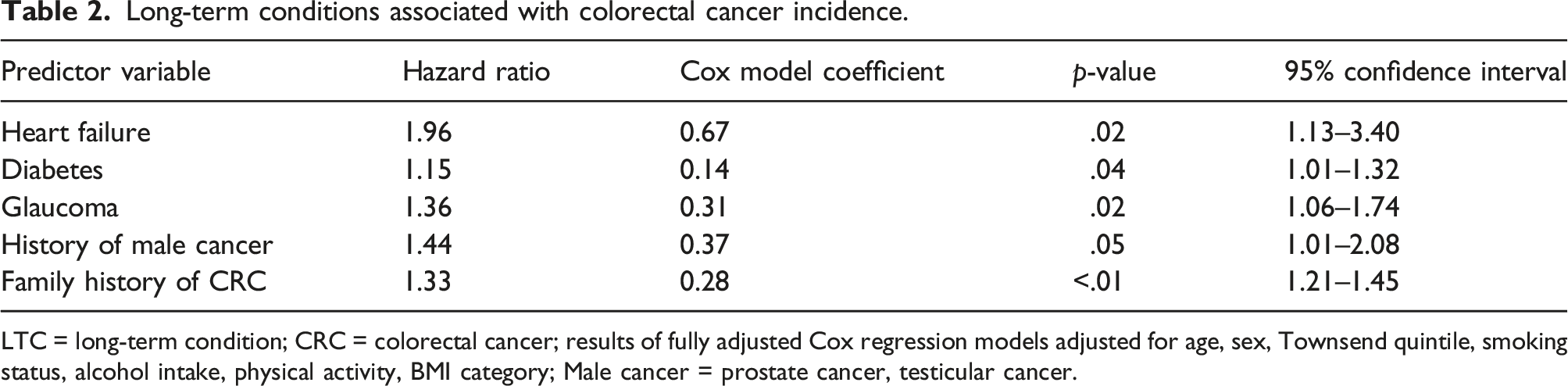
LTC = long-term condition; CRC = colorectal cancer; results of fully adjusted Cox regression models adjusted for age, sex, Townsend quintile, smoking status, alcohol intake, physical activity, BMI category; Male cancer = prostate cancer, testicular cancer.
Presence of multimorbidity did not have a statistically significant association with CRC incidence, regardless of multimorbidity count (that is, the number of co-existing LTCs; for four or more LTCs HR 1.04, CI 0.86–1.26; three LTCs HR 1.05, CI 0.90–1.23; two LTCs HR 1.07, CI 0.94–1.21; one LTC HR 1.03, CI 0.93–1.14; see Supplementary Material 2, Supplementary Table S2).
With regard to CRC mortality, Lasso models identified CKD, alcohol problems, heart failure, COPD, stroke or TIA, epilepsy, diabetes, RA, osteoporosis, constipation, polycystic ovarian syndrome (PCOS), male cancers and colonic polyps as potential predictors of CRC mortality.
Long-term condition associated with colorectal cancer mortality.

LTC = long-term condition; CRC = colorectal cancer; Results of fully adjusted Cox regression models adjusted for age, sex, Townsend quintile, smoking status, alcohol intake, physical activity, BMI category.
Supplementary Tables S4 and S5 (presented in Supplementary Material 3) show prevalence values for the indicator LTCs identified in this analysis for participants with and without CRC, and for those who died from CRC alongside those who did not.
Discussion
Our results showed a 0.73% incidence of CRC and 0.18% CRC mortality in the UKB population during the follow-up period. This reflects an annual incidence rate of 104.8 cases per 100,000 per year and mortality rate of 26.2 deaths per 100,000 per year in the study population. Cancer Research UK (CRUK) reports average CRC incidence rates of 74.3 cases per 100,000 population annually for the UK general population in the time period 2008–2014, 52 and 28.6 CRC deaths per 100,000 population annually over the same time period. 53 This suggests a higher rate of CRC incidence in the UKB study population as compared to the UK general population but a broadly similar rate of CRC mortality which may be due to demographic differences in our population compared to the whole UK population.
We report novel associations between CRC incidence and certain LTCs, namely, heart failure, glaucoma and male cancers, as well as between epilepsy and osteoporosis and CRC mortality, and confirm previously reported associations of diabetes with both CRC outcomes.30,31,54 These results highlight those patients who might be more at risk of developing and dying from CRC. It will be important to consider possible aetiological pathways that may underlie these associations.
In diabetic as opposed to non-diabetic participants in this study, HR for CRC incidence was 1.15, and HR 1.32 for CRC mortality. These results echo those found in a large international systematic review and meta-analysis, 30 adding weight to an existing international body of evidence, and confirming this association in a UK-specific population.
In contrast to other published work,23,26,27 this analysis did not demonstrate statistically significant associations between CRC outcomes and certain known risk factors, for example, IBD, colonic polyps, nor between multimorbidity and CRC outcomes. This may reflect chance occurrence, or systematic differences between the UKB population and those examined in other studies (e.g., older population aged ≥67 studied by Gross et al., 27 Danish and South Australian populations studied by Erichsen et al. 23 and Pule et al., 26 respectively) may have led to these findings.
Strengths and limitations
The UKB is a substantial dataset, both in participant numbers and breadth of data, and therefore represents a rich and powerful data resource with robust statistical power. This enables adjustment for multiple confounding factors in the analysis. A further advantage of the range of this dataset is its inclusion of health-related variables, including a wide range of LTCs, lifestyle factors and medical family history.
Potential limitations include the potential for selection bias, as UKB recruited volunteer participants who are not representative of the whole UK population. Notably, these participants tend to be healthier, older, more affluent, and with less diverse ethnic representation as compared to the general UK population. 55 As a result, association effect sizes found in this work may underestimate those true effect sizes existing in the UK population. As with any observational study, there is a risk of unmeasured confounding. The use of variable selection methods has potential to introduce selection bias in the results, 46 however this risk is likely to be lower in a dataset of this size. This study takes a descriptive, exploratory approach and therefore associations found cannot demonstrate causative relationships between factors
Potential applications
There are several interesting potential applications of these findings, if these associations are found to be consistent in other validation studies. The findings that heart failure, diabetes and glaucoma and male cancers predict CRC incidence, and that epilepsy, diabetes and osteoporosis predict CRC mortality may have potential impact in clinical practice. For example, if a patient who has these higher-risk predictor LTCs presents with symptoms suspicious for CRC, a clinician aware of these associations may more readily consider CRC as a potential differential diagnosis and this may trigger a lower threshold for referral and further investigation of CRC symptoms in high-risk patients. This could therefore could improve early diagnosis and intervention for CRC, a key objective of public health policy internationally.4,56
This impact on clinical decision making could be achieved by various routes: e.g. through clinician education and awareness-raising regarding associations between high-risk LTCs and CRC, or through incorporation of the identified predictor conditions found in this study (heart failure, glaucoma, male (testicular and prostate) cancers) into either existing CRC risk-stratification tools (e.g., CCRAT 18 , QCancer 48 ), or in novel tools, which could help to refine risk-stratification of patients in routine clinical practice, with potential benefits for earlier CRC investigation and diagnosis.
Furthermore, these findings could benefit population screening programmes, for example, targeting of efforts to maximise CRC screening uptake towards higher-risk patients, that is, those with predictor LTCs.
Further research
To investigate the degree of generalizability of this study’s findings to a UK or wider population there would be value in validating this analysis using other dataset(s), for example, routinely collected health data, where a more truly representative population sample would mitigate selection bias. Similar analyses in international datasets are also important for exploring and addressing the global health impact of CRC. Future analyses including genetics and/or causality data may also confirm and explain the findings from this work.
Exploring associations of LTCs and CRC outcomes with other factors, such as CRC screening participation, may prove a fruitful area for future research. CRC primary preventive efforts could be improved by explanatory work understanding the mechanisms underlying the LTC-CRC associations shown in this study.
Future qualitative work exploring human and individual factors, experiences, beliefs and behaviours that may influence these relationships would complement the findings in this paper and inform future interventions.
Conclusion
We have demonstrated significant associations between several common LTCs and CRC incidence and mortality, though not between multimorbidity and CRC outcomes – findings which merit further validation and exploration. Novel findings that presence of heart failure, glaucoma and male cancers were associated with CRC incidence and that presence of epilepsy and osteoporosis were associated with CRC mortality were demonstrated; and known associations between diabetes and both indicator CRC outcomes were again confirmed. These findings have potential implications for clinical practice, CRC risk-stratification, and targeting of CRC screening.
Supplemental Material
Supplemental Material - Long-term conditions, multimorbidity and colorectal cancer risk in the UK Biobank cohort
Supplementary Material for Long-term conditions, multimorbidity and colorectal cancer risk in the UK Biobank cohort by Neave ME Corcoran, Frances S Mair, Barbara Nicholl, Sara Macdonald, and Bhautesh Dinesh Jani in Journal of Multimorbidity and Comorbidity.
Footnotes
Acknowledgements
This work was completed using the UK Biobank Resource under project application number 14151. We would like to thank the participants in the UK Biobank study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: N.C. was funded by a Scottish School of Primary Care/NHS Education for Scotland clinical academic fellowship. B.D.J.’s time was partly funded by Dawkins and Strutt research grant from the British Medical Association
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.