
Abstract
Background:
Pregnancy is a natural physiological process. However, it significantly affects mothers’ health-related quality of life through various physical, psychological, social, and environmental changes. Understanding the determinants of health-related quality of life during antenatal care can guide maternal health interventions.
Objectives:
To assess health-related quality of life and associated factors among mothers attending antenatal care in South Wollo Zone public hospitals, Northeast Ethiopia.
Design:
An institution-based cross-sectional study.
Methods:
Systematic random sampling method was used in five randomly selected hospitals among mothers attending antenatal care from March 1 to 30, 2024. Health-related quality of life was measured using World Health Organization Quality of Life – BREF (WHOQOL-BREF) questionnaire. Data were entered into EpiData 3.1 and exported to SPSS 25 for analysis. Multivariable linear regression analysis was performed by selecting variables with a p-value of <0.25 in simple linear regression. Then, variables having p-value <0.05 at 95% confidence interval with an unstandardized B-coefficient were considered significant predictors.
Results:
The mean scores for physical, psychological, social relationship, and environmental health-related quality of life domains were 71.0, 72.1, 66.1, and 65.7, respectively. Among the participants, 76.1% rated their health-related quality of life as neither poor nor good, and 42.3% reported being neither dissatisfied nor satisfied in terms of their health satisfaction. Physical health was negatively affected by pregnancy-related illness, older age, and depression. Psychological domain declined with depression, rural residence, and perceived social stigma. Depression and perceived social stigma impaired social relationships. Environmental quality of life was lower among depressed participants, rural residents, and those reporting current alcohol use.
Conclusion:
Overall, participants demonstrated moderate health-related quality of life across all domains, with most perceiving their health status as neutral. Health professionals should follow holistic care, including physical, psychological, social, and environmental interventions. Targeted interventions are needed to address negatively associated predictor variables for all domains of health-related quality of life.
Plain language summary
Pregnancy is a process that can affect mothers’ health-related quality of life. It causes changes in women’s physical, emotional, social and environmental aspects of health. Although Ethiopia has implemented antenatal care programs, the quality-of-life aspects of pregnant mothers remain neglected. This motivated us to investigate health-related quality of life and associated factors among mothers attending antenatal care in Northeast Ethiopia. Understanding these factors can help health workers provide better counseling and support during pregnancy.
The researchers looked at what affects the quality of life of pregnant women attending antenatal care in Northeast Ethiopia. By identifying these factors, they aimed to help improve counseling services and develop better care and support programs for pregnant women during their antenatal visits.
The physical, psychological, social relationship and environmental domains of health-related quality of life average scores were 71.0, 72.1, 66.1, and 65.7, respectively. Depression was negatively associated with all four domains of health-related quality of life.
Attentions should be needed for all domains of health-related quality of life among pregnant mothers to ensure positive maternal-child health outcomes. This study identified important target variables that could be a focus of future efforts to ensure positive health related quality of life. Health professionals should provide holistic care, including physical, psychological, social and environmental interventions, with particular attention to address negatively associated predictor variables.
Introduction
Quality of life (QOL) is an individual’s perception of his or her position in life in the context of culture and value systems in which he or she lives and in relation to his or her goals, expectations, standards, and concerns.1,2 Health-related quality of life (HRQOL) refers to the aspects of QOL affected by health states. 3
Pregnancy is not necessarily a joyful period, during which physical, psychological, and social changes may negatively affect women’s HRQOL. Several studies have indicated a decrease in HRQOL, especially in physical function and mental domains, resulting from sleep deprivation, fatigue, anxiety, and mood changes during pregnancy.4–6
Women usually have little information about the long-lasting physical and mental health problems that may result as a consequence of pregnancy, childbirth, and puerperium; therefore, they are unprepared when they face such problems. As a result, their QOL will be compromised for a prolonged period.7–9
Due to compromised HRQOL during pregnancy, maternal mortality remains unacceptably high. Ninety-five percent of all maternal deaths occur in low- and lower-middle-income countries, and most of these deaths could be prevented. 10 The African continent contributed approximately two-thirds (65%) of maternal deaths worldwide. In sub-Saharan Africa, a woman’s lifetime risk of dying during pregnancy or childbirth is 1 in 36 compared with 1 in 4900 in developed countries. 11 One in 41 women in sub-Saharan African countries died from maternal causes. 12
In 2023, an estimated 260,000 women died from pregnancy-related causes, with over 90 % of these deaths occurring in low and low-middle-income countries. Approximately, the global maternal mortality ratio was 197 deaths per 100,000 live births. Sub-Saharan Africa continues to be the highest burden, accounting for around 70% of maternal deaths in 2023. 13
Antenatal care (ANC) is the care provided by skilled health professionals to pregnant women to ensure the best health conditions for both mothers and babies during pregnancy. It promotes health, supports risk identification, and enables the prevention and management of pregnancy-related conditions affecting both the mother and the fetus, while also encouraging healthy behaviors and parenting skills. 14 According to various observational studies, ANC has positive effects, such as decreasing maternal and perinatal mortality and improving pregnancy outcomes. 15 Evidence of the effectiveness of ANC is necessary for decision-makers to establish adequate policies and strategies and allocate proper resources for implementation. Self-reported HRQOL is an appropriate outcome measure in evaluations of maternal health interventions. 16
Although ANC programs have been introduced in Ethiopia, HRQOL is a neglected aspect of maternity care. There is limited evidence on how pregnancy and ANC utilization influence HRQOL among Ethiopian women. Thus, this study aimed to assess the levels and determinants of HRQOL among pregnant women attending ANC in public hospitals of South Wollo Zone, Northeast Ethiopia. It adopts the WHOQOL conceptual model, which posits that individual health perceptions are shaped by physical, psychological, social, and environmental determinants. Furthermore, this study provides valuable information to the South Wollo Zone Health Office, health professionals, and policy makers to plan resources and to implement targeted interventions.
Methods
Study settings, design, and period
The study was conducted in public hospitals of the South Wollo Zone, Northeast Ethiopia. An institution-based cross-sectional study with quantitative approaches was conducted from March 1 to 30, 2024.
Populations
The source populations were all pregnant mothers attending ANC in public hospitals in the South Wollo Zone, and the study populations were all pregnant mothers attending ANC in selected public hospitals in the South Wollo Zone during the study period. The inclusion criteria were pregnant mothers who attended ANC and whose age was equal to or greater than 18 years, and the exclusion criteria were pregnant mothers who were critically ill during follow-up and who had hearing impairments.
Sample size determination
The single population proportion formula [n = (Za/2)2P(1 − P)/d2] was used. The assumptions were a 95% confidence level, which yielded a Z α/2 = 1.96 for the standard normal distribution curve, a 5% margin of error (d), and a 50% estimated prevalence of HRQOL. A prevalence of 50% was used because, to the authors’ knowledge, there was no similar study using the same tool among mothers attending ANC in Ethiopia. After accounting for a 10% nonresponse rate, the final sample included 423 mothers who attended ANC.
Sampling technique and procedure
The South Wollo Zone has 14 public hospitals, of which one-third of the hospitals, which are five hospitals, were selected by simple random sampling. Based on the number of mothers with ANC from each selected hospital in 1 month, the total sample size was allocated proportionally (Boru Meda Hospital = 65, Akesta Hospital = 117, Queen Zewditu Hospital = 56, Haik Hospital = 101, Tenta Hospital = 84). Then, from each selected hospital, by using a list of registration numbers as a sampling frame, mothers were selected using a systematic random sampling technique every two intervals (K = 867/423 = 2.04 ≈ 2), where K was calculated from the total number of mothers who attended ANC (867) divided by the sample size (423) of the study. The first study subject was selected by the lottery method.
Data collection tools and study variables
The data were collected using an interviewer-administered questionnaire with five parts (Supplementary file 1).
Sociodemographic characteristics: Including residency, age, educational level, marital status, occupation, community health insurance status, and number of children.
HRQOL questionnaire: The dependent variable of this study was HRQOL, and the tool was adopted from the World Health Organization Quality of Life Instruments (WHOQOL-BREF-26) validated tool.17–19
Clinical profiles: Current treatment, pregnancy-related illness or complication, type of pregnancy-related illness or complication, duration of pregnancy in months, disease before pregnancy, type of disease before pregnancy, and ANC health education.
Psychosocial factors: The Depression and Perceived Social Stigma Assessment Checklists were used to assess depression and perceived social stigma, respectively.19–21
Behavioral factors: Current cigarette smoking and alcohol consumption were assessed by preparing substance abuse tools from the literature.22–24
Data collection procedures and quality control
To ensure the quality of the data, properly designed data collection instruments were used. For the purpose of data collection, the English versions of the instruments were translated into the Amharic language. Five midwives serving as data collectors (one for each hospital) and one midwife serving as supervisor were selected for data collection, and 1 day of training was given to them. Pretests were performed on 5% of the total sample at Dessie Comprehensive Specialized Referral Hospital. During the pretest, the reliability of the Amharic version tool was assessed by computing the Cronbach’s alpha for dependent variables (physical = 0.81, psychological = 0.84, environmental = 0.79, and social = 0.76) and for independent variables (depression = 0.86, perceived social stigma = 0.88). The respondents were encouraged by data collectors to respond to all items to minimize the large nonresponse rate.
Operational definitions
HRQOL was measured using the WHOQOL-BREF, a validated instrument consisting of 26 items grouped into four domains: physical health (seven items), psychological health (six items), social relationships (three items), and environmental health (eight items). The remaining two items, overall perception of self-rated HRQOL and self-reported health satisfaction, were not included in any domain. Each item was scored on a 5-point Likert scale ranging from 1 to 5. Negatively phrased items were reverse-coded prior to analysis. Domain scores were calculated by computing the mean score of items within each domain, and these mean scores were then multiplied by four to make them comparable with scores from other WHOQOL instruments. Finally, the scores were transformed to WHOQOL-100 scale scores.17–19 Participants were classified as depressed if they had a mean score of 10 or higher, and not depressed if their mean score was below 10, based on the depression assessment checklist.19,20,25 Perceived social stigma was defined as a score above the 66th percentile, whereas no perceived social stigma was defined as a score at or below the 66th percentile on the perceived social stigma assessment checklist. 21 Current cigarette use was defined as pregnant mothers who consumed cigarettes at least once in the past 30 days.22,24 Current alcohol use was defined as pregnant mothers who consumed any alcohol at least once in the past 30 days.22–24
Statistical analysis
The collected data were entered into EpiData version 3.1 and exported to SPSS version 25 for analysis. The extent and pattern of missing data were assessed using frequency tables. As the proportion of missing values was minimal and appeared to be random, complete-case analysis was used, whereby observations with missing values were excluded from analyses. Reverse coding was performed on three negative items in the physical and psychological health domains, and the score of each domain was obtained by computing the mean score of the items. For the descriptive analysis, the means, standard deviations, frequencies, and percentages were calculated and are presented in tables and text. For the purpose of analysis, dummy variables (for k categories, k − 1 dummy variables) were created for categorical variables such as educational status, marital status, and occupational status.
Linear assumptions, including normality, homogeneity of variances, multicollinearity, and linearity, were checked in all domains, and the assumptions were met. Multicollinearity was tested using the variance inflation factor (VIF), and no multicollinearity was detected, because all VIF values were below 4.58 for all predictors
According to the WHO HRQOL guidelines, a linear regression analysis model was used to identify factors associated with HRQOL with respect to the physical, psychological, social relationship, and environmental health domains. Simple linear regression analysis was performed between the dependent variable and each independent variable. Then, the data were subjected to multivariable linear regression analysis at a p-value <0.25 with a 95% CI. Multivariable linear regression analysis was performed by using the forward selection method, and variables with a p-value <0.05 at the 95% CI with an unstandardized B-coefficient were considered to be significant predictor variables. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cross-sectional studies was used to guide the reporting of this study (Supplementary file 2). 26
Ethics approval
Ethical approval was obtained from Wollo University College of Medicine and Health Sciences Research Ethical Review Committee (ethical approval reference number: CMHS 2369/20/15). Subsequently, copies of the ethical approval letters and an official letter of cooperation were sent to the selected public hospitals in South Wollo Zone. Permission to conduct the study was then obtained from the selected hospitals.
Results
Sociodemographic characteristics
From the total sample size (n = 423), 414 mothers participated in the interviews, which was a 97.9% response rate. Among the participants, 63.0% lived in urban areas. The mean age of the respondents was 29.6 years ±5.0 SD with minimum and maximum ages of 19 and 44 years, respectively. Overall, 91.1% were married, and 61.4% were enrolled in membership in community health insurance (Table 1).
Sociodemographic characteristics of mothers attending ANC.

Unemployed = wants a job but doesn’t have one; it can be for both genders. Housewife = working at home and not seeking outside employment, in our context, women.
ANC, antenatal care.
Clinical profile of the respondents
Of all mothers who attended ANC, 51.9% received both oral medication, such as iron supplementation, and professional counseling services. Among the participants, 8.7% had pregnancy-related illnesses or complications. Of the participants who had pregnancy-related illnesses or complications (n = 36), 69.4% had hypertension in pregnancy. Of the 414 respondents, 15.2% had never attended ANC health education (Table 2).
Clinical characteristics of mothers attending ANC.

ANC, antenatal care.
Psychosocial and behavioral characteristics of respondents
With regard to the psychosocial characteristics of the participants, 11.4% and 33.6% of the mothers had depression and perceived social stigma, respectively. Regarding behavioral characteristics, 2.4% and 9.4% of them were current cigarette and alcohol users, respectively (Table 3).
Psychosocial and behavioral characteristics of mothers attending ANC.

ANC, antenatal care.
HRQOL of respondents
The mean physical, psychological, social relationship, and environmental HRQOL scores were 71.0 ± 9.3, 72.1 ± 8.1, 66.1 ± 9.9, and 65.7 ± 8.5, respectively (Table 4). During multivariable linear regression, the total variation explained by the model (R²) was 46% for the physical health domain, 43% for the psychological domain, 38% for the social domain, and 34% for the environmental domain.
The four domains of HRQOL with the mean scores of mothers attending ANC (n = 414).
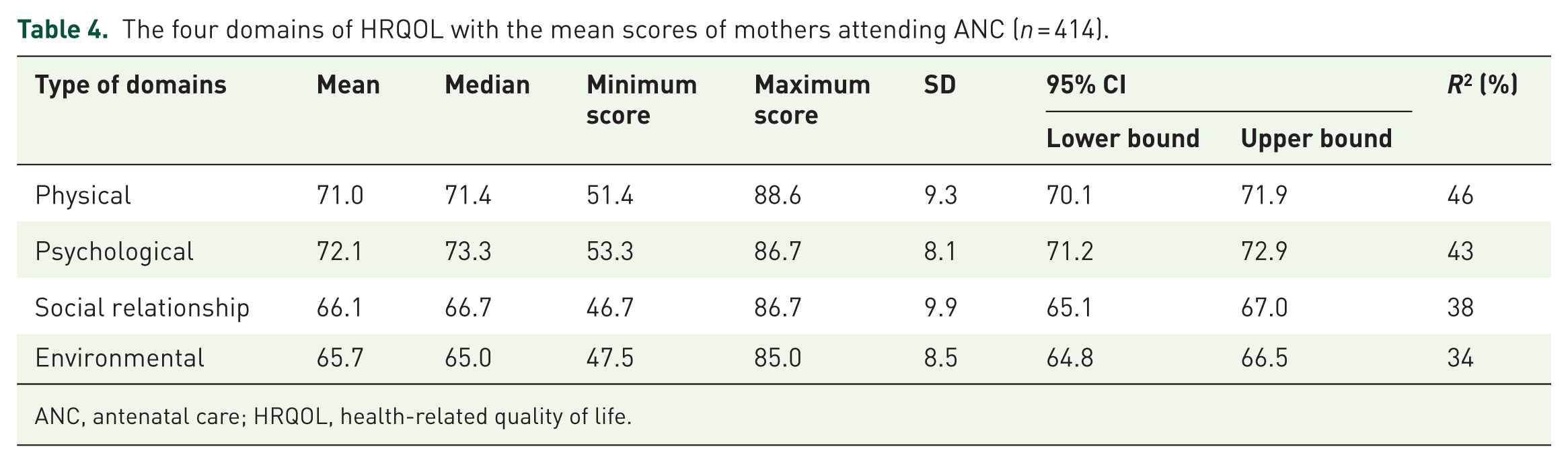
ANC, antenatal care; HRQOL, health-related quality of life.
Self-rated HRQOL and self-reported health satisfaction of respondents
Among the total participants, 76.1% had neither poor nor good self-rated HRQOL, and 42.3% were neither dissatisfied nor satisfied with their self-reported health satisfaction (Table 5).
Self-rated HRQOL and self-reported health satisfaction of mothers attending ANC.
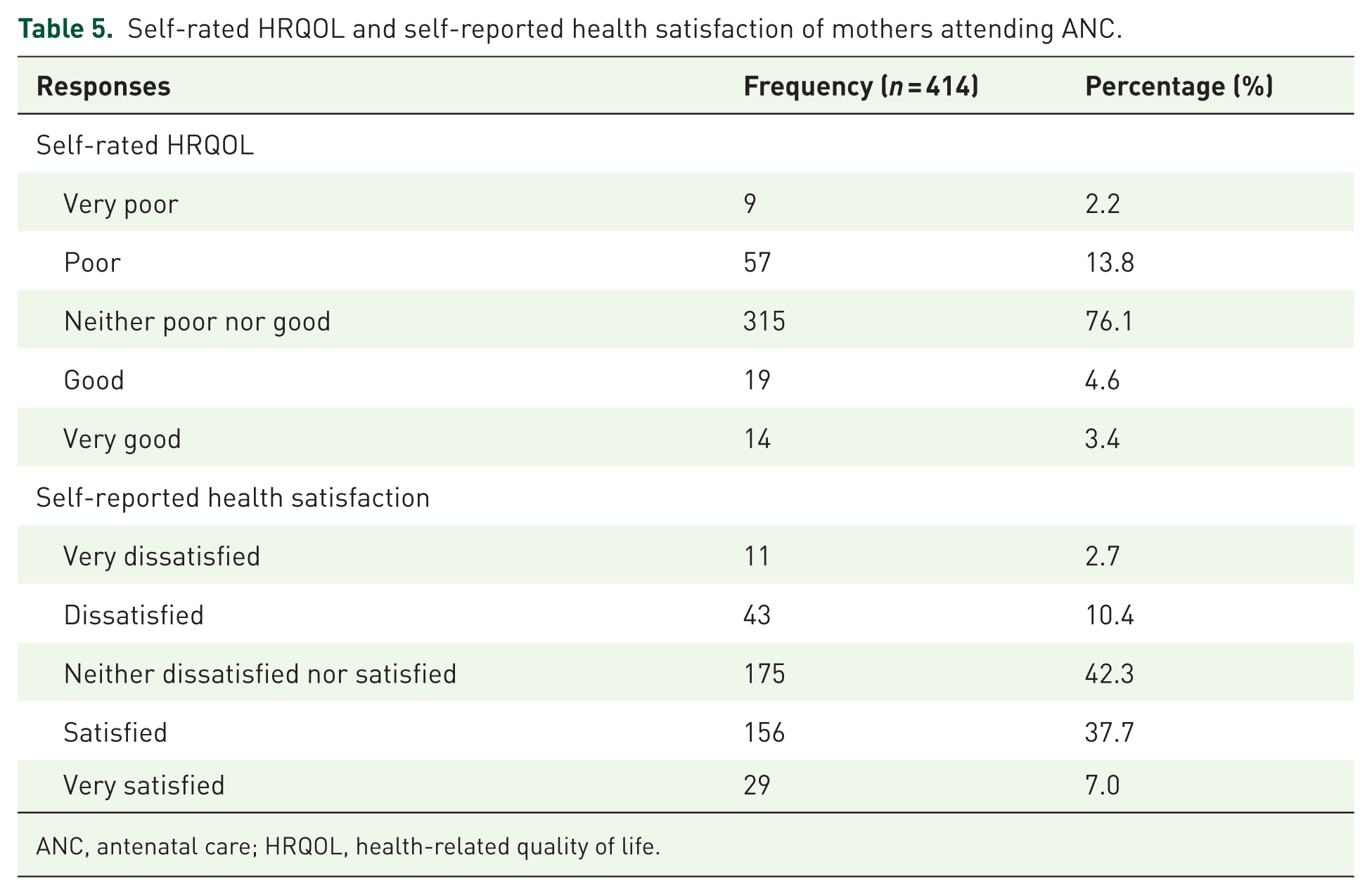
ANC, antenatal care; HRQOL, health-related quality of life.
Factors associated with physical HRQOL
Variables that were entered into simple linear regression analysis and passed to multivariable linear regression analysis with a p-value <0.25 were residency, age, educational level, marital status, occupation, current treatment, pregnancy-related illness or complication, duration of pregnancy in months, disease before pregnancy, attended ANC health education, depression, perceived social stigma, and current alcohol use. In multivariable linear regression analysis, the duration of pregnancy in months was directly related to physical HRQOL, whereas the presence of pregnancy-related illness, age, and depression were inversely related to physical HRQOL.
As the duration of pregnancy increased by 1 month, mothers’ physical HRQOL increased by 1.3, keeping the effect of other variables constant. Mothers who had pregnancy-related illness were on average 5.4 points lower in physical HRQOL as compared with those mothers who did not have pregnancy-related illness, keeping the effect of other variables constant (Table 6).
Multivariable linear regression analysis of factors associated with physical HRQOL in mothers attending ANC (n = 414).

ANC, antenatal care; HRQOL, health-related quality of life.
Factors associated with psychological HRQOL
Variables that were entered into simple linear regression analysis and passed to multivariable linear regression analysis with a p-value <0.25 were residency, age, educational level, marital status, occupation, membership in community health insurance, number of children other than current pregnancy, current treatment, pregnancy-related illness or complication, duration of pregnancy in months, Attended ANC health education, depression, and perceived social stigma. In multivariable linear regression analysis, college/university level of education and duration of pregnancy in months were directly related to psychological HRQOL, whereas depression, rural residency, and perceived social stigma were inversely related to psychological HRQOL.
Mothers who had university level of education were on average 0.7 higher in psychological HRQOL as compared with those mothers who were illiterate, keeping the effect of other variables constant. Mothers who experienced depression were on average 4.5 points lower in psychological HRQOL as compared with those mothers who did not experience depression, keeping the effect of other variables constant (Table 7).
Multivariable linear regression analysis of factors associated with psychological HRQOL in mothers attending ANC (n = 414).

ANC, antenatal care; HRQOL, health-related quality of life.
Factors associated with social relationship HRQOL
Variables that were entered into simple linear regression analysis and passed to multivariable linear regression analysis with a p-value <0.25 were residency, educational level, marital status, occupation, membership in community health insurance, current treatment, duration of pregnancy in months, attended ANC health education, depression, perceived social stigma, and current alcohol use. In multivariable linear regression analysis, depression and perceived social stigma were inversely related to social relationship HRQOL, whereas college/university education level, self-employment status, regularly attended ANC health education, and sometimes attended ANC health education were directly related to social relationship HRQOL.
Mothers who experienced depression were on average 4.3 points lower in social relationship HRQOL as compared with those mothers who did not experience depression, keeping the effect of other variables constant. Mothers who had a college/university level of education were on average 1.2 higher social relationship HRQOL as compared with those mothers who were illiterate, keeping the effect of other variables constant (Table 8).
Multivariable linear regression analysis of factors associated with social relationship HRQOL in mothers attending ANC (n = 414).
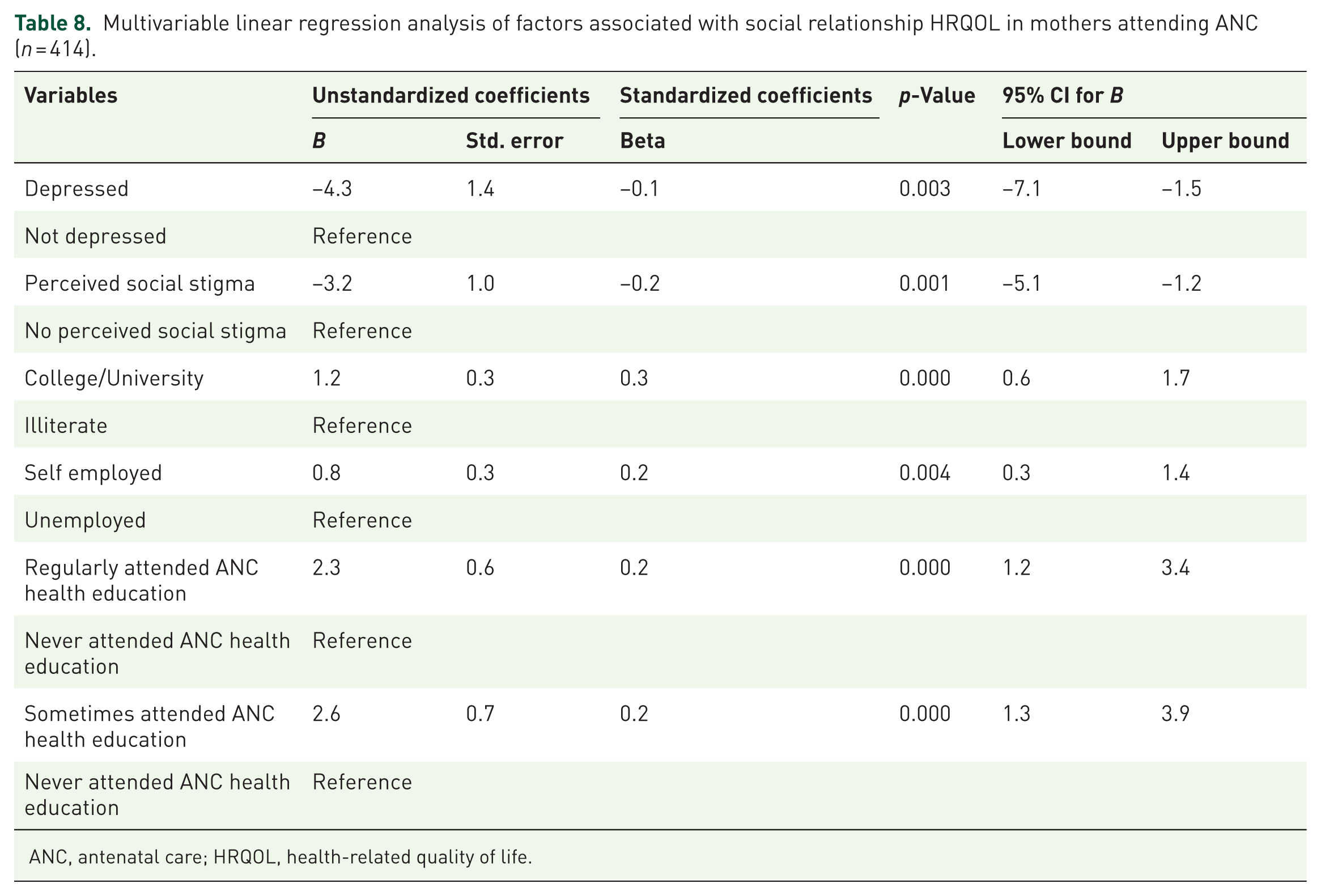
ANC, antenatal care; HRQOL, health-related quality of life.
Factors associated with environmental HRQOL
Variables that were entered into simple linear regression analysis and passed to multivariable linear regression analysis with a p-value <0.25 were residency, educational level, occupation, membership in community health insurance, current treatment, pregnancy-related illness or complication, duration of pregnancy in months, attended ANC health education, depression, current cigarette use, and current alcohol use. In multivariable linear regression analysis, college/university level of education, secondary school level of education and duration of pregnancy in months were directly related to environmental HRQOL, whereas depression, rural residency, and current alcohol use were inversely related to environmental HRQOL.
Mothers who had a college/university level of education were on average 1.3 higher in environmental HRQOL as compared with those mothers who were illiterate, keeping the effect of other variables constant. Mothers who experienced depression were on average 3.4 points lower in environmental HRQOL as compared with those mothers who did not experience depression, keeping the effect of other variables constant (Table 9).
Multivariable linear regression analysis of factors associated with environmental HRQOL in mothers attending ANC (n = 414).

Discussion
Pregnancy is not always a joyful period and can negatively affect women’s well-being and HRQOL.4–6 Investigating the HRQOL of pregnant mothers and associated factors is needed to design appropriate interventions. In this study, 76.1% of participants reported a moderate level of HRQOL, rating it as neither poor nor good. The findings indicate that the majority of participants perceived their HRQOL as moderate, falling between poor and good. This suggests that most respondents viewed their overall QOL as average. This percentage was greater than studies conducted in the cities of the Colombian Caribbean (44.6%) and Kathmandu (8.5%).27,28 Similarly, in this study, 42.3% of participants reported a neutral level of health satisfaction, indicating that they were neither satisfied nor dissatisfied. This suggests a moderate perception of health status, with many individuals not expressing positive or negative feelings about their health. This percentage was also higher than a study conducted in the cities of the Colombian Caribbean (31.8%). 27 The difference may be explained by the fact that only 4.6% of the study participants in this study reported good self-rated HRQOL, whereas 35.0% and 91.5% of participants in the Colombian Caribbean and Kathmandu, respectively, reported good self-rated HRQOL.27,28 Regarding satisfaction, only 7.0% of participants in the current study were very satisfied, whereas 26.8% of participants in the Colombian Caribbean reported being very satisfied with their self-reported health. 27
Regarding the HRQOL domains, the physical, psychological, social and environmental mean scores were 71.0 ± 9.3 (95% CI: 70.1–71.9), 72.1 ± 8.1 (95% CI: 71.2–72.9), 66.1 ± 9.9 (95% CI: 65.1–67.0), and 65.7 ± 8.5 (95% CI: 64.8–66.5), respectively. This can be interpreted as, participants reported relatively higher mean scores in the physical and psychological domains, indicating better perceived functioning and well-being in these areas. In contrast, relatively lower mean scores were observed in the social and environmental domains, suggesting comparatively poorer perceptions of social relationships and environmental conditions. These findings imply that interventions aimed at improving HRQOL should not only maintain physical and psychological health but also prioritize strengthening social networks and enhancing environmental conditions, as these domains appear to be key areas of unmet need. In this study, the physical and psychological domains of HRQOL were comparable to those reported in a study conducted among Iranian pregnant women, where the mean scores for the physical and mental dimensions were 70.2 and 71.88, respectively. However, the social domain score in the present study was slightly lower than that reported in the Iranian study (67.43). 29 The similarity between the findings of this study and those of the Iranian study may be attributed to similarities in the study designs.
The current study showed that HRQOL was highest in the psychological domain. This was in line with a study performed in Kathmandu. In this study, the lowest value was found in the environmental domain. This finding was inconsistent with a study performed in Kathmandu, where the lowest was found in the physical domain. 28
The duration of pregnancy in months was directly related to the physical, psychological, and environmental domains of the HRQOL. However, another finding was inconsistent with the present study, which reported that the physical domain of HRQOL decreased and the mental domain was constant during pregnancy. 30 Cultural reasons, social explanations, economic, family, environmental, and educational effects, opinions about the female and motherhood role, life understandings, and others can explain these differences. 31 Furthermore, this finding contradicts the findings of a study performed in Kathmandu, where the duration of pregnancy was not associated with the physical or psychological domains. 28 A possible explanation is that, in this study, mothers who were pregnant, particularly during the first trimester, reported high levels of nausea, vomiting, and loss of appetite. These symptoms predisposed them to insufficient energy for daily activities, resulting in physical weakness, fatigue, and dissatisfaction with their capacity for work. In addition, the severity of nausea, vomiting, and loss of appetite interfered with their enjoyment of life and was associated with negative emotional states, including low mood, despair, anxiety, and depression.32,33 However, as pregnancy progresses, nausea typically decreases for many women, which may lead to improvements in nausea-related aspects of HRQOL; however, overall HRQOL may be influenced by the emergence of other physical and psychological symptoms later in pregnancy. 33
The presence of pregnancy-related illness and increased age were inversely related to physical HRQOL. This finding was in line with a study conducted in pregnant women in which pregnancy-related illnesses such as nausea, vomiting, obesity, complications during pregnancy, epigastralgia, and back pains, as well as medical conditions such as hypertension and diabetes, were inversely related to QOL.34–36 Similarly, the relationship between age and physical HRQOL was in line with a study conducted in Kathmandu, where younger pregnant women were significantly more likely to have good physical HRQOL. 28 However, another study contradicted the findings of the current study, which reported no significant differences in HRQOL in relation to age. 37 This variation may be due to lifestyle differences in terms of age across the different studies.
Depression had an inverse relationship with all domains of HRQOL. This indicates that depression should be interpreted within the broader context of perinatal mental health, where psychological well-being is shaped not only by biological and hormonal changes but also by social and environmental factors. Depressive symptoms during pregnancy are often exacerbated by limited social support, heightened caregiving expectations, and cultural norms that contribute to emotional distress in motherhood.38,39 This finding was in line with a study performed using the WHOQOL-BREF, which revealed that depression during pregnancy was associated with impairment in all four domains. 40 This finding was also consistent with a study in which women with depressive symptoms had significantly lower HRQOL scores in all domains except physical functioning.41,42 However, in another study, pregnant women with depression had a significantly worse HRQOL for physical pain. 43 Furthermore, studies revealed that a history of depression was associated with physical health impairment or low scores on the physical health domain.27,30 A possible explanation might be that depression during pregnancy and HRQOL have an inverse relationship; the worsening of depression symptoms contributes to the loss of physical, psychological, and general health by affecting the pathways of the neuroendocrine and immune systems.44,45
A college or university level of education was positively associated with the psychological, social, and environmental domains of HRQOL. This finding is consistent with a study conducted in public health facilities, which reported that being educated was associated with a higher quality of social relationships compared with being uneducated. 46 This may be because higher levels of education increase overall awareness of health and enhance social interaction through prolonged learning processes.
Rural residency had an inverse relationship with psychological and environmental HRQOL. This finding was compatible with other studies in which rural residence was inversely associated with HRQOL. 47 Surprisingly, other studies also reported that pregnant women in rural areas had worse HRQOL than did their urban peers.27,48 A possible reason might be that pregnant women in urban areas have more access to health services, education, and transportation, all of which are associated with improved HRQOL.49,50
Perceived social stigma had an inverse relationship with the psychological and social aspects of HRQOL. This indicates that individuals who experience higher levels of stigma tend to report poorer psychological well-being and weaker social relationships. This finding suggests that stigma operates as a psychosocial stressor that undermines both emotional functioning and social connectedness. These findings highlight the importance of addressing social stigma as a key component of interventions aimed at improving psychological health and social well-being.51,52 This was consistent with other studies in which QOL was impacted by perceived or enacted social stigma through social interactions. 53 Another study also showed a significant negative correlation between social stigma and the life satisfaction of women. 54
Self-employed status and ANC health education attendance were directly related to social relationship HRQOL. This finding was comparable to that of other studies in which low education negatively affected the QOL of pregnant women. 55 The secondary school education level had a direct effect, whereas current alcohol use had an inverse relationship with environmental HRQOL. This finding was similar to that of another study in which a history of alcohol dependence was associated with poor QOL. 34
Strengths and limitations of the study
This study had notable strengths. HRQOL was assessed using a linear regression analysis model based on the WHO guidelines with respect to the physical, psychological, social relationship, and environmental health domains. The study used standardized questionnaires, and the response rate was high. However, this study also had limitations. The methodology of face-to-face interviews may lead to social desirability bias by overestimating or underestimating the results. Since the study design was a cross-sectional method, the direction of relationships between variables cannot always be determined.
Conclusion
The mean HRQOL scores in the physical, psychological, social relationship, and environmental health domains ranged from 65 to 72 points out of 100. The duration of pregnancy in months was positively associated with physical HRQOL, whereas pregnancy-related illness, increased age, and depression were negatively associated with physical HRQOL. College/university level of education and duration of pregnancy in months were positively associated, whereas depression, rural residency, and perceived social stigma were negatively associated with psychological HRQOL. Depression and perceived social stigma were negatively associated, whereas college/university education level, self-employment status, and attended ANC health education regularly or sometimes were positively associated with social relationship HRQOL. College/university level of education, secondary school level of education, and duration of pregnancy in months were positively associated, whereas depression, rural residency, and current alcohol use were negatively associated with environmental HRQOL. Therefore, health policy makers, hospitals, and health professionals, particularly midwives, should contribute to a holistic approach to care, including physical, psychological, social, and environmental interventions, and to address negatively associated predictor variables for pregnant mothers attending ANC. ANC programs should provide health education sessions focusing on pregnancy-related health, mental well-being, and alcohol use, by giving special attention to women with lower educational levels and rural residency. Furthermore, integrating mental health screening and stigma reduction interventions into routine ANC could improve HRQOL outcomes. Future researchers should employ qualitative study approaches to explore the lived experiences that influence HRQOL among pregnant women. Longitudinal studies would also help to establish causal relationships between identified predictors and HRQOL outcomes.
Supplemental Material
sj-docx-1-reh-10.1177_26334941261441728 – Supplemental material for Health-related quality of life and associated factors among mothers attending antenatal care in South Wollo Zone Public Hospitals, Northeast Ethiopia: multicentered study
Supplemental material, sj-docx-1-reh-10.1177_26334941261441728 for Health-related quality of life and associated factors among mothers attending antenatal care in South Wollo Zone Public Hospitals, Northeast Ethiopia: multicentered study by Hawa Wolie, Ehtenesh Berihun, Missale Kassahun, Sisay Gedamu Addis, Debrnesh Goshiye, Mitaw Girma, Dessalegn Haile and Adane Birhanu Nigat in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941261441728 – Supplemental material for Health-related quality of life and associated factors among mothers attending antenatal care in South Wollo Zone Public Hospitals, Northeast Ethiopia: multicentered study
Supplemental material, sj-docx-2-reh-10.1177_26334941261441728 for Health-related quality of life and associated factors among mothers attending antenatal care in South Wollo Zone Public Hospitals, Northeast Ethiopia: multicentered study by Hawa Wolie, Ehtenesh Berihun, Missale Kassahun, Sisay Gedamu Addis, Debrnesh Goshiye, Mitaw Girma, Dessalegn Haile and Adane Birhanu Nigat in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
Authors would like to acknowledge Wollo University for financial support of this research. We would also acknowledge hospital administrators, data collectors, supervisors and the study participants for their valuable contribution in the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.