
Abstract
Background:
Pelvic organ prolapse (POP) is a major contributor to gynecological morbidity worldwide, including Ghana, with an estimated global prevalence of 30.9%. Surgery remains the definitive treatment for anatomical correction, but evidence on its functional outcomes in sub-Saharan Africa is limited.
Objectives:
This study evaluated the impact of surgical repair on pelvic floor symptoms and sexual function among Ghanaian women.
Design:
A prospective, hospital-based before-and-after study was conducted in Ghana between July 2018 and December 2019.
Methods:
Women with stage II or higher POP (n = 96) were assessed preoperatively and 3 months postoperatively via the validated Pelvic Floor Distress Inventory-20 (PFDI-20) and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (IUGA-Revised (PISQ-IR)) tools. Pre- and postoperative mean scores for the urinary, anorectal, mechanical, and sexual function domains were compared via paired t tests. Statistical significance was defined as p < 0.05.
Results:
Surgical repair appeared to be linked to improvements across all PFDI-20 subscales: POPDI-6 (28.47–1.91, p < 0.001), UDI-6 (17.14–3.26, p < 0.001), and CRADI-8 (5.01–2.15, p < 0.001). Nearly 87% of the participants were sexually inactive, and among these, the PISQ-IR demonstrated marked gains in condition-specific and condition-impact domains (p < 0.001), although no significant changes were observed in partner-related or global quality domains. The incidence of perioperative complications was minimal and was limited to urinary retention in 4.2% of the patients.
Conclusion:
Surgical management of POP among Ghanaian women was associated with substantial improvements in bulge, urinary, and bowel symptoms, with additional benefits in selected aspects of sexual health. These findings reflect initial symptom relief and quality of life improvements and should not be interpreted as long-term efficacy. These findings provide essential local data to fill knowledge gaps and inform preoperative counseling, guide decision-making, and shape postoperative expectations in similar resource-limited contexts.
Plain language summary
Pelvic organ prolapse (POP) is a condition in which the pelvic organs descend because the muscles forming the pelvic floor weaken and can no longer support the organs within the pelvis. This condition affects approximately 31% of women worldwide, including those in Ghana. While surgery can correct the anatomical issues, there is limited knowledge about its impact on the daily symptoms and sexual life of women in sub-Saharan Africa. A study was conducted on Ghanaian women with moderate-to-severe POP. These women were assessed before and three months after surgery, to evaluate the surgery's effect on the burden of POP symptoms, including sexual function. The study took place from July 2018 to December 2019. Improvements were observed in symptoms associated with POP, such as urinary and bowel issues. Nearly all the women (87%) were not sexually active before surgery and remained so three months after surgery. Among these women, improvements were noted in their sexual well-being related to their condition. However, there was no change in partner-related and overall quality aspects of their sexual well-being. In summary, POP surgery appeared to provide rapid relief from bulge, urinary, and bowel symptoms, along with some sexual health benefits for these Ghanaian women. This local data aids in counseling patients in resource-limited settings, though it represents early findings rather than long-term evidence.
Keywords
Introduction
Pelvic organ prolapse (POP) is characterized by the descent of one or more of the pelvic organs, including the anterior vaginal wall, posterior vaginal wall, uterus (cervix), or vaginal apex (vault or cuff scar following hysterectomy), beyond their normal anatomic confines. 1 It is a prevalent condition that imposes a significant burden on women’s health. This condition is associated with a wide spectrum of distressing symptoms affecting urinary, anorectal, and sexual functions.2 –7 These symptoms underline impaired hygiene and physical discomfort, resulting in psychosocial distress and reduced quality of life.8,9 In 2021, an estimated 13.9 million new cases of POP were reported globally, representing an increase from 8.4 million cases in 1990. 10 Despite this increase in absolute case numbers, the age-standardized incidence rate declined from 374.84 per 100,000 women in 1990 to 317.51 per 100,000 in 2021, reflecting demographic transitions and improvements in health care access in some regions. 10 Notably, the burden remains disproportionately high in low sociodemographic index settings, where the age-standardized incidence, mortality, and disability-adjusted life years attributable to POP were 433 per 100,000, 0.03 per 100,000, and 13.07 per 100,000, respectively. 10
A meta-analysis reported a global estimated prevalence of 30.9% for POP, although reported rates vary depending on the diagnostic method used 11 with studies employing physical examination reporting a prevalence of 41.8% compared with 25% in those relying on symptom-based reporting. 11 In sub-Saharan Africa, prevalence estimates vary widely according to the population studied and diagnostic criteria, with rates as high as 46% and 64.6% reported in Gambia and Tanzania, respectively.12,13 In Ghana, studies have reported a prevalence of 2.68% in a hospital-based cohort and 12.07% in a community-based survey, both of which employed pelvic examination as the diagnostic standard.14,15
Surgical correction remains the definitive treatment for symptomatic POP, with the primary objectives of restoring anatomic support, alleviating functional impairment, and improving quality of life. Evidence from high-income settings has demonstrated improvements in prolapse-related symptoms, urinary and anorectal function, and sexual well-being following surgery.16 –19 Similar evidence has emerged from some African countries, albeit within various cultural and healthcare resource contexts.17,20 In Ghana, however, research has focused predominantly on the epidemiology and symptom burden of POP14,15 with no empirical data on the impact of surgical interventions on functional outcomes. This knowledge gap limits the ability of clinicians to provide evidence-based preoperative counseling and hinders informed decision-making regarding surgical approaches and postoperative expectations.
The present study assessed the impact of surgical treatment for POP among Ghanaian women. Specifically, we sought to assess changes in bulge-related symptoms, urinary function, bowel function, and sexual function following reconstructive surgery.
Methods
Study design and setting
We conducted a prospective, hospital-based before-and-after study over an 18-month period (July 2018–December 2019) at two referral centerss in Ghana: Komfo Anokye Teaching Hospital (KATH), a tertiary teaching hospital in Kumasi, and St. Martin’s Catholic Hospital, a secondary-level facility with dedicated urogynecology services.
KATH is the second largest hospital in Ghana and the only tertiary health institution in the Ashanti Region. The hospital is accredited for postgraduate medical training by the West African College of Physicians and Surgeons and the Ghana College of Physicians and Surgeons. It has 13 clinical directorates, including the Obstetrics and Gynecology directorate. The urogynaecology unit, established in 2012, is under the Obstetrics and Gynecology directorate. The unit is run by two consultant urogynecologists, two fellows (senior residents), and two dedicated nurses. An average of 10 patients with POP are seen at the urogynecology clinic held once a week.
St Martin’s Catholic Hospital, located in the Amansie South district of the Ashanti region of Ghana, has a bed complement of 105 and provides a wide range of services, including maternal and reproductive health, child health, general surgery, and specialized chronic disease clinics such as hypertension, diabetes, HIV/AIDS, and TB. The hospital has a urogynaecology specialist who performs various kinds of pelvic surgeries, including POP repair. Approximately 30 pelvic reconstruction surgeries are performed in the hospital annually.
Study population and inclusion/exclusion criteria
The study population included women aged ≥18 years with a diagnosis of stage II or higher POP, confirmed via the Pelvic Organ Prolapse Quantification (POP-Q) system. 21 Patients who opted for surgery and were scheduled for it were included in the study after they have been counseled on the available treatment options, including pessaries and surgery; the benefits and complications of each option; and the appropriate operative procedure to correct their POP. The exclusion criteria were (i) previous pelvic reconstructive surgery and (ii) the presence of neurologic disorders affecting pelvic floor function.
Sample size determination
The sample size was determined on the basis of the mean scores for various urogenital, defecation, and sexual symptoms associated with POP before-and-after surgery.22,23 Assuming a two-sided significance level of 5% and 80% power to detect varying differences in the mean scores of the various symptoms before and after surgery in a sensitivity analysis, the minimum sample size based on constipation 22 was determined to be 88. To account for attrition, an upwards adjustment of 10% was done and 96 women were consecutively recruited into the study.
Study procedure and data collection
All patients with POP reporting to the centers were clinically evaluated by a urogynecologist or a urogynecology fellow. Those who were diagnosed with stage II disease or higher according to the POP-Q system and opted for surgical management were approached by the principal investigator or by a urogynecology fellow (senior resident) trained on the purpose and procedures of the study and how to administer the questionnaires. The purpose and procedures were explained to the participants, and those who consented were consecutively recruited until the required sample size was reached.
Sociodemographic (age, parity) and clinical (stage of prolapse) data were collected on admission before surgery via an investigator-developed, pretested, structured questionnaire. The type of surgery performed and perioperative complications were noted and recorded after surgery.
Prolapse-related symptoms and urinary and anorectal functional assessments were performed via the Pelvic Floor Distress Inventory-20 (PFDI-20), 24 (Supplemental material) whereas sexual function was assessed via the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire, IUGA-Revised (PISQ-IR). 25 The functional assessments via the PFDI-20 and PISQ-IR were performed 1 day before surgery and were repeated 3 months after surgery. The questionnaires were administered by the principal investigator or the senior residents.
The PFDI-20 has 20 questions grouped into 3 parts: the Pelvic Organ Prolapse Distress Inventory-6 (POPDI-6), the Urinary Distress Inventory-6 (UDI-6), and the Colorectal-Anal Distress Inventory-8 (CRADI-8). The POPDI-6 assesses symptoms that result directly from the effect of prolapse, such as pressure in the lower abdomen, heaviness in the pelvis, bulge in the vagina, splinting for bowel movement, incomplete bladder emptying, and splinting for urination. The UDI-6 addresses symptoms of urination, such as frequency of urination, urge urinary incontinence, stress urinary incontinence, dribbling of urine, obstructive micturition, and pain in the lower abdomen. The CRADI-8 assesses 8 anorectal symptoms, such as constipation, obstructive defecation, formed stool incontinence, loose stool incontinence, painful defecation, urgency of defecation, and rectal prolapse during defecation. Each question on the PFDI-20 is scored from 0 to 4, with 0 indicating the absence of symptoms. In the presence of symptoms, responses are graded from 1 to 4 based on the degree of bother, with 1 “not at all,” 2 “somewhat,” 3 “moderately,” and 4 “quite a bit.” The mean value of all the answered items within the corresponding scale (possible value 0–4) is then multiplied by 25 to obtain a scale score ranging from 0 to 100, with zero (0) indicating no dysfunction and 100 representing the worst symptom or dysfunction. Subscales with missing items were calculated by averaging only the answered items within the subscale then multiplying by 25 to get the final scale scores.
The PISQ-IR consists of two parts: the not sexually active (NSA) part for women who are not sexually active and the sexually active (SA) part for sexually active women. The nonsexually active women part of the PISQ-IR has four domain-specific subscales (NSA-PR: Not sexually active—Partner Related, NSA-CS: Not sexually active—Condition Specific, NSA-GQ: Not sexually active—Global Quality, and NSA-CI: Not sexually active—Condition Impact), and the sexually active women part has six domain-specific subscales (SA-AO: Sexually Active: Arousal, Orgasm, SA-PR: Sexually Active: Partner Related, SA-CS: Sexually Active: Condition Specific, SA-GQ: Sexually Active: Global Quality, SA-CI: Sexually Active: Condition Impact, and SA-D: Sexually Active: Desire). Individual items in the PISQ-IR are either scored from 1 to 4 or from 1 to 5. When an item (question) is marked as a reverse response, the score for that item is subtracted from 5 or 6 to arrive at the final response for that item. The mean scores for specific subscales were obtained by summing the valid responses to the items in the subscale and then dividing the results by the number of items with valid responses. At least half of the items in each subscale must be answered (completed) for valid scoring. There was no imputation for missing (non-valid) responses. Higher scores for the NSA part indicate a greater impact of the condition on sexual activity, whereas a greater score for the sexually active part indicates better sexual function.
These validated questionnaires were pretested with 15 women experiencing POP at the St. Michael’s Hospital clinic in Pramso, Ghana, to ensure their clarity, cultural relevance, and ease of understanding before being used in the main study.
Reconstructive surgical procedures were individualized based on clinical findings and patient preferences. Apical suspension techniques performed included sacrospinous ligament fixation (SSLF), McCall’s culdoplasty, uterosacral ligament suspension, and abdominal sacrohysteropexy or colpopexy. These procedures were performed either alone or in combination with vaginal or abdominal hysterectomy and/or anterior and posterior colporrhaphy. Colpocleisis was reserved for women who were unsuitable for extensive reconstructive surgery and who expressed no desire to maintain vaginal sexual function. All surgeries were performed by experienced urogynecologists or senior residents under supervision, including visiting International Urogynaecological Association (IUGA)-affiliated specialists.
Data management and statistical analysis
The data were entered into a password-protected database and analyzed using SPSS version 20 (IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as means with standard deviations for continuous variables and proportions for categorical variables. Measures of functional outcome at baseline and at 3 months post-surgery were compared for significant differences using paired-sample t tests. A two-sided p value <0.05 was considered statistically significant. Before performing the t-test on the sample of 96 participants, the assumption of normality for the differences between pre- and post-surgery outcomes was evaluated. Visual inspections using Q-Q plots and histograms confirmed that each group approximately followed a normal distribution.
Results
Sociodemographic and clinical characteristics of the participants
More than half of the participants (52.08%) were over 60 years old, whereas only 2.08% were under 20 years old. Most of the women (60.41%) had more than five deliveries. Nearly half (47.92%) presented with stage III POP, followed by 34.38% with stage IV POP and 17.70% with stage II POP (POP-Q system; Table 1).
Sociodemographic and clinical characteristics of the participants.

Surgical procedures performed
More than 95% (93/96) of the procedures were performed vaginally, with abdominal procedures accounting for less than 5% (3/96). The commonest procedure performed was vaginal hysterectomy with SSLF (60/96), followed by colpocleisis with perineorrhaphy 12.5% (12/96). (Table 2). The most common perioperative complication was urinary retention (4.16%), followed by severe buttock pain (2.08%).
Types of procedures performed.

AVR, anterior vaginal repair; HUSL, high uterosacral ligament fixation; PVR, posterior vaginal repair; SSLF, sacrospinous ligament fixation.
Changes in prolapse-related, urinary, and bowel symptoms following surgical repair of POP
Following POP repair, significant improvements were observed in pelvic floor symptoms across all three subscales of the PFDI-20: the POPDI-6, the CRADI-8, and the UDI-6 (Table 3).
PFDI-20 before-and-after surgery.
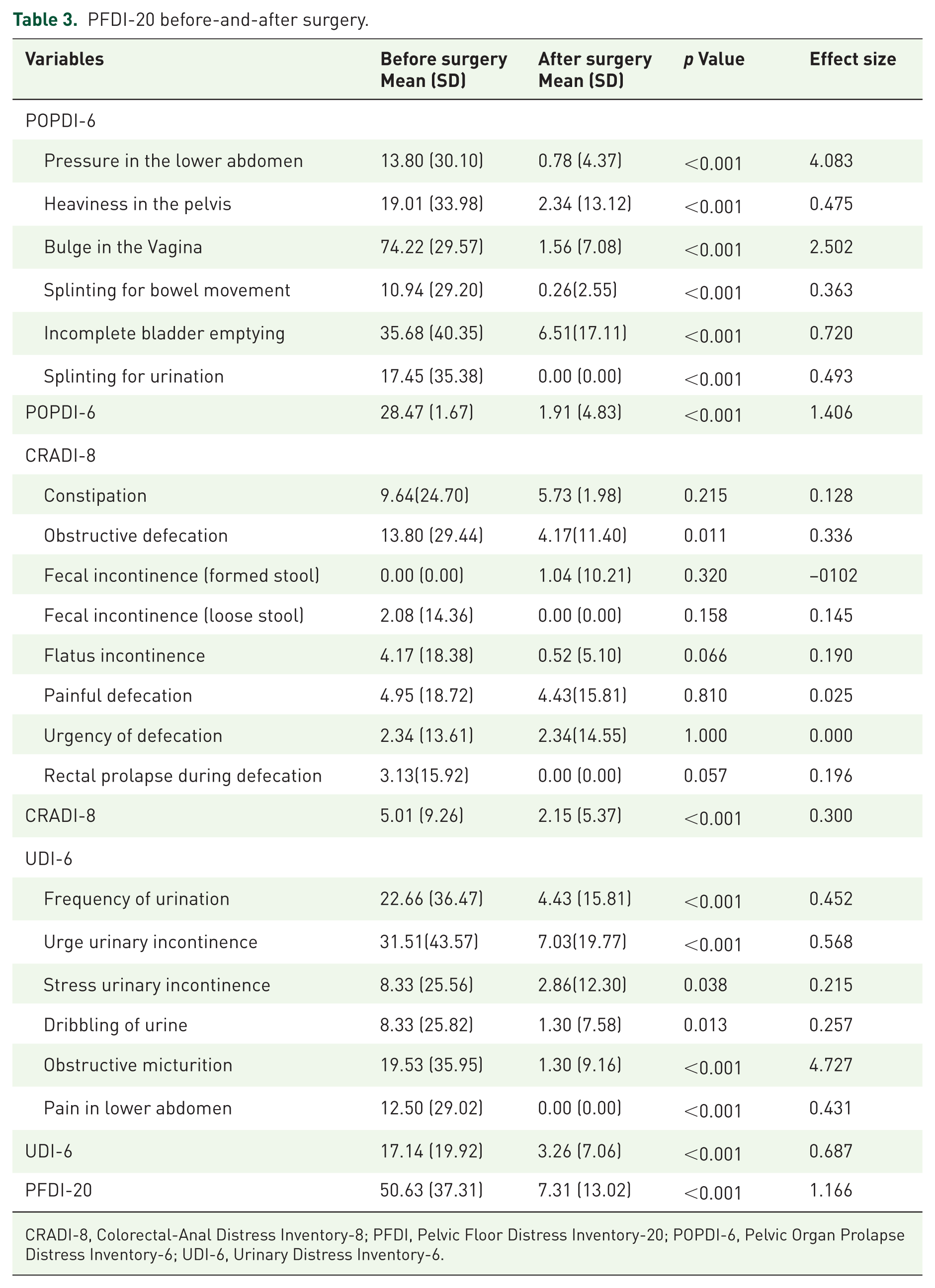
CRADI-8, Colorectal-Anal Distress Inventory-8; PFDI, Pelvic Floor Distress Inventory-20; POPDI-6, Pelvic Organ Prolapse Distress Inventory-6; UDI-6, Urinary Distress Inventory-6.
The POPDI-6 scores substantially decreased from a preoperative mean of 28.47 (SD = 1.67) to 1.91 (SD = 4.83) postoperatively (p < 0.001), Significant reductions were observed in all individual POPDI-6 items, particularly “bulge in the vagina” (mean reduction from 74.22 to 1.56) and “pressure in the lower abdomen” (from 13.80 to 0.78). Notably, “splinting for urination” resolved completely post-surgery (mean = 0.00).
Although most individual components of the CRADI-8 did not demonstrate statistically significant changes postoperatively, the overall CRADI-8 score decreased significantly from 5.01 to 2.15 (p < 0.001).
The UDI-6 scores decreased markedly from 17.14 (SD = 19.92) to 3.26 (SD = 7.06) (p < 0.001). Improvements were observed across all areas, with the most notable reductions in urge urinary incontinence (from 31.51 to 7.03) and obstructive micturition (from 19.53 to 1.30). Postoperative resolution of lower abdominal pain was also noted (mean = 0.00).
Overall, the total PFDI-20 score significantly decreased from 50.63 (SD = 37.31) preoperatively to 7.31 (SD = 13.02) postoperatively (p < 0.001), indicating a clinically meaningful improvement in pelvic floor-related distress following POP surgery.
Sexual function before-and-after POP repair
Majority of participants (86.5%) were NSA at baseline, and the number remained the same 3 months after surgery. Statistical analysis of the PISQ-IR SA participants was not performed because of the low number (13.5%, 13/96) of sexually active participants. The mean scores and standard deviations of the domains of the PISQ-IR of participants who were NSA are shown in Table 4.
Comparison of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (IUGA-Revised (PISQ-IR)) before-and-after surgery.
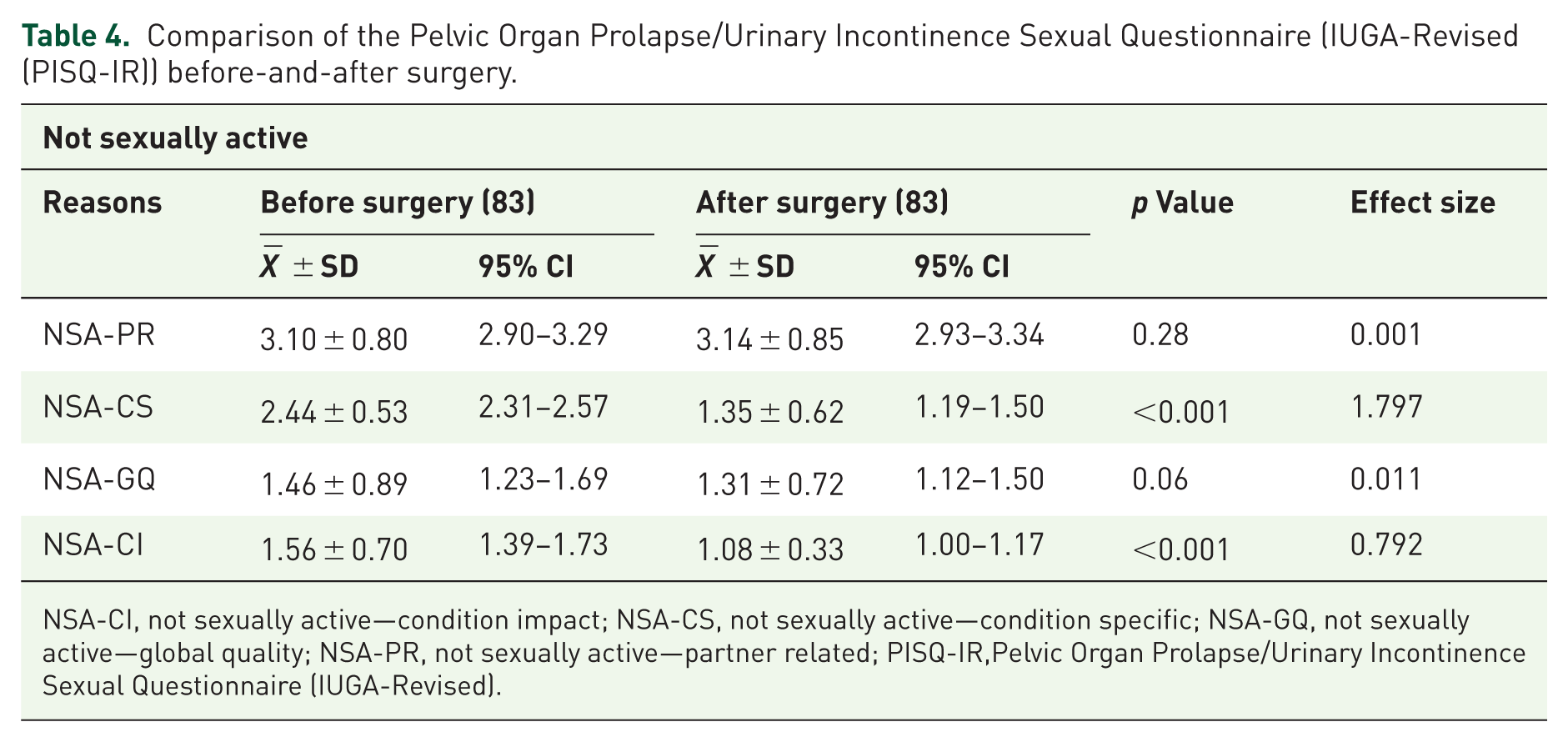
NSA-CI, not sexually active—condition impact; NSA-CS, not sexually active—condition specific; NSA-GQ, not sexually active—global quality; NSA-PR, not sexually active—partner related; PISQ-IR,Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (IUGA-Revised).
There was no statistically significant difference between the preoperative and postoperative mean values of the NSA-PR and the NSA-GQ domains of the PISQ-IR. The mean score of the NSA-PR was 3.10 (±0.80) preoperatively and 3.14 (±0.85) 3 months postoperatively, with a p value of 0.28. Similarly, the mean values (±SD) of the NSA-GQ domain preoperatively and postoperatively were 1.46 (±0.89) and 1.31 (±0.72), respectively (p = 0.06). The NSA-CS and NSA-CI domains, however, significantly improved between the preoperative and postoperative mean values. The NSA-CS mean value decreased from 2.44 ± 0.53 to 1.25 ± 0.62, with a p value of <0.001, and the NSA-CI mean value decreased from 1.56 ± 0.7 to 1.08 ± 0.33, p < 0.001.
Discussion
Key results
This prospective study provides novel and context-specific evidence on the functional benefits of surgical intervention for POP among Ghanaian women. To our knowledge, this is one of the few studies in West Africa to rigorously evaluate patient-reported functional outcomes following reconstructive surgery for POP. These findings suggest that surgical repair is highly effective in reducing the multidimensional symptom burden associated with POP, including prolapse-specific complaints, urinary dysfunction, and bowel difficulties. Furthermore, the results offer important insights into the complex relationship between prolapse surgery and sexual function in a predominantly sexually inactive population.
Sociodemographic and clinical characteristics of respondents
The characteristics of our study population reflect the well-established epidemiological patterns of POP. 26 Most participants were older, multiparous women, which is consistent with the role of cumulative obstetric trauma and aging as key risk factors. 26 The fact that more than four-fifths of women presented with advanced-stage prolapse (stage III or IV) is striking. This late presentation highlights systemic barriers to accessing care in sub-Saharan Africa, including sociocultural stigma, lack of social support, and financial constraints.27 –29 These findings are in line with similar reports from other sub-Saharan African contexts, including Uganda, Ethiopia, and the Democratic Republic of the Congo,28,30,31 where advanced-stage POP is the norm at first presentation.
Types of surgery performed
In this prospective study, various surgical procedures were performed to achieve the observed improvements in the PDFI-20 scores. These procedures included abdominal sacrocolpopexy and vaginal procedures such as SSL fixation, uterosacral ligament fixation, McCall’s culdoplasty, and colpocleisis, along with other concomitant surgeries. The diversity of these procedures introduces potential confounding factors that require careful interpretation. Apical suspension procedures like mesh-based sacrocolpopexy offer superior long-term anatomical support compared to vaginal apical suspension procedures, but they carry the risk of mesh erosion, which may worsen dyspareunia or cause de novo urinary urgency. 32 Patient-reported functional outcomes, such as quality of life, sexual function, and symptom relief for POP, are similar between sacrocolpopexy and vaginal apical suspension procedures. 33 Colpocleisis has demonstrated similar improvements to sacrospinous ligament suspensions in quality-of-life scores, with both procedures showing equivalent results in prolapse symptoms, emotional distress, and general health domains, and satisfaction rates exceeding 85%–90%. However, colpocleisis precludes sexual intercourse by design, limiting its use to sexually inactive patients. 34
The 4.2% complication rate observed in our cohort is notably lower than the 15.59%–32.53% pooled rates reported in a meta-analysis that compared robot-assisted sacrocolpopexy with laparoscopic and abdominal sacrocolpopexies and vaginal procedures. 35 The perioperative complications assessed in this meta-analysis by Grigoryan et al. included cystotomy, enterotomy, vascular or ureteral injury, blood transfusion, wound infection, fever, bowel obstruction, urinary retention, and mesh erosion. The difference in complication rates could be due to several reasons. Meta-analysis aggregate different studies with diverse definitions of complications, surgeons’ experience, and patient comorbidities, and as such, pooled complication rates could be inflated. In addition, women in our cohort underwent primarily vaginal surgeries with sacrospinous fixation as the predominant apical procedure, unlike the meta-analysis, where the predominant surgery was sacrocolpopexy. Sacrocolpopexy involves extensive intraabdominal dissections and synthetic mesh placement, which inherently increases the risk of complications such as cystotomy, enterotomy, and mesh erosion. Furthermore, the follow-up period in our cohort extended to 3 months postoperatively and possibly excluded delayed complications such as mesh erosion and bowel obstruction, which manifest later in mesh-based sacrocolpopexies. This low rate of perioperative morbidity observed in our study underscores the safety of prolapse surgery when performed by trained specialists, even in low-resource environments. 36
Changes in pelvic floor symptoms and Sexual function of participants
The substantial reduction in PFDI-20 scores provides compelling evidence of the effectiveness of reconstructive surgery in this cohort. The most pronounced change was observed in the POPDI-6 subscale, reflecting the resolution of vaginal bulge symptoms and consistent with the alleviation of symptoms following surgery.37,38 Improvements in urinary symptoms, as measured by the UDI-6, were equally notable. The alleviation of incomplete bladder emptying and voiding difficulties may reflect the restoration of normal urethrovesical alignment through anterior and apical compartment repair.39,40 In addition, the marked reduction in urgency and urge incontinence is consistent with the hypothesis that prolapse correction can mitigate overactive bladder symptoms by restoring anatomical support and reducing detrusor overactivity. 40
The CRADI-8 results require a more nuanced interpretation. Improvements were largely confined to obstructive defecation, which is consistent with the mechanical correction of rectoceles and related posterior compartment defects.41,42 However, the absence of significant improvement in fecal incontinence or chronic constipation is unsurprising. These symptoms are often multifactorial and driven by dietary habits, colonic transit abnormalities, or intrinsic sphincter dysfunction, which are not directly addressed by prolapse surgery.43,44
The evaluation of sexual function adds an important layer of understanding to the impact of POP surgery. The very high prevalence of sexual inactivity (86.5%) underscores the profound disruptive effect of prolapse on intimate relationships, a trend well documented in the global literature.15,45 Notably, our analysis of the PISQ-IR revealed significant gains in NSA-CS and NSA-CI domains among sexually inactive women. These findings suggest that surgery possibly eliminates physical barriers to sexual activity, such as bulge symptoms and discomfort, thereby restoring the potential for sexual engagement.46 –49 It is important to state that the results on sexual function are primarily based on the NSA domains of the PISQ-IR and therefore reflect perceived impact and potential for future sexual activity, rather than measured sexual performance.
Nevertheless, the absence of significant changes in the NSA-PR and NSA-GQ global calls for careful interpretation. These domains capture the relational and psychosocial aspects of sexual health, which are shaped not only by physical symptoms but also by long-standing abstinence, partner health, relationship quality, and cultural perceptions of sexuality, particularly in postmenopausal women.50,51 These dynamics may play a significant role in shaping postoperative sexual experiences and may require longer than 3 months or a different intervention to resolve. In other words, meaningful changes in sexual activity or relational factors might require a longer time frame than 3 months and, in some cases, couple-based counseling. These results reinforce the importance of preoperative counseling to set realistic expectations: while surgery may restore the anatomical and functional capacity for intercourse, it does not guarantee the recovery of broader relational or psychological aspects of sexual health.
The improvements in functional outcomes in our cohort were achieved using the open abdominal and vaginal surgical route, which involves greater tissue dissection and longer recovery time. Emerging techniques such as vaginal natural orifice transluminal endoscopic surgery (vNOTES) offer a minimally invasive hybrid by combining vaginal accessibility with laparoscopic efficacy in the repair of POP.52 –54 Though direct comparative studies of vNOTES and traditional surgical methods used in this cohort remain limited, the newer techniques have been shown to offer comparable improvements in the PFDI-20 scores 55 and better anatomical correction.52,54,56 alongside advantages of shorter hospital stay, shorter operating time, better cosmetics, and fewer perioperative complications compared to the laparoscopic and traditional approaches.52,54,56 Future studies comparing vNOTES to traditional techniques used in this study are necessary to evaluate PFDI-20 trends against reduced morbidity.
Strengths and limitations
The strengths of this study include its prospective design, use of validated patient-reported outcome measures,24,25 and focus on a Ghanaian population, filling a critical evidence gap in the region.
However, several limitations must be acknowledged. The follow-up period of 3 months captures functional outcomes, such as initial symptoms relief and quality of life improvements. However, surgical repair of POP is known for its potential delay in recurrence and de novo symptoms that often emerge after a period of 1 year.38,57 The short follow-up of 3 months is considered a limitation in the study; therefore, care should be taken in interpreting the findings from this study as long-term efficacy.
The findings of this study should be interpreted within the specific context of our patient population, which predominantly comprises older, multiparous women, about 70% of whom are likely postmenopausal (age range of 50 years and above) with advanced-stage prolapse who opted for surgical management. The substantial improvement in the PDFI-20 scores could be due to the diminished protective effect of estrogen deficiency on pelvic connective tissue strength 58 which has the potential of worsening the preoperative symptoms burden of PFDI-20 and thereby exaggerating postoperative gains. 59 Therefore, our results cannot be generalized to all women with POP in Ghana or sub-Saharan Africa, particularly younger women, those with early stage prolapse, or individuals opting for non-surgical management.
The findings on sexual function are primarily based on the NSA domain of the PISQ-IR, as statistical analysis of the sexually active domains was not conducted due to the limited number of sexually active participants (13/96). As a result, these findings cannot be generalized to SA women.
The reliance on self-reported measures, although validated, may introduce response bias. The small subset of SA participants limited subgroup analyses of sexual outcomes. Furthermore, the absence of an independent control group makes causal inference difficult.
Conclusion
The improvements observed across the prolapse, urinary, and bowel domains highlight surgery as a possible high-yield intervention, particularly in contexts where nonsurgical management options are limited or underutilized. Importantly, the data generated provide relevant evidence to support patient counseling, inform shared decision-making, and guide realistic expectations regarding both the benefits and limitations of surgery.
Future studies should aim at prospective designs of 12–24 months follow-up with larger and more diverse that is, younger and sexually active cohorts, to enhance generalizability and clinical applicability. Incorporating objective anatomical and functional assessments would complement patient-reported outcomes. Mixed-methods research, which combines quantitative tools with qualitative interviews, could provide deeper insights into cultural, relational, and psychosocial barriers to sexual health recovery.
Footnotes
Acknowledgements
The authors are grateful to the study participants and the management of the study hospitals.
Declarations
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence policy
No generative AI was used in the writing, analysis, or production of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.