
Abstract
Background:
Unsafe induced abortion contributes a significant public health concern in Ethiopia and is one of the leading causes of maternal morbidity and mortality. Previous studies have explored the burden of induced abortion. However, little evidence exists in the context of Hawassa city.
Objective:
To identify the Risk factors associated with induced abortion among women attending health facilities in Hawassa city, Sidama Region, southern Ethiopia, 2024.
Design:
An institution-based unmatched case-control study design.
Methods:
A multistage sampling technique was employed to select 513 women of reproductive age attending public health facilities in Hawassa city from June 25 to August 25, 2024. Data were collected electronically through face-to-face interviews via a structured questionnaire adapted from previous studies. Descriptive analysis was conducted to describe the participants. Bivariable and multivariable binary logistic regression were used to identify risk factors associated with induced abortion.
Results:
In this study, 513 (172 cases and 341 controls) women were included, for a response rate of 95.4%. Primary education (adjusted odds ratio (AOR) = 2.58, 95% CI: 1.20, 5.53), early sexual debut before age 18 (AOR = 5.40, 95% CI: 2.80, 10.41), previous history of abortion (AOR = 3.50, 95% CI: 1.78, 6.90), poor knowledge about contraceptives (AOR = 5.11, 95% CI: 2.69, 9.72), and alcohol consumption (AOR = 2.76, 95% CI: 1.53, 4.98) were associated with increased odds of induced abortion. Conversely, ever use of contraceptives was associated with lower odds of induced abortion (AOR = 0.38, 95% CI: 0.21, 0.72).
Conclusion:
The current study points out that early sexual debut before age 18, previous history of abortion, poor knowledge about contraceptives, and alcohol consumption were factors associated with induced abortion. These findings highlight further investigation in longitudinal studies.
Plain language summary
• Induced abortion remains a significant public health problem in developing country particularly Ethiopia and is one of the leading causes of maternal mortality and morbidity.
• An institution-based unmatched case-control study design was employed among 513 reproductive-age groups of women attending public health facilities in Hawassa city from June 25 to August 25, 2024.
• The current study figure out pertinent risk factors for induced abortion such as Primary education, early sexual debut before age 18, previous history of abortion, poor knowledge about contraceptives, and alcohol consumption, were associated with increased odds of induced abortion. Conversely, ever use of contraceptives was associated with lower odds of induced abortion.
• These findings underscore highlights the need for further investigation in longitudinal studies to explore more in detail causal risk factors. Comprehensive interventions targeting education, sexual and reproductive health awareness, contraceptive knowledge and use, and alcohol consumption to reduce the prevalence of induced abortion and its associated health risks in this population.
Introduction
According to the World Health Organization (WHO), an “unsafe abortion” occurs when a pregnancy is terminated either by an unskilled provider, without the required medical skills, in a setting in unhygienic conditions that fails to meet basic medical standards, or both. 1
Induced abortion continues to be a major global public health issue, especially in low- and middle-income countries (LMICs), where there is often restricted availability of safe abortion services. 2 The WHO estimates that approximately 73 million induced abortions occur annually worldwide, of which around 45% are unsafe, and the majority of the proportion concentrated in developing nations. 3 Unsafe induced abortion remains a critical global public health challenge, disproportionately affecting low-resource settings, including Ethiopia.2,4 In Ethiopia, this burden is reflected in 620,000 induced abortions per year, 5 while studies have documented a pooled pregnancy termination prevalence of 22% nationally. 6 The prevalence of induced abortion in Ethiopia is particularly barriers because of its frequent association with unsafe practices, which can result in severe complications and, in some cases, maternal mortality. 9 Previous studies conducted in Ethiopia focused on different aspects related to induced abortion, including its magnitude and health-seeking behaviors.14 –16
Furthermore, unsafe induced abortion is among the leading causes of maternal morbidity and mortality in the country, 7 Another studies have shown similar evidence face an increased risk of morbidity and mortality.6,7
Unsafe abortion is a major global problem for women's health, causing 5%–14% of all maternal deaths from complications like severe bleeding and infection. It also has serious health and socioeconomic effects on women and their communities.2,4 It contributes to 4.7%–13.2% of maternal deaths annually. 8 The recent large meta-analyses report showed clearly that induced abortions are associated with maternal complications.9,10 In developed regions, an estimated 30 fatalities per 100,000 cases are reported, while this figure increases to 220 fatalities per 100,000 cases in developing regions. 2 Induced abortions contribute to 13% of maternal mortality in Ethiopia, 7 with far-reaching consequences that extend beyond individual health outcomes. These preventable tragedies not only devastate individual lives but also impose substantial strains on Ethiopia’s healthcare system and economic productivity. 11 Recent estimates project annual costs of US$553 million for treating post abortion complications, coupled with US$922 million in lost income due to long-term disability stemming from unsafe procedures. 12 This dual financial burden underscores the critical importance of investing in accessible reproductive healthcare services to mitigate both human and economic costs. There have been efforts to address the issue of induced abortion and reduce the risks associated with it at different levels. Globally, the WHO has given recommendations and policies for safe abortion care and post abortion care, thus emphasizing the need to provide safe and legal abortion services and post abortion care. 11 Regionally, several African countries have made progress in liberalizing abortion laws and policies, aiming to reduce the burden of unsafe abortions. 12 In 2005, Ethiopia revised its penal code, which permits abortion in cases of rape, incest, or fetal abnormality, and for women with physical or mental disabilities. In addition, the government has attempted to increase the capacity of health care workers in comprehensive abortion care, and safe abortion services have been incorporated into public health facilities. 9 Nevertheless, many issues remain unchanged, such as restricted access to services, cultural norms and practices, and a shortage of personnel, especially in rural areas. Thus, more efforts should be made to identify and overcome the risk factors associated with unsafe induced abortion.9,13
Evidence has shown that knowledge and attitudes toward contraceptives have been widely explored as potential risk factors of induced abortion. Several studies in Ethiopia have shown that women with limited knowledge or negative attitudes toward contraceptive methods are more likely to undergo unsafe induced abortions than are those with better knowledge and positive attitudes.28 –30 Moreover, inadequate knowledge about the use of contraceptives, their effectiveness, and potential side effects of contraceptive methods may lead to inconsistent or improper use, increasing the risk of unintended pregnancy and subsequent abortion.29,31 Studies in Ethiopia have shown that women who never use contraceptives are more likely to undergo unsafe induced abortions than are those with a history of contraceptive use.29,32
On the other hand, few studies focused on the specific risk factors associated with induced abortion have been carried out in this context. 17 Most of the previous studies were cross-sectional studies, which have a limited ability to establish causal relationships between the risk factors and the outcome of induced abortion.13 –15 Furthermore, the findings from these studies have been inconsistent, with varying factors identified as influencing a woman’s decision to seek an induced abortion.6,15 This necessitates a more thorough study design, such as an unmatched case-control study, to understand the complicated interactions between variables. Moreover, the literature has focused mainly on general socioeconomic and reproductive health-related factors, whereas the impact of behavior, including those originating from partners, has emerged as underutilized in the Ethiopian context.16,17 Moreover, most of the earlier studies were conducted on the burden of induced abortion in other regions in Ethiopia. However, studies of the associated risk factors of induced abortion in specific study areas are limited. Therefore, this study aims to identify the risk factors associated with induced abortion among women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia. The main motivation of this study was to identify associated factors with induced abortion to inform public health strategies that may reduce maternal mortality and morbidity, particularly in the context where unsafe procedures are practiced.
Methods and materials
Study area and period
The study was conducted in Hawassa city, the capital of the Sidama Regional State, which is located in the Great Rift Valley of southern Ethiopia. Hawassa city is bounded by the southern Arsi Zone in North, Wondo Genet Woreda in East, Melga Woreda in Southeast, Shebedino Woreda in South, and Lake Hawassa in West China and North West. The city is divided into eight administrative subcities and 32 kebeles (20 urban and 12 rural). According to the 2023 Hawassa city administration projection, the total number of people living in the city administration is 402,903, of which 205,078 (50.9%) are females. 18
Hawassa city is a major urban center and a hub for healthcare services in the region. The city has 83 public and private health institutions: one Public Comprehensive Specialized Referral Hospital, two Public General Hospitals, two Public Primary Hospitals, four Private Primary Hospitals, 11 Public Health Centers, 17 Public Health Posts, and 53 Private Clinics. 18 The study was carried out in five public health facilities within the city: Adare General Hospital, Motite Fura Primary Hospital, Alamura Health Centre, Millennium Health Centre, and Tilte Health facility. The study was conducted between June 25 and August 25, 2024 (Figure 1). The current study focused on induced abortion in general, not differentiating between unsafe and safe procedures.
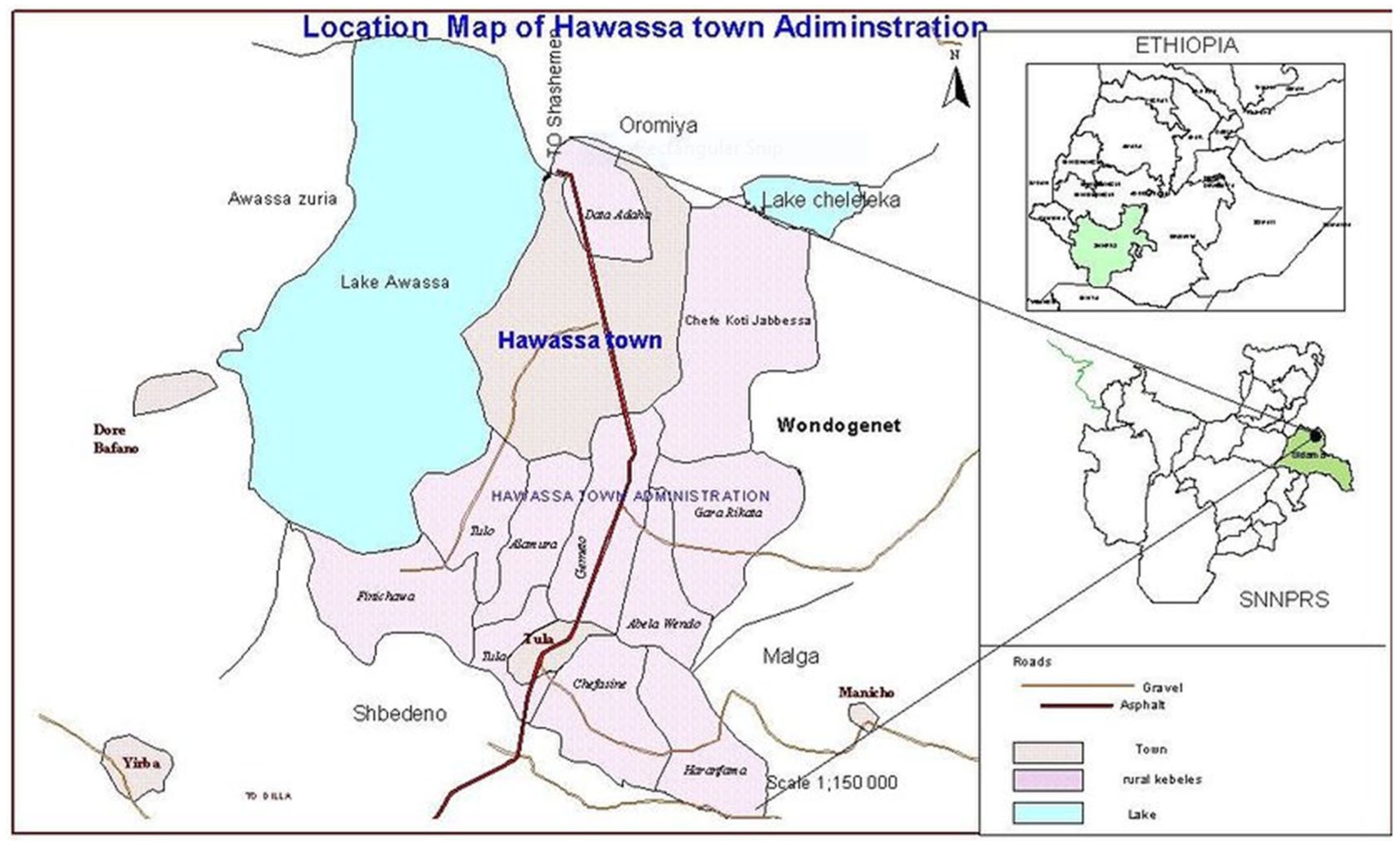
Administrative map of Hawassa city. 18
Study design
An institution-based unmatched case-control study design was employed. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplement Material). 19
Population
Source and study population
All women of reproductive age visiting public health facilities in Hawassa city composed the source population.
Cases: Reproductive-age group of women who underwent an induced abortion at the selected public health facilities in Hawassa city during the data collection period. Researchers considered clinical records as the primary source, and spontaneous abortions were excluded based on the physician’s diagnosis.
Controls: Reproductive-age group of women who attended antenatal care visits and family plans at public health facilities in Hawassa city during the data collection period.
Inclusion and exclusion criteria
Cases: All women of reproductive age who underwent an induced abortion at the selected public health facilities in Hawassa city during the data collection period were included.
Controls: All women of reproductive age attending antenatal care visits and family planning at public health facilities in Hawassa city during the data collection period were included.
Patients: Women who had severe medical illnesses and were unable to communicate during the data collection were excluded.
Controls
Women who were currently pregnant with a gestational age beyond 28 weeks, those with severe medical illness, and those who were unable to communicate were excluded.
Sample size determination
The sample size for the unmatched case-control study was determined via Epi Info version 7.2 statistical software (Centers for Disease Control and Prevention (CDC), Atlanta, America). The calculation was based on the following assumption: confidence level: 95%, power: 80%, ratio of controls to cases: 2:1, proportion of controls with exposure: 7.5%, 17 adjusted odds ratio (AOR): 2.9. 17
On the basis of these assumptions, the sample size was 326. To account for the multistage sampling design, a design effect (deff = 1.5) was incorporated, resulting in a required sample size of 489. Additionally, to accommodate the nonresponse rate, an additional 10% of the final sample size was added, resulting in a final sample size of 538 participants, consisting of 179 cases and 359 controls.
Sampling technique and procedure
From a total of four public hospitals and 10 health centers in Hawassa city, two hospitals (Adare General Hospital and Motite Fura Primary Hospital) and three health centers (Alamura Health Centre, Millennium Health Centre, and Tilte Health Centre) were randomly selected from the list of public health facilities in Hawassa city.
The total sample size was then proportionally allocated to each selected facility on the basis of the estimated number of women seeking induced abortion services. The monthly average numbers of induced abortion services at Adare, Motite Fura, Alamura, Millennium, and Tilte were 74, 45, 38, 56, and 25, 20 respectively. To obtain samples from each health facility, the proportional allocation formula was used (which is as follows: sample size/population size * stratum size, where sample size (cases) = 179 and population size is the sum of all strata = 238). Accordingly, 56, 34, 29, 41, and 19 cases were selected from Adare, Motite Fura, Alamura, Millennium, and Tilte, respectively.
During field data collection, qualified female participants were recognized via healthcare facility documentation (patient register) at reproductive health centers. Recruitment: After identification, women who met the inclusion criteria were contacted privately in a secure setting by trained data collectors. After the services, provisional voluntary participants were recruited. Besides, researchers ensured confidentiality and kept sensitive aspects of abortion care, not including personnel identifying data, and written consent was taken from each study participant. Finally, a systematic sampling method was used to recruit the study participants from the selected facilities during the data collection period. Every other woman meeting the inclusion criteria was selected, where 2 kth is the sampling interval calculated by dividing the estimated number of eligible women at each facility during the data collection period by the allocated sample size for that facility (k = 238/179 ≈ 2). The initial woman was selected as a binary choice, represented by 0 and 1, to determine her inclusion. Selected one, and subsequently, every alternate woman is chosen until the sample size is fully filled (Figure 2).

Schematic representation of the sampling procedures used to identify the risk factors of induced abortion among women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia.
Variables
Dependent variable
Induced abortion (yes/no)
Independent variables
Data collection instruments and data collection procedures
A structured questionnaire was adapted from previous similar studies conducted in Ethiopia.15 –17,21 The questionnaire was divided into four sections on the basis of the categories of independent variables identified in the literature review: sociodemographic characteristics, reproductive health-related factors, contraceptive-related factors, and behavioral and other related factors.
The questionnaire was initially prepared in English and then translated into Amharic, the local language widely spoken in the study area. The translated version was back-translated to English to ensure consistency and accuracy. The questionnaire was then coded and uploaded to the Kobo Toolbox, a secure open-source data collection platform, for electronic data capture via mobile devices.
Five nurses with previous experience in data collection were recruited and trained to administer the questionnaire. The data collectors approached eligible women at the selected public health facilities after they received the relevant health services (induced abortion or other reproductive health services). The data collectors then administered the questionnaire via mobile devices equipped with the Kobo application. The questionnaire was completed through face-to-face interviews in a private setting to ensure confidentiality and privacy. To ensure smooth data collection and data quality, a public health officer with previous experience in data collection and proficiency in the Kobo collection application supervised the process daily.
Data quality assurance
The assurance of data quality was achieved through different strategies. The questionnaire was pretested on a small sample of women (5% of the total sample size) from a public health facility (Tulla General Hospital and Tulla Health Centre), not included in the study, one week prior to the actual data collection, to identify and address any potential issues or ambiguities. In addition, the data collectors received two days of training on the study objectives, data collection procedures, ethical considerations, and use of the Kobo application. The Kobo Toolbox application was programmed with a built-in range and consistency checks to minimize data entry errors. Regular supervision and monitoring of the data collection process were conducted by the principal investigator and field supervisor to ensure adherence to the study protocol and address any challenges or concerns.
Data processing and analysis
The data collected through the Kobo application were downloaded and exported to the Statistical Package for Social Sciences (SPSS) version 26 (New York, USA) for analysis. The researchers have conducted data cleaning through data inspection, checked missing values, outliers, duplications, and the consistency of data. Descriptive statistics, including frequencies, proportions, continuous variables computed on means, and standard deviations, were calculated to summarize the sociodemographic, reproductive health, contraceptive, and behavioral characteristics of the study participants. The results are presented in text, tables, and graphs. The reliability test was tested using Cronbach’s α, which was calculated to be 0.747.
Bivariable binary logistic regression was conducted to assess the association between each independent variable and induced abortion. Variables with a p value < 0.25 were included in the multivariable binary logistic regression analysis. During multivariable binary logistic regression, the fit of the regression model was evaluated via the Hosmer & Lemeshow test (p value = 0.153). The variance inflation factor (VIF) was used to check for multi-collinearity among continuous independent variables (VIF < 10). Variables with a p value of <0.05 were considered independent risk factors of induced abortion. The magnitude of association is shown via the AOR with a 95% CI.
Operational definitions
Results
Sociodemographic characteristics
A total of 513 (172 cases and 341 controls) women participated in the study, with a response rate of 95.4%. The mean (SD) age of the cases was 24.3 (±6.1), whereas the mean age of the controls was 27.9 (±5.4) years. Compared with the controls (19.1%), more than half (52.3%) of the cases were aged ⩽24 years. With respect to marital status, 83 (48.3%) of the cases were unmarried, whereas 255 (74.8%) of the controls were married. Seventy (40.7%) of the cases had a primary education, whereas 161 (47.2%) of the controls had a college education or above. With respect to occupation, 98 (57.0%) of the cases were housewives, whereas 166 (48.7%) of the controls were employees. The vast majority of both groups resided in urban areas (170 (98.8%) of the cases and 328 (96.2%) of the controls). The median (IQR) monthly income for cases was 5000 (4000) birr, and for controls, it was 7000 (3125) birr. Income levels were generally lower among cases, with 58 (33.7%) earning ⩽3000 Birr, than among controls, where 124 (37.1%) earned 6001–9000 Birr (Table 1).
Sociodemographic characteristics of women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia, 2024.

Reproductive health-related factors
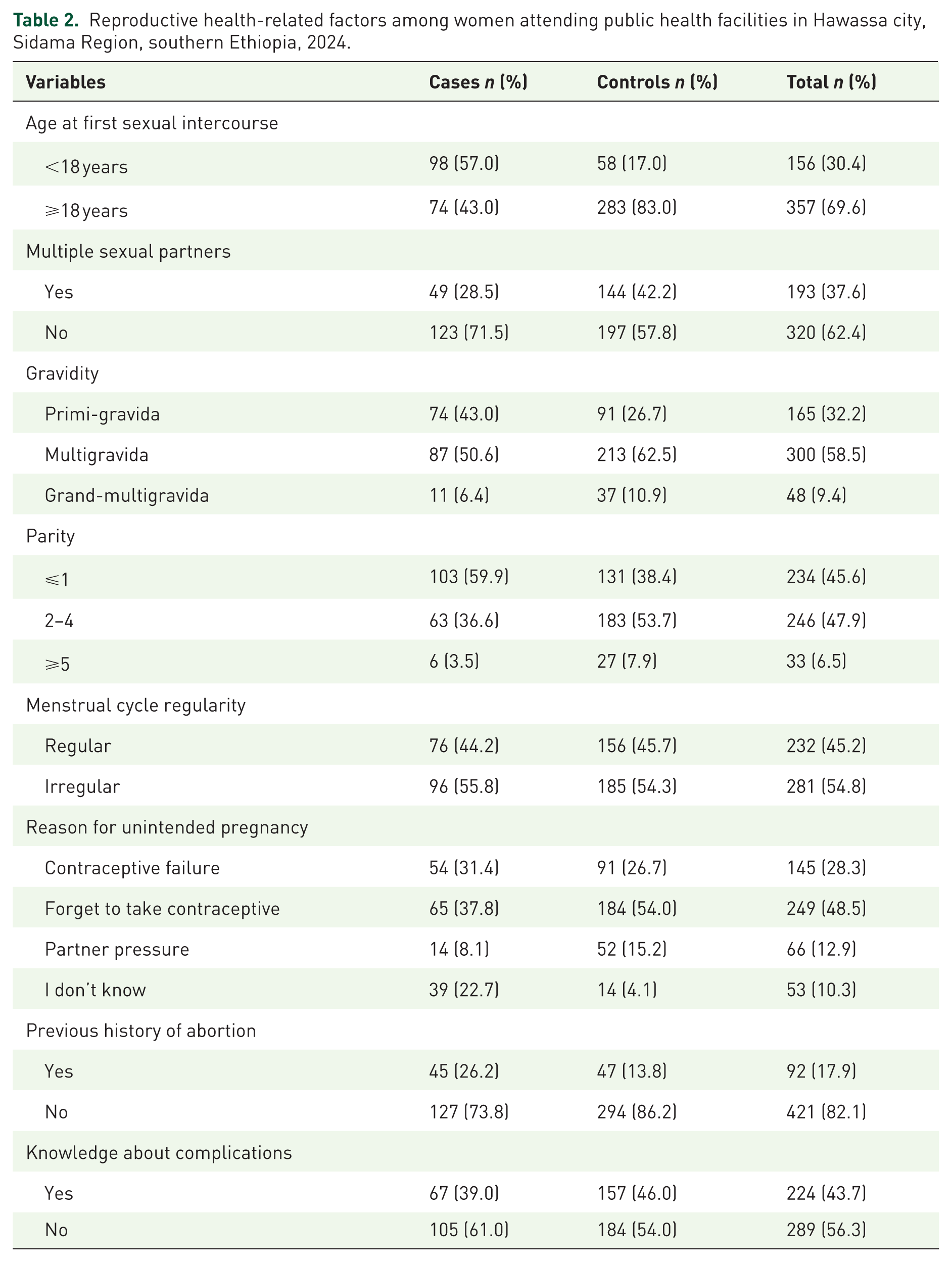
More than half, 98 (57.0%) of the cases reported sexual debut at <18 years, whereas 58 (17.0%) of the controls reported sexual debut at <18 years. Forty-nine (28.5%) cases and 144 (42.2%) controls had multiple sexual partners in their lifetime. More than half (50.6%) of the cases and 213 (62.5%) of the controls were multigravidas (2–4 pregnancies). Compared with controls (38.4%), cases had a greater proportion of women with ⩽1 parity (59.9%). Sixty-five (37.8%) of the cases revealed that the main reason for unintended pregnancy was forgetting to take contraceptives, which was even more common among controls (184, 54.0%). With respect to the history of abortion, 45 (26.2%) cases and 47 (13.8%) controls reported previous abortions. Approximately 67 (39%) of the cases and 157 (46%) of the controls were aware of abortion complications (Table 2).
Reproductive health-related factors among women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia, 2024.
Contraceptive-related factors
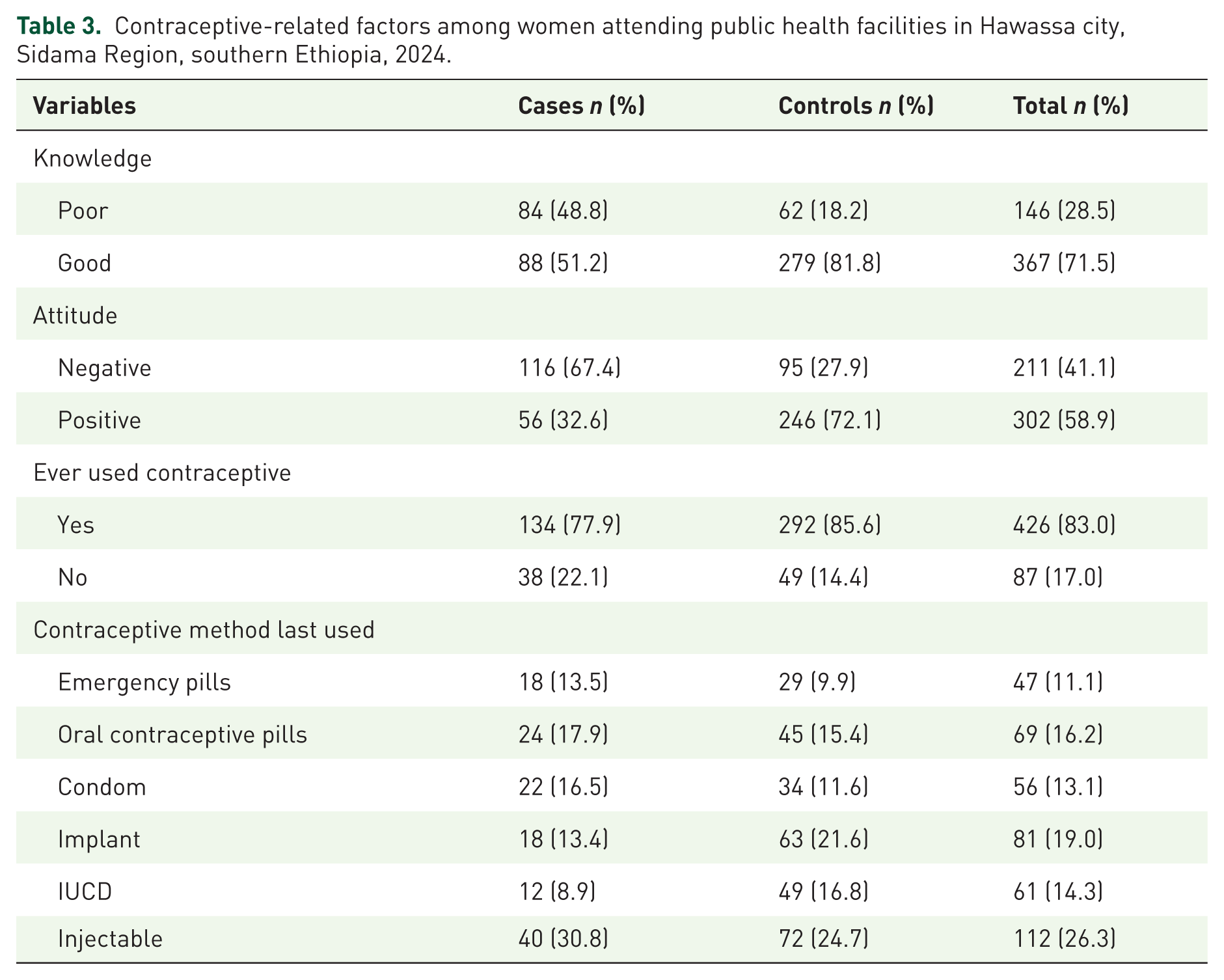
The mean (SD) contraceptive knowledge score of the cases was 5.9 (1.4), whereas the control group had a mean knowledge score of 7.1 (±0.9). Nearly half (84(48.8%) of the patients had poor knowledge of contraceptives, whereas 62 (18.2%) of the controls had poor knowledge. The mean (SD) attitude scores among the cases and controls were 29.2 (±2.7) and 31.3 (±2.1), respectively. Similarly, 116 (67.4%) of the cases had a negative attitude toward contraceptives, whereas 95 (27.9%) of the controls had a negative attitude toward contraceptives. Both groups reported high rates of ever using contraceptives, with 134 (77.9%) cases and 292 (85.6%) controls. Among those who used contraceptives, injectables were the most common method for both patients (30.8%) and controls (24.7%; Table 3).
Contraceptive-related factors among women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia, 2024.
Behavioral and other related factors
Seventy-one (41.3%) patients and 52 (15.2%) controls consumed alcohol in the past 3 months. With respect to chat chewing, 22 (12.8%) patients and 38 (11.1%) controls chewed khat in the past three months. Social support was mostly moderate in both groups (61.0% of the cases and 61.6% of the controls), although poor support was more common among the cases (21.5%) than among the controls (9.1%). The cases experienced higher rates of physical violence (34.9%) and sexual violence (31.4%) than did the controls, who reported rates of 19.4% and 27.3%, respectively. Partner alcohol use was reported by 37.8% of the cases, whereas it was reported by only 30.4% of the controls. Furthermore, 6.9% of the cases reported that their partner smoked cigarettes, whereas 5.7% of the controls reported the same. Chat chewing among partners was also more common among the cases (20.9%) than among the controls (14.4%; Table 4).
Behavioral and related factors among women attending public health facilities in Hawassa city, Sidama Region, southern Ethiopia, 2024.

Risk factors associated with induced abortion
In the bivariable logistic regression analysis, several factors were found to be significantly associated with induced abortion, including age, marital status, educational status, age at first sexual intercourse, gravidity, history of abortion, knowledge, attitudes, contraceptive use, alcohol consumption, social support, and experiences of physical violence. After adjusting for potential confounders in the multivariable logistic regression, the independent risk factors of induced abortion were identified as educational status, age at first sexual intercourse, history of abortion, knowledge, contraceptive use, and alcohol consumption.
Women with a primary education had 2.58 times greater odds of having an induced abortion than those with a college education or higher (AOR = 2.58, 95% CI: 1.20, 5.53). In addition, women who initiated sexual intercourse before the age of 18 years had 5.40 times greater odds of induced abortion than those whose first sexual intercourse occurred at or after 18 years of age did (AOR = 5.40, 95% CI: 2.80, 10.41). The odds of induced abortion were 3.5 times greater among women with a previous history of abortion than among those without such a history (AOR = 3.50, 95% CI: 1.78, 6.90). Women with poor knowledge of contraceptives had 5.11 times greater odds of induced abortion than those with good knowledge (AOR = 5.11, 95% CI: 2.69, 9.72). Contraceptive use was also a significant factor, with women who had ever used contraceptives having 62% lower odds of induced abortion than those who had never used contraceptives (AOR = 0.38, 95% CI: 0.21, 0.72). Finally, alcohol consumption was found to increase the odds of induced abortion by 2.76 times compared with women who did not consume alcohol (AOR = 2.76, 95% CI: 1.53, 4.98; Table 5).
Bivariable and multivariable analysis of determinants of induced abortion among women attending public health facilities in Hawassa City, Sidama Region, southern Ethiopia, 2024.

Statistically significant.
AOR, adjusted odds ratio; COR, crude odd ration.
Discussion
In this case-control study, researchers evaluated the risk factors of induced abortion among women attending public health facilities in Hawassa City, Sidama Region, southern Ethiopia. The findings revealed that primary educational status, age at first intercourse less than 18 years, previous history of abortion, poor knowledge of contraceptives, prior contraceptive use, and alcohol consumption were independent factors significantly associated with induced abortion.
The current study revealed that women with a primary education had approximately three times greater odds of having an induced abortion than those with a college education or higher. This finding concurs with other studies conducted in Addis Ababa 17 and the Amhara Region, 25 which revealed that a high probability of induced abortion was associated with a low educational status in women. This association could be explained by the fact that women with lower education levels have limited access to sexual and reproductive health information, leading to poor contraception knowledge and usage and high vulnerability to unplanned pregnancies. In addition, lower educational status is often associated with fewer economic opportunities that reduce financial security, which may influence decisions regarding pregnancy continuation. 4
The study found a fivefold increased association (AOR = 5.0) for induced abortion among women with adolescent sexual debut (age < 18 years) compared to those initiating at ⩾18 years. This finding is consistent with studies performed in Addis Ababa, 17 Arba Minch, and Wolayita Sodo town, 16 Nigeria, 26 and a systematic review of studies in Ethiopia 6 that reported higher odds of induced abortion among those who initiated sexual activity at a younger age. This could be explained by the fact that adolescents engaging in early sexual activity may lack adequate knowledge about contraception and reproductive health, increasing their vulnerability to unintended pregnancies.6,27 Moreover, younger women are more likely to be stigmatized socially and to face economic hardships associated with unintended pregnancies, which could lead to a greater likelihood of induced abortions. 27 Thus, this robust association underscores the critical need for targeted sexual health interventions addressing early reproductive transitions.
The study revealed that a previous history of abortion was associated with induced abortion by 3.5 times compared with those without such a history. This finding is supported by studies from the Tigray Region, Ethiopia, 28 and Burkina Faso, 29 who reported that women with a history of previous induced abortions were more likely to have undergone subsequent abortions. However, a study conducted in Bahir Dar, Ethiopia, reported the opposite, where 71% fewer women requested abortion among those with a previous abortion history. 21 Repeated induced abortion accounts for a substantial proportion of induced abortions in many countries, and the estimated pooled prevalence of repeat-induced abortion in Ethiopia is 30.89%. 30 The greater likelihood of repeat abortions might be because women who have undergone a previous abortion may face challenges with effective contraceptive use or persistent socioeconomic factors that contribute to unintended pregnancies. In addition, experiencing an earlier abortion may minimize perceived obstacles or stigma from women or make them more likely to see the option once they confront subsequent unwanted pregnancies. 28
Induced abortion was associated with knowledge about contraceptives; women with poor knowledge had five times greater odds of induced abortion than those with good knowledge. This finding is consistent with studies conducted in Arba Minch and Wolayita Sodo towns, southern Ethiopia, 16 Ethiopia, 31 and Ghana, 32 which revealed that limited knowledge about contraceptive methods was associated with a greater likelihood of induced abortion. This could be because inadequate knowledge about contraceptive methods may lead to inconsistent or incorrect use, increasing the risk of unintended pregnancies. Moreover, women with limited contraceptive knowledge may be less aware of their reproductive options, potentially leading to delayed or inadequate family planning practices.
The findings of the study revealed that women who ever used contraceptives had 62% lower odds of induced abortion than those who never used contraceptives. This result is consistent with studies performed in Hawassa city, southern Ethiopia, 33 and Debre Markos, northwestern Ethiopia. 34 Evidence suggests that women with prior contraceptive use exhibit a reduced associations of undergoing induced abortion. Furthermore, contraceptive utilization demonstrates a protective association against repeat abortion procedures. This may be explained by the fact that women with a history of contraceptive use are likely to have more knowledge and understanding of family planning methods, which could result in more effective prevention of pregnancy. 34 In addition, the use of contraceptives in the past could be an indicator of better contact with reproductive health services, which may provide broader benefits for reproductive health outcomes and choices.
Furthermore, the study revealed that alcohol consumption increased the associations of induced abortion threefold compared with not consuming alcohol. This finding is supported by studies from Hosanna, southern Ethiopia 35 ; Debre Markos, northwestern Ethiopia 34 ; and a multilevel analysis of Ethiopian Demographic and Health survey (EDHS), Ethiopia. 36 Emerging evidence highlights alcohol consumption as a risk factor for induced abortion, with studies demonstrating its association with both first-time and recurrent pregnancy termination. 37 This pattern underscores the role of alcohol use in exacerbating reproductive health risks and repeat procedures. One possible explanation for this association is that alcohol consumption may lower judgment and decision-making capacities, leading to risky sexual behavior and unintended pregnancies. 37 In addition, women who use alcohol may also be more likely to have other risk behaviors or socioeconomic disadvantages that contribute to their use of alcohol and their decision to have an induced abortion.
Strengths and limitations of the study
This case-control study has several notable strengths that increase the reliability and validity of its findings. First, the sample size was relatively sufficient to give weight to the population represented and to strengthen the generalizability of the results. This is further enhanced by a remarkably high response rate, which adds to the robustness of the study with minimal selection bias. In the current study, the problem of establishing temporal relationships between risk factors and outcomes was reduced because incident cases were used. In addition, the random selection of both cases and controls from the same health facilities and the random selection of the facilities themselves strengthen the validity of this study and reduce potential confounding.
Despite these strengths, several limitations in the current study must be considered when interpreting its results. The institution-based public health facility case-control design might not have included cases from the general community; hence, it may affect the generalizability of the findings. Induced abortion is a sensitive topic, and thus, there may be social desirability bias, control selection: respondents may not like to report certain factors of influence due to associated stigma or the fear of being judged. This may be the reason for the underestimation of true risk factors. In addition, some questions depend on the recall of participants about events in the past, introducing the potential for recall bias that may affect the accuracy of the reported information. Furthermore, the current study did not collect data on whether the induced abortion was performed using a medical or surgical procedure. So, researchers recommended future research to explore the detailed reasons. Moreover, there is no measurement available in this study to gauge whether an abortion can be deemed safe or unsafe.
Public health implications
The recent study was focused on identifying the risk factors associated with induced abortion among women attending health facilities in Hawassa city, Sidama Region, southern Ethiopia. Thus, our findings figure out pertinent associated factors with induced abortion. These findings have several public health implications, including increasing contraceptive counseling frequency, extending access to comprehensive sexual and reproductive health education for adolescents, and implementing interventions to reduce harmful alcohol use, which might have more than a marginal impact on risk. Indeed, the current study reported associations and not causations. So, longitudinal and intervention studies are needed to elucidate the causal pathways and may inform the development of effective evidence-based policies and programs for reducing induced abortion.
Conclusion
This case-control study identified peculiar risk factors of induced abortion among women attending public health facilities in Hawassa city. The findings revealed that induced abortion is significantly influenced by multiple interrelated factors, including educational status, early sexual debut, previous abortion history, contraceptive knowledge, contraceptive use patterns, and alcohol consumption. These findings underscore the complex interplay between sociodemographic, behavioral, and healthcare-related factors in determining the likelihood of induced abortion. This study highlights significant gaps in reproductive health education, contraceptive awareness, and behavioral risk factors that need to be addressed through comprehensive interventions.
Supplemental Material
sj-doc-2-reh-10.1177_26334941251409056 – Supplemental material for Risk factors associated with induced abortion among women attending public health facilities in Hawassa city, Sidama Region, Ethiopia: a case-control study
Supplemental material, sj-doc-2-reh-10.1177_26334941251409056 for Risk factors associated with induced abortion among women attending public health facilities in Hawassa city, Sidama Region, Ethiopia: a case-control study by Tsegaye Alemu and Christina Neway in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-1-reh-10.1177_26334941251409056 – Supplemental material for Risk factors associated with induced abortion among women attending public health facilities in Hawassa city, Sidama Region, Ethiopia: a case-control study
Supplemental material, sj-docx-1-reh-10.1177_26334941251409056 for Risk factors associated with induced abortion among women attending public health facilities in Hawassa city, Sidama Region, Ethiopia: a case-control study by Tsegaye Alemu and Christina Neway in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We would like to express our gratitude to Yanet-Liyana College, School of Graduate Studies, for providing the ethical letter. We would also like to extend our special thanks to the Hawassa City Administration Health Office, the selected health facilities, and their staff for their cooperation and assistance during the data collection process. Our sincere appreciation goes to the dedicated data collectors and supervisor for their tireless efforts in ensuring the success of the data collection phase. Finally, we would like to offer our heartfelt thanks to the study participants for their willingness to share essential information, which was critical to the success of this research.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.