
Abstract
Background:
Adolescents in sub-Saharan Africa shoulder a disproportionate burden of sexually transmitted infections (STIs), yet data for pregnant teenagers in these settings are sparse.
Objectives:
The study estimated the prevalence of STI seropositivity and its associated factors, among pregnant adolescents at Mbarara Regional Referral Hospital (MRRH), Uganda.
Design:
Hospital-based cross-sectional study.
Methods:
Consecutive pregnant adolescents (10–19 years) attending the MRRH antenatal clinic or maternity ward between 1 July and 30 September 2024 were enrolled. A structured questionnaire captured socio-demographic, sexual-behavioural, obstetric, clinical and nutritional variables. Blood samples were tested for HIV (Determine™/STAT-PAK™), syphilis (Treponema pallidum haemagglutination assay) and Hepatitis B (HBsAg rapid test). The composite STI outcome was seropositivity for any infection: HIV, syphilis or HBsAg. Independent associations were examined with Firth-penalised logistic regression; adjusted odds ratios (aOR) and 95% confidence intervals (CI) are reported.
Results:
Among 249 participants (median age 18 years, interquartile range 18–19), the overall prevalence of STI seropositivity was 12.1% (95% CI: 8.3–16.8). Prevalence by each STI was HIV 8.8%, syphilis 4.0% and HBV 0.4%. Multigravidae had higher odds of infection than primigravidae (aOR: 2.81, 95% CI: 1.01–7.84). Having ever used a non-barrier modern contraception tripled the odds of STI (aOR 3.04, 95% CI: 1.10–8.45), whereas marriage or cohabitation reduced risk by 63% (aOR 0.37, 95% CI: 0.14–0.96).
Conclusion:
Nearly one in eight pregnant adolescents at MRRH were infected with HIV, syphilis or HBV, with these STIs more likely to be among multigravidae and former users of non-barrier contraception and less likely among married/cohabiting pregnant adolescents. These findings support integrating repeat HIV–syphilis testing, dual-method contraceptive counselling and targeted interventions for multigravidae into youth-friendly antenatal services to advance STI-elimination goals.
Plain language summary
Pregnancy is a big step for any girl, and it can be harder if she carries a hidden sexually transmitted infection (STI), an infection that she may not see or feel. These hidden STIs: human immunodeficiency virus (HIV), syphilis and hepatitis B, can harm both mother and baby if they are not found and treated. From July to September 2024, we worked at Mbarara Regional Referral Hospital in south-western Uganda and obtained special information and small blood samples from 249 pregnant girls aged 10 to 19 years. We discovered that 30 of them (about one in every eight) had at least one infection: 22 had HIV, 10 had syphilis and one had hepatitis B. The likelihood of having these STIs was higher in girls who had been pregnant before compared to those who were pregnant for the first time. Girls who had ever used family-planning pills, injections or implants, methods that prevent pregnancy but do not block germs, also showed a three-times greater likelihood, possibly because condom use stopped after they changed to these methods. By contrast, girls who were married or living with one steady partner were less likely to be infected. In Uganda, most health centres test for HIV and syphilis only once, early in pregnancy, so new infections that appear later can be missed. Our findings recommend giving a second test later in pregnancy, teaching all girls to use condoms together with other family-planning methods, and paying special attention to adolescents who have been pregnant before. Finding and treating these hidden infections early will help teenage mothers deliver healthier babies and keep themselves safe for the future.
Introduction
Sexually transmitted infections (STIs) are infections predominantly spread through sexual contact, including vaginal, anal and oral sex, and may be transmitted through mother-to-child transmission during pregnancy and childbirth. 1 STIs remain an unfinished agenda for global sexual and reproductive health.2–4 Worldwide, pooled prevalence estimates among pregnant women were about 3% for human immunodeficiency virus (HIV), 5% for syphilis, and 1% for hepatitis B, climbing two-fold to four-fold in low-income countries. 5 Adolescent girls and young women (AGYW) shoulder a big share of this burden: hepatitis B/HIV co-infection is almost seven-fold higher in 15- to 24-year-olds than in older mothers, 6 and AGYW in sub-Saharan Africa contributed to 63% of all new HIV infections in 2021. 7 Local Ugandan data mirror these global patterns: the 2020–2021 Uganda Population-based HIV Impact Assessment (UPHIA) recorded a HIV prevalence of 1.7% among adolescent girls aged 15–19 years, 8 syphilis affects 5.9% of pregnant women in Kampala 9 and 3.1% of pregnant women at Mbarara Regional Referral Hospital (MRRH) were seropositive for hepatitis B surface antigen (HBsAg). 10 Nearly 25% of girls aged 15–19 years in Uganda are already childbearing, with adolescent pregnancies contributing disproportionately to adverse pregnancy outcomes11,12
The biological interplay of the STIs further intensifies risk. Syphilitic ulcers and immune activation ease HIV entry; a Zambia-Tanzania study showed that syphilis more than doubled HIV-acquisition risk and accelerated disease progression. 13 Maternal HBV viraemia drives vertical transmission risk as one-third of infants become infected without any maternal prophylaxis, over 80% when the maternal viral load exceeds 2 × 105 IUmL−¹; routine newborn vaccination plus hepatitis-B immunoglobulin trims this risk to 16%, and adding third-trimester antivirals drives the risk to <1%.14,15 Untreated maternal syphilis increases foetal loss or stillbirth by 21%, newborn death by 9% and preterm or low-birth-weight births by 6%. 16 Taken together, the combined presence of these infections magnifies obstetric risk yet remains under-recognised in routine antenatal care.17–19 HIV infection in pregnancy increases the risk of vertical transmission, preterm birth, low birth weight and maternal morbidity, particularly when viral suppression is not achieved. 20 Without antiretroviral prophylaxis, the vertical transmission rate ranges from 15% to 45%, which can be reduced to below 5% with optimal maternal treatment and infant prophylaxis. 21 Although this study did not assess vertical transmission, its inclusion here underscores the broader public health relevance of HIV during pregnancy.
Risk factors for STI acquisition in pregnant adolescents operate at behavioural, structural and biological levels. Behavioural risk factors such as having more than one lifetime sexual partner, a history of prior STI, substance use and being unmarried or not cohabiting have all been associated with increased likelihood of acquiring an STI in pregnancy.22–24 In Uganda, fewer than 20% AGYW use condoms consistently, and out-of-school AGYW are more likely to have multiple partners, amplifying exposure to HIV, syphilis and other STIs. 25 Structurally, late antenatal booking among adolescent mothers tracks with low decision-making autonomy, poor danger-sign awareness, long travel and poverty. 26 Biologically, the immature cervical epithelium in adolescents displays higher pro-inflammatory cytokine levels, suggesting increased mucosal susceptibility to pathogens compared with adults. 27
Despite these insights, critical knowledge gaps persist. Most studies aggregate adolescents with older women, focus on single pathogens or derive from urban or non-Ugandan settings, leaving little age-specific evidence on the combined burden and determinants of HIV, syphilis and hepatitis B in pregnant adolescents, particularly in rural south-western Uganda. Accordingly, this study aimed to determine the prevalence and associated factors for STI seropositivity among adolescent pregnant women at MRRH in south-western Uganda.
Materials and methods
Study design and setting
A hospital-based cross-sectional study was conducted from 1 July to 30 September 2024 in the antenatal clinic and maternity ward of MRRH, a 600-bed teaching hospital for Mbarara University of Science and Technology in southwestern Uganda. MRRH performs ≈ 11,000 deliveries annually, of which ~10 % involve adolescents. This manuscript was prepared in line with the STOBE guidelines for cross-sectional studies (Supplemental Material). 28
Participants and recruitment
Inclusion criteria: We enrolled adolescents who met all of the following: (i) pregnant and aged 10–19 years at presentation and (ii) presented to MRRH for antenatal care, admission for delivery or management of miscarriage and medical termination of pregnancy during the study period. We included those receiving post-abortion care because miscarriage and medical termination represent part of the pregnancy continuum among adolescents and are routinely managed within the same maternity service, thereby minimising potential selection bias that could have arisen from excluding these groups. Exclusion criteria were the inability to verify date of birth (no national ID and no recall). We defined adolescents as 10–19 years, consistent with World Health Organisation and the Uganda Demographic and Health Survey (UDHS) standards used in national surveys. 12 Eligible women were enrolled by consecutive sampling until the target sample size was reached, as this method was the most feasible approach to ensure adequate recruitment within the study period given the relatively small and hard-to-reach population.29,30
Sample size
The sample size was estimated using the formula for comparing two proportions: n = [(Zα/2√(2P(1 − 2)) + Zβ√(P1(1 − P1) + P2(1 − P2))]2/(P1 – P2)2 where P = (P1 + P2)/2, Zα/2 = 1.96 (two-sided α = 0.05), and Zβ = 0.84 (power = 80%). Given a prior STI prevalence of 11.8 % among married women (P1) 24 and an assumed STI prevalence of 26.5% among unmarried women, with 80% power and a two-sided α = 0.05. This yielded 224 participants, inflated by 10% for non-response to obtain 253. Although a conservative prevalence of 50% would yield the largest sample size, we used the 11.8% estimate as the most comparable regional data available and to maintain feasibility within the three-month recruitment window (Table S1, Supplemental Material).
Data collection procedures
Two trained diploma-level midwife-research assistants administered a structured questionnaire (socio-demographics, sexual-behavioural and obstetric characteristics). Venous blood (3 mL, EDTA tube) was collected and transported at room temperature to the MRRH International Organization for Standardization-certified laboratory. Laboratory assays included the following: HIV – Alere Determine™ and HIV 1/2 STAT-PAK™ rapid tests (serial algorithm), Syphilis – Treponema pallidum haemagglutination assay (TPHA) and Hepatitis B – Hepatitis B surface antigen (HBsAg) rapid test (SD-Bioline™). Syphilis – TPHA test indicates lifetime exposure and cannot differentiate previously treated syphilis from active infection. Laboratory assays were performed by trained laboratory technologists who were blinded to participants’ questionnaire responses to minimise bias. All assays followed the manufacturer’s instructions and internal quality-control checks. We collected additional antenatal care (ANC) clinical/nutritional measures (urinary tract infection, hypertension, anaemia, mid-upper arm circumference and random blood glucose) that we do not report or analyse in this manuscript, as they belong to a separately prespecified secondary analysis; this avoids hypothesis multiplicity within the current aims.
Variables
The primary outcome was STI seropositivity, defined as a positive STAT-Pak test (or prior HIV diagnosis), HBsAg or TPHA, three infections integrated into the ANC testing package at MRRH. Other STIs such as gonorrhoea, chlamydia, Hepatitis C, Trichomonas, HSV-2 or HPV were not included as they are currently not part of ANC standard of care in Uganda. 31 Our outcome definition was based on current serological positivity (HIV, syphilis or HBsAg) at enrolment, regardless of acquisition route. Prior STI treatment was not ascertained, apart from recording known prior HIV diagnosis, because verification from records was inconsistent, and self-reported information was prone to recall bias.
Independent variables were defined a priori from questionnaire responses and bedside measurements and were recoded to minimise sparse cells. Socio-demographic covariates comprised age (13–17 vs 18–19 years), marital status (single/divorced vs married/cohabiting), residence (rural versus urban), highest education (primary or less vs secondary/tertiary), employment status (unemployed/dependent versus working) and self-reported monthly income (low, middle or high tertile). Sexual-behavioural indicators included age at sexual debut (<18 vs ⩾18 years), lifetime number of sexual partners (one vs ⩾ two), partner concurrency (none vs ⩾ one), knowledge or prior use of HIV pre-exposure prophylaxis (PrEP; yes/no), history of transactional sex (ever/never) and ever use of modern contraception (yes/no). Ever use of modern contraception was determined through asking participants whether they had ever used any modern contraceptive method, including oral pills, injectables, implants and intrauterine devices, excluding condoms. Information on duration of use and adherence patterns (typical vs consistent use) for the contraceptives was not collected. Obstetric factors were gravidity (primigravida versus multigravida), gestational-age category at interview (< 37 vs ⩾ 37 completed weeks), number of ANC visits (< 4 vs ⩾ 4), trimester of first ANC booking (first versus later) and pregnancy intendedness (planned vs unplanned). The continuous forms of age, monthly income, gestational age and laboratory values were retained for descriptive statistics; dichotomised or ordinal forms were entered into multivariable models to minimise sparse cells. The number of ANC visits (<4 vs ⩾4) referred to the number of visits completed by the time of data collection, not those planned for the entire pregnancy. The monthly income was self-reported in Uganda shillings (UGX) and classified into tertiles based on the empirical distribution of our sample (low < 20,000; middle 20,000–<50,000 and high ⩾50,000). These cut-points are sample-specific quantiles used to rank participants relative to one another, analogous in principle to the UDHS wealth-index quintiles, which also capture relative socio-economic status within the survey wave. 12
Statistical analysis
Data were exported from REDCap v13.6 to Stata 18 (StataCorp, College Station, TX, USA) for analysis. Categorical variables were presented as frequencies and percentages; continuous variables as means ± standard deviation (SD) or median (interquartile range, IQR). Overall and STI-specific prevalence were reported with exact 95 % confidence intervals (CI). Covariates were screened in univariable ordinary logistic regression; variables with p < 0.20 or a priori confounders advanced to multivariable modelling. Because the expected events-per-parameter ratio was < 5, multivariable modelling used Firth’s bias-reduced penalised logistic regression. 32 Two prespecified models were fitted: a six-variable core model (significant at p < 0.05 in univariable analysis) and a full model with core variables plus age group, education, occupation and age at sexual debut. Adjusted odds ratios (aOR) with profile likelihood 95 % CIs and two-sided p-values are presented. Model performance was assessed by the area under the receiver-operating characteristic curve (AUC) with 95 % CI for discrimination, and by calibration-in-the-large, calibration slope and a decile plot for observed versus predicted risk to assess calibration. Given the anticipated small number of outcome events, additional resampling procedures (e.g. bootstrapping or cross-validation) were not undertaken because they offer limited insight while inflating sampling variability in very small datasets. For sensitivity analysis, the final model was re-estimated with ordinary maximum-likelihood logistic regression; resulting aORs and CIs were compared with Firth estimates. Missing data were <3% for any variable, permitting complete-case analysis. Statistical significance was set at p < 0.05.
Results
Participants
A total of 253 pregnant adolescents were screened; 4 lacked complete serology and were excluded, leaving 249 participants for analysis (Figure 1). Missing values for explanatory variables were <3 % for any single variable.

Study flow diagram.
Socio-demographic and sexual-behavioural characteristics
Participants had a median age of 18 years (IQR 18–19) and were predominantly married or co-habiting (n = 203, 81.5%), Christian (n = 220, 88.4%), urban-dwelling (n = 135, 54.2 %), had sexual debut at 17 years or less (n = 187, 75.1%) and educated to primary level or below (n = 205, 82.3%). Fewer than one in five reported ever using a modern contraceptive, excluding condoms (n = 39, 15.7%), and only 4.8% (n = 12) were aware of or had used HIV pre-exposure prophylaxis, while 4.0% (n = 10) acknowledged previous transactional sex (Table 1).
Socio-demographic and sexual-behavioural characteristics of pregnant adolescents, overall and by sexually transmitted infection status, N = 249.

p-Values from tests: aWilcoxon rank-sum test and the rest (unmarked) from the chi-squared test.
Missing data: Monthly income tertile (5/249, 2.0%), type of marriage arrangement (1/249, 0.4%) and pregnancy partner identity (1/249, 0.4%).
Ever use of modern contraception excludes the use of condoms (information on duration of use and adherence patterns was not collected in this study).
IQR, interquartile range; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; UGX, Uganda shillings (1 United States $ = 3585 UGX as on 22 July 2025).
Obstetric characteristics
The participants were largely primigravid (n = 205, 82.3%), with a median gestational age of 38 weeks (IQR: 29–39). Almost two-thirds (n = 157, 63.1%) of the pregnant adolescents had attended ⩾4 antenatal visits, 71.5% (n = 178) booked for ANC in the first trimester, and 30.9% (n = 77) reported their pregnancy was unplanned (Table 2).
Obstetric characteristics of pregnant adolescents, overall and by STI status, N = 249.
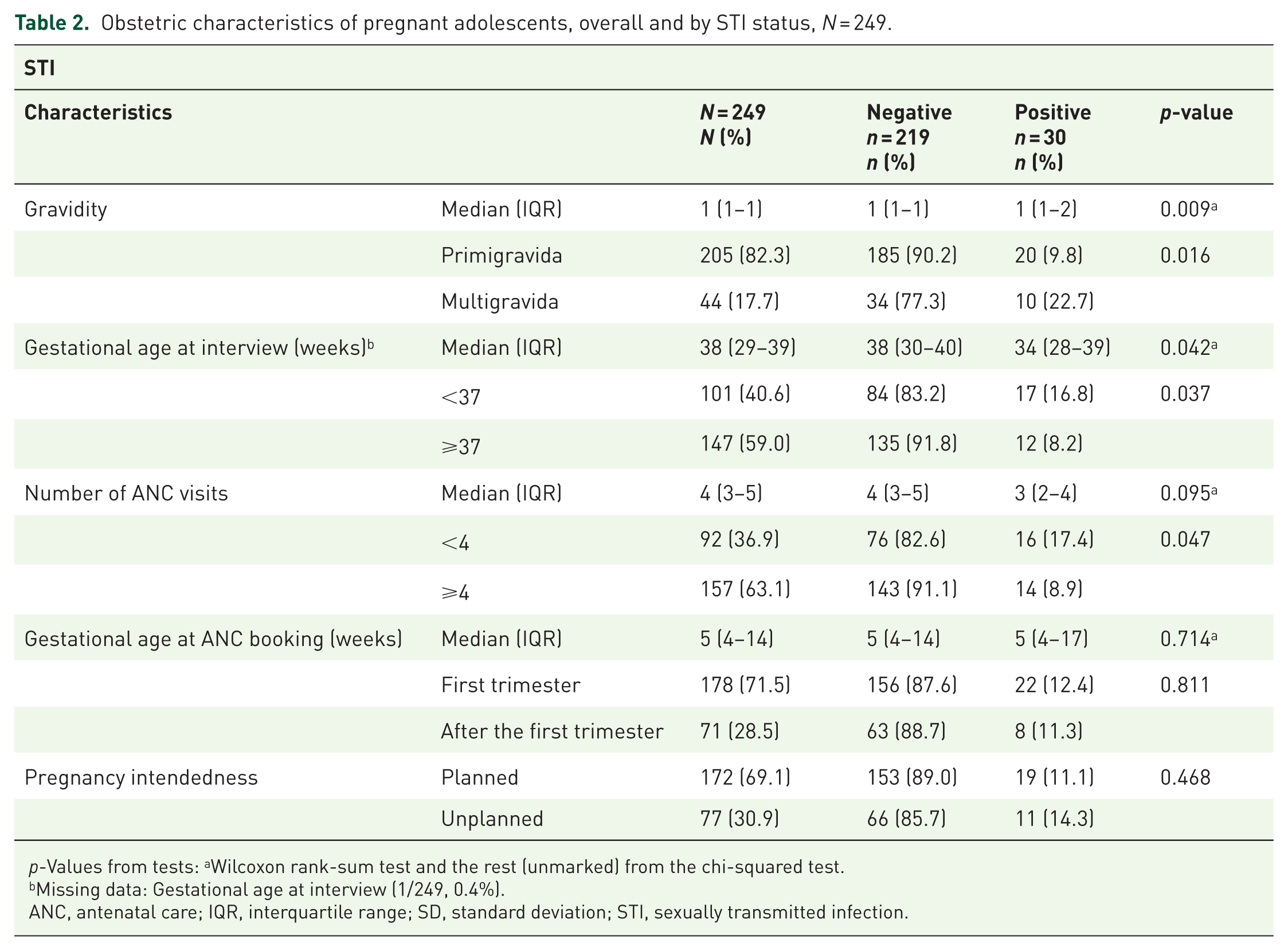
p-Values from tests: aWilcoxon rank-sum test and the rest (unmarked) from the chi-squared test.
Missing data: Gestational age at interview (1/249, 0.4%).
ANC, antenatal care; IQR, interquartile range; SD, standard deviation; STI, sexually transmitted infection.
Prevalence of STIs
The overall prevalence of STI seropositivity was 12.1% (95 % CI: 8.3%–16.8%). HIV infection was frequent (8.8%), followed by syphilis (4.0); hepatitis B prevalence was lowest (0.4%) (Table 3).
Seroprevalence of individual STI and composite STI outcome, N = 249.

CI, confidence interval; HIV, human immunodeficiency virus; STI, sexually transmitted infection.
Factors associated with STI seropositivity
On crude logistic-regression analyses, we identified higher odds of STI among pregnant adolescents who had ever used modern contraception, excluding condoms versus non-use of the modern contraceptives (OR: 4.74, 95 % CI: 2.06–10.92); knowledge or use PrEP versus lack of knowledge or non-use of PrEP (OR: 8.88, 95 % CI: 2.65–29.69); history of transactional sex versus none (OR 5.46, 95 % CI 1.45–20.63), and multigravidity versus prime gravidity (OR 2.72, 95 % CI 1.17–6.31) while participants who were married or cohabiting had lower odds of STI compared to those single or divorced (OR: 0.33, 95% CI: 0.14–0.75; Table 4).
Univariable logistic regression for factors associated with STI.

Wald test p-Values.
Ever use of modern contraception excludes the use of condoms.
ANC, antenatal care; CI, confidence interval; OR, odds ratio; PrEP, pre-exposure prophylaxis; UGX, Uganda shillings (1 United States $ = 3585 UGX as on 22 July 2025).
In the Firth-penalised multivariable model adjusting for marital status, contraceptive use, PrEP knowledge/use, gravidity, gestational age and transactional sex, three variables retained independent associations with STI. Being married or co-habiting was protective (adjusted OR: 0.37, 95 % CI: 0.14–0.96; p = 0.040), whereas ever use of modern contraception, excluding condoms (aOR: 3.04, 95 % CI: 1.10–8.45; p = 0.033) and multigravidity (aOR: 2.81, 95 % CI: 1.01–7.84; p = 0.048) were associated with increased odds of STI (Table 5).
Adjusted odds ratios from Firth-penalised logistic regression models.
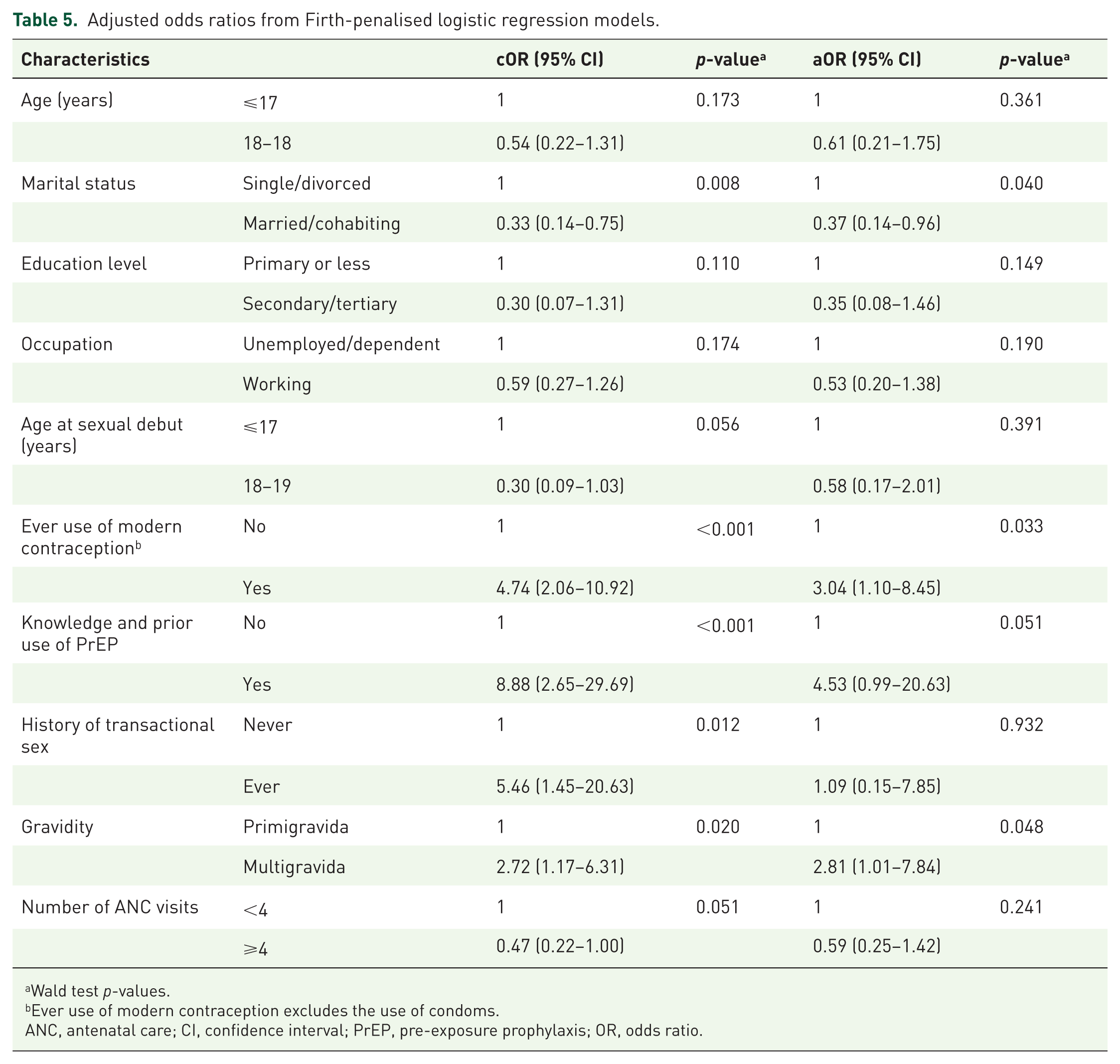
Wald test p-values.
Ever use of modern contraception excludes the use of condoms.
ANC, antenatal care; CI, confidence interval; PrEP, pre-exposure prophylaxis; OR, odds ratio.
Model performance
The final model showed good discrimination with an apparent area under the receiver-operating-characteristic (AUC) of 0.79 (95 % CI 0.70–0.88) (Figure S1, Supplemental Material). Calibration was acceptable: the calibration-in-the-large was 0, the calibration slope of 0.90 and observed proportions in each decile of the predicted probability closely followed the 45-degree reference line (Figure S2, Supplemental Material).
Sensitivity analysis
Re-fitting the final model with ordinary maximum-likelihood logistic regression produced odds ratios that differed by <10% from the Firth estimates (Table S2, Supplemental Material). Confidence intervals were slightly wider, and only the association with knowledge or prior use of PrEP crossed the 0.05 significance threshold. Because penalised likelihood yields bias-reduced coefficients and more stable standard errors in low events-per-parameter settings, the Firth model was retained as our primary analysis.
Discussion
Key results
In this hospital-based study of 249 pregnant adolescents, nearly one in eight was seropositive for any of the STIs, with HIV (8.8%), syphilis (4.0%) and hepatitis B (0.4%). Factors independently associated with STI seropositivity were ever use of modern contraception (excluding condoms) and multigravidity, while marriage/cohabitation reduced the odds of STI seropositivity by nearly two-thirds.
Comparison with other studies
Our composite prevalence of STIs is similar to those of prior studies in northwestern Ethiopia (15.2%) 33 and southern Ethiopia (14.6%) 24 but lower in a South African study (32%), reflecting the geographical burden in the different individual STIs included in each study. The individual STI prevalence exceed the pooled global estimates for pregnant women (HIV ≈ 3%, syphilis ≈ 5%, HBV ≈ 1%) reported in a 2023 meta-analysis, 5 underscoring the disproportionate burden borne by adolescents in low-income settings. The prevalence of syphilis (4%) is almost identical to the 5.9% observed among adult antenatal attendees in Kampala, 9 but the adolescent HIV prevalence (8.8%) is five-fold higher than the 1.7% recorded in the 2020–2021 UPHIA statistics for girls aged 15–19 years. 8 The hepatitis B prevalence in our study is markedly lower than the 3.1% HBsAg prevalence previously documented at the same hospital, 10 perhaps reflecting successful infant vaccination since 2002.
The factors associated with STI seropositivity are consistent with those described previously. Being unmarried/not cohabiting has been associated with STI diagnosis.23,24 Positive association between ever use of non-condom modern contraceptive and STI agrees with findings from a meta-analysis that long-acting reversible contraception markedly reduces condom uptake and is linked to STI. 34 Literature rarely examines multigravidity as a determinant of STI in pregnant women. Most antenatal studies pool adolescents with older women, analyse single infections or treat gravidity merely as a demographic descriptor without entering it into multivariable models. Consequently, our finding that multigravidity independently increased the odds of STI is among the first to fill this evidence gap. It is important to note that comparator findings come from mixed-age studies, so our study is among the first to study STIs among pregnant adolescents.
Interpretation and public-health implications
The high HIV and syphilis prevalence in these pregnant adolescents suggests that pregnancy alone does not confer protection from sexual exposure and that current goal oriented antenatal packages, which may screen once for syphilis and HIV, may miss incident infections acquired later in gestation. 19 Ever use of hormonal contraception likely reflects earlier attempts at fertility control; once pregnant, condom negotiation power may further diminish, perpetuating exposure. Multigravidity signals repeated unprotected intercourse and possibly previous gaps in postpartum STI prevention.
Collectively, these findings support three programmatic priorities: Integrated re-testing, repeat HIV–syphilis dual testing every 3 months for all adolescents, with point-of-care treatment or antiretroviral optimisation 31 ; enhanced counselling, emphasising dual-method contraception and partner testing for multigravidae and contraceptive users; and youth-friendly antenatal platforms, combining biomedical services with empowerment interventions that address relationship power dynamics and school re-enrolment.
Strengths and limitations
Strengths include age-specific focus, simultaneous assessment of three high-impact pathogens, quality-assured laboratory algorithms and use of Firth-penalised logistic regression to minimise small-sample bias. Limitations are inherent to the cross-sectional design (temporal ambiguity), single-centre sampling, which may under-represent peri-urban or non-attending adolescents, and limited power for rare outcomes such as hepatitis B. Behavioural variables were self-reported and subject to social-desirability bias, although confidential interviews and adolescent counsellors mitigated this risk. Additionally, there is a potential seasonal variation in the STI prevalence given the 3-month recruitment period. The definition of ‘ever’ use of contraception did not capture duration or adherence, which may influence associations with STI risk. Also, we did not capture data on prior STI diagnosis or treatment history beyond HIV, which limited our ability to distinguish between new and recurrent infections. Finally, reliance on a prevalence estimate from Ethiopia for sample size determination may limit regional generalisability, although it balanced statistical power with feasibility in the given study context.
Generalisability
Our study comprised consecutive pregnant adolescents attending antenatal or delivery care at Mbarara Regional Referral Hospital, a public tertiary unit serving 10 districts where > 80% of births occur in facilities. 12 Consequently, estimates should apply to pregnant adolescents who reach public maternity services in rural and peri-urban south-western Uganda. Similar HIV/syphilis prevalence reported in Kampala and other East-African antenatal studies suggest broader relevance to high-burden settings.9,24 Nonetheless, out-of-facility adolescents, primary-care sites without referral bias, and regions with markedly different pathogen epidemiology or screening policies were not sampled. In addition, reliance on a prevalence estimate from Ethiopia for sample size determination may constrain broader extrapolation. Finally, the 3-month recruitment window may have missed seasonal variation, further limiting generalisability. Results should therefore be generalised confidently to facility-attending pregnant adolescents in comparable East-African contexts but extrapolated with caution elsewhere.
Conclusion
Pregnancy does not insulate Ugandan adolescents from a syndemic of HIV and syphilis; nearly one in eight enter pregnant adolescent maternity wards infected, and modifiable behavioural and reproductive factors compound risk. Scaling up repeat integrated screening, reinforcing dual-method counselling, and targeting multigravidae could accelerate progress towards the World Health Organization 2030 elimination goals. Future studies should extend recruitment periods to capture seasonal variation, incorporate additional STIs such as gonorrhoea and chlamydia into testing panels, and better characterise contraceptive use patterns and prior STI treatment histories. Although vertical transmission was not assessed in the present study, it remains an important gap; such prospective approaches would allow evaluation of incident infections, vertical transmission and the effectiveness of adolescent-tailored interventions on maternal–neonatal outcomes.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251403816 – Supplemental material for Prevalence and associated factors of sexually transmitted infections among adolescent pregnant women at Mbarara Regional Referral Hospital, Uganda
Supplemental material, sj-docx-1-reh-10.1177_26334941251403816 for Prevalence and associated factors of sexually transmitted infections among adolescent pregnant women at Mbarara Regional Referral Hospital, Uganda by Henry Ochola, Onesmus Byamukama, Charles Tushabomwe-Kazooba, Annah Amwikirize, Anorld Kamugisha, Moses Ntaro and Joseph Ngonzi in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941251403816 – Supplemental material for Prevalence and associated factors of sexually transmitted infections among adolescent pregnant women at Mbarara Regional Referral Hospital, Uganda
Supplemental material, sj-docx-2-reh-10.1177_26334941251403816 for Prevalence and associated factors of sexually transmitted infections among adolescent pregnant women at Mbarara Regional Referral Hospital, Uganda by Henry Ochola, Onesmus Byamukama, Charles Tushabomwe-Kazooba, Annah Amwikirize, Anorld Kamugisha, Moses Ntaro and Joseph Ngonzi in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We sincerely appreciate the unwavering assistance provided by the entire staff of the Department of Obstetrics and Gynaecology, Mbarara University of Science and Technology, and by the management of Mbarara Regional Referral Hospital throughout the study. Special thanks go to Sr Kyasiimire Daphine and Sr Akampwera Racheal for their diligent data collection, and to all the women who generously agreed to take part in this research.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.