
Abstract
Background:
Infertility affects around 17.5% of reproductive-aged individuals worldwide, posing significant personal and public health challenges. Although Medically Assisted Reproduction and Assisted Reproductive Technology (ART; e.g., in vitro fertilization) have advanced outcomes, many couples fail to conceive due to unaddressed pelvic, uterine, or systemic factors.
Objectives:
We aim to (1) define the current usage of Restorative Reproduction Medicine (RRM) in clinical practice, (2) compare RRM outcomes with conventional ART, and (3) propose an integrated model of RRM plus ART for optimal fertility care.
Design:
A systematic review following PRISMA guidelines was conducted (INPLASY registration no. INPLASY2024110069).
Data sources and methods:
We searched PubMed, Scopus, and Web of Science (January 1995–October 2024), combining terms such as “restorative reproductive medicine,” “intrauterine adhesions,” “myomas,” “polyps,” “hydrosalpinx,” “endometritis,” “BMI,” “thyroid dysfunction,” “microbiome,” and “assisted reproductive technology.” Inclusion criteria: studies on uterine/systemic factors affecting infertility, focusing on surgical/pharmacological RRM interventions and ART limitations. Exclusion criteria: male-only infertility, case reports, narrative reviews, non-English publications. Quality assessment employed the Newcastle-Ottawa Scale and the Cochrane Risk of Bias Tool. We also briefly noted potential publication bias due to language and study-type restrictions.
Results:
From >25,000 initial titles, 3 sequential screenings yielded 145 key articles addressing uterine (septum, myomas, polyps, adhesions) and systemic (body mass index (BMI) extremes, thyroid dysfunction, microbiome imbalance) factors. Surgical corrections (e.g., hysteroscopic removal of polyps/myomas, salpingectomy for hydrosalpinx) significantly improved natural conception and ART success (⩾20%–40% increase in clinical pregnancy). Chronic endometritis treatment, endometrial microbiome modulation, and BMI/thyroid optimization further improved pregnancy rates by 15%–20%. Comparisons of RRM versus ART alone indicated that RRM often lowers overall cost and may reduce miscarriage, while ART offers immediate embryo transfer. Combining RRM to correct pathologies prior to ART can boost implantation and live birth rates (⩾40%–70% improvement in some studies).
Conclusion:
Restorative Reproductive Medicine comprehensively addresses pelvic and systemic abnormalities, thereby enhancing fertility outcomes and complementing ART. A proposed integrated model—RRM diagnostics/interventions followed by ART if needed—maximizes success, reduces time/cost, and emphasizes holistic reproductive health. Further multicenter trials are warranted to standardize protocols and fully realize RRM’s potential in modern fertility care.
Keywords
Introduction
Infertility affects 17.5% of reproductive-aged individuals worldwide, presenting a profound challenge to public health and personal well-being, 1 assisted reproductive technologies (ARTs), including in vitro fertilization (IVF), have revolutionized infertility treatment, yet significant limitations remain. Many couples fail to achieve pregnancy even with advancements like euploid embryo transfer, often due to unaddressed systemic or uterine.2,3
Definition and scope of RRM
Restorative Reproductive Medicine (RRM) focuses on diagnosing and correcting the root causes of infertility, aiming to restore natural fertility rather than bypass these factors.4 –15 In contrast, conventional Medically Assisted Reproduction and ART rely on laboratory or pharmacologic interventions (e.g., IVF) that often circumvent the underlying pathology.2,9
Current usage in practice
Although RRM is used in various clinical contexts (e.g., surgical correction of myomas/polyps, antibiotic treatment for endometritis, thyroid optimization, etc.), it remains underrepresented. Many clinics default to ART protocols without comprehensive attempts to correct uterine or systemic abnormalities. This gap may partially explain persistent implantation failures even with euploid embryo transfers. Recent data also suggest that addressing modifiable factors (e.g., obesity, subclinical hypothyroidism, microbiome dysbiosis) can yield natural conception or enhance ART outcomes.16 –23 Thus, RRM is an attractive—and sometimes more cost-effective—approach to fertility management.
Rationale for this review
Despite documented improvements in pregnancy outcomes following RRM interventions, there is limited consolidation of these findings. By systematically evaluating the literature on uterine and systemic factors, we aim to highlight the value of RRM, define its limitations, and propose integrated RRM–ART strategies.
Methods
Protocol and registration
This review was registered on the International Platform of Registered Systematic Review and Meta-Analysis Protocols (INPLASY) under registration no. INPLASY2024110069, adhering to PRISMA guidelines. 24
Search strategy
Using PubMed, Scopus, and Web of Science from January 1995 to October 2024, we combined controlled vocabulary and keywords: “restorative reproductive medicine,” “pelvic factors of sterility,” “uterine abnormalities,” “intrauterine adhesions,” “myomas,” “polyps,” “hydrosalpinx,” “endometritis,” “BMI,” “thyroid dysfunction,” “reproductive microbiome,” “assisted reproductive technology,” etc. Boolean operators refined the search for relevant abstracts in English.
Eligibility criteria
Inclusion:
I. Studies on uterine/systemic factors in infertility (e.g., fibroids, polyps, endometritis, obesity)
II. Investigations addressing or proposing RRM interventions (surgical, pharmacological, or lifestyle)
III. Observational, cohort, randomized controlled trials (RCTs), meta-analyses, and systematic reviews.
Exclusion:
I. Male-factor—only infertility, non-English papers, single case reports, narrative reviews.
Data extraction and quality assessment
Two reviewers independently extracted data (study design, population, interventions, outcomes). Quality was evaluated using the Newcastle-Ottawa Scale (observational) and the Cochrane Risk of Bias Tool (RCTs). 25 Publication bias (e.g., language bias, limited sample sizes) was acknowledged but not formally meta-analyzed.
Data synthesis
We performed a thematic synthesis, clustering articles by uterine (fibroids, polyps, adhesions, septum) versus systemic (thyroid, body mass index (BMI), microbiome, endometritis) factors, and extracted outcome metrics such as clinical pregnancy, live birth, and miscarriage rates after interventions. 25 Additional emphasis was placed on comparing RRM approaches versus standard ART. The methods used to decide which results to collect.
Within our systematic review without a meta-analysis, study selection follows rigorous inclusion/exclusion criteria and a structured appraisal of study quality. Study Selection to ensure a transparent, reproducible selection process was performed by the PICO model, helping to define the research scope:
P (Population): Define the target group (e.g., infertile women, patients with endometriosis).
I (Intervention): Specify treatments or exposures (e.g., IVF, laparoscopic surgery).
C (Comparator): Identify comparison groups (e.g., no treatment, other interventions).
(Outcome): Choose outcomes (e.g., live birth rate, miscarriage rate).
We developed inclusion and exclusion criteria. Clearly state eligibility criteria before screening: Inclusion criteria:
Study type (RCTs, observational studies, case-control, cohort)
Population characteristics
Type of intervention/exposure
Outcome measures
Publication status (peer-reviewed)
Exclusion criteria:
Studies without full text
Case reports, letters, editorials
Low sample size studies
Studies without outcome data
Screening process (PRISMA flowchart)
Title and abstract screening
Two independent reviewers screen studies based on title and abstract
Disagreements resolved by third-party adjudication.
Full-text review
Selected abstracts undergo a full-text review to confirm relevance.
Data extraction
Extract key data (authors, year, study design, sample size, interventions, outcomes).
Risk of bias (RoB) assessment for a systematic review without meta-analysis
Reporting bias → Were results selectively reported? (Supplemental Material 1).
Reporting the study selection process PRISMA flow diagram to show the number of studies used:
○ Identified
○ Screened
○ Excluded (with reasons)
○ Included
○ Final analysis
The RoB (RoB2, ROBINS-I, and/or Grade) results were reported in a narrative synthesis (Supplemental Material 1).
Results
Search outcome and PRISMA flow after an initial pool of ~25,000 studies, 3 sequential screenings (Table 1) reduced to 145 articles that met our inclusion criteria (Figure 1, Supplemental File).
Screening progress for key pelvic and uterine factors.
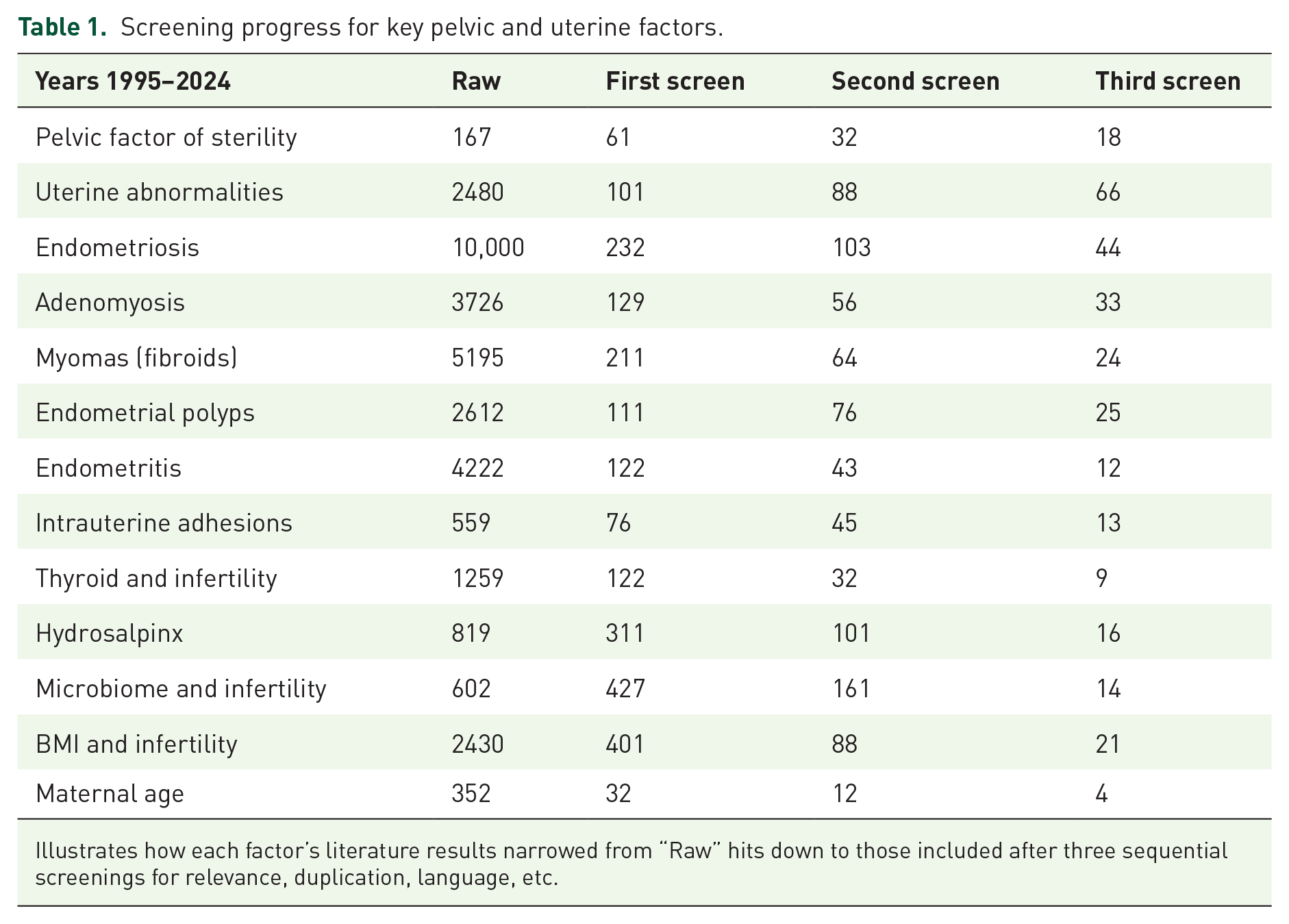
Illustrates how each factor’s literature results narrowed from “Raw” hits down to those included after three sequential screenings for relevance, duplication, language, etc.
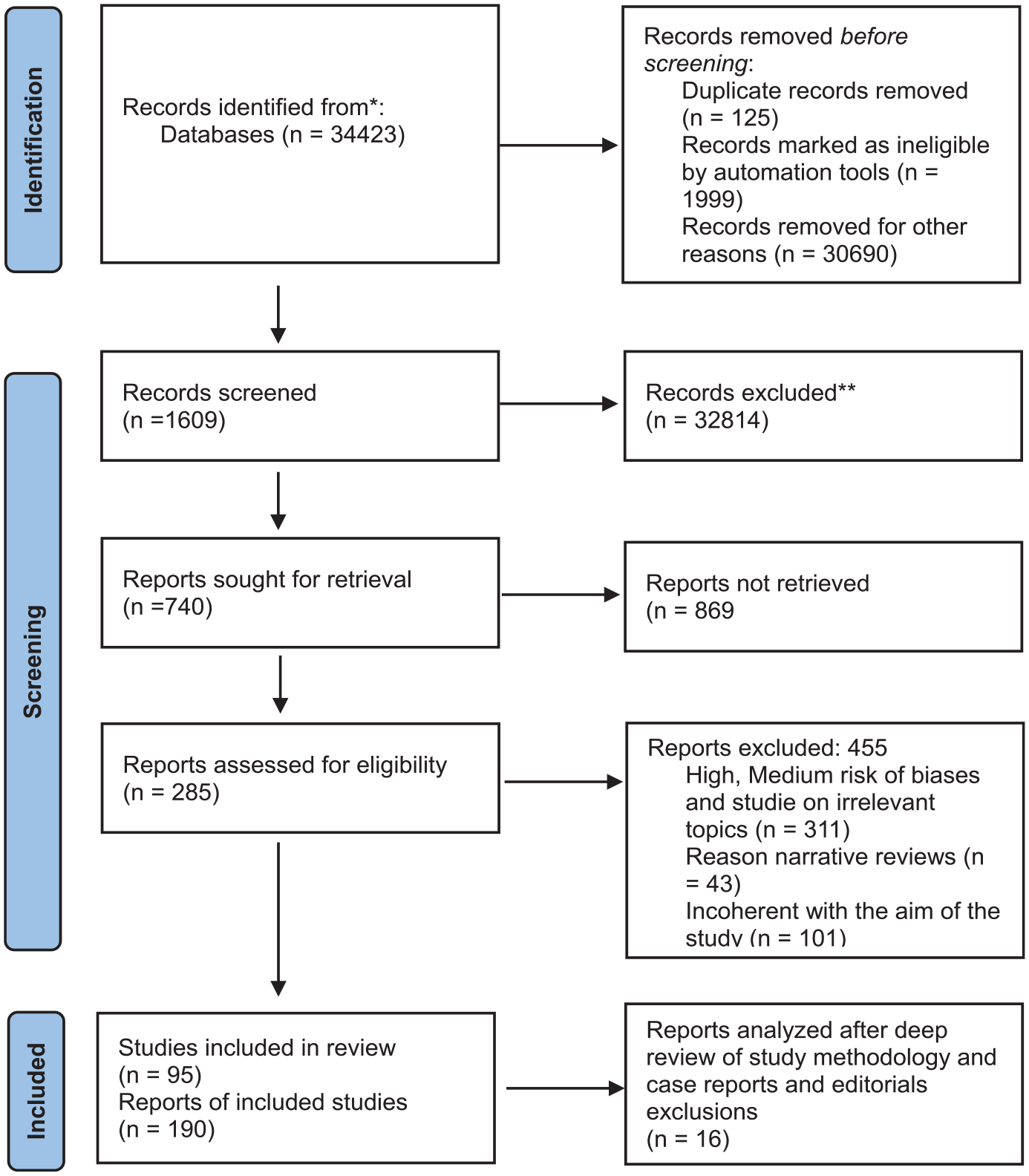
PRISMA flow diagram.
Figure 1 PRISMA graphical selection publications after selection and inclusion from literature search as methodology used (Page et al. 24 )
Pelvic and uterine abnormalities
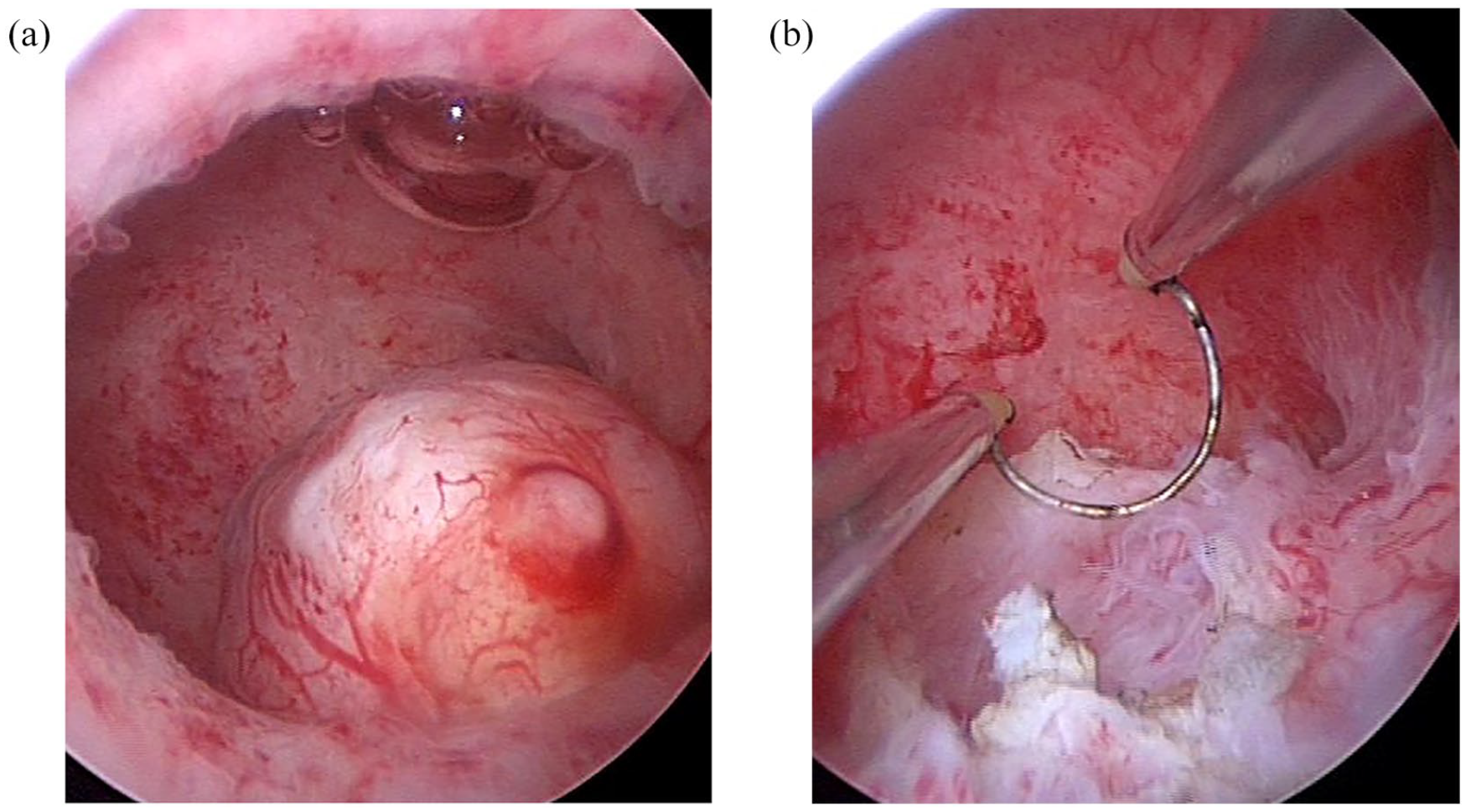
The incidence of pelvic factor infertility is often associated with conditions such as pelvic inflammatory disease (PID), endometriosis, prior pelvic surgeries, or congenital anomalies. According to the Practice Committee of the American Society for Reproductive Medicine 10 tubal damage or blockage is responsible for 35% of infertility cases in women in the United States, while pelvic adhesions contribute to an additional 15%–20%. PID, a major contributing factor, was shown in a meta-analysis by Sutton et al. 15 to increase the likelihood of tubal blockage by 33% among affected women. Endometriosis, which impacts up to 50% of infertile women, often leads to pelvic adhesions and chronic inflammation, as described by de Ziegler et al. 26 These mechanisms distort pelvic anatomy and compromise fertility potential (Figure 2; Table 2).

(a, b) Ovaries before surgical correction of pelvic adhesions. Filmic adhesions are obstacles for oocyte dehiscence even in the presence of hysterosalpingography documenting tubal patency.
Surgical interventions and outcomes for pelvic factor infertility.

The table summarizes the outcomes associated with various surgical interventions based on clinical studies. It highlights the improvement in pregnancy and live birth rates following targeted surgical corrections for pelvic factor infertility.
Intrauterine adhesions
Intrauterine adhesions (IUAs) can cause subfertility and recurrent pregnancy loss. Studies show hysteroscopic adhesiolysis improves spontaneous conception rates by 25%–60%. 7 Long-term recurrence is possible, hence second-look hysteroscopy is recommended.
Uterine septum
A septate uterus is associated with poor vascularization and high miscarriage rates (~50%). Hysteroscopic metroplasty (Table 3) can boost clinical pregnancy rates to 60%–70% and reduce miscarriage to 10%–15%.11,13
IVF outcomes in uterine septae with and without surgical removal, highlighting differences in implantation, clinical pregnancy, and miscarriage rates.

IVF, in vitro fertilization.
Myomas (fibroids)
Submucosal myomas significantly reduce implantation by distorting the cavity.5,6 Hysteroscopic myomectomy raises pregnancy rates by 50%–70%. 33 However, fibroid recurrence can approach 30%. Minimally invasive (Figure 3) or robotic approaches facilitate better outcomes, especially for type 0–1 submucosal fibroids (Tables 4 and 5).
Hysteroscopic view of submucosal myoma; labeled “before and after resection.”
Summary table for myomas (fibroids).

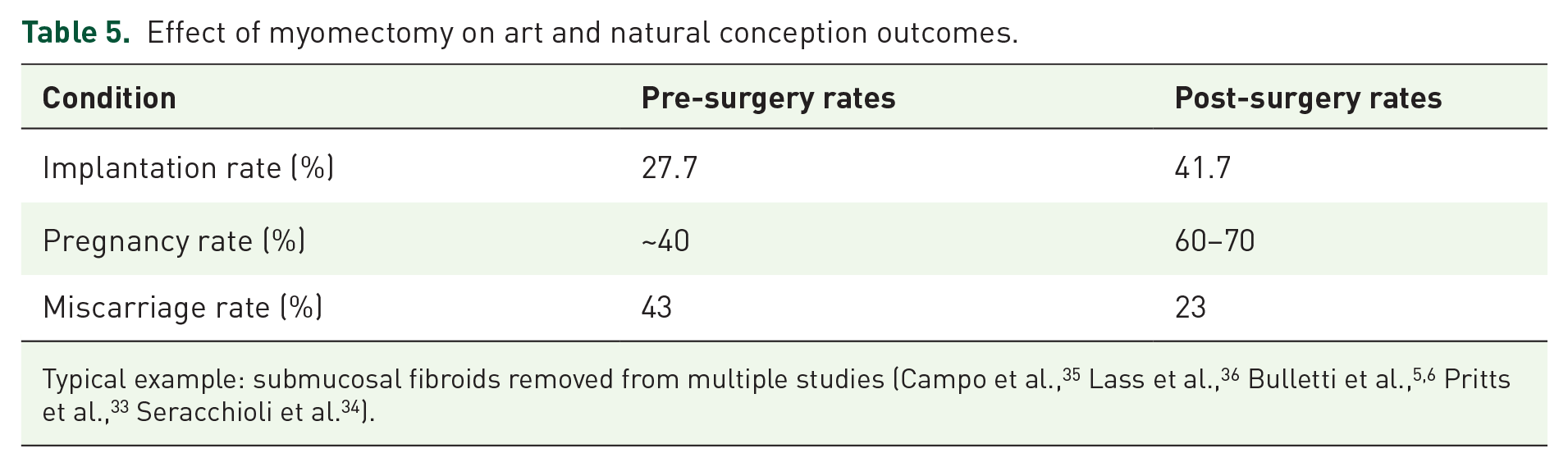
Effect of myomectomy on art and natural conception outcomes.
Endometrial polyps
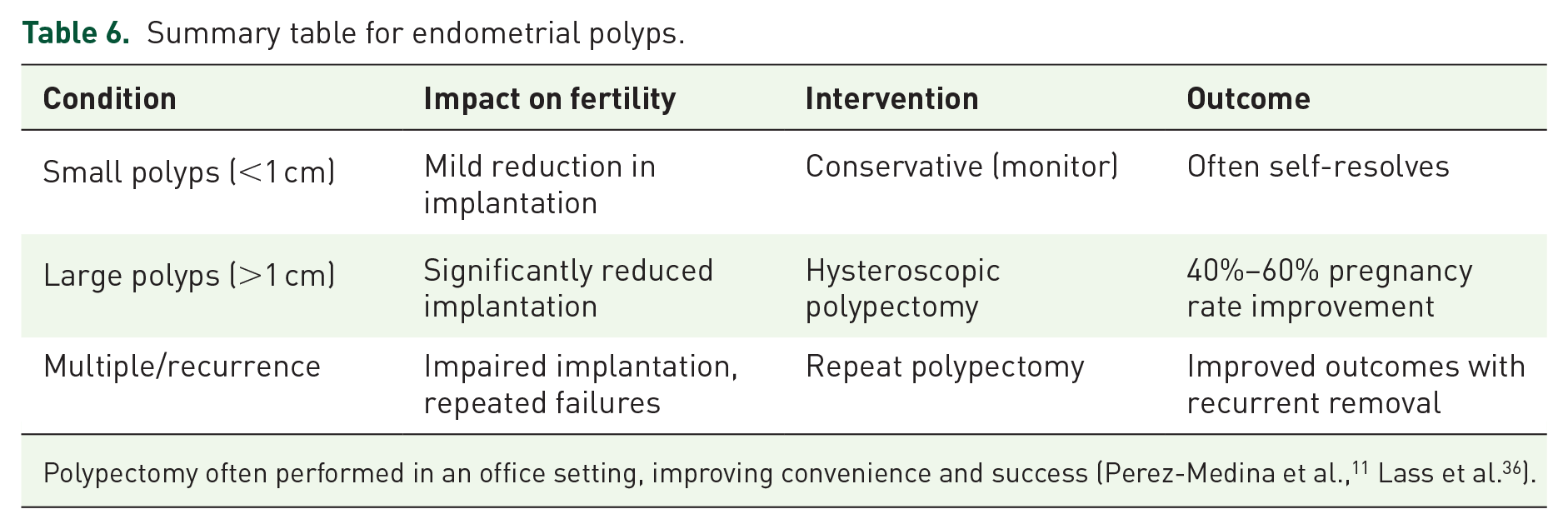
Associated with 10%–35% prevalence in infertile women.11,36 Polypectomy significantly increases pregnancy rates by ~30%–50% in natural and ART cycles (Table 6). Office hysteroscopy is cost-effective in diagnosing and removing polyps.
Summary table for endometrial polyps.
Chronic endometritis
Persistent inflammation with plasma cells in the endometrium is observed in 10%–30% of infertile women. Antibiotic therapy (e.g., doxycycline) reestablishes normal endometrial function, boosting pregnancy and lowering miscarriage rates.3,37,38
Hydrosalpinx
Untreated hydrosalpinx leaks embryotoxic fluid into the uterus, reducing implantation by over 50%. 29 Salpingectomy prior to IVF raises pregnancy rates from ~23% to 36%–40%8,39 (Figure 4).
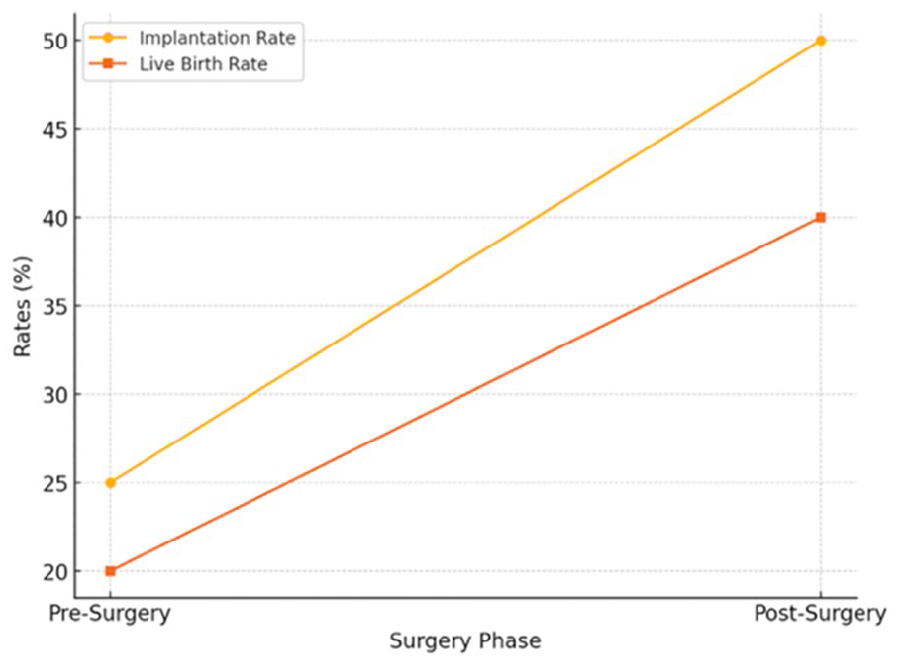
Line graph of IVF outcomes pre- and post-salpingectomy in hydrosalpinx. The line graph illustrates the impact of salpingectomy on IVF outcomes, showing pre- and post-surgery implantation and live birth rates.
Reproductive microbiome
Recent studies link non-Lactobacillus–dominated endometrial or vaginal flora to implantation failure.18,40 Although evidence is still evolving, probiotic or antibiotic regimens might restore microbial balance and improve fertility outcomes (Figure 5).

Microbiome profiles in fertile versus infertile women. This bar graph illustrates the microbiome profiles in fertile versus infertile women. It compares Lactobacillus prevalence and bacterial diversity, highlighting a higher Lactobacillus prevalence and lower bacterial diversity in fertile women, contrasting with the microbiome imbalance observed in infertile women.
Body mass index
Obesity affects endometrial gene expression and shifts the window of implantation (WOI).20,21 Weight reduction improves pregnancy rates by ~15%–20%. 1 Overweight women (BMI ⩾ 25) have significantly lower spontaneous and ART success 22 (Figure 6).
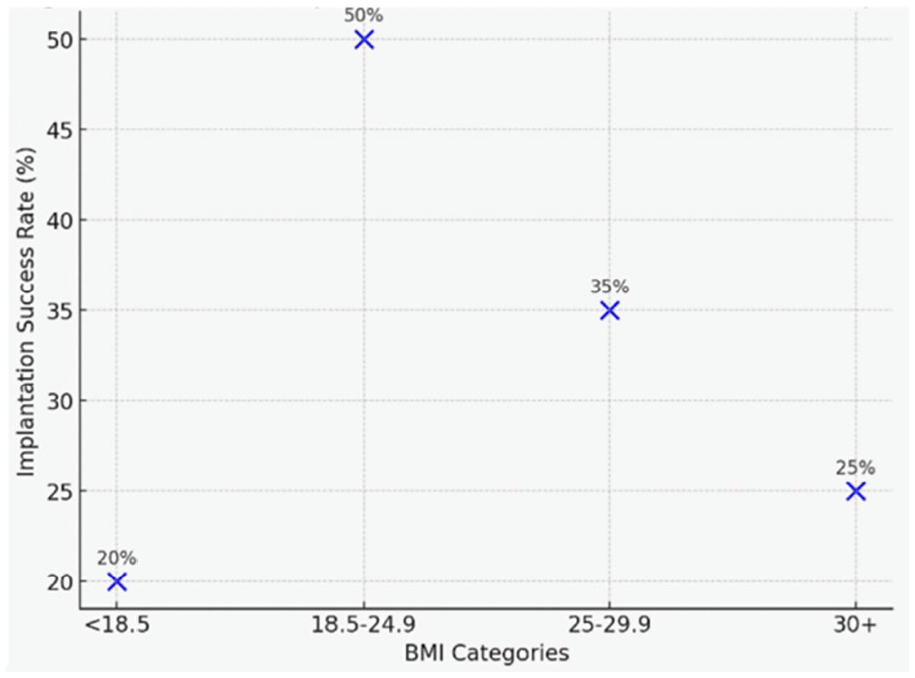
Scatter plot linking BMI categories to implantation success rates.
Thyroid dysfunction
Subclinical hypothyroidism or autoimmune thyroiditis disturbs ovulation and increases miscarriage risk. Levothyroxine therapy can restore fertility if TSH (Thyroid Stimulating Hormone) is elevated.41,42 Debate remains around euthyroid autoimmune states.
Maternal age (beyond ovarian aging)
Age correlates with diminished uterine vascularity and possible immune dysregulation. 43 This further reduces implantation, independent of oocyte quality (Figure 7). Early fertility planning or egg freezing is advised 23 (Figure 8).

Line chart: Age & BMI combined effect on fertility. Y-axis: success rate, X-axis: age brackets, multiple lines for normal versus high BMI. A line chart illustrates the effects of age and BMI on fertility success rates, comparing normal and high BMI categories of age and BMI on fertility success rates, comparing normal and high BMI categories.

Schematic: Optimal maternal starting ages for family planning. It could be a simple timeline or slope indicating recommended childbearing age with/without ART. This schematic graph illustrates the optimal maternal starting ages for family planning based on the number of children desired, with and without the inclusion of ARTs. It highlights the earlier age thresholds required for achieving family goals without ART intervention.
BMI (Figures 6 and 7) is influencing fertility success rate of women at different age groups.
Table 7 highlights the average costs and success rates of RRM, ART, and combined approaches, showcasing the balance between cost and efficacy.
Comparative success rates for RRM interventions versus ART “RRM alone” versus “ART alone” versus “Combined RRM + ART.

Cost-effectiveness of RRM, ART, and combined approaches.
ART, assisted reproductive technology; IVF, in vitro fertilization; RRM, Restorative Reproductive Medicine.
A synergy emerges when combining RRM (to correct pelvic/systemic factors) before or alongside ART, leading to cumulative live birth rates up to 40%–70%35,44 (Tables 7 and 8). Figures vary by region. RRM interventions can reduce the total ART cycles needed, increasing the overall cost-effectiveness (Figure 9). The diagnostic and therapeutic RRM options for decision making are reported in the flow chart of Figure 10.
Comparative cost-effectiveness analysis: RRM versus ART alone.

ART, assisted reproductive technology; IVF, in vitro fertilization; RRM, Restorative Reproductive Medicine.

Comparative success rates for RRM Interventions versus ART. This bar chart shows the success rates of natural conception after RRM interventions (e.g., IUAs, myomas, polyps, hydrosalpinx) compared to ART outcomes without addressing these conditions.

Diagnostic flowchart for RRM-ART integration. A flowchart outlines decision-making pathways for combining RRM with ART. Illustrated flowchart outlining the diagnostic and treatment strategies for pelvic factor infertility and uterine anomalies in reproductive medicine.
Discussion
Both endometriosis and adenomyosis play pivotal roles in pelvic factor infertility. Endometriosis is defined by ectopic implantation of endometrial-like tissue, which provokes inflammation and adhesions, whereas adenomyosis is characterized by endometrial tissue invading the myometrium, thereby reducing uterine receptivity and contractility. Evidence from Bulletti et al. 4 and Zondervan et al. 45 indicates that moderate to severe endometriosis correlates strongly with diminished fertility, frequently warranting surgical intervention to restore reproductive potential. Similarly, adenomyosis is associated with lower implantation and live birth rates, even in ARTs, as shown by Chapron et al. 28 and De Ziegler et al. 8
Surgical interventions remain central in addressing pelvic factor infertility
Procedures such as laparoscopy, salpingectomy, tuboplasty, and adhesiolysis show substantial efficacy. Laparoscopy serves both diagnostic and therapeutic roles (Figures 3 and 4; Tables 2–6). For instance, Nezhat et al. 46 found that laparoscopic excision of endometriosis yielded a 50% clinical pregnancy rate within a year of surgery, while adhesiolysis improved spontaneous pregnancy rates by 40%–60%. Salpingectomy is especially helpful in cases of hydrosalpinx, where fluid-filled fallopian tubes impair embryo implantation in IVF. In one study, Strandell et al. 39 reported an increase in IVF pregnancy rates from 23% to 42% following salpingectomy. Tuboplasty, used to repair damaged fallopian tubes, reached patency rates of 80% and pregnancy rates of 30%–50% within 2 years (Gomel et al. 47 ). Likewise, adhesiolysis raised spontaneous conception rates by 25%–60%, particularly in younger patients or those with minimal adhesions (Tulandi et al. 48 ).
Although beneficial, surgical approaches carry inherent risks—including infection, recurrence of adhesions, and potential trauma to reproductive organs. To address these challenges, combining surgery with ART and harnessing progress in microsurgical techniques, robotic surgery, and adhesion-prevention measures has proved promising. Hormonal suppression therapies for endometriosis also bolster outcomes of surgical interventions.
Uterine abnormalities
Uterine abnormalities, particularly uterine septae (Table 3), pose a major obstacle to successful implantation and pregnancy. A uterine septum, the most common congenital anomaly, occurs in 1%–3% of the general population but at higher rates among women with infertility or recurrent pregnancy loss. 49 Poor vascularization and disturbed uterine contractility caused by the septum lower implantation rates and elevate the risk of pregnancy loss. Women with untreated septae typically have implantation rates of 15%–20%, compared to 30–40% in women with normal uteri. Miscarriage rates can approach 50%. 49 However, hysteroscopic metroplasty significantly improves outcomes, increasing implantation to 35%–50%, clinical pregnancy to 60%–70%, and reducing miscarriage to 10%–15%, as shown by Pérez-Medina et al. 11 Meta-analyses by Valle and Ekpo 13 similarly confirm these improvements in both natural conception and ART cycles.
ART outcomes underscore the negative impact of uncorrected uterine anomalies. Implantation in women with such anomalies sits at 15%–25%, whereas it rises to 40%–50% in women without these issues, with live birth rates often falling below 30%. Post-surgical correction, in contrast, substantially enhances outcomes—implantation rates rise to 35%–50% and live birth rates to 50%–65%, notably after metroplasty for a septate uterus or correction of a bicornuate uterus (Table 3).
Submucosal myomas (fibroids) and endometrial polyps
Submucosal myomas (fibroids)5,6,33,50 and endometrial polyps 11 are also significant sources of uterine abnormalities that undermine fertility, largely through distorting the uterine cavity and interrupting implantation (Figure 3). These structural issues are tied to heightened miscarriage rates and diminished success in both natural conception and ART. Surgical removal—myomectomy for submucosal fibroids or polypectomy for endometrial polyps—has led to marked fertility improvements: pregnancy rates have been shown to climb by 50%–70% post-myomectomy and 40%–60% post-polypectomy, underscoring the critical importance of surgical intervention for unexplained infertility or recurrent pregnancy loss.33,35
Submucosal fibroids (Figure 3; Tables 4 and 5), present in roughly 10%–15% of infertile women, are particularly problematic because of their location adjacent to the endometrial lining. They compromise implantation through cavity distortion, chronic inflammation, and impaired uterine contractility. 33 Myomas are classified by location—submucosal, intramural, or subserosal—and submucosal variants have the most profound effect on implantation and live birth rates, especially in ART cycles. For instance, untreated submucosal fibroids may reduce IVF pregnancy rates from 41.7% to 27.7%.35,51 Hysteroscopic myomectomy effectively reverses these mechanical and inflammatory barriers.5,6,34,52 Hysteroscopic myomectomy is now considered the gold standard for submucosal fibroids in infertile women,34,53 boosting both natural and ART outcomes, with pregnancy rates of 50%–70% after surgery. Live birth rates also rise notably, particularly for women under 35 years of age.35,53,54 Key success factors include myoma size, classification (type 0 or 1), and patient age. Nevertheless, recurrence happens in up to 30% of cases, calling for long-term follow-up. 54
Endometrial polyps
Endometrial polyps, benign intrauterine growths, similarly hamper fertility. Their prevalence among reproductive-age women is 10%–35%, and they degrade the endometrial environment by lowering receptivity, prompting local inflammation, and impeding sperm or embryo transit. 36 Transvaginal ultrasound and hysteroscopy are essential for detecting and removing polyps. Hysteroscopic polypectomy (Table 6) significantly enhances fertility outcomes, with spontaneous conception rates rising by 50% within 6 months and ART success rates jumping by 30%–50%.11,36 Office-based polypectomy further reduces the need for hospital procedures, and supplemental hormonal therapies can curb recurrence in high-risk patients. In sum, surgically rectifying these structural anomalies remains a key pillar in RRM, improving both natural and ART-based conception.
Ultimately, pelvic factor infertility and uterine structural irregularities are major impediments to successful conception (Figure 2; Table 2). When judiciously used, surgical and restorative measures can substantially improve results in both natural cycles and ART. Looking ahead, regenerative medicine approaches—such as stem cell therapy or bioengineered uterine tissues—may offer new solutions for challenging presentations. These findings stress the importance of individualized strategies in reproductive medicine to optimize fertility outcomes.
Emerging work suggests that imbalances within the female reproductive tract microbiome can negatively affect fertility. In particular, the endometrial microbiome has been linked to implantation failure and pregnancy loss (Figure 5). Some studies associate increased proportions of non-Lactobacillus bacteria in the endometrium with adverse reproductive outcomes. 40 Additionally, disturbances in the vaginal microbiome (e.g., bacterial vaginosis) are implicated in infertility. Comparative research involving healthy women and those with infertility suggests that routine vaginal microbiota screening might be beneficial for patients seeking infertility treatment. 40
Although these results underscore a possible correlation between microbiome imbalances and fertility difficulties, the data are still developing. Future studies are crucial to decode the mechanisms involved and design effective microbiome-based interventions to bolster fertility outcomes.
Chronic endometritis
Chronic endometritis (CE), which is a persistent inflammation of the endometrial lining often evidenced by plasma cells, is found in 10%–30% of infertile women. Diagnosis is confirmed by histopathological detection of plasma cells, and antibiotic regimens (e.g., doxycycline or metronidazole) can restore endometrial receptivity in 80%–90% of cases. 3
Impact on embryo implantation
CE disturbs endometrial receptivity by impairing implantation markers like HOXA10 and HOXA11. 55 It also hinders decidualization and disrupts the uterine immune environment. 55
Evidence from studies
Cicinelli et al. 37 identified CE in 30.3% of women experiencing recurrent, unexplained implantation failure. Those with CE exhibited significantly reduced implantation and pregnancy rates compared to unaffected women. 37
Antibiotic therapy can improve clinical pregnancy rates (up to 61.3% vs 43.1% in untreated) and slash miscarriage risk (down to 2.2% from 16.0%). 38
A systematic review and meta-analysis by Liu et al. 38 indicated that antibiotic treatment significantly boosted live birth rates in cases of reproductive failures linked to CE.
Hence, while CE negatively impacts implantation and pregnancy outcomes, suitable antibiotic treatment can reverse these effects and elevate reproductive success.
Hydrosalpinx
Hydrosalpinx, or fluid accumulation in the fallopian tube due to distal blockage, illustrates the importance of pre-ART intervention. Untreated hydrosalpinx can slash implantation rates by more than 50%. 29 Salpingectomy, integrated into RRM protocols, enhances uterine receptivity and overall fertility success (Figure 4).
Mechanisms affecting implantation
Embryotoxic fluid from hydrosalpinx can seep into the uterus, damaging embryo development and attachment. Studies also suggest decreased expression of crucial implantation markers (like HOXA10) in the presence of hydrosalpinx.18,19 Mechanical interference from fluid accumulation further disrupts embryo–endometrium contact.18,19
Surgical removal and outcomes
A randomized multicenter trial found that salpingectomy before IVF significantly raised pregnancy rates (36.6% vs 23.9% without intervention). 39
Restoration of endometrial receptivity (e.g., HOXA10 normalization) occurs once the affected tube is removed.18,19
Reduced miscarriage rates have also been observed, reinforcing the pivotal role of salpingectomy in improving embryo implantation success.18,19,21
Overall, surgical removal of hydrosalpinx mitigates its adverse effects, thereby enhancing IVF outcomes. 56
Body mass index
BMI extremes disrupt hormonal homeostasis, influencing ovulation and implantation.20 –22 Obesity in particular raises miscarriage risk and diminishes ART success, while modest weight loss can improve fertility by 15%–20%. 1 Age-related ovarian decline further underscores the need for timely fertility preservation, especially for women older than 35 years (Figures 6 and 7).
Elevated BMI can shift the Endometrial Impact and alter gene expression of WOI indicated with inconclusive debate as relevant to embryo attachment. 21 A systematic review by Turner et al. 23 confirmed that overweight and obese women have significantly lower clinical pregnancy rates compared to normal-BMI individuals, highlighting BMI’s direct effect on fertility. Graphical data from Bellver et al. 21 illustrated how obesity significantly displaces the WOI, reducing endometrial receptivity.
Beyond the decline in oocyte quality, advanced maternal age affects multiple factors: uterine receptivity, fibroid incidence, hormonal equilibrium, vascular perfusion, and immune responses (Figure 7).
Balancing age and family size
For a 90% likelihood of having one child, experts recommend starting attempts by age 35, using ART if needed. To achieve two or three children, couples should ideally begin at ages 31 or 28, respectively. Without ART, the thresholds shift to 32, 27, and 23 23 (Figure 8).
Physiological changes with age
Hormonal: Increased FSH, decreased inhibin B
Vascular: Reduced uterine blood flow may compromise the endometrium 57
Immune: Imbalances in immune cells such as NK cells can hamper embryo implantation.43,58
These factors collectively lower fertility in older women.41,59,60 Although ART bypasses some age-related concerns, RRM addresses coexisting uterine/systemic issues. Combining RRM with ART often maximizes success, reduces costs, and spares couples added emotional strain.
Subclinical hypothyroidism
Subclinical hypothyroidism and autoimmune thyroiditis can hinder ovulatory cycles and pregnancy maintenance. Treatments like levothyroxine 41 have been shown to enhance conception and reduce miscarriage. However, euthyroid women with thyroid autoantibodies remain controversial regarding the impact of levothyroxine on outcomes.41,42,60 Despite these debates, optimizing thyroid function is a recognized strategy to improve fertility potential.42,60
Comparative outcomes of RRM versus ART
RRM versus ART reflects two fundamentally distinct infertility approaches. RRM aims to correct underlying pathologies for natural conception, whereas ART bypasses these issues via laboratory methods (e.g., IVF). RRM’s focus on uterine and systemic abnormalities boosts natural conception (Figure 9). For example, hysteroscopic adhesiolysis for IUAs yields a 40%–60% restoration of natural fertility,61 –63 while removing submucosal fibroids or endometrial polyps can raise spontaneous pregnancy rates by 50%–70% or 40%–60%, respectively.11,35 By contrast, ART success depends on patient age; for example, women under 35 can reach ~40% live birth per IVF cycle, whereas that rate plummets to ~10% in women over 40 (www.eshre.eu).
Long-term outcomes differ as well. Natural pregnancies following RRM often show fewer complications (e.g., preterm labor, cesarean delivery) relative to ART-conceived pregnancies, which carry elevated obstetric risk.44,52,62,63 RRM typically requires more time for diagnostic workups and interventions but is often more cost-effective for younger patients (Figure 10; Table 6). ART provides immediate embryo transfer possibilities but imposes a high financial and emotional burden. 1
When RRM alone fails, combining it with ART yields complementary benefits. For instance, salpingectomy for hydrosalpinx enhances implantation/live birth rates by 40%, 21 while addressing uterine anomalies and optimizing BMI or thyroid function further raises cumulative live birth in ART. 44 Overall, RRM addresses root causes for sustained reproductive health, whereas ART delivers prompt results without resolving underlying issues. An integrated approach merges their strengths, delivering better outcomes with lower costs64 –68 and reduced stress (Figure 9; Tables 7 and 8).
Human reproductive efficiency stands at around 30%, with up to 75% of losses resulting from embryonic failures, often unnoticed by the mother. 44 This precariousness underscores the need to address modifiable factors to optimize outcomes in both natural conception and ART.
Infertility rates have not visibly declined as well as their contributing conditions. Factors include the delayed timing of first pregnancy, leading to diminished ovarian reserve, plus chronic conditions like endometriosis, fibroids, and chronic anovulation, or acute issues (e.g., pelvic surgery, PID). Each has lasting effects on female fertility.
Uterine anomalies—septate uterus, fibroids, IUAs—significantly contribute to infertility and recurrent pregnancy loss. For instance, an untreated septum can lead to miscarriage rates as high as 50%, while hysteroscopic metroplasty can raise implantation from 15%–20% to 35%–50%, reducing miscarriage to 10%–15%. 11 Fibroids (especially submucosal) hamper endometrial receptivity, with hysteroscopic myomectomy boosting natural and ART pregnancy rates by 50%–70%. 35 Recurrence remains a concern, reaching 30% in some series. 54 Emerging robotic surgery and molecular profiling may enhance precision and forecast recurrence. Hydrosalpinx fluid can be embryotoxic and degrade endometrial receptivity. Studies reveal improvements in IVF pregnancy rates (e.g., from 23.9% to 36.6%) after salpingectomy, emphasizing the necessity of prior intervention19,39 (Figure 4).
BMI, age, and thyroid function significantly influence reproductive outcomes. High BMI postpones the WOI, 21 with modest weight loss improving fertility by 15%–20%. 1 Advancing maternal age lowers endometrial receptivity, raising fibroid incidence, and altering hormone balance. 43 Thyroid dysfunction (including hypothyroidism and autoimmunity) disrupts ovulation and heightens miscarriage risk, often correctable via levothyroxine. 42
Microbial shifts in the endometrium or vagina can worsen implantation failure, though further evidence is needed to standardize interventions such as probiotics or targeted antibiotics. 16
RRM treats the root causes, complementing ART’s lab-based methods. RRM interventions—polypectomy, salpingectomy, antibiotic therapy for endometritis—can significantly bolster ART outcomes by restoring uterine receptivity and reducing miscarriage. However, RRM often demands time-intensive diagnostics and may be less effective in advanced maternal age or severe cases. Combining RRM with ART can optimize success rates, shorten repeated ART cycles, and lessen emotional/financial burdens.
Limitations and future directions
Challenges include prolonged treatment times, recurrence of conditions (myomas, IUAs), and limited feasibility in advanced maternal age. Advanced diagnostic tools like AI imaging, molecular profiling, and biomarker panels may expand RRM’s reach. Large-scale, multicenter RCTs are needed to generate robust evidence, while better synergy between RRM and ART could standardize protocols. Enhanced patient education around the long-term benefits of integrated approaches is also essential.
Ultimately, RRM’s holistic model addresses uterine, systemic, and lifestyle factors for sustainable fertility. By tackling the underlying causes that ART alone bypasses, RRM cuts repeated IVF cycles and increases cost-effectiveness. Nevertheless, the success of RRM–ART integration hinges on structured protocols, expanded research, and accessible resources. This synergy can transform modern infertility management, delivering higher success rates and improved well-being to a broader patient population.
Conclusion
RRM provides a comprehensive, root-cause–focused path to address infertility. By diagnosing and correcting uterine anomalies (myomas, polyps, adhesions) and systemic factors (BMI extremes, thyroid dysfunction, microbiome imbalances), RRM can significantly improve spontaneous and ART-related conception rates (Table 9). An integrated approach, using RRM to optimize fertility health prior to or in parallel with ART, yields higher implantation and live birth rates, while reducing repeated IVF cycles and overall costs. Although RRM can require more time and may not suffice for complex or severe cases alone, its synergy with ART appears especially valuable. Further multicenter randomized trials are needed to refine combined RRM–ART protocols and maximize patient outcomes. After a large selection of studies and a small number of selection sample studies the RoB remain the major limitation of this review (Supplemental Material 1). Observational studies generally have the highest RoB due to lack of randomization and potential data errors. RCTs are the most reliable but require careful consideration of blinding and attrition. Systematic reviews provide valuable insights, but selection and heterogeneity bias should be considered. Despite the major difficulties in designing robust studies on surgical treatments, future studies should aim for robust randomization, standardized methodologies, and transparent reporting to minimize bias.
Conclusive remarks.

ART, assisted reproductive technology; BMI, body mass index; RCT, randomized controlled trial; RRM, Restorative Reproductive Medicine.
To fully realize this potential, we need:
Evidence-based guidelines clarifying how and when to interleave RRM steps with ART,
Large-scale RCTs comparing ART alone versus integrated RRM–ART,
Patient education on the benefits of addressing underlying pathologies prior to embryo transfer, and
Advanced diagnostics (like endometrial receptivity arrays, next-generation microbiome sequencing, AI imaging) to identify and correct subtle factors.
By uniting RRM’s strengths with ART’s capabilities, this integrated strategy can transform infertility care, increasing success rates, reducing complications, and offering hope to a broader range of patients.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251345844 – Supplemental material for Revitalizing reproductive health: innovations and future frontiers in restorative medicine
Supplemental material, sj-docx-1-reh-10.1177_26334941251345844 for Revitalizing reproductive health: innovations and future frontiers in restorative medicine by Francesco Maria Bulletti, Evaldo Giacomucci, Maurizio Guido, Antonio Palagiano, Maria Elisabetta Coccia and Carlo Bulletti in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We thank Dr. Marco Berrettini for early data screening assistance.
Author’s note
An Associate Editor of Therapeutic Advances in Reproductive Health is an author of this paper. Therefore, the peer review process was managed by alternative members of the Editorial Board and the submitting Editor had no involvement in the decision-making process.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.