
Abstract
Background:
Septate uterus is a congenital uterine malformation associated with adverse reproductive and obstetrical outcomes. Hysteroscopic septum resection (HSC) with/without balloon stent placement is a treatment option for reconstituting to a normal uterine cavity; however, procedure safety and efficacy of office-based-ultrasound guided (US) HSC in patients undergoing fertility treatment is not thoroughly studied.
Objectives:
(1) To assess the safety and efficacy of office-based US-guided HSC septoplasty; (2) compare the safety and effectiveness of adjuvant intrauterine-balloon-Cook stent (IUBS) and (3) to evaluate the reproductive outcomes after each method.
Design:
Retrospective cohort study.
Methods:
We conducted a retrospective cohort study (n = 90) of patients undergoing HSC at the CReATe Fertility Centre, Toronto, Canada between 2011–2022. The Congenital Uterine Malformation by Experts (CUME-2018) guideline’s criteria were used for diagnosis and classification of malformation/septum size as 1—arcuate uterus <10 mm (52% (47/90)), 2—septum 10–19 mm (31% (28/90)), 3—septum 20–40 mm (7% (6/90)), and 4—complete septa (10% (9/90)). The main outcomes were the rate of procedure complications and the efficacy of septum removal. Secondary outcome measures were reproductive outcomes after septoplasty and the safety and effectiveness of adjuvant IUBS placement. T-test and chi-square test, McNemar test, and Cochran-Mantel–Haenszel test were used for stratified statistical analysis.
Results:
Office-HSC under US guidance was performed in 82 patients (US group) and septoplasty with laparoscopic guidance in 8 patients laparoscopy (LSC) group. IUBS placement had 34% (28/82) of patients in the US group and 12.5% (1/8) in the LSC group. There were no intraoperative or postoperative complications (uterine perforations, excessive bleeding, or infections) in either group. The rate of repeated procedures, implantation, pregnancy, and live birth rates (LBR) were not different when comparing septoplasty with and without IUBS. However, for patients diagnosed with septum class-2, -3, and -4, septoplasty improved their pre-treatment-LBR from 21.6% (8/37) to 77.1% (27/35) post-treatment (p = 0.00005) and decreased pre-treatment miscarriage rate (MR) from 73% (27/37) to post-treatment 29% (7/24) (p = 0.0007) in both groups.
Conclusion:
Hysteroscopic septum resection with transabdominal US guidance in the office setting is a safe and effective procedure in patients with infertility. Office hysteroscopy should be considered in the management of patients with uterine septum to improve LBR and reduce MR. The value of IUBS needs further evaluation in a larger sample-size study.
Plain language summary
Septate uterus is the most common finding concerning the shape of the uterine cavity. It can cause problems with conceiving, pregnancy and childbirth. The aim of this study was to assess how safe and effective the procedure of removal of the uterine septum is in doctors’ office using hysteroscope and ultrasound guidance.
This study summarizes the outcomes from septum resection performed in a single fertility clinic for more than a decade. Data was collected from medical records, and stored ultrasound imaging data.
• Ninety patients were included in this study, and based on the size of uterine malformation were classified as 1-arcuate uterus (<10 mm), 2-septum (10–19 mm), 3-septum (20–40 mm) and 4-complete septa.
• 82 patients were treated by office-based procedure and 8 had hospital based correction of the uterine septum.
• All procedures were completed without complications.
• After removal of the uterine septum the live birth rate increased compared with their pre-treatment live birth rate.
In conclusion, office-based hysteroscopic removal of uterine septum is a safe and effective intervention to improve fertility outcomes for patients with septate uterus.
Introduction
Cruveilhier and von Rokitansky first described uterine abnormalities at the beginning of the 19th century. 1 A septate uterus is a congenital uterine malformation resulting from failure to resorb the fused midline Müllerian ducts during early embryonic life, prior to the 20th gestational week. With an incidence rate of 1–15/1000 women,2–5 the septate uterus is a common uterine anomaly and is associated with poorer reproductive and obstetrical outcomes. 6 Women with a septate uterus are found to be at higher risk for infertility, recurrent pregnancy losses (RPL), as well as obstetric complications, such as preterm birth and malpresentation.7–9 It has been reported that 28%–45% of women affected by an intrauterine septum experience RPL.10,11 Septum attributes such as length and thickness appear not to be correlated with adverse pregnancy and reproductive outcomes.12–15
Impairment of implantation and development of embryos in patients diagnosed with uterine septum has been attributed to (1) molecular mechanisms such as low expression of homeobox protein Hox-A10 and vascular endothelial growth factor receptor genes; (2) reduced glandular and ciliated cells in the endometrial lining of the septate portion of the uterus; and (3) increased content of muscular tissue within the septum that could lead to uncontrolled uterine contractions and poor septum vascularization.16,17
It has been documented that embryo implantation on the septum site results in a higher rate of spontaneous abortion, compared to embryo implantation on the lateral uterine walls. 18 Endometrial biopsy samples from uterine septal tissue reveal reduced sensitivity to pre-ovulatory hormonal changes, when compared to endometrial biopsy samples from the lateral uterine walls. 19
Hysteroscopic septum resection (hysteroscopic metroplasty) is a procedure focused on removing the uterine septum and restoring normal intrauterine cavity contour. A meta-analysis of 38 observational studies found substantial benefits after metroplasty for women experiencing infertility and recurrent pregnancy loss including a significant reduction in spontaneous abortions, preterm deliveries, and an increase in live birth rate (LBR) by 50-fold. 7 Studies have also documented more successful pregnancy outcomes following septum resection in women undergoing in vitro fertilization (IVF).20,21
Hysteroscopic resection of uterine septum performed with ultrasound (US) guided or laparoscopy (LSC) guidance increases the odds for successful intervention and reduces the risks of complications such as uterine perforation, as well as incomplete septum resection. 22 Currently, hystero/laparoscopy is widely performed and is a gold standard for diagnosing and treating infertility. 23 There are notable issues associated with the LSC guidance technique such as increased operating time and resources, in addition to direct health risks for the patient. 24 US guidance during hysteroscopic septum resection may result in similar outcomes as the LSC approach with the additional benefits of safety, convenience (shorter waiting time), efficiency, and reduced discomfort, as it can be performed in the office setting. Kresowik et al. demonstrated reduced perforation rates in patients who underwent US-guided hysteroscopic septum resection compared to LSC assistance with no ultrasound guidance. 25 Intrauterine adhesions after hysteroscopic septum resection (HSC) septum removal are relatively common 6%–24% and can have serious consequences. 26 Oral estrogen, placement of intrauterine devices, or postoperative placement of intrauterine balloon stents has been considered treatments for the prevention of adhesions; however, there is insufficient evidence to recommend routine adhesion prevention. 27 The Cook™ balloon uterine stent has a triangular shape to conform to the uterine cavity shape. When it is used after HSC septum resection, it can mechanically separate the endometrial cavity, including the cornual regions, to prevent the formation of post-treatment adhesions. Often a small Foley catheter spherical balloon is used, but this does not conform to the cavity shape as well, so a Foley catheter is theoretically less effective than the intrauterine balloon. 28 In fact, current literature is heterogeneous and biased, and we cannot draw definitive conclusions about which method is preferable.29,30
The objectives of our study were to assess the safety and efficacy of US-guided office-based septoplasty, with or without, adjuvant intrauterine balloon stent (IUBS) in regard to procedure outcomes (complications and need for repeat procedures) and pregnancy outcomes (LBR, spontaneous abortions). A smaller group of standard hospital-based LSC-guided HSCs performed during the same period was analyzed in addition.
Methods
Study design and setting
This retrospective cohort study was conducted at the CReATe Fertility Centre, Toronto, Canada. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 31
Data collection
In this retrospective study, we included patients with infertility who underwent hysteroscopic septum resection between 2011 and 2022. A total of 90 patients were included in the study. Data related to patient demographics, medical and reproductive history, treatment procedure, complications, need for a repeat procedure, and pregnancy outcomes were collected from patient medical records. For septum classification, we used Congenital Uterine Malformation by Experts (CUME 2018) guidelines inclusion criteria, which included women who had been diagnosed with a uterine septum greater than 1 cm in length and underwent hysteroscopic septum resection. 32 The malformation/septum size was classified as class 1—arcuate uterus (<10 mm), 2—septum size (10–19 mm), 3—septum size (20–40 mm), and 4—complete septa. Patients with a septum length <1 cm were included only in the analysis for treatment safety. Uterine septum diagnosis was established using 3D sonohysterography and/or MRI.
All ultrasound-guided office hysteroscopic procedures evaluated during the study were completed at the CReATe Fertility Clinic while laparoscopic procedures were all performed in a hospital-based operating room at Sunnybrook Health Sciences Centre or Women’s College Hospital, all in Toronto, Canada.
Sample size
The sample size computation was conducted for a logistic regression model, assuming a type I error rate of 0.05, type II error rate of 0.2, baseline pregnancy rate of ~0.25, and an odds ratio of 2. In this case, the required sample size to detect improvement in post-procedure pregnancy outcomes, an odds ratio as small as 2, in line with the results observed in previous studies, 33 is 85 subjects. In our clinic, we had approximately 20 patients/year who underwent treatment for uterine malformations. Thus, we would achieve our desired sample size by analyzing 5 years of patient charts who have undergone hysteroscopic metroplasty.
Septum resection procedure
All patients were referred to CReATe Fertility Centre for assessment and treatment of infertility. All of them underwent routine fertility assessments, and detailed medical and reproductive histories were recorded. Pelvic ultrasonography (US) and sonohysterography were performed for all patients using 2D/3D US. Patients diagnosed with uterine malformation were treated either by office-based HSC metroplasty at CReATe Fertility Centre or LSC-guided HSC septoplasty in operating rooms at Sunnybrook Health Sciences Centre or Women’s College Hospital, Toronto, Canada.
Office-based diagnostic hysteroscopy was performed in lithotomy position under intravenous conscious sedation (midazolam/fentanyl) in the proliferative phase of the menstrual cycle (days 4–9 after the menses phase). After vulvovaginal disinfection and draping, the cervix was gently dilated to 5 mm. A 5-mm continuous-flow mini-hysteroscope with an operative channel allowing the use of scissors (Olympus, Tokyo, Japan). A 0.9% NaCl solution was used as a distention medium. The procedure was performed under transabdominal US guidance. Visualization of external and internal uterine contours, both tubal ostia, condition of the endometrium, and the depth from the interstitial line to the apex of the indentation and angle of the indentation were performed. Septa and any preexisting adhesions were removed by longitudinal incisions using micro-scissors under ultrasound guidance, to form a normal uterine shape. In some cases to prevent intrauterine adhesions, a Cook™ balloon stent was placed for 10 days in the intrauterine cavity under ultrasound guidance to ensure proper placement. Oral estradiol (4 mg BID × 10 days) together with doxycycline (100 mg BID × 10 days) was given to the patients postoperatively. This was followed by medroxyprogesterone 10 mg × 5 to 10 days after stent removal. The decision to place a stent was made at the discretion of the MD, usually based on the size (depth and width) of the septum. A sonohysterogram was scheduled after the next period to check for complete uterine septum removal and adhesion formation. The subsequent fertility treatment plan was optimized based on specific patient circumstances.
Laparoscopic procedure
LSC-guided HSC septoplasty was performed in the operating rooms at either Sunnybrook Health Sciences Centre or Women’s College Hospital, Toronto, Canada. Under general anesthesia, the patient is placed in a dorsal lithotomy position, a weighted speculum is placed in the vagina, and the cervix is grasped anteriorly with a tenaculum. After minimal dilatation of the cervix, an 8 mm hysteroscope was inserted with saline as the distension media. The laparoscopy procedure was performed simultaneously by a second surgeon through an umbilical incision with a 10 mm laparoscope. One to three 5 mm ports were placed in the lower quadrants as needed for manipulators and irrigation. Metroplasty was performed using scissors under laparoscopic guidance to avoid perforation. Methylene-blue due transit test was generally performed to test tubal patency after the metroplasty.
Statistical methods
Continuous variables are presented as mean (standard deviation) and dichotomous variables are presented as counts (percentage). Baseline characteristics of participants from both guidance groups (LSC and US) were compared using t-tests for continuous variables and chi-square tests for count data. Univariate and multivariate logistic regression analyses were used to evaluate the association between guidance technique and repeat procedures, complications, implantation, and pregnancy. Adjusted models accounted for age (years), Anti- Müllerian Hormone (AMH) (pmol/L), and sperm quality (abnormal vs normal). McNamar test and Cochran-Mantel–Haenszel test were used for stratified analysis.
Two-sided p-values <0.05 were considered significant unless otherwise stated. All analyses were conducted in the R Statistical Package.
Results
Medical charts and associated ultrasound imaging data were reviewed for a total of 90 women who had undergone hysteroscopic septum/subseptum resection: US guidance was performed in 82 patients (US group) and 8 patients had the septoplasty with laparoscopic guidance (LSC group). In the US group, 34% (28/82) had IUBS placement after the procedure and 66% (54/82) did not. In the LSC group, 12.5% (1/8) had IUBS placement after the procedure and 87.5% (7/8) did not. Of the total 90 patients, 52% (47/90) had an arcuate uterus in class 1, 31% (28/90) were in class 2, 7% (6/90) in class 3, and 10% (9/90) in class 4. Pregnancy outcomes within 2 years of the septoplasty were recorded and included in the analysis. Patients with a class 1 arcuate uterus (n = 47) were excluded from the outcome analysis as per current American Society of Reproductive Medicine (ASRM) 2021 Müllerian anomalies classification standards and outcome analysis. 34
There was no statistically significant difference between age, BMI, smoking, diagnosis of primary or secondary infertility, male factor, previous septoplasty, endometriosis, or other diagnosis between the groups that did not use IUBS n = 61 and the group that had IUBS placement after the HSC septoplasty (Table 1). Causes for primary and secondary infertility ranged from advanced reproductive age, polycystic ovarian syndrome, poor ovarian reserve, and male factor. No statistically significant difference in other baseline characteristics was noted between the two groups (Table 1).
Baseline patient demographic and clinical preoperative characteristics.
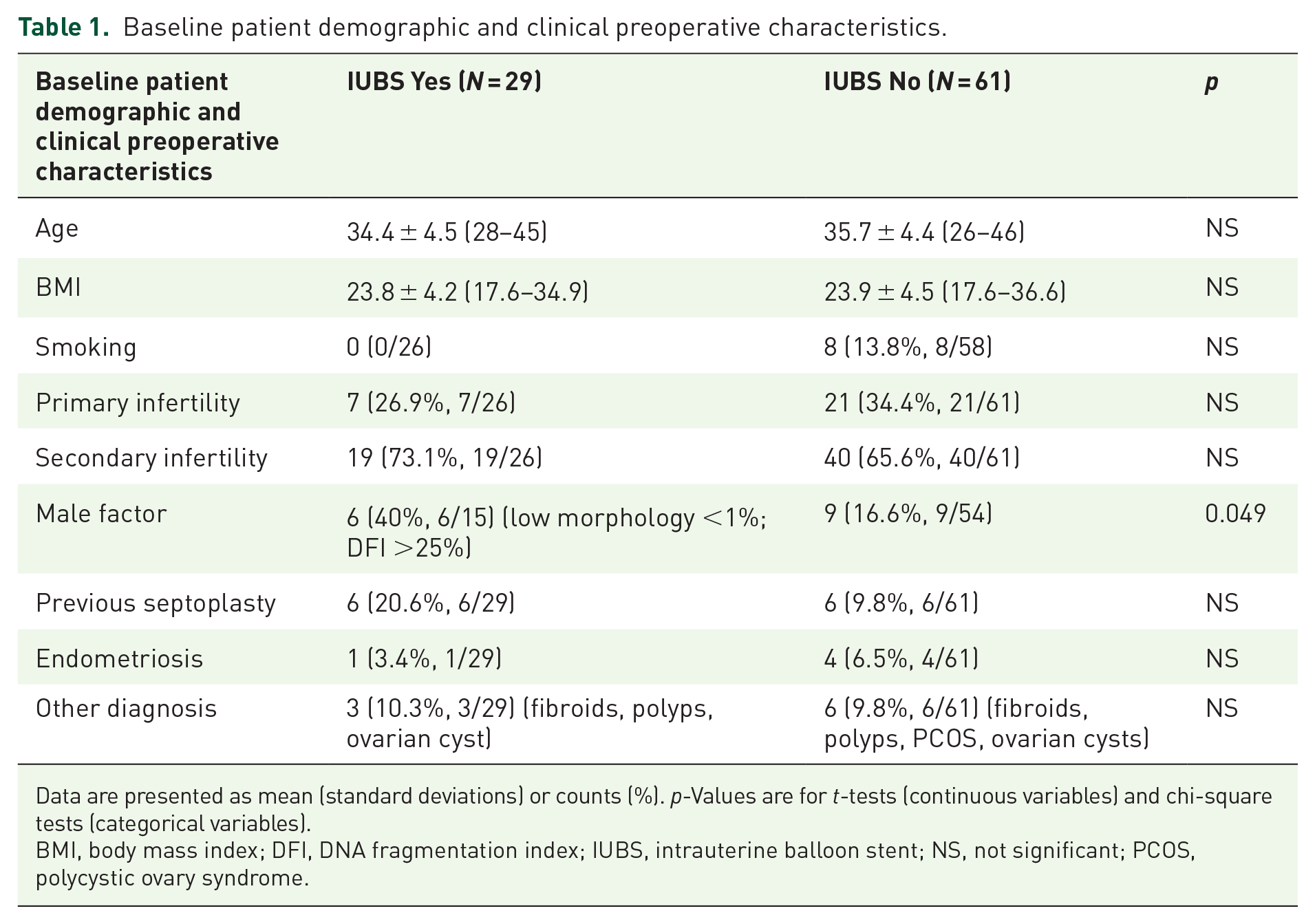
Data are presented as mean (standard deviations) or counts (%). p-Values are for t-tests (continuous variables) and chi-square tests (categorical variables).
BMI, body mass index; DFI, DNA fragmentation index; IUBS, intrauterine balloon stent; NS, not significant; PCOS, polycystic ovary syndrome.
Table 2 summarizes the use of IUBS for patients with different septum sizes and according to CUME 2018 classification. In summary, IUBS was used in 11/47 (23%) patients with arcuate uterus, in 10/28 (36%) patients with septum from 10 to 20 mm, 4/6 (67%) patients with septum from 20 to 49 mm, and 4/9 (45%) patients with complete septum. HSC without adjuvant IUBS was performed in 36/47 (77%) patients with the arcuate uterus, 18/28 (64%) with septum from 10 to 20 mm, 2/6 (33%) with septum from 20 to 39 mm, and in 5/9 (55%) patients with complete septum (Table 2).
Use of adjuvant IUBS among patients with different sizes of septum and according to CUME 2018 classification.
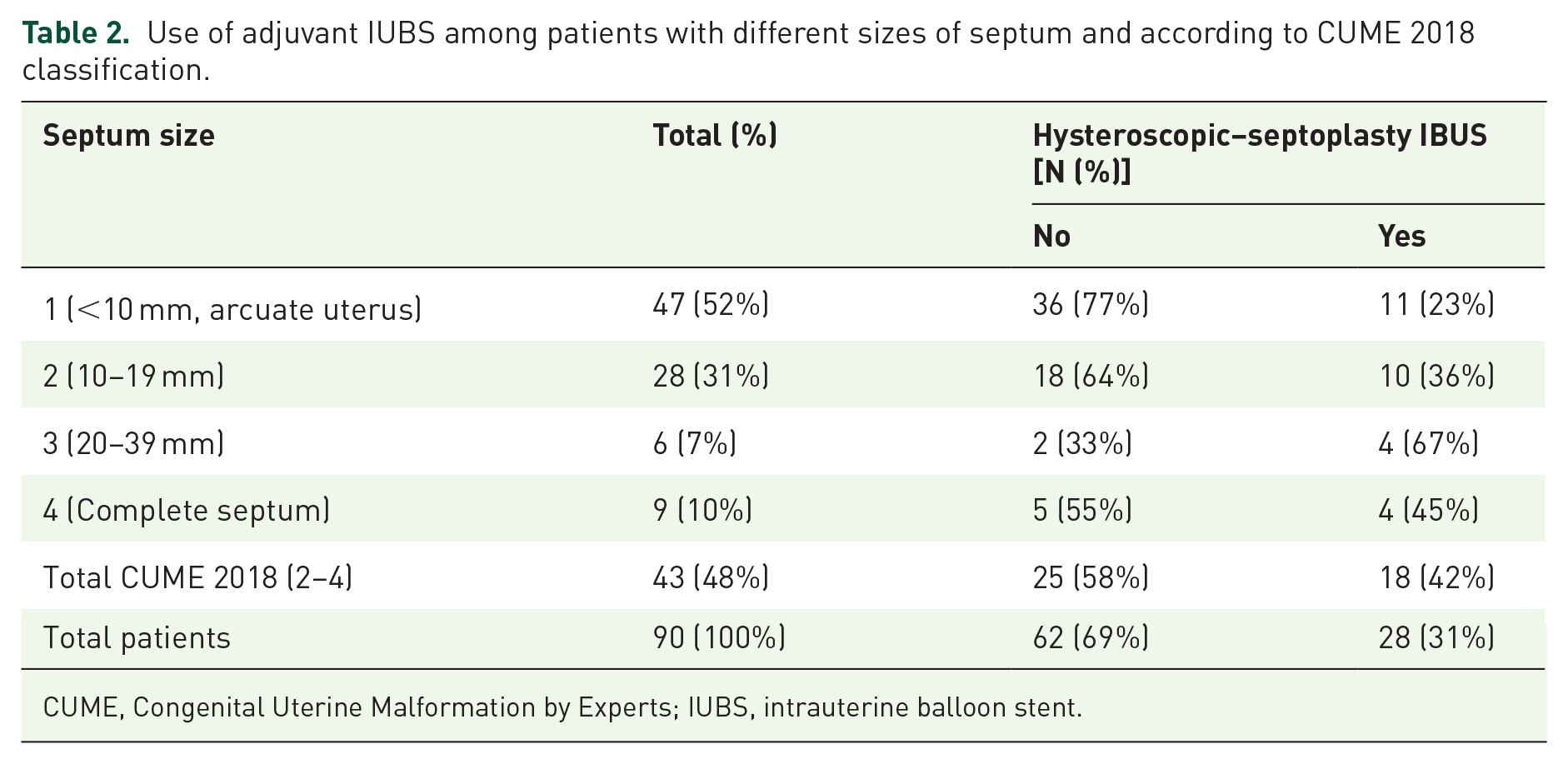
CUME, Congenital Uterine Malformation by Experts; IUBS, intrauterine balloon stent.
No intraoperative and postoperative complications (uterine perforations, excessive bleeding, or infections) or side effects were noted during all the procedures related to office HSC septoplasty under US guidance performed for 82 (91%) patients and HSC septoplasty with LSC guidance for 8 (9%) patients. The use of IUBS was relatively safe with no complications or side effects reported. Resection of the septum was successful for 76.5% (65/85) of the patients who had follow-up evaluation by 3D sonohysterography. Five patients did not have follow-up evaluations. The rate of repeated procedures (septum revision and/or adhesiolysis) for patients with IUBS placement after septoplasty was 28%, whereas for patients without IUBS placement was 35% which was not statistically different but the number of cases in each group was not powered to show a difference (Supplemental Table 1).
Reproductive outcomes for patients with septate uterus diagnosed by CUME 2018 criteria are summarized in Table 3. LBR and spontaneous abortion rates before and after septoplasty are presented in Figure 1(a) and (b). Septoplasty in this group of patients increased the LBR by sevenfold (OR 6.9, 95% CI (2.5–18.9), McNemar p = 0.004) without significant difference between patients that had IUBS placed after intervention and those that did not. There were no differences in the fertility treatments used in patients with IUBS (Intrauterine insemination (IUI)-21.4%; IVF-78.6%) and without IUBS (IUI-47.6%; IVF-52.4%), (p = 0.11) (Supplemental Table 2). The reproductive outcomes of the whole study cohort are summarized in Supplemental Table 3.
Reproductive outcomes after septoplasty for patients diagnosed by CUME 2018 criteria with and without the use of IUBS. Live birth rate and spontaneous abortion rate were compared pre- and post-treatment.

The Italic identifies the statistically significant differences.
CUME, Congenital Uterine Malformation by Experts; IUBS, intrauterine balloon stent; LB, live birth; NS, not significant (p > 0.05); SA, spontaneous abortion.

Reproductive outcomes after hysteroscopic septum resection with and without adjuvant intrauterine balloon stent (IUBS). (a) Live birth rate. (b) Spontaneous abortion rate.
Septoplasty significantly reduced the rate of spontaneous abortions in the group of patients diagnosed with septate uterus by CUME 2018 criteria from 73% (27/37) prior to the treatment to 29% (7/24) after the treatment (p = 0.04, OD 0.35 (0.12–0.9)) (Table 3).
There were no statistical differences in LBR and spontaneous abortion rate when comparing LSC-guided septoplasty to office-based US septoplasty with and without IUBS (Supplemental Table 3).
Discussion
Hysteroscopic metroplasty has emerged as a beneficial procedure for women with a history of infertility, recurrent pregnancy loss, or recurrent implantation failure. Although many studies have examined procedure and pregnancy outcomes following LSC-guided metroplasty, very few studies have evaluated the efficacy of using US guidance. In addition, there is limited literature comparing the two forms of guidance in terms of important patient outcomes.
This retrospective chart review of US-guided hysteroscopic septum resection provides evidence that US-guided hysteroscopic septum resection can be performed in an office-based setting without incurring additional risks for repeat procedures or complications when compared to the conventional LSC approach. Specifically, we observed similar outcomes between LSC- and US-guided HSC uterine anomaly resection in terms of complication rate and the need for repeat procedures. Both forms of guidance and post-treatment placement of IUBS appear to present similar outcomes in terms of pregnancy rates, complications, and the need for repeat procedures. However, the IUBS was more often used in the larger septum cases and results should be interpreted with caution since the decision to place a stent was made at the discretion of the surgeon. Additional analysis with larger numbers will be needed to do this type of sub-analysis. A similar observation of the limited benefit of adjuvant IUBS after septoplasty was noted in a recent ASRM guidance paper. 35 In our cohort, there were no differences in the fertility treatments used to achieve pregnancy after septoplasty with and without IUBS (Supplemental Tables 2 and 4). IUI was used in 47.6%, IVF in 23.8%, and IVF with PGT-A in 28.5% of patients after septoplasty without IUBS. Fertility treatments in patients after septoplasty with IUBS were IUI in 21.4%, IVF in 35.7%, and IVF-PGT-A in 42.85%. Sample size and multiple treatment modalities limit the power to detect the superiority of a treatment approach.
With US guidance, there is the added ability to visualize both the uterine cavity and the fundal uterine contour allowing for increased precision, control, and resection accuracy. Consequently, estimation of the uterine fundus thickness is much simpler when compared to LSC which only allows for external visualization. With a better approximation of fundus thickness, risks for perforation are much lower and there is a greater likelihood of achieving complete septum resection and eliminating the need for a repeat procedure. 11 Unlike LSC, US guidance is noninvasive, and it is easier to perform.
Generally, US-guided procedures in our clinic have an average waiting period of 1 week compared to 2–3 months for operating room-based procedures. The large difference in waiting times can be attributed to the flexibility of being able to perform US-guided procedures in an office-based setting versus hospital-based procedures. Accordingly, substituting ultrasound-guided office procedures for laparoscopy allows for faster booking times, reduced operating time, eliminates the need for general anesthesia, and faster recovery. Furthermore, hysteroscopy can inadvertently resolve cervical stenosis which often goes undiagnosed with standard ultrasound evaluations and accounts for up to 5% of infertility diagnoses. 36 It is defined as the inability to pass a 2.5 mm Hegar dilator through internal cervical os, while external cervical os (ECO) stenosis is when the ECO diameter is less than 4.5 mm.37,38 Operative hysteroscopy is the gold standard for managing cervical stenosis, showing high success rates, particularly in severe cases and has added benefit for patients with infertility.39,40
Our study showed that office-based hysteroscopic metroplasty is a safe and effective intervention to improve fertility outcomes for patients with septate uterus. There were no intraoperative or postoperative complications (uterine perforations, excessive bleeding, or infections) and septoplasty significantly improved the LBR in treated patients. These results give reassurance to both clinicians and infertility patients and have the potential to reduce wait times for elective hospital-based operative procedures and avoid risks associated with operative laparoscopy and general anesthesia. In Canada, especially after the COVID pandemic, patients seeking fertility treatment are facing long wait times to be seen by fertility specialists and even longer to receive elective hospital-based operative procedures, which may impact the outcome of their fertility treatment.
Our study described comparable outcomes in procedure safety and pregnancy outcomes between both forms of guidance during septum resection. Similar studies conducted in the past reported improved outcomes with the use of US guidance. Procedures other than septum resection have also transitioned to US guidance due to improved results. US imaging can be used to guide the catheter during embryo transfer, helping the operator to align it with the curvature of the uterus, to ensure the embryo is deposited in an appropriate position within the endometrial cavity. 41 In a randomized controlled trial (RCT) evaluating the efficacy of surgical termination of pregnancy (dilation and curettage), it was found that using continuous ultrasound guidance during the first trimester resulted in lower complication rates when compared to the conventional procedure without ultrasound guidance. Specifically, the group randomized to receive ultrasound guidance had reduced recovery time, blood loss, and overall procedure time.42,43 Our study was not powered to determine if there is a superiority of office-based hysteroscopy with ultrasound guidance compared to laparoscopic-guided hysteroscopy due to the small sample size. So far, the only randomized controlled study by Rikken et al., evaluating the effectiveness of metroplasty versus expectant management, did not show a significant improvement in ongoing pregnancy rate, pregnancy loss rate, LBR, and preterm birth in patients who had HSC septum resection. 44 However, this study had several limitations that preclude the interpretation of the data, including the small sample size (n = 68 women) and heterogeneity in terms of patients’ characteristics and reproductive disorders, as well as the three different classifications used to define uterine septum (American Fertility Society (AFS) 1988; European Society of Human Reproduction and Embryology (ESHRE)/ESGE consensus 2013, and ASRM 2016). The importance of a discrepancy between different definitions of the septate uterus was discussed by Ludwin et al. 45 They found that only 2.7% (7/261) of patients were diagnosed as septate uterus according to all three definitions of septum: ESHRE/ESGE 2016, CUME-2018, and ASRM 2016. ESHRE/ESGE classification detected significantly more cases than ASRM-2016 (31% vs 5%, RR = 6.7, p < 0.0001) and CUME-2018 (31% vs 12%, RR = 2.6, p < 0.0001). In addition, the ASRM-2016 classification could not classify 6.5% of cases (gray zone: neither normal, arcuate, or septate). 45 Similarly, Detti et al. compared 4 different classification methods of diagnosis of uterine septum/subseptum in 125 women (AFS-10 mm 1988/2003, ESHRE-ESGE 2013 classification, ASRM 2016 criteria, and 5.9-mm length cut off, 2017). 46 The 5.9 mm cutoff was diagnosed as septate 89/125 uteri, but the ASRM 2016 classification diagnosed only 8/125 as septate uterus, and 25/125 were in the gray zone. ESHRE-ESGE 2013 classification inconsistently diagnosed sub-septations and some septa over 1 cm were not diagnosed. 46 These studies indicate that standardization of diagnostic methods and classifications in clinical practice is crucial for accurate diagnosis of uterine septa and for better prediction of the cutoff values necessitating metroplasty. Contrary to the RCT study by Rikken et al., 44 a meta-analysis of 22 studies that evaluated pregnancy and obstetrics-related outcomes after hysteroscopic metroplasty in women diagnosed with a uterine septum (n = 998) compared with no treatment (n = 699) have shown a higher rate of term delivery by 2.2-fold, decrease in spontaneous abortion rate by 50%, and a lower rate of malpresentation by 70% in the treated group. 33 In addition, Jiang et al. in their meta-analysis showed that HSC metroplasty can increase LBR by fourfold and reduce spontaneous abortion rates by 64% in patients with primary infertility and recurrent spontaneous abortions. 47
Our data did not have the power to demonstrate the benefit of adjuvant intrauterine balloon stent placement after HSC septoplasty. Similar findings were observed in a small RCT (n = 28) by Abu Rafea et al., who evaluated the effect of intrauterine placement of Foley balloon after HSC septum resection. 48 They compared two groups: the first group (14 patients) with a Foley balloon filled with 5 ml normal saline placed in the patient’s uterus after HSC resection for 5 days, and the second group of 14 patients without additional treatment after HSC metroplasty. Control HSC was performed 3 months after treatment in both groups, and there were no differences in the outcomes. 48
Our study has the advantage of using well documented and systematically recorded patient data, operative procedures, and imaging data in the same office environment with minimal operator differences. The septoplasty was performed by highly experienced surgeons who are academically affiliated and are involved in the training of REI fellows, ensuring high standards in diagnostic and therapeutic approaches selected. The ultrasound measurements were done by experienced ultrasonographers at the time of diagnosis, operative procedure, and postoperative follow-up with direct input from the MD. To reduce the potential bias, all ultrasound records were reviewed, and all necessary measurements were updated for the study and classified the malformation/septum based on CUME 2018 guidelines. The main limitations of this study are its retrospective nature and the relatively small size of the studied groups which have prevented us from adjusting for all pertinent covariates for each of the outcomes (BMI, smoking, and different IVF cycle parameters).
In the future, it would be valuable to assess these outcomes on a larger sample size and to conduct an RCT comparing office-based procedures and the use of a balloon stent versus not. A subgroup analysis of pregnancy outcomes following each type of fertility treatment would also provide greater insight into whether these procedures have varying effects based on the type of fertility treatment received post-resection.
Conclusion
In summary, this study provides evidence supporting the use of ultrasound guidance during hysteroscopic septum resection. Compared to the laparoscopic-guided approach, ultrasound guidance displayed similar procedure safety and pregnancy outcomes, with the added benefit of being able to perform the procedure in an office-based setting. The findings presented are in line with current literature which suggests that patients would benefit greatly from the ultrasound-guided procedure as there is the added benefit of convenience, comfort, safety, and practicality. Population-based studies with larger sample sizes, RCT design, and longer follow-up periods should be conducted in the future to assess all patients important outcomes more accurately. The added value of IUBS needs to be evaluated with a larger sample size.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251324951 – Supplemental material for Safety and effectiveness of office hysteroscopic metroplasty with and without uterine stent placement in infertile population: a 10-year retrospective study
Supplemental material, sj-docx-1-reh-10.1177_26334941251324951 for Safety and effectiveness of office hysteroscopic metroplasty with and without uterine stent placement in infertile population: a 10-year retrospective study by Mitko Madjunkov, Jak Ozsarfati, Ari Baratz, Karen Glass, Prati Sharma and Clifford Librach in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors would like to thank all staff, patients, and their families at CReATe Fertility Centre.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.