
Abstract
Background:
Placenta previa with antepartum hemorrhage (APH) is common and closely related to maternal and fetal morbidity and mortality. It is of the utmost importance to prepare for the possibility of APH using perinatal factors prior to delivery.
Objective:
To develop and validate a nomogram predicting APH in women with placenta previa based on the perinatal factors.
Design:
This was a retrospective and prospective cohort study of pregnant women with placenta previa.
Methods:
The model was developed in the retrospective and validated in the prospective cohort study. Multivariate logistic regression was applied to discover independent variables and develop a nomogram to predict the possibility of APH. An Excel form computer interface was constructed to use the model.
Results:
There are 1601 and 693 participants in the retrospective and prospective cohort study. Maternal age (odds ratio 0.950, 95% confidence interval 0.918–0.984), married (0.533, 0.309–0.920), parity (1.240, 1.024–1.502), threatened abortion (5.059, 3.648–7.014), and complete placenta previa (1.833, 95% CI 1.469–2.289) were independent variables for APH in placenta previa women. The area under the curve and concordance index were 0.828 and 0.676, respectively. The model was a good fit by the Hosmer–Lemeshow test (p = 0.352). The prospective validation proved the reliability of the prediction nomogram. The Excel form computer interface was practical.
Conclusion:
A nomogram based on perinatal factors was developed and validated to predict APH in women with placenta previa. The reliable tool may thereafter offer important assistance for decision-making processes.
Introduction
Placenta previa is characterized by the placenta covering part or all of the internal cervical os.1,2 It is related to poor maternal and neonatal morbidities including malpresentation, preterm deliveries, low Apagar scores, intrauterine growth restriction, adherence of the placenta, maternal hemorrhage, thrombophlebitis, septicemia, the need for blood transfusion, hysterectomy, and even maternal and neonatal mortality.3,4 We previously reported that the prevalence of placenta previa was about 1.25% among Chinese pregnant women. 5 In recent years, the incidence of placenta previa has been increasing due to increasing previous cesarean deliveries, uterine surgery, advanced maternal age, multiparity, and smoking.6–8
Antepartum hemorrhage (APH) is a serious complication of pregnancy that is characterized by bleeding from the genital tract before the fetus’s delivery.9–11 Significant morbidities associated with APH include preterm delivery, higher rates of NICU admission, low birth weight, massive intrapartum bleeding, postpartum hemorrhage, blood transfusion, hysterectomy, and even neonatal and maternal death. 12 It is more common in placenta previa women.13,14 Studies, including ourselves, have reported that APH has an incidence of 50%–52% in placenta previa women.9,13 So far, the etiology and pathogenesis have not yet been clearly identified of APH in pregnant women with placenta previa. There were some studies to explore the risk factors and found that cervical length, placental type and location site, and maternal age were associated with APH.14–17 However, the results are often contradictory. For example, Dibaba B et al. found the risk of APH could increase fourfold in advanced maternal age in their case–control study with 420 participants. 18 At the same time, Kuribayashi et al. found younger than 30 years was associated with a 2.08-fold increased risk of APH in their retrospective cohort study with 233 participants. 15 Perhaps, small sample sizes and lack of validation are the main reasons for this contradictory result.
Considering the danger of APH resulting from placenta previa, it is of the utmost importance to prepare for the possibility of APH in placenta previa women using perinatal factors prior to delivery. Unfortunately, there is no clinically available predictive model for the management of placenta previa APH thus far. We wanted, first, to investigate the risk factors associated with APH, second, to build a prediction nomogram, a clinically usable and simple statistical visual tool, and then, to verification of use value, using our large database with 2294 participants, the early prediction and timely management of APH in placenta previa women.
Methods
Participants
This was a retrospective and prospective cohort analysis for participants who presented to our center for placenta previa at a tertiary care medical center between January 2012 and December 2022. The Local Ethics Committees approved (FSFY-Med-2019044) access to participant information via electronic medical records. In the training cohort, a retrospective study with 1601 women was delivered from January 1, 2012 to December 31, 2019. In the validation cohort, a prospective study with 693 women was hospitalized from January 1, 2020 to December 31, 2022. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies of Epidemiology (STROBE) cohort studies statement. 19
Inclusion criteria included gestational age between 28 and 42 weeks with a viable delivery and diagnosed placenta previa after delivery. Exclusion criteria were the following: gestational age <28 weeks or gestational age >42 weeks at delivery, fetal malformation, intrauterine fetal death, coagulation dysfunction in women, or incomplete antenatal records. Participants were divided into placenta previa with APH (PP-APH) and placenta previa without APH (PP-non-APH).
Data collection
Maternal demographic, pre- and post-natal information, including age, parity, pre-existing disease before pregnancy, in vitro fertilization, prior dilatation and curettage, regular antenatal care, and gestational age, birth weight, gender, Apgar score at 5 min and mode of delivery, and risk factors associated with APH before 28 gestational age, and pregnancy complications, was obtained from the electronic medical records. Each included participant is anonymized prior to analysis in the form of an Excel file.
Definitions
The diagnosis of placenta previa was based on a transvaginal or transabdominal ultrasound performed at the time of admission, and it was verified during the delivery, as previously described.20–22 Placenta previa was classified as complete placenta previa (CPP) and non-CPP (partial, marginal, or low-lying placenta). 1 Antepartum hemorrhage was defined as cumulative vaginal bleeding greater than 20 ml between 28 weeks and prior to delivery. 9 Threatened abortion is defined as bleeding through the vagina, with a closed cervix, and the presence of the fetal heartbeat, that occurs before the 28 gestational ages. 23 Marital status was divided into married and unmarried.
Statistical analysis
Continuous data were reported as mean ± standard deviation, and count data were reported as rate (%), and compared using the t-test and chi-squared test, respectively. Univariate and multivariate logistic regression analyses were used to determine the effects of perinatal factors on APH. The nomogram model was built using multivariate logistic regression to estimate the likelihood of antepartum hemorrhage. A multivariate logistic regression was performed to identify distinct predictors (p < 0.05) who were then employed to build a nomogram based on the data for predicting the likelihood of antepartum hemorrhage. Predictor lines were created forward to establish that the points were on the “Total Points” axis; and then, a line was traced downstairs to reflect on the bottom scales, thereby defining the likelihood of antepartum hemorrhage. The visually appealing model of prediction was subsequently externally validated. To evaluate the model’s goodness of fit, the Hosmer–Lemeshow test and coefficient of determination (R2) were used.24,25 The predictive accuracy and conformity of the model were assessed using the receiver operating characteristic (ROC) curve, area under the ROC curve (AUC), concordance index (C-index), calibration curve, and Brier score.26,27 The decision curve analysis evaluated the model’s clinical value for participants. Boot-strapping with 1000 resamples was used to evaluate both discrimination and calibration. Statistical significance was confirmed when p < 0.05. Statistical analyses were carried out using R version 4.3.1 and SPSS 20 (IBM-SPSS Inc., Chicago, IL, USA). An Excel form computer interface was constructed to use the model.
Results
Participant characteristics
A total of 1678 participants was obtained from our center for placenta previa in the training cohort between January 2012 and December 2019; 77 participants were not included due to incomplete antenatal records. There was no significant difference in the perinatal outcomes between the included cases and incomplete cases, apart from the incomplete antenatal variables (Table S1). In the end, data from 1601 participants were included and analyzed in the training cohort. The mean maternal age was 32.57. The rates of mothers with 1, 2, and above 3 parity were 29.2%, 56.0%, and 14.7%, respectively. In total, 96.2% of the participants had married, 14.9% suffered threatened abortion, and 54.0% had CPP (Table 1).
General characteristics of all participants in training and validation cohort.

In the prospective validation cohort, 693 participants were used for validation purposes from January 1, 2020 to June 30, 2022. The mean maternal age was 32.98. The rates of mothers with 1, 2, and above 3 parity were 32.9%, 52.1%, and 14.9%, respectively. Married participants accounted for 97.1%, 17.2% suffered threatened abortion, and 56.3% had CPP. There was comparability for the perinatal outcome variables between training and validation cases, except for the cesarean section variable (Table 1).
According to the definition of APH, 710 participants (710/1601, 44.3%) were included in the APH group, and 891 participants (891/1601, 55.7%) were included in the non-APH group in the training cohort. Table 2 shows the 20 perinatal factors.
General characteristics of participants and multivariate logistic regression analyses for screening predictors.

APH, antepartum hemorrhage.
Predictive factors selection
Five perinatal factors were independent predictors of antepartum hemorrhage (APH), according to a multivariate logistic regression analysis. These are the following: maternal age (odds ratio (OR) 0.950, 95% confidence interval (CI) 0.918–0.984), married (OR 0.533, 95% CI 0.309–0.920), parity (OR 1.240, 95% CI 1.024–1.502), threatened abortion (OR 5.059, 95% CI 3.648–7.014), and CPP (OR 1.833, 95% CI 1.469–2.289) (Table 2).
Nomogram development
The above five factors were used to establish the logistic regression model (Table 3), and further to integrate to the nomogram (R2 = 0.133, C-index = 0.676) (Figure 1). The scoring model of AHP was as follows: 0.458 − 0.031 * maternal age + 0.212 * parity – 0.656 * (married = 1) + 1.638 * (threatened abortion = 1) + 0.581 * (complete placenta previa = 1). More higher total score for each participant revealed an increased probability of APH. Furthermore, the model was an excellent fit using the Hosmer–Lemeshow test (p = 0.352).
The logistic regression of five perinatal factors for constructing the model.

CI, confidence interval; OR, odds ratio; SE, standard error.
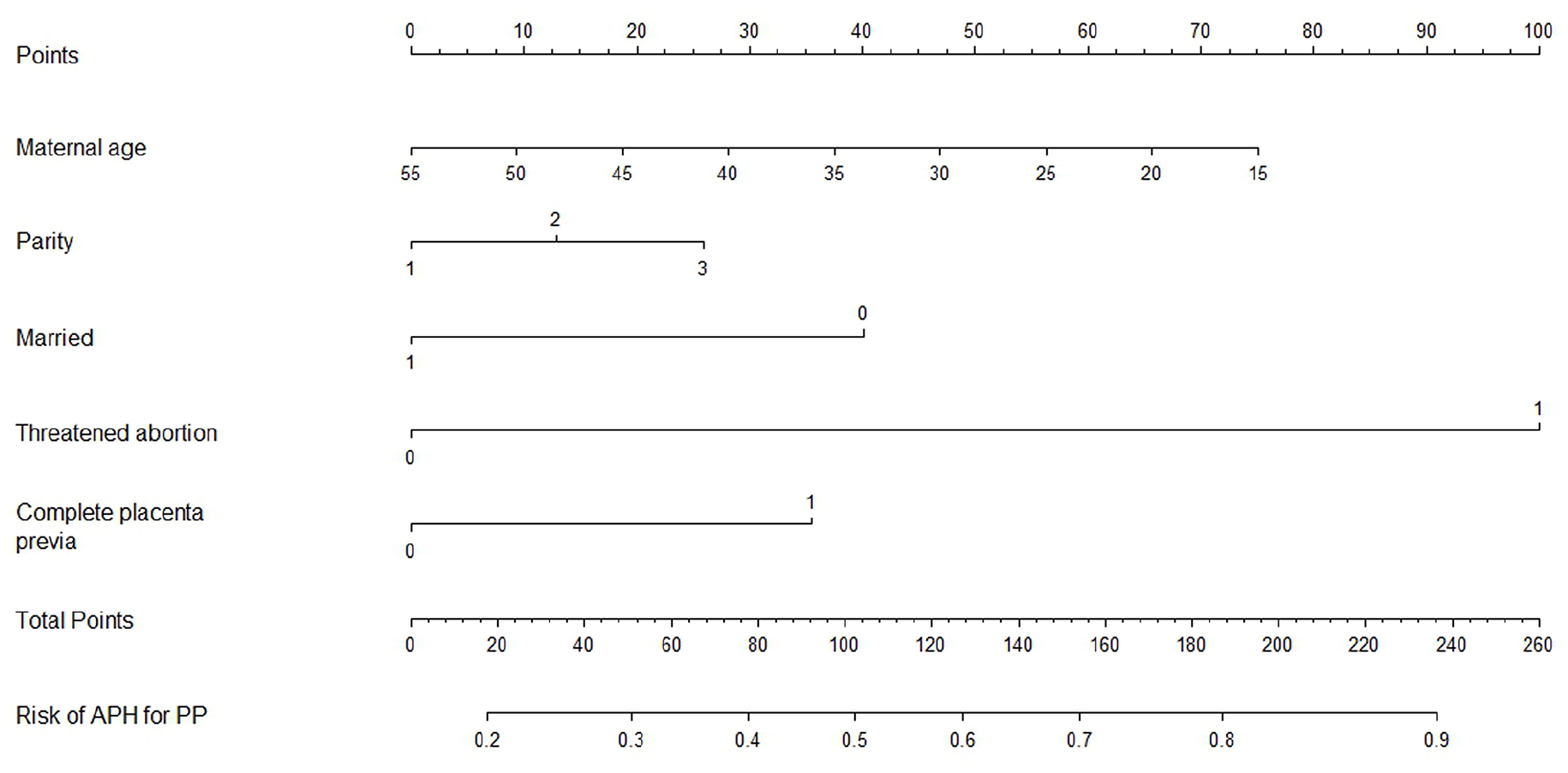
Nomogram for the APH for PP women.
Predictive accuracy of the nomogram
The AUC was 0.828 (95% CI 0.808–0.848) (Figure 2(a)), and the calibration curve was near the ideal diagonal line (Figure 3(a)) in the training cohort. The decision curve analysis showed a better net benefit in the predictive model (Figure 4(a)). The Brier score of the nomogram was 0.222 in the training cohort (Figure 5(a)). On the other hand, 693 participants from January 1, 2020 to June 30, 2022 were applied for validating and evaluating the nomogram. The AUC was 0.817 (95% CI 0.785–0.850) (Figure 2(b)), indicating that the nomogram was accurate in the validation cohort. The calibration curve was likewise very near to the ideal diagonal line, and the model displayed good uniformity overall in the validation cohort (Figure 3(b)). Moreover, the decision curve analysis also showed the net benefit of the predictive model, as well as that in the validation cohort (Figure 4(b)). The Brier score was also 0.222 (Figure 5(b)).

ROC curves. Training cohort (a), validation cohort (b).
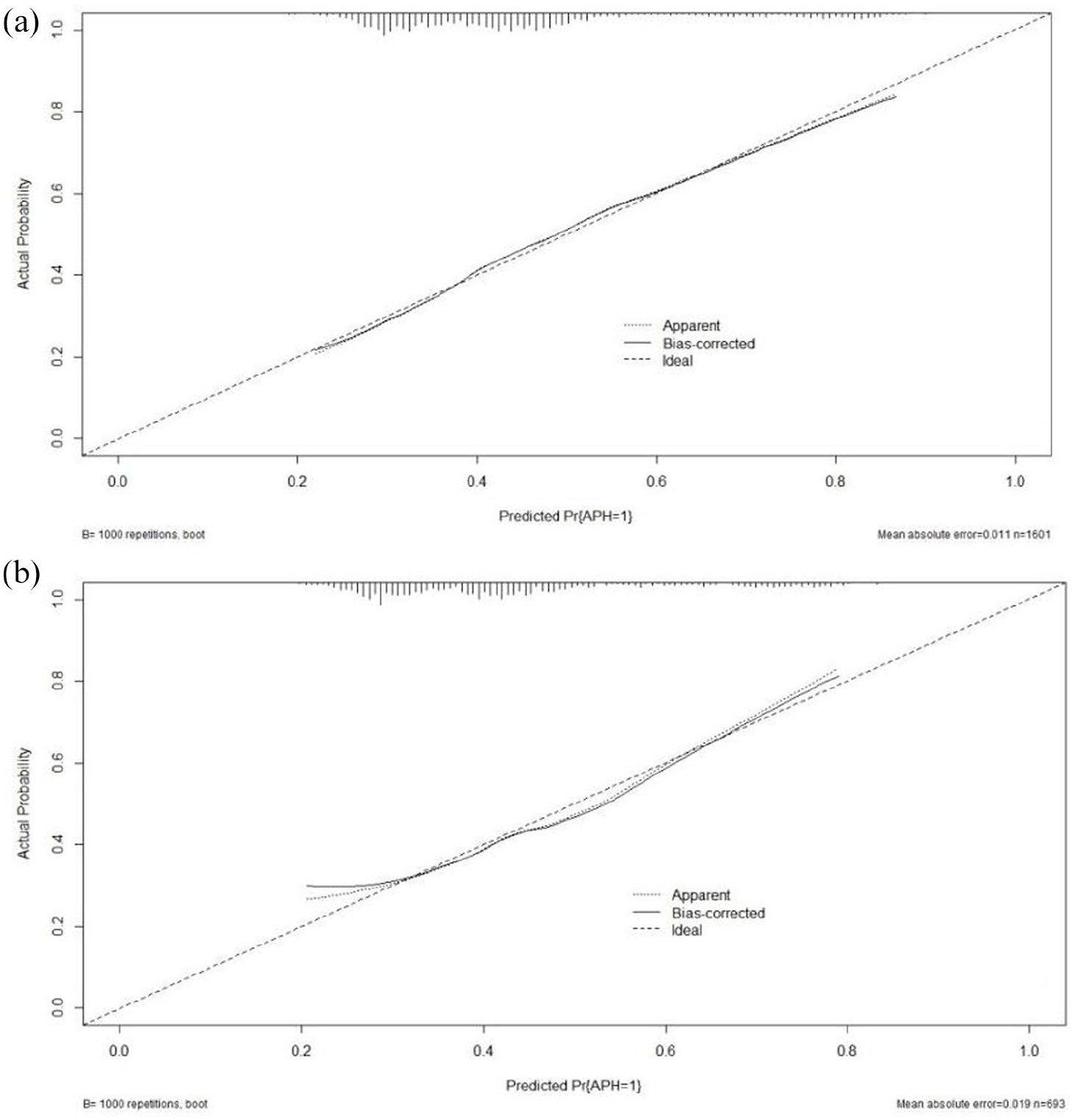
Calibration curve for predicting the probability of APH for PP women. Training cohort (a), validation cohort (b).

The Brier score for the prediction nomogram of APH for PP women. Training cohort (a), validation cohort (b).

The decision curve analysis curve for predicting the probability of APH for PP women. Training cohort (a), validation cohort (b).
Computer interface
We constructed an Excel form computer interface to calculate the likelihood of APH in pregnant women with placenta previa using the aforementioned prediction model. An example of the interface is represented in Figure 6.
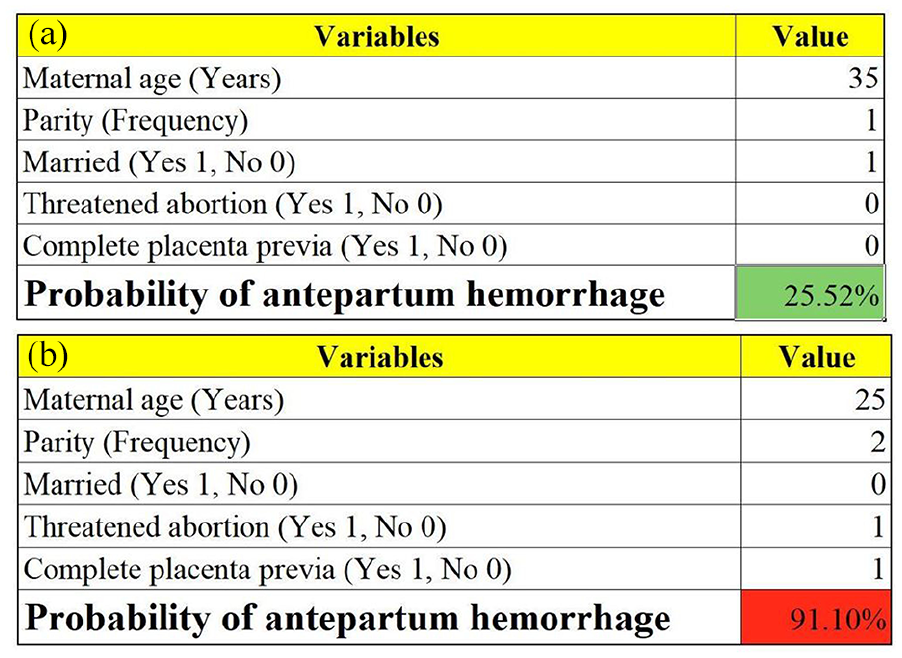
Examples of the computer interface (Excel form). Two examples of placenta previa women with low (a) and high risk (b) of antepartum hemorrhage.
Discussion
We developed and validated a nomogram according to five perinatal factors (maternal age, marital status, parity, threatened abortion, and placenta previa type) that accurately predicted the probability of antepartum hemorrhage in placenta previa women in this study.
The majority of the variables used in our nomogram have been determined to be warning signs for antepartum hemorrhage. As we know, maternal age was associated with adverse obstetrical outcomes.28,29 Previously, meta-analyses revealed that pregnancy outcomes, such as preterm birth, gestational diabetes mellitus, preeclampsia, placental abruption, placenta previa, and postpartum hemorrhage, were more common in older-aged pregnancies. 30 However, there is a controversy between maternal age and antepartum hemorrhage. A case–control study found maternal age could increase the risk for antepartum hemorrhage. 18 On the other hand, Kuribayashi et al. showed maternal age could reduce the risk of antepartum hemorrhage in placenta previa women. 15 Interestingly, we also found maternal age was a positive factor for placenta previa women in antepartum hemorrhage, and the result was consistent with Kuribayashi et al.’s study.
Furthermore, maternal age was included in the predictive model in this study and indicated that it was an independent predictor. The maternal age appeared to be negatively linked with the nomogram points, resulting in which the younger the mother, the greater the risk of antepartum hemorrhage. This could reflect population-specific factors. On the one hand, very young pregnant women (such as adolescents) are not yet fully mature due to their physical development and may have a higher risk of preterm birth, low birth weight, and other conditions, which are sometimes accompanied by APH. On the other hand, this population may be at increased risk of pregnancy complications due to poor nutritional status or lack of adequate knowledge of pregnancy health care.
It is debatable if parity is a risk factor for adverse pregnancy outcomes. Previous studies indicated that the pregnancy complications and adverse outcomes evaluated were increased in the primiparous women when compared to the multiparous women.31,32 However, most studies revealed that multiple parities could lead to adverse pregnancy outcomes, such as anemia in pregnancy, preterm birth, placenta abruption, placenta previa, oligohydramnios, and macrosomia.33–37 In terms of the relationship between antepartum hemorrhage and parity, our findings are consistent with previous systematic reviews and meta-analysis studies indicating that parity had a positive correlation with antepartum hemorrhage in placenta previa. 9
Various studies have been published about the pregnancy effect on marital status. In a cross-sectional study, the authors found that married women were more likely to have a 40% decreased likelihood of giving birth to an underweight baby. 38 Married women could receive physical, emotional, and financial assistance from their partners to help them stay mentally well throughout the entire pregnancy and delivery and lower their risk of experiencing unfavorable pregnancy outcomes. In this study, marriage could reduce the risk of antepartum hemorrhage for placenta previa women and is the third independent predictor. It is important to note that marital status may reflect the influence of underlying factors (e.g., social support, socioeconomic status).
Threatened abortion is a common complication of pregnancy, occurring in about 20% of recognized pregnancies. 39 Our study showed that the incidence of threatened abortion was 16.04% in placenta previa women. Threatened abortion can have serious psychological repercussions, such as anxiety, sadness, and post-traumatic stress disorder, as well as extensive bleeding, infection, and surgery-related complications.40,41 In addition, the current studies suggest that threatened abortion is also associated with maternal risk of non-gestational diabetes and cardiovascular diseases later in women’s lives.23,42,43 As an independent predictor, placenta previa women suffering threatened abortion were more likely to develop antepartum hemorrhage in this study.
CPP could increase maternal and neonatal mortality and morbidity. The type of placenta previa is frequently a key factor in deciding on the delivery method as well as pre-delivery preparations like blood product preparation and potential obstetrical surgeries. Antepartum hemorrhage has been correlated with the type of placenta previa; however, conflicting studies have led investigators to different conclusions. On one hand, the authors found no association between the type of placenta previa and antepartum hemorrhage.13,15 On the other hand, lots of studies revealed that when compared to women with incomplete placenta previa, women with CPP had a higher incidence of antepartum hemorrhage.16,44,45 We further found that CPP is an important predictor of antepartum hemorrhage in this study.
Some studies have explored the influencing factors of APH in placenta previa.14–17,46,47 However, most of them only involve univariate and multivariate regression analyses. The results of this stage of research are difficult to apply to clinical practice, and the prediction model has not been well verified and evaluated, so it is difficult to evaluate the accuracy and clinical practicability of the results. We evaluated the prenatal risk factors for antepartum hemorrhage in placenta previa women and developed a likelihood prediction model for the early identification and management of antepartum hemorrhage in placenta previa women. Our validation cohort demonstrated the model’s good accuracy and conformity. Clinicians can employ the nomogram, a visual, clinically usable, and individualized model, as an easy-to-use and understandable tool for realistic prediction. What needs to be emphasized is that it is an advantageous and valuable tool when making decisions, but eventually, it remains a clinical judgment.
As far as we are aware, we were the first to create and verify a straightforward technique to estimate the potential incidence of antepartum hemorrhage in placenta previa women in an extensive group of individuals. However, several limitations need to be noted. First, recall bias is inevitable and might have influenced the results because of the nature of retrospective analysis. Second, owing to a lack of data, several potentially meaningful predictors, including cervical length, weight gain during pregnancy, maternal occupation, income level, education level, and others, were not evaluated in this study. Third, the validation cohort is from the same single medical center, potentially limiting generalizability to other populations with different demographic, clinical, or healthcare system characteristics. Researchers, including ourselves, will evaluate additional potential indicators in conjunction with clinical variables in a subsequent multicenter study to establish a more precise forecasting algorithm for antepartum hemorrhage in a determination to lower maternal and newborn mortality.
Conclusion
This study revealed that maternal age, marital status, parity, threatened abortion, and type of placenta previa were predictors of antepartum hemorrhage in placenta previa women. We developed a first perinatal prediction nomogram according to several perinatal predictors for the early prediction of antepartum hemorrhage in placenta previa women, and our outside validation supported the credibility of this model. Our prediction score may prove to be a valuable resource for doctors, midwives, and obstetric nurses, and the nomogram may thereafter offer important assistance for decision-making processes.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251315127 – Supplemental material for Prediction nomogram for antepartum hemorrhage in placenta previa women
Supplemental material, sj-docx-1-reh-10.1177_26334941251315127 for Prediction nomogram for antepartum hemorrhage in placenta previa women by Dazhi Fan, Pengzhen Hu, Jiaming Rao, Dongxin Lin, Jie Yang, Zhengping Liu and Xiaoling Guo in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941251315127 – Supplemental material for Prediction nomogram for antepartum hemorrhage in placenta previa women
Supplemental material, sj-docx-2-reh-10.1177_26334941251315127 for Prediction nomogram for antepartum hemorrhage in placenta previa women by Dazhi Fan, Pengzhen Hu, Jiaming Rao, Dongxin Lin, Jie Yang, Zhengping Liu and Xiaoling Guo in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.