
Abstract
Background:
Reproductive healthcare is essential for all people, including lesbian and bisexual women. However, lesbians and bisexual women are among society’s most marginalised and excluded members.
Objective:
This study aimed to explore the challenges faced by lesbian and bisexual women in accessing Sexual and Reproductive Health (SRH) Services in Bulawayo, Zimbabwe.
Design:
An exploratory, descriptive qualitative study was conducted on two populations that included eight participants identified through the Voice of the Voiceless organisation in Bulawayo and 10 key informants and probed the challenges faced by lesbians and bisexual women when accessing SRH services.
Methods:
Data were gathered through 10 key informant interviews and 1 focus group discussion (FGD; with 8 participants). The interviews and FGDs were recorded, transcribed verbatim, coded and thematically analysed.
Results:
The themes that emerged included the uptake of SRH services among lesbians and bisexual women, the challenges faced by lesbians and bisexual women when accessing SRH services, and strategies to aid the uptake of SRH services by lesbians and bisexual women. The findings showed that the uptake of SRH services was generally low and was influenced by factors such as clinical settings. The challenges mentioned included stigma and the unavailability of specific lesbian and bisexual women’s services. By contrast, the most frequent strategies included affirmative training for healthcare providers and improved clinical settings to become friendly and inclusive.
Conclusion:
There is an imperative for targeted SRH services that address the distinct needs of lesbians and bisexual women, in line with the 95-95-95 strategy and Sustainable Development Goals target 3.7. The observed low uptake of these services can be attributed to several systemic barriers, including inadequate training of health providers, negative attitudes and lack of inclusive policies. Enhancing the sensitivity of health facilities, strengthening links to sexual health education and implementing supportive legal frameworks are essential steps to improve SRH outcomes in this population. These findings elucidate critical gaps within the current healthcare system and present significant opportunities for policymakers to formulate evidence-based strategies to ensure equitable access to SRH services, thereby advancing public health objectives.
Plain language summary
According to the United Nations, everyone should have access to healthcare related to sex and reproduction to improve their chances of fully protecting themselves from sexually transmitted infections, such as HIV and AIDS, and eliminate it by 2030. However, lesbian and bisexual women in Bulawayo often face challenges accessing services related to sexual health and reproduction. This study aimed to understand the difficulties faced by these women in accessing these services. Researchers interviewed experts, lesbians, and bisexual women to gain a better understanding of their difficulties. They discovered that many women rarely use these health services for two main reasons. First, some women fear judgment or discrimination by health care providers. Second, often no specific services are offered to address the needs of lesbian and bisexual women. To improve access to care, this study recommends that healthcare workers receive training to be more welcoming and to understand lesbian and bisexual women. Additionally, healthcare facilities should be designed to be inclusive and offer services that specifically cater to the sexual and reproductive health needs of this population.
Keywords
Background
Ensuring universal access to services such as Sexual and Reproductive Health (SRH) is one of the primary goals of the United Nations Sustainable Development Goals (SDG) 3.7 and 5.6. 1 Furthermore, the World Health Organization’s 13th General Programme of Work included a strategic focus on Universal Health Care, focusing mainly on Sexual and Reproductive Health and Rights. 2 This is a critical opportunity to ensure that SRH services are included in global, regional and national efforts to achieve universal healthcare. Sexual reproductive healthcare is essential for all people, including those who self-identify as lesbian or bisexual. Lesbians’ and bisexual women’s health issues and SRH care are inextricably linked because both require individuals’ autonomy in making their most intimate decisions. 3
In many regions and countries, the negative effects of the criminalisation of sexual and gender minorities are exacerbated by rights-violating laws and policies. Countries such as Uganda have laws prohibiting same-sex relationships and gender nonconformity, and other countries such as Botswana have laws prohibiting ‘cross-dressing’ or ‘impersonating the opposite sex’, which exacerbate SRH inequities among sexual and gender minorities. 4 Criminalisation can also make HIV testing and access to social services and support more difficult, increasing the prevalence of HIV/sexually transmitted infections (STIs) and physical/sexual violence. 5 Consequently, despite the availability of SRH services, the number of sexual and gender minorities using these services remains poor, even in Zimbabwe.6–12 Some policies are generally not supportive and lead to discrimination between gender and sexual minority populations, thus shunning these SRH services.10,11,13–15
In Zimbabwe, lesbians and bisexual women are among society’s most marginalised and excluded members. They are particularly exposed to stigma, assault and discrimination because of their actual or perceived sexual orientation and gender identity. 16 This can have long-term social and psychological ramifications and major negative consequences on society. This is because of the community’s lack of acceptance. 5 Lesbians and bisexual women face several overlapping structural barriers in exercising their basic SRH rights, including access to SRH care. SRH care includes various services, such as STI treatment, human papillomavirus (HPV)-related cancer prevention and other reproductive tract morbidities. 17
In Bulawayo, lesbians and bisexual women cannot access specific healthcare services because of the strong heteronormative attitudes still present among medical professionals, such as ignorance of the existence of female sex relations. Due to their discomfort, most lesbian and bisexual women avoid routine testing for STIs, cervical cancer and HPV, which increases their risk of contracting these diseases and puts them at a higher risk than their heterosexual counterparts. Consequently, if the barriers to SRH services that lesbian and bisexual women face in Bulawayo are not addressed, the country may fall short of meeting the UNAIDS 95-95-95 targets for ending AIDS and other STIs by 2030. 18 Therefore, this study explores the challenges faced by lesbian and bisexual women in accessing SRH services in Bulawayo.
Methods
Study area
The study was conducted on lesbian and bisexual women, as captured in the Voice of the Voiceless Organisation (VoVo) clientele. VoVo in Bulawayo is driven by a feminist collective of Lesbians, Bisexual and Transgender activists working to empower marginalised communities such as lesbian and bisexual women by challenging exclusionary attitudes and norms and affirming their human rights. 19 Bulawayo is the second capital city of Zimbabwe, with an estimated population of 874,479 by 2023. 20 The city is served by private and public health facilities, the majority of which are public and government owned. The city has many clinics run by the Ministry of Health and Child Care (sometimes in collaboration with non-governmental organisations (NGOs) and donors) and three referral health facilities, namely, United Bulawayo Hospitals, Mpilo Central Hospital and a mental institution, Ingutsheni Hospital. 12 The private sector also manages several healthcare facilities in the city. According to the National Aids Council of Zimbabwe, the city has a significant number of key populations, including the LGBTI community. 21 However, because of the country’s constitution criminalising homosexuality and the lack of legal recognition for same-sex relationships, individuals who identify as LGBTI may encounter discrimination and stigmatisation. Consequently, only a limited number of individuals within this community can openly express themselves, without fear of repercussions. A map of the study area is shown in Figure 1.
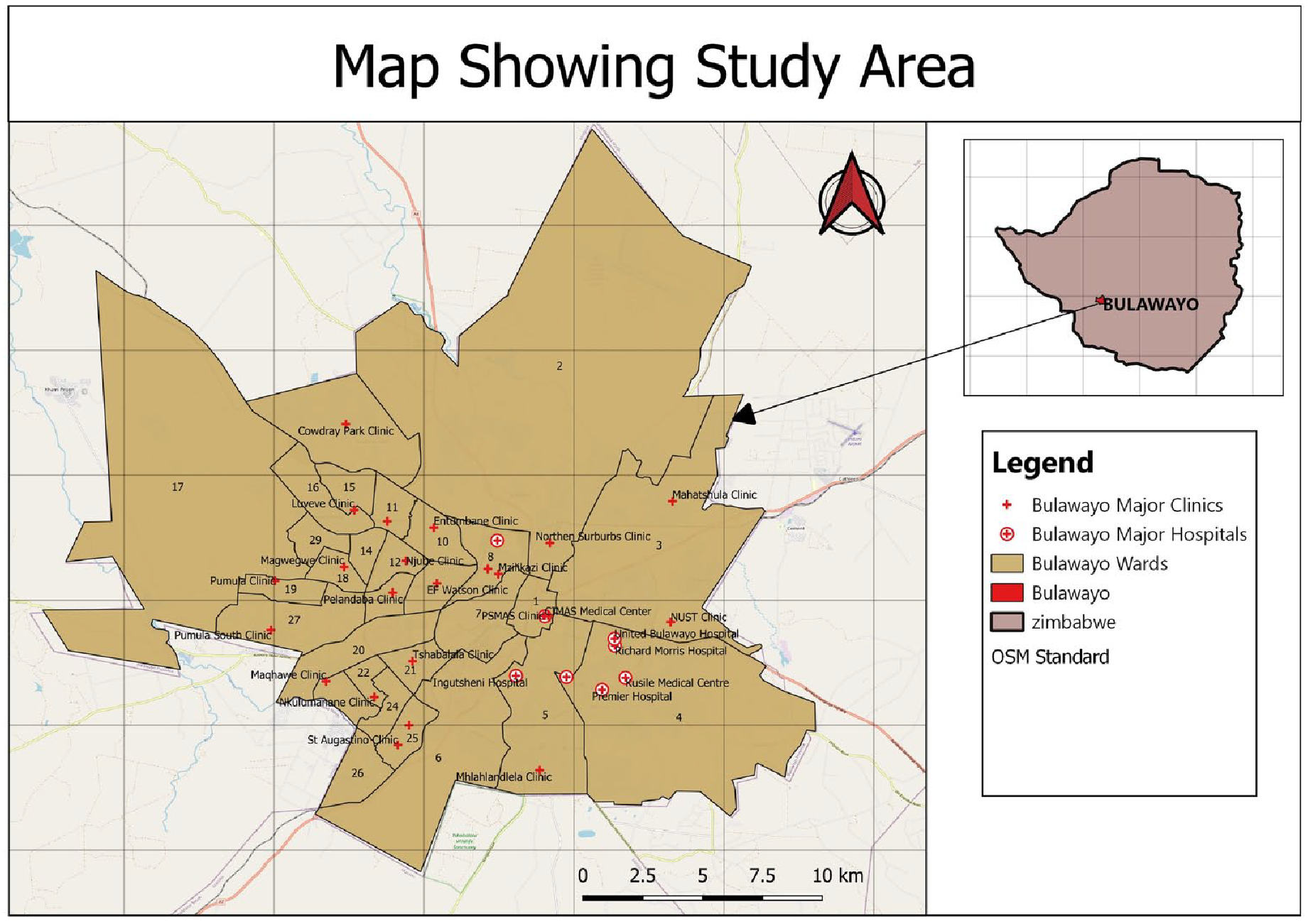
Study area map.
Study design
An exploratory, descriptive qualitative study was conducted on selected participants and key informants, and the challenges faced by lesbians and bisexual women when accessing SRH services. This design centred mainly on the participants’ lived experiences helped answer the research questions more in-depth, reflecting on the patterns and seeking to understand them more deeply. 22 This study design was appropriate because it allowed the researchers to collect detailed information about lesbian and bisexual women’s challenges and how these subsequently shaped their uptake of SRH services in Bulawayo.
Target population and sampling
The study population for the focus group discussion (FGD) consisted of lesbian and bisexual women aged 18 years and older who visited the VoVo in Bulawayo. Convenience sampling was used to recruit eight participants (Lesbian and Bisexual women). The process involved reaching individuals who were accessible and available to participate in the study. The recruitment process took place in February 2023 and informed consent was obtained from all participants before the FGD. Data saturation was achieved during the discussions, indicating that no new information was generated. Furthermore, key informants for interviews were purposively selected, and they included key population officers, program managers and program officers at Civil Society Organisations (CSOs) that serve lesbians and bisexual women; nurses and counsellors serving lesbians and bisexual women; a researcher; and a full-time Public Health lecturer. Data saturation was also achieved during the interviews, ensuring comprehensive insights from all the informants.
Data collection procedure and tools
Data were gathered using a key informant interview and an FGD, guided by an interview and FGD guide with open-ended questions, and enabled the collection of relevant data through the enquiry of challenges faced by lesbians and bisexual women when accessing services and strategies that can aid the uptake of services by lesbians and bisexual Women in Bulawayo. The interviews and FGD were recorded using a tape recorder after the participants gave their consent before recording. Pseudonyms were used to ensure the privacy and confidentiality of participants. The FGD lasted approximately 45 min, whereas the interviews took between 20 and 40 min to complete. The interviews and FGD were conducted in English, isiNdebele or Shona (depending on participants’ preferences), as these are the three major languages spoken in Zimbabwe. Validity in translation was ensured by translating the tools into native languages and then using an independent translator to translate them back to English from native languages. Differences were noted, and anomalies in interpretation were attended to ensure consistency in interpretation by the participants. Furthermore, the tools were pretested to ensure that meaning was retained. The audio recorded the FGD and interviews, and the recordings were later transcribed verbatim and then analysed using thematic analysis. Interviews were conducted by the first author.
Data management and analysis
The recorded data from the FGDs and in-depth interviews were transcribed verbatim and imported into MAXQDA Version 20 Pro for analysis. MAXQDA is developed and distributed by VERBI Software GmbH, a German company based in Berlin https://www.maxqda.com/help-mx24/welcome. Two researchers (M.Y.K. and W.N.N.) independently coded the transcripts. The initial coding utilised a combination of deductive codes derived from key concepts in the literature and inductive codes emerging from the data. An iterative process of open coding identified key themes, followed by axial coding, to explore the relationships between them. Regular meetings between coders facilitated discussion and refinement of the codebook, ensuring consensus and enhancing conceptual clarity. Ultimately, the main themes and sub-themes identified from the interrogated data were presented to answer the study’s objectives. Adherence to the COREQ checklist throughout the analysis and reporting process ensured a comprehensive and transparent account of the research process. 23 The completed COREQ checklist is provided in the Supplemental Material.
Results
Key informants for the study included one openly lesbian identifying Programs Manager, one Programs Officer of a CSO, two Counsellors, one from the public health facilities and the other being based at a CSO, two nurses, one from a public health facility and the other from one of the NGO clinics, two Key Population Officers, a Full-time Lecturer and a Researcher on LGBTI and Sex Worker issues (Table 1).
Key informants.

NGO, non-governmental organisation; PSI, Population Services International.
Lesbians and bisexual women access various SRH services (Table 2). Respondents indicated that services accessed by lesbians and bisexual women were similar to those accessed by heterosexual women or anyone else. However, they noted that lesbians and bisexual women might need other services not available in public health facilities; as such, lesbian and bisexual women end up accessing these services from private institutions and NGOs:
. . . . Therefore, in most facilities I have worked with, the SRH services are the same; we offer the same services such as family planning, cervical cancer screening, general HIV testing, and condom distribution. However, the unfortunate part is that we do not offer dental dams; therefore, because we do not offer dental dams, it may be something that we need to look into in terms of public health, and we also do not offer finger cots. Because of the nature of the sex they engage in, these become risk areas where one can then contract HIV. (KI_5)
SRH services available for lesbian and bisexual women in Bulawayo.
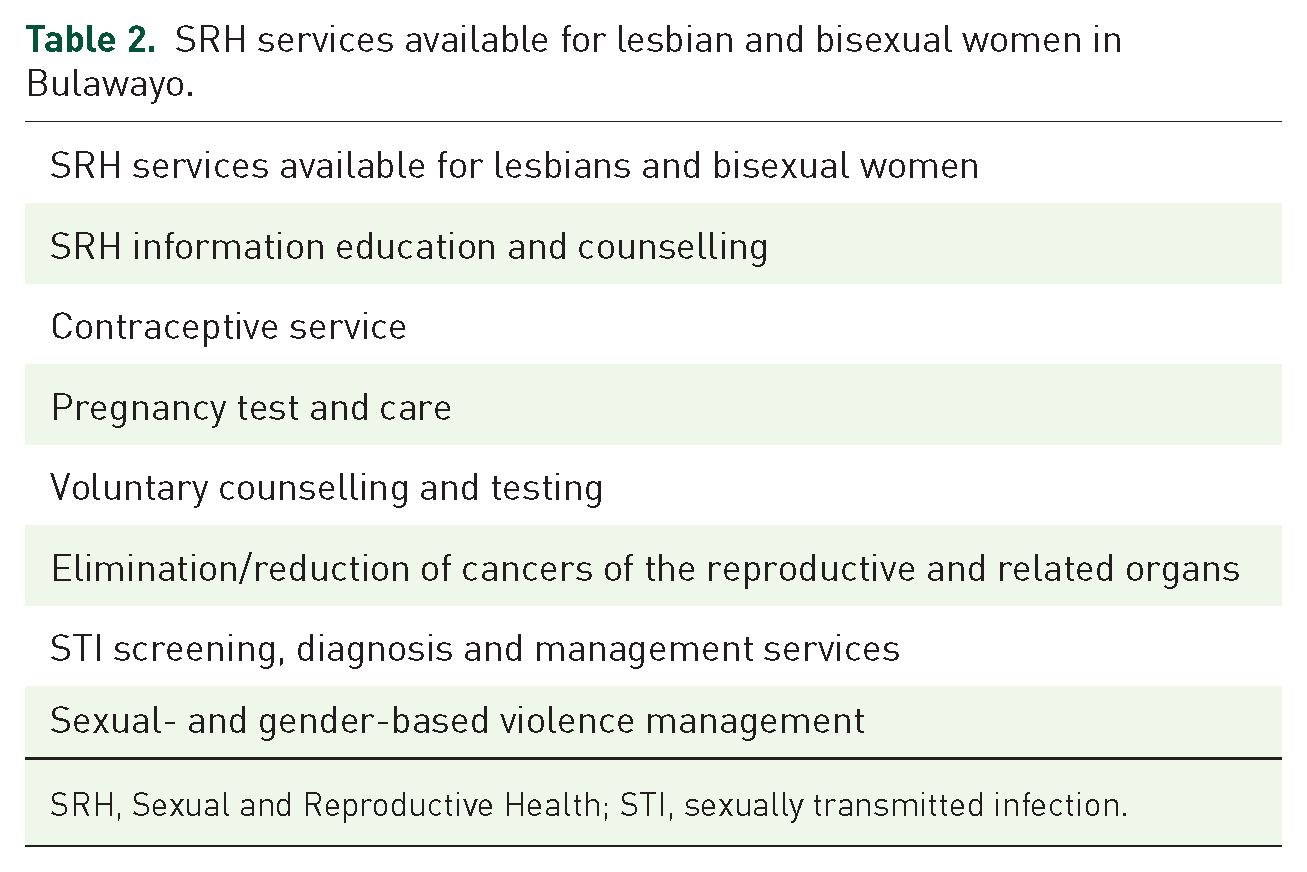
SRH, Sexual and Reproductive Health; STI, sexually transmitted infection.
Findings from FGD
The FGD participants included three lesbians, four bisexual women and one queer woman. The youngest participant was 22 years old, and the oldest participant was 35 years old. Four participants highlighted formal employment, three students and one unemployed person (Table 3).
FGD participants.
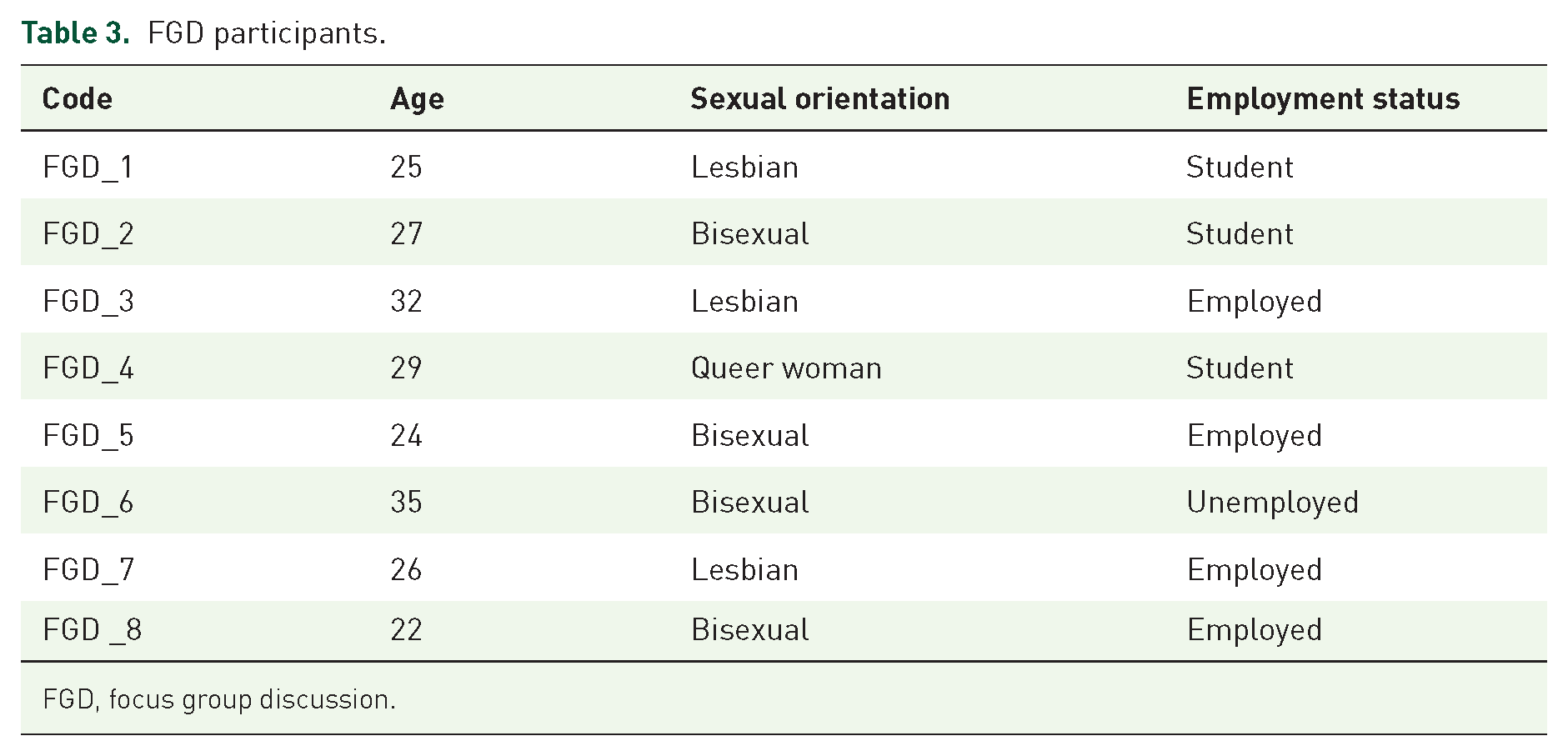
FGD, focus group discussion.
Themes that emerged from FGD
Two main themes were obtained, guided by the objectives and FGD guides. In addition, 10 sub-themes were obtained, as guided by the research objectives and data collection tools, as summarised in Table 4. These themes are discussed in detail in the following sections.
Themes that emerged from focus group discussion.

NGO, non-governmental organisation; SRH, Sexual and Reproductive Health.
Challenges faced by lesbians and bisexual women in accessing SRH services in Bulawayo
Six sub-themes emerged under the main theme, ‘challenges faced by lesbians and bisexual women in accessing SRH services in Bulawayo’. These are detailed below.
Stigma, discrimination or victimisation at the hands of healthcare providers
Respondents cited stigma, discrimination and victimisation in healthcare settings and society as challenging when accessing SRH services. Stigma and discrimination even lead to failure to get justice and redress from the Republican police for same-sex intimate partner violence:
Living a secret and engaging in unsafe practices for fear of discrimination in my area of residence, I can’t seek services at my local clinic because my aunt works there, and we are already not in good books because she knows I am lesbian. I fear being discriminated against and being judged by who I am. I live my life in fear, hoping that my secret will not come out because I stay in the locations and the people there can be so homophobic. (FGD Participant_3) Nurses, especially at the clinics in my hood, are very homophobic, so I avoid getting services there and would rather look for an EPM or Peer Educator. (FGD Participant_4) . . . because I thought this was a safe space with no judgment, and when I mentioned that I was lesbian, the response was really ‘amazing’ in a negative way because she blatantly just said, Do you know that these are demons, right? (FGD Participant_1)
Lesbian and bisexual women bear the brunt of insensitive healthcare workers
A sub-theme emerged: those assigned females at birth but identifying lesbians or bisexual women face enormous challenges in healthcare settings from insensitive healthcare workers who have low knowledge levels on the needs of lesbians and bisexual women. According to the participants, the healthcare workers expressed shock. This kind of reaction has resulted in some lesbian and bisexual women not returning for further treatment and resorting to self-medication using unofficial means:
Nothing is said about us, lesbians and bisexual women’s needs, in these hospitals. Information on safe sex is not gender-affirming; for example, condom demonstrations lack open conversation and services are structured in a binary manner. It is aggravated when people stare at you, and you can tell they are unsure whether you are a man or a woman. I try to avoid going to the clinic as much as possible, so I sometimes buy the medications I need from the black market. I know the risks, but it is better than going to a place where I feel violated. (FGD Participant_5)
Low SRH knowledge levels among lesbians and bisexual women
Participants felt that there were knowledge gaps between lesbian and bisexual communities, which implies that they had access to services. According to respondents, low knowledge levels of sexual risks associated with same-sex sexual practices are because they never really try to find knowledge of SRH. They might not get any help from it even if they find it out, as the information is heteronormative:
It has never bothered me to look for information concerning my SRH needs because even if I find out, where will I get them? Everything is about a man and a woman. (FGD Participant_2)
Little to no choice of healthcare facilities to access health for lesbians and bisexual women in Bulawayo
Participants highlighted that while choosing a healthcare facility from which to get service should be a right or an entitlement, this was not the case with lesbians and bisexual women in Bulawayo. Their choices were limited to a few NGO facilities running programs that support access to SRH services for lesbian and bisexual women:
. . . haha haha prefer? Do we have choices in Zimbabwe? We all go to PSI because we do not have any other options. (FGD Participant_5) . . . as time went on, because I continued to use that same outlet for healthcare services, we did see an improvement in terms of Sensitisation of Health Care Workers there as well as introducing new models such as the Differentiated Service Delivery model and where we have people that are already part of the Key Populations offering those services so it created that environment where you know you are getting services from someone that resonates with your struggle, so at the end of the day PSI is where I go for my services, and I have also referred some people there as well because there are no better alternatives. (FGD Participant_6)
Unavailability of specific SRH resources for lesbians and bisexual women
Another sub-theme that emerged under the main theme of challenges in accessing SRH services was the unavailability of specific services for lesbian and bisexual women. Respondents highlighted that most lesbian and bisexual women access SRH services from private institutions to meet their needs:
. . . It then prevents us from accessing some of the services that we would require, which may necessitate us visiting a private doctor and paying excessive fees just to receive the services we require. (FGD Participant_1)
Criminalisation of same-sex relationships
One of the sub-themes that emerged from the theme of challenges in accessing SRH services by lesbian and bisexual women is the criminalisation of same-sex relationships. The respondents referred to the constitution as a challenge or barrier; however, they could not explicitly point out what was a hindrance in the constitution:
Constitution not inclusive, and it condemns same-sex marriages. (FGD Participant_6) The current constitution hinders the uptake of SRH services among lesbians and bisexual women in Bulawayo. (FGD Participant_8)
Strategies to aid the uptake of SRH services by lesbians and bisexual women
Four sub-themes emerged under the main theme ‘strategies to aid the uptake of SRH services by Lesbians and bisexual women’. These are detailed below.
Friendly and affirming services
Participants cited that strategies that can help aid the uptake of SRH services for lesbians and bisexual men in Bulawayo are friendliness and affirmation. They prefer an environment that does not make them feel any different but affirms who they are, not ‘OTHER’ them:
. . . a place where I do not feel OTHERED. A place where they have sufficient knowledge, not where I have to explain how I regard my sexual orientation and gender identity. (FGD Participant_6) For me, it’s the environment; am I comfortable? Is there certain signage that when I walk in, I see that OK, these people acknowledge that I am lesbian and I am here, and they can help me get the best services, and it always comes even with a smile. (FGD Participant_3)
Using NGO facilities to access SRH services in Bulawayo
Participants expressed that while they would prefer many options of where to access health services, they are left with no option except to know that they can only access affirming health services from NGO-run healthcare facilities, such as Population Services International (PSI). These facilities provide friendly services as they have been sensitised to serving lesbians and bisexual women:
. . . we did see an improvement in terms of sensitisation of Health Care workers there as well as introducing new models such as the Differentiated Service Delivery model at PSI and where we have people who are already part of the Key Populations offering those services, so it created that environment where you know you are getting services from someone who resonates with your struggle. (FGD Participant_4) I find it easy to get my services at PSI Colours because I can get assistance from the DSDAs to quickly be served and receive the best services, especially since I can easily get my PrEP refill. I occasionally visit CeSHHAR because their services are pleasant. The nurses are not judgemental. (FGD Participant_1) Currently, most of us are receiving services and commodities from centres, such as GALZ, PSI, VoVo, and SRC. The services are far better than one would expect at a city council clinic in the locations. (FGD Participant_7)
Peer-led services as a strategy to aid the uptake of SRH for lesbians and bisexual women in Bulawayo
Respondents cited that their lesbian and bisexual peers were sources of SRH services. They shared that even at a health facility, they would prefer to be served by someone who identifies with their struggles:
. . . where we have people already part of the Key Populations offering those services, so it created an environment where you know you are getting services from someone that resonates with your struggle . . .. (FGD Participant_5) Some lesbians and bisexual women do not access SRH services due to stigma or labelling, and if much literacy or sensitisation is done for individuals and health care workers, otherwise Peer Educators are the most effective way for convenient services. (FGD Participant_3)
Training and sensitisation of healthcare providers on sexual orientation, gender identity, expression and sexual characteristics
Another sub-theme that emerged under the main theme was training healthcare providers and community sensitisation on sexual orientation, gender identity, expression and sexual characteristics (SOGIESC). Respondents highlighted that training healthcare providers help them to be able to be open about sexual practices without any fear of discrimination and stigma:
There is a need to facilitate training of health care providers so that they can be able to understand and be aware of the SRH needs of the lesbians and bisexual women and also so that we can become more open about our sexual practices. FGD Participant_2.
Themes that emerged from in-depth key informant interviews
Three themes were obtained, guided by the objectives and the interview guides. In addition, 12 sub-themes were obtained, guided by the research objectives and data collection tools, as summarised in Table 5. These themes are discussed in detail in the following sections.
Themes that emerged from in-depth key informant interviews.

SOGIESC, sexual orientation, gender identity, expression and sexual characteristics; SRH, Sexual and Reproductive Health.
Uptake of SRH services by lesbians and bisexual women
Clinical setting and availability of lesbians and bisexual women-specific SRH services
Under this sub-theme, respondents noted that public health facilities tend to shun individuals who identify as lesbian and bisexual women. These facilities do not include lesbian and bisexual women. Most health facilities lack services tailored to the needs of lesbian and bisexual women. This has resulted in most of the population going to a private institution or avoiding services and passing as heterosexual women to access services. However, this is challenging because most SRH services will not be met:
As a result, the majority of lesbians and bisexuals avoid public SRH services in favour of SRH services supported by NGOs, while some the few people who can afford it prefer private service providers. (LGBTI-friendly services are provided by NGOs such as the Association of LGBTI People in Zimbabwe (GALZ), the Center for Sexual Health and HIV-AIDS Research (CeSHAR), and the CeSHAR. Sexual Rights Centre (SRC) and PSI (KI_2)) The use of services by lesbians and bisexual women is generally fair, as most lesbians and bisexual women can pose as heterosexuals and do not need to disclose. However, it is fair to those who are not open to their sexuality. Still, for those who wear their sexuality on their sleeves, it becomes tricky because they have to fight the institutional barriers and societal perspectives because of who they identify as. (KI_5)
Attitudes of healthcare workers and past experiences
Healthcare workers’ attitudes can also determine the uptake of SRH services by lesbian and bisexual women in Bulawayo. A sub-theme that emerged on the uptake of SRH services by lesbians and bisexual women in Bulawayo is that while the healthcare workers’ role is to treat patients with dignity and respect, the case is mostly not the same when it comes to lesbians and bisexual women; in some instances, healthcare workers often stigmatise and discriminate against this population to the extent of insulting them; hence, they end up avoiding SRH services. Negative experiences with healthcare providers contribute to lesbian and bisexual women’s uptake of SRH services:
One of the many challenges, especially in public health hospitals, is the attitude of health care workers. While we would love to see our members receive services at the nearest facilities, most lesbian and bisexual women avoid these facilities and instead go downtown to sensitive institutions. (KI_6) Another thing to consider is the attitude of the medical staff themselves. Changing one’s attitude towards a particular issue is extremely difficult, regardless of how much training and awareness is provided. Although changing attitudes among older nurses is more difficult, progress has been made particularly among younger nurses. Younger nurses are more understanding and taking courses to learn more about lesbian, bisexual, and transgender issues. (KI_1)
Disclosure of sexual orientation
Another theme emerged: the uptake of SRH services among lesbians and bisexual women varies depending on the disclosure or non-disclosure of sexual orientation and gender identity to healthcare providers. Those who did not disclose their sexual orientation had limited negative incidences linked to their sexual orientation and could access services as heterosexual women. However, those with conditions such as fissures or any other reasons that required them to open up about their sexual practices have had many negative experiences, including a religious beliefs-based rebuke from healthcare workers:
. . . As a result, they have to pretend to be heterosexual and pose as heterosexual women, making it impossible for them to open up their sexual activities and seek comprehensive, equitable, and appropriate services for their needs. (KI_9)
High prevalence of risky sexual behaviour pushes lesbians and bisexual women to seek SRH services
Another sub-theme that emerged is the high prevalence of risky sexual behaviour among lesbian and bisexual women. The respondents highlighted a tendency among lesbian and bisexual women to want to please someone by engaging in sexual activities with someone. It was highlighted that in Zimbabwe, it is difficult for lesbians and bisexual women to live a ‘normal’ as same-sex relationships do not receive support compared to the heterosexual majority:
Lesbians and bisexual women engage in risky behaviours such as finger sex, oral sex, and group sex. This motivates people to use services. (KI_4) . . . usually some seek services after engaging in unprotected sex, especially after a night of heavy drinking. (KI_8) The biggest motivating factor for seeking services is probably if they have had unprotected sex and are unsure of their partner’s status. It’s difficult for them to live the ‘normal’ life in quotes, especially regarding sexuality issues. (KI_5)
Challenges faced by lesbians and bisexual women when accessing SRH services
Low levels of education and knowledge of SRH among lesbians and bisexual women
A sub-theme that emerged regarding the challenges faced by lesbians and bisexual women when accessing SRH is that there are low levels of education and knowledge of SRH among lesbian and bisexual women. The key informants cited that gaps in knowledge exist because there is little or no information, education or communication material for lesbians and bisexual women. The respondents also cited the information gap regarding SRH among lesbian and bisexual women, which, in turn, reduces the demand for HIV and other SRH services:
They do not have enough communication and IEC information, education, and communication] materials to disseminate information about SRH services. Of course, these IEC materials are physically produced by the government and proofread by the National AIDS Commission, so there is not much of this information. (KI_9) I observed inadequate information about HIV services, especially among the young lesbian and bisexual women I served here. You know, people come and start taking PrEP, then they stop taking it, and a few months later, they come back, and, unfortunately, they have HIV. Organisations should conduct an active outreach campaign because seeing these things here is heartbreaking. (KI_3) There is an information gap in understanding health-related issues, interpreting our health needs, and looking at the health-seeking behaviours of lesbians and bisexual women. There is little or limited research on the challenges of lesbians and bisexual women and interventions available for them. (KI_1)
Stigma and discrimination
Another sub-theme that emerged under the main theme of challenges in accessing SRH services was stigma and discrimination from healthcare workers towards lesbian and bisexual women. Respondents highlighted that younger nurses understand and conduct courses that help them better understand lesbian and bisexual issues:
Discrimination and stigma from community health workers impede their accessibility, their attitude changes negatively, or service delivery is poor when they know that one is lesbian or bisexual. There is whispering, finger pointing which hinders service accessibility and reduces confidence among lesbian/bisexual clients. (KI_4) The age-old stigma and discrimination stemming from the harsh homophobia mobilised during the Mugabe period continue to haunt LGBTI people in general and public sexual and reproductive health service providers in particular. As a result, most LGBTI people shun public reproductive health facilities. (KI_10)
Unavailability of lesbian and bisexual women-specific services
Another sub-theme that emerged under the main theme of challenges in accessing SRH services was the unavailability of specific services for lesbian and bisexual women. The respondents highlighted that most lesbian and bisexual women access SRH services as heterosexual women to avoid stigma and discrimination. However, due to a lack of appropriate and specific SRH services, the SRH needs of this population are not met:
Sometimes you will find that the services are not tailored to the needs of lesbians and bisexual women, and of course, then they have to be treated as normal women due to institutional barriers, stigma and discrimination, so it then prevents them from accessing some of the services that they would need which might mean they would go to a private doctor where they have to pay exorbitant amounts just for them to get the services that they need because there is no way you would go to Princess Margret and say I have got fissures because of my partner already it sets bells ringing because of the nature of sex that they engage in. (KI_7)
Criminalisation of same-sex sexual practices
Under the main theme of challenges faced by lesbians and bisexual women when accessing quality SRH services in Bulawayo, a sub-theme emerged: criminalising same-sex sexual practices in Zimbabwe is a fertile ground for all other challenges. The respondents highlighted that criminalisation makes lesbians and bisexual women scared of being visible even to healthcare workers, as they fear being arrested:
. . . The biggest challenge has been the relationship between the country’s laws and what biomedical science tells us. The criminalisation of same-sex relations makes people who engage in those activities feel criminalised. However, from a public health perspective, women who engage in same-sex relations must be identified and placed at the centre of all HIV interventions. It is difficult to find the same people you are criminalising. (KI_4) The biggest challenge, as I have pointed out, is certain provisions of the constitution, for example, same-sex marriages under the sexual offenses act, are classified as a criminal offense, and yet we have national documents that seek us to have biomedical interventions for women who have sex with women. (KI_2)
Strategies to aid the uptake of SRH services by lesbians and bisexual women
Self-awareness
A sub-theme that emerged on the strategies to aid the uptake of SRH services by lesbian and bisexual women in Bulawayo is the importance of self-awareness, which, in turn, helps one understand their risks and make informed choices:
In my opinion, as a counsellor, the priority is the person himself. A person can be a facilitator or barrier to themselves. Lesbians and bisexual women must be aware of who they are, accept themselves, and be out of the country. That way, they can demand their rights and be treated with respect and dignity. (KI_4) . . . and we do more than service provision. We make the person understand who they are, know their risk so that we can create a holistic person. (KI_2) Addressing self-stigma. Sometimes, people do not come out in the open, because they are hard on themselves. The lesbian and bisexual women community should accept who they are and be visible. (KI_7)
Sensitisation of the community on SOGIESC
Another sub-theme that emerged was the need to sensitise the community on basic SOGIESC. This will help the community to know who lesbian and bisexual women are and reduce discrimination and stigma:
We need to do sensitisation meetings, capacity building workshops and just go back to the basics SOGIESC (Sexual orientation gender identity and expression and sexual characteristics) where you are just teaching people on basic SOGIESC, where we teach health institutions, health service providers and the society. (KI_5) If we use the public health perspective to channel our movement toward access to equitable health services for lesbians and bisexual women, we are on a better footing than anything else. Therefore, we need to go there before we look at the policy and structural reforms. Let us look at one who is at the grassroots; if we change the grassroots, it is easier to influence policy reform because these are the same people who elect our policymakers, but if we elect someone who does not know it, then it becomes difficult, everyone needs to be educated on SOGIESC. (KI_10)
Lesbian and bisexual women affirmative training for healthcare providers
Another sub-theme that emerged under the main theme of strategies to aid the uptake of SRH services by lesbians and bisexual women was educating, training and sensitising health caregivers. Respondents highlighted that sensitisation of healthcare givers helps to reduce discrimination and stigma towards lesbian and bisexual women. This could increase the number of lesbian and bisexual women who access SRH services:
There is a need to facilitate sensitisation of health care providers so that they can understand and be aware of the SRH needs of the lesbians and bisexual women. (KI_1) We are fortunate to have partnerships with specific health facilities that can provide non-discriminatory, acceptable, and affirming health services. Working closely with peer educators and EPMs, lesbian and bisexual women can be referred to facilities trained, sensitised, and functioning as centres of excellence. We can refer to them and track and receive feedback on the quality of their services. Such feedback enables us to engage with service providers to improve their services continuously. (KI_4) However, some healthcare workers have become sensitised and are now champions for the lesbian/bisexual community in service delivery. As a result, there is less stigma and discrimination. (KI_2)
Human rights advocacy work of CSOs
The other sub-theme that emerged is that the work being done by civil society organisations can improve the circumstances for lesbian and bisexual women:
The fact is that civil society must continue its advocacy efforts for policy changes to occur. In civil society, we monitor the quality of services at the two PEPFAR-funded sites to identify improvement areas. (KI_8)
Discussion
This study found that concerns about discrimination and stigma from healthcare workers towards lesbian and bisexual women and the unavailability of lesbian and bisexual women-specific services were the leading challenges to accessing SRH services by lesbian and bisexual women in accessing SRH services. Those seeking health services frequently report discrimination and mistreatment by healthcare providers. This high level of stigma prevents them from accessing and using HIV prevention and treatment services. 24 The study also found that lesbian and bisexual women bear the brunt of insensitive healthcare workers. Some studies agree with this and suggest that access to services is impacted by unfavourable attitudes of healthcare workers (HIV service providers are frequently poorly equipped to serve key populations, and staff working in programs for these populations may lack the necessary sensitivity, skills and knowledge).25,26
The findings show that the unavailability of lesbian and bisexual women-specific services is also a challenge faced by lesbian and bisexual women. This influences the level of SRH service uptake in this group. These findings are strongly supported by those found by Narasimhan et al. that the lack of specific SRH resources for LGBT people is a barrier to accessing services. 27 Delany-Moretlwe et al. also revealed in their findings that most health systems were designed and implemented to accommodate heterosexual people because most information and resources do not address the practical SRH health issues confronted by sexual and gender minority (SGM) populations. 25
The findings also indicated low levels of education and knowledge of SRH among lesbian and bisexual women due to a lack of information, education and communication material for lesbians and bisexual women. The gap in knowledge regarding SRH among lesbian and bisexual women has reduced the demand for HIV and other SRH services. The study findings also showed that criminalising same-sex relationships is the basis for all the challenges lesbian and bisexual women face. It is also not inclusive and hinders the uptake of SRH services among lesbian and bisexual women. Mkhize and Maharaj and other authors support the findings that the criminalisation of same-sex marriages makes lesbians and bisexual women scared of being visible even to healthcare workers as they fear that they might be arrested.2,6,28
To improve the uptake of SRH among lesbian and bisexual women, the findings indicate that it is imperative to ensure the availability of lesbian and bisexual women-specific services. This is essential in ensuring that services are available at any time and in lesbian and bisexual women-friendly healthcare facilities. These findings are supported by Logie et al. and Narasimhan et al., who state that there is a need for the specialisation of services for lesbians and bisexuals to take up services by key populations for improvement.27,29
In addition, this study found that standard training in professional skills and ethical practices is required for healthcare professionals. Furthermore, there is a need to sensitise the community on basic SOGIESC, which will help the community know who lesbian and bisexual women are, and reduce discrimination and stigma. These findings echo similar sentiments as Mkhize and Maharaj and Radix and Maingi; LGBTI affirmative training for healthcare providers is needed, and sensitisation of the community on who the SGM persons are.25,28,30
This study also identified strategies to improve SRH service uptake among lesbian and bisexual women. In general, lesbian and bisexual women prefer SGM-friendly and inclusive clinical settings. 28 It was also noted that there is a need to enact a non-discrimination policy and legislative reform to include this group of people to achieve universal healthcare for all. The study also found that self-awareness among lesbian and bisexual women is needed to make one understand their risks and make informed choices. Studies have indicated the need to equip vulnerable populations with sufficient knowledge and target service providers to ensure a welcoming environment that would encourage good health-seeking behaviours in populations of interest.13,31–33 This needs to be taken into consideration in programming, as well as in the development of policies to ensure that they encourage the uptake of SRH services through the provision of adequate information.
Limitations
This study focuses on participants in the urban setting of Bulawayo. They were open to their sexuality and had ties or relationships with the Voice of the Voiceless. Only one focus group was included, which resulted in a small sample size. This could have resulted in those who had not disclosed being excluded, and their voices not being heard. As a result, the participants in this study had already expressed their sexual preferences, had been educated about their rights in general, and were ready to share their challenges with the health systems in seeking SRH services.
Conclusion
SRH services are crucial for achieving the 95-95-95 strategy and SDG target 3.7, which aims to ensure universal access to care, irrespective of sexual orientation. However, significant barriers undermine this goal for lesbian and bisexual women, primarily due to discrimination, stigma and lack of specialised services. Negative attitudes from healthcare providers and insufficient demand further exacerbate their vulnerability to contracting and spreading HIV infection. The absence of services tailored to unique needs diminishes SRH service uptake, highlighting the urgent need for clinical settings that are sensitive and responsive to this population. Targeted training for healthcare providers is essential to enhance access and improve health outcomes by focusing on inclusivity and cultural competency. Additionally, community sensitisation to sexual orientation and gender identity can help reduce stigma. Strengthening the connections between clinics and sexual health education programs, along with implementing non-discrimination policies, will create an enabling environment for lesbian and bisexual women to seek care. By addressing these critical challenges and supporting health intervention initiatives through appropriate legal and regulatory frameworks, a pathway for improving SRH outcomes can be established. These findings present a significant opportunity to influence policy and practice, ensuring that SRH services are accessible and equitable for all women regardless of their sexual orientation.
Supplemental Material
sj-docx-1-reh-10.1177_26334941241289553 – Supplemental material for Exploring challenges to the uptake of sexual and reproductive health services among lesbian and bisexual women in Bulawayo, Zimbabwe: a qualitative enquiry
Supplemental material, sj-docx-1-reh-10.1177_26334941241289553 for Exploring challenges to the uptake of sexual and reproductive health services among lesbian and bisexual women in Bulawayo, Zimbabwe: a qualitative enquiry by Methembe Yotamu Khozah and Wilfred Njabulo Nunu in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.